
Abstract
Objective
This study aims to investigate the relationship between oral health-related quality of life (OHRQoL) and emotional distress (ED), including anxiety and depression, in orthodontic patients.
Methods
A cross-sectional study was conducted involving 603 orthodontic patients, consisting of 401 females (66.5%) with a mean age of 24.15 ± 7.72 and 202 males (33.5%) with a mean age of 24.16 ± 7.72. A questionnaire containing questions of demographic information, the Oral Health Impact Profile (OHIP-14) and the Huaxi emotional-distress index (HEI) was employed to assess OHRQoL and ED. According to the HEI score, the respondents were divided into ED group (HEI > 8) and non-ED group (HEI ≤ 8). Data were analyzed using Kolmogorov–Smirnov test, Mann–Whitney test and logistic regression analysis with the significance level set at p < 0.05.
Results
The prevalence of poor OHRQoL and ED of the study sample was 28.4% and 19.57%, respectively. There was a significantly higher prevalence of ED among poor OHRQoL patients (35.67%) compared to those with good OHRQoL (13.19%) (p < 0.001). Poor OHRQoL and risky drinking behavior addressed higher significant correlation with ED patients than non-ED patients (p < 0.05). There were no statistical differences in other factors such as gender, age, and appliance type (p > 0.05). Poor OHRQoL orthodontic patients were at a higher risk of suffering from anxiety and depression compared to those with good OHRQoL (age-risky drinking behavior-sex-adjusted: OR = 4.00; all p < 0.001).
Conclusion
Oral health-related quality of life (OHRQoL) is related to emotional stress. Namely, patients with poor OHRQoL are more likely to experience anxiety and depression. As a result, orthodontists should consistently assess the emotional well-being and OHROoL of patients over the treatment course for better treatment outcomes.
Introduction
Malocclusion is a prevalent oral condition present in both children and adults.Citation1–3 Orthodontic treatment is a standard approach for treating dental misalignment.Citation4 Orthodontic treatment with orthodontic appliances usually involves a prolonged treatment duration, during which patients may experience inconvenience and discomfort, such as pain (including mucosal, tongue, and gingival discomfort caused by orthodontic appliances), reduced masticatory efficacy, dietary changes, speech difficulties, and social challenges.Citation5–7 Additionally, orthodontic appliances can lead to increased accumulation and retention of dental plaque, making oral hygiene maintenance more complex.Citation8,Citation9 Poor oral hygiene can result in permanent tissue damage, such as dental caries and periodontal diseases.Citation10,Citation11 In fact, approximately 50% to 70% of orthodontic patients experience issues such as gingivitis and dental fluorosis.Citation12 Orthodontic patients, especially those undergoing fixed orthodontic treatment, must employ additional measures (eg, mouthwash, interdental brushes, dental floss, regular professional dental cleaning, etc.) and invest time and effort in maintaining good oral hygiene.Citation13,Citation14 This presents a significant challenge, which may consequently lead to psychologically and emotionally adverse impact, ultimately impacting the oral health-related quality of life (OHRQoL) and emotional well-being (including depression and anxiety) of orthodontic patients.
Anxiety and depression are common emotional distress conditions in dentistry,Citation15–17 which is frequently co-occurring. Previous study reported that the odds of depression and anxiety comorbidity are 75% and 81%, respectively.Citation18 The psychological distress has negative impact on the treatment outcomes and management.Citation19 Orthodontic patients with anxiety or depression are more likely to resist future treatment,Citation20 exhibit poor compliance, and report lower treatment satisfaction.Citation21 Some clinicians reported that they usually feel pressured to manage patients with anxiety or depression.Citation22 Understanding the relationship between the quality of life, emotional distress, and orthodontic treatment is essential for providing better care to these patients.
Oral Health-Related Quality of Life (OHRQoL) is defined as
a subjective assessment that reflects an individual’s comfort during activities such as eating, sleeping, and engaging in social interactions; their self-esteem; and their satisfaction with respect to oral health.Citation23
It is evident that the OHRQoL of orthodontic patients may undergo changes during orthodontic treatment, and it might even decrease. The psychological dimension of poor OHRQoL has been associated with anxiety and depression, and impaired OHRQoL is considered a predictor of such emotional distress.Citation24,Citation25 However, these studies often had limited subject populations, primarily focusing on females or patients with specific diseases such as oral tumors, without addressing orthodontic patient populations.
The orthodontic patients who are suffering from dental treatments may have a great chance to experience unpleasant OHRQoL as well as comorbid emotional distress. The emotional well-being and OHRQoL of orthodontic patients have been of great concern, but previous research has not provided conclusive guidance for orthodontic practitioners.Citation26,Citation27 Consequently, the problem that this study seeks to address is the complex interplay between emotional distress (anxiety and depression) and the OHRQoL of orthodontic patients.
Therefore, in this study, we aimed to investigate the relationship between quality of life related to oral health and emotional distress, specifically depression and anxiety, among orthodontic patients. We hypothesize that the OHRQoL of orthodontic patients is related to emotional stress. The rationale for the study lies in the need to address the potential emotional and psychological consequences of orthodontic treatment, which can impact the overall well-being of patients. By exploring this relationship, the study seeks to provide insights that can benefit orthodontic practitioners and enhance patient care.
Materials and Methods
This study was approved by the Institutional Review Board of West China Hospital of Stomatology (Approval no. WCHSIRB-D-2020-209).
Subjects
The sample size was calculated using G*Power version 3.1.9.7, assuming: effect size = 0.3; α (two tailed) = 0.05; power (1-β) err prob = 0.9. At least 590 participants were required for the study.
Consecutive patients aged 12 and above seeking care at the Department of Orthodontics were recruited over a three-month period. West China Hospital of Stomatology is a Class A tertiary hospital in Southwest China with a large number of patients. Eligible patients signed the informed consent when completing the questionnaires. We conducted a cross-sectional survey with 603 patients, consisting of 401 females (66.5%) with a mean age of 24.15 ± 7.72, and 202 males (33.5%) with a mean age of 24.16 ± 7.72. These patients visited the Department of Orthodontics of West China Hospital of Stomatology (Chengdu, China) from July 2020 to September 2020.
The inclusion criteria comprised (1) willingness to participate in the survey; (2) patients diagnosed with Class I/II/III malocclusion undergoing orthodontic treatment with clear aligners or labial fixation appliances; (3) patients capable of finishing the questionnaire independently. Exclusion criteria included (1) presence of major psychiatric disorders and/or drug abuse; (2) presence of major trauma and/or operations; (3) current consumption of central nervous system agents; and (4) cognitive impairment and/or illiteracy; (5) time to fill in the questionnaire too short (<200 seconds) or too long (>800 seconds), or have significant inconsistencies in answers.
Data Collection
All participants completed a two-part questionnaire. The first part collected respondents’ personal information, including gender, age, education, income, smoking, alcohol consumption, treatment duration, and appliance type. The other part evaluated the levels of emotional stress (ED) and oral health-related quality of life (OHRQoL).
Emotional Distress Analysis
Assessment of the level of ED (anxiety and depression) was conducted by the Huaxi emotional-distress Index (HEI). It is a feasible screening tool for emotional distress (anxiety and depression) designated in non-psychiatric clinical settings in China. This screening instrument was derived from a comprehensive revision of various popular assessment instruments for psychological and emotional distress, in which the most valid and optimal items and scales for evaluating depression and anxiety were adopted and adjusted for Chinese patients.Citation28 The internal consistency of HEI was satisfactory, with Cronbach’s α = 0.90 reported by Wang J, et alCitation28 and α = 0.918 by Wang Y, et alCitation29 respectively.
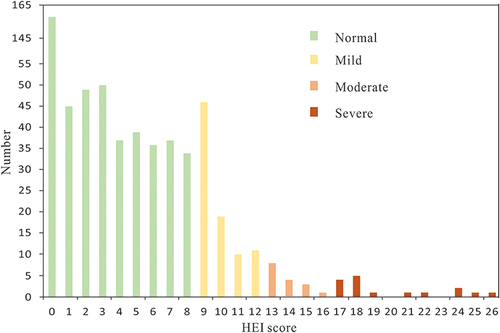
HEI consists of 9 self-reported items (5 items pertaining to depression and 4 to anxiety) evaluated on a 5-point Likert-scale: 0 to 4 point (never to nearly all the time). The total HEI score is a sum of scores of the 9 items. A higher HEI score indicates a higher level of severity in the corresponding emotional distress. The standard cut-off scores for each level were as follows: normal (0–8 points); mild (9–12 points); moderate (13–16 points); and severe (17–36 points).
Oral Health-Related Quality of Life Analysis
OHRQoL was evaluated by the Oral Health Impact Profile (OHIP-14).Citation30,Citation31 This widely utilized scale has demonstrated satisfactory reliability (Cronbach’s α = 0.942 reported by Yang et al)Citation32 and is applicable to public oral investigations.Citation33–37 The OHIP-14 questionnaire is a widely used scale for measuring OHRQoL applied for all age. The scale has 14 questions distributed across seven domains: functional limitations, somatic pain, psychological discomfort, physical disability, psychological impairment, social impairment, and disability. For each question, respondents are asked to rate how frequently they had experienced an oral impact during treatment. The response to the specific item was scored on a 5-point Likert-type response scale: “never” = 0; “hardly ever” = 1; “occasionally” = 2; “fairly often” = 3; and “very often” = 4. A sum of all item scores generated a total OHIP-14 score from 0 to 56.Citation38
Higher OHIP-14 scores denoted poorer oral-related quality of life. In this study, OHIP-14 >14 were considered to have a poor OHRQoL whereas OHIP-14 ≤14 were classed as good OHRQoL.
Statistical Analysis
The data were analyzed by Microsoft Excel 2019 and SPSS (version 23.0). Microsoft Excel was used for editing, sorting, and coding. The Excel file was then imported into SPSS software. Quantitative variables were presented by measures of centrality (mean and median) and variability (standard deviation and interquartile range). A Kolmogorov–Smirnov test was performed to determine the distribution type of the data. OHIP-14 scores and HEI scores in this study were in skewed distributions. Comparison of the median of continuous variables was analyzed using Mann–Whitney test. Logistic regression model was used to estimate odds ratios (ORs) and 95% confidence intervals (95% CIs) of the association between OHRQoL and risk of having ED. In all analyses, p-value <0.05 was considered statistically significant.
Results
Of the 603 subjects in this study, 401 (66.5%) patients were females and 202 (33.5%) were males. The mean age of the sample was 24.15 ± 7.72 years, with age ranging from 12 to 48. The mean orthodontic treatment period was 20.42 ± 14.25 months.
The majority of the study sample reported good OHRQoL (71.6%) and non-ED status (80.43%) (). The median scores of HEI score and OHIP-14 score were 3 (0, 8) and 9 (4, 15), respectively.
Table 1 Sample Characteristics
In this study, 19.57% of the population were classed as ED patients, and 28.4% were reported to have poor OHRQoL (). Individuals with poor OHRQoL had a higher prevalence of ED (35.67%) than good OHRQoL (13.19%). The majority (86 out of 118, 73%) of ED patients were in mild level while the rest (32 out of 118, 27%) had moderate or severe ED ().
Figure 1 Histogram of the Hua Xi Emotional-distress Index (HEI) score in the overall study sample (N = 603).
OHRQoL and risky drinking behavior exerted significant effect on subjects’ emotional status (p < 0.05) (). Subjects with poor OHRQoL and excessive alcohol use had a significantly higher possibility of having emotional distress. Scores of all domains of OHIP-14 of ED patients were significantly higher than those in non-ED patients (p < 0.001) ().
Table 2 Effects of Factors on Emotional Distress
Table 3 Effect of OHIP Domains on Emotional Distress
Compared with good OHRQoL patients, poor OHRQoL were at a higher risk of ED (OR = 4.37; 95% CI: 2.77, 6.90; p < 0.0001) in the unadjusted model (). After adjustments for age (Model 1: OR = 4.19; 95% CI: 2.65, 6.63; p < 0.0001), age and risky drinking behavior (Model 2: OR = 4.07; 95% CI: 2.56, 6.45; p < 0.0001), and age, risky drinking behavior and sex (Model 3: OR = 4.00; 95% CI: 2.52, 6.36; p < 0.001), OR values varied very slightly, that is, the association between poor OHRQoL and ED did not change after three-time adjustment.
Table 4 Logistic Regression Analysis of Association Between OHRQoL and ED
Discussion
The aim of the study is to evaluate the correlation between oral health-related quality of life (OHRQoL) and anxiety and depression (emotional distress, ED) of orthodontic patients. The results indicate patients with poor OHRQoL and excessive alcohol use are more likely to experience anxiety and depression.
Compared with objective indicators, OHRQoL reflects patients’ subjective self-evaluation of oral function, oral symptoms, and oral social-psychological effectsCitation30, which are important reports of patients’ self-perception. M Romero-Maroto evaluated the dental-related social impact, psychological impact and anxiety level of orthodontic patients. They found that the greater the dental-related social impact and psychological impact of orthodontic patients, the more severe the anxietyCitation39. Anthony J Ireland measured the anxiety and orthodontic pain in 1000 adolescents and discovered a positive correlation between the twoCitation40. Feifei Zhang investigated the brain magnetic resonance imaging (MRI) of 48 orthodontic patients and reported anxiety as a mediator of the neural mechanisms of orthodontic painCitation41. These studies indirectly support our findings, and we speculate that emotional stress and OHRQoL in orthodontic patients influence each other. Although the underlying mechanism of the correlation between OHRQoL and anxiety and depression is not clear, we believe that improving the oral life quality of orthodontic patients helps manage their emotions, which is conducive to orthodontic treatment management.
Consistent with the present study, a meta-analysis carried out by Vidigal et al suggested that orthodontic treatment does not decrease quality of life of orthodontic patients.Citation42 A systematic review done by Mandava et al even found evidence showing that fixed orthodontic treatment can improve OHRQoL.Citation43 Johal et al discovered that fixed appliances negatively impact dental quality of life during the first 3 months of the treatment period.Citation44 We believe that OHRQoL can worsen at the initial stage of treatment when patients have not yet adapted to the discomfort and pain, as well as unaesthetic appearance that comes along with fixed orthodontic appliances. What mentioned above may result in a sense of unsatisfaction, hence, lead to a decrease in OHRQoL. Once the patients have adapted to these unpleasant events and gain positive feedback of the orthodontic correction during treatment, the level of OHRQoL is likely to increase. Therefore, it will benefit patients’ therapeutic experience if orthodontists inform the inconveniences and provide reassurance, relieve discomfort and pain during treatment that may arise before they receive the treatment.
Although most individuals had a good OHRQoL, a certain concerning number of patients may develop emotional distress. In the present study, 19.12% of the orthodontic patients had emotional distress of anxiety or depression, which was close to 18.7% in the study of Joanie Roy DDS et al.Citation45 The incident rate of moderate-to-severe anxiety or depression of our sample was 5.30%, which matched the reported result of 5.4% by Wu et al for non-psychiatric outpatients using the same measuring scale in the study.Citation46 That is, about one in every five orthodontic patients may have anxiety or depression, which manifests that emotional distress is a common issue among orthodontic patients. The chance of possessing a low emotional status was much higher for those with poor OHRQoL in this study. The positive correlation between OHRQoL and depression and anxiety found in our study is consistent with Choi et al’s longitudinal study which reported a significant correlation between a higher total OHIP-14 score and increased levels of depression and anxiety.Citation47 Agou et al’s study confirmed the mediator role of emotional well-being when assessing patients’ OHRQoLCitation48. Therefore, we suggest that clinicians should take a combination of emotional health and OHRQoL into consideration during evaluation of orthodontic treatment.
In this study, we observed that physical pain and psychological discomfort were the areas where patients expressed the most dissatisfaction, while most individuals reported good oral health-related quality of life. Common issues included pain, altered taste perception, discomfort while eating, and feeling self-conscious in front of others. To improve patients’ quality of life, several strategies can be implemented. Orthodontic pain can be managed through various methods, including medication,Citation49 mechanical therapies,Citation50 behavioral interventions such as cognitive-behavioral therapy (CBT),Citation51 musicCitation52 and exercise.Citation53 Combining these approaches, especially during the initial phases of orthodontic treatment when pain is most pronounced, can alleviate patients’ discomfort and help them adapt more comfortably to their orthodontic appliances.
Additionally, emotional support and reassurance during patient visits, along with follow-up telephone calls,Citation54 can contribute to reducing orthodontic patients’ pain experience. To address eating-related discomfort, dietary guidance tailored to the patient’s specific needs should be provided. For individuals experiencing social discomfort due to orthodontic treatment, encouragement and emotional support during follow-up appointments can be invaluable. Given that our study highlighted the emotional distress reported by adult females, clinical care should place particular emphasis on understanding and addressing the emotional well-being of this demographic.
Notably, we found that alcohol use appears to be one of the methods orthodontic patients express anxiety or depression, and most of these patients are adults. Many studies have proved that alcohol use problem in adolescence is significantly associated with adult alcohol abuse and adverse consequences.Citation55–57 The questionnaire we employed defines the problem as consuming an excessive amount (more than recommended) of alcohol per week, per day or per time. That is, there is a clear risk of harm to health due to drinking behavior or alcohol consumptionCitation58. In this study, adolescents only made up 3.7% of the study population; however, 16% of them admitted that they have an over-drinking history. The result gave a small but alerting number of orthodontic patients in young age having drinking problem. Meanwhile, there is very little study concerning this topic. Hence, more attention should be paid to the orthodontic patient group with drinking problem in the future study, especially to teenager. Considering that adolescents are the main group of orthodontic clinics, we suggest public education on alcohol use, such as posting posters or signs on the corridor walls and waiting halls in the clinics.
The sex differences in anxiety and depression levels during orthodontic treatment remain contentious. In previous studies, adult orthodontic patients have attracted much attention, and adult female orthodontic patients are generally considered to have more complex psychological characteristics than male counterparts.Citation59–61 Some studies gave a different opinion that adult female patients tend to describe a higher level of anxiety and depression.Citation58,Citation62 However, in this study, the differences in age and sex were statistically insignificant. The result is consistent with Adrián Curto et al’s study which employed the same protocol for OHRQoL.Citation26 The contradiction may be due to the discrepancies in evaluation protocol or sample ethnic.
Although the effect of age was insignificant in this study, we propose that more attention should be paid to adults’ emotional status and OHRQoL. The analysis of impacts on the gender and the types of orthodontic appliance showed that compared to the underage, grown-ups are more readily differentiated. Choi et al suggested that the self-reported OHRQoL of adults seemed more negative than that of teenagers.Citation47 We found that literature in the consistent field mainly focuses on children and adolescence. Undoubtedly, there is an increasing demand of orthodontic therapy among adults; therefore, more efforts and attentions are required to investigate the OHRQoL and emotional well-being of the grown population to better understand this group.
The findings found insignificant correlation between types of orthodontic appliances and ED. Meanwhile, in Gao et al’s study,Citation63 the anxiety levels of invisible appliance treatment patients did not differ significantly from those of fixed ones. However, previous studies have concluded that invisible aligner patients experience less pain compared to fixed alignersCitation63–65. We suppose that physical pain may not significantly affect patients’ emotional status once people get used to the appliances. We suggest that for pain-sensitive patients, clinicians could provide invisible aligners as an option to reduce the pain and anxiety or depression that may be experienced by patients during treatment course.
Strengths of our study include identifying a significant relationship between OHRQoL and emotional distress in orthodontic patients, contributing valuable insights to the field. We undertook a comprehensive exploration of the topic by assessment of a broad range of factors, including demographic information, OHRQoL, and emotional distress, thus enhancing the depth of our analysis.
However, the study has limitations. Firstly, the predominance of female participants due to the continuous recruitment method employed in our sample introduced gender imbalance, which, while accurately reflecting the orthodontic patient population, may limit the generalizability of our findings to a broader demographic. Additionally, as a cross-sectional study, it cannot establish causality between variables, necessitating further study to determine the causal relationship between poor OHRQoL and emotional distress. Finally, we used a relatively simplified assessment tool for emotional distress, whereas a more comprehensive and sophisticated instrument such as the Depression, Anxiety, and Stress Scale 21 (DASS21) could have provided a deeper understanding of the relationships between variables.
To build upon the findings of our study, future research should address the identified limitations and explore new avenues of inquiry. It is essential to expand the scope of research to include larger and more diverse samples of orthodontic patients, allowing for a more comprehensive understanding of the dynamics of psychological well-being and OHRQoL during and after orthodontic treatment. Longitudinal studies should be considered to establish causal relationships between OHRQoL and emotional distress, shedding light on the specific mechanisms that underlie this correlation.
Conclusion
To conclude, the oral health-related quality of life (OHRQoL) is related to emotional stress. Namely, patients with poor OHRQoL are more likely to experience anxiety and depression. As a result, orthodontists should consistently assess the emotional well-being and OHROoL of patients over the treatment course for better treatment outcomes.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding authors (Xin Xiong and Shufang Du) upon reasonable request.
Ethics Statement
This study is in line with the Declaration of Helsinki. The studies involving human participants were reviewed and approved by the Ethical Committee of West China Hospital of Stomatology (WCHIRB-D-2020-209).
Disclosure
The authors declare that they have no conflicts of interest in this work.
Additional information
Funding
References
- Egić B. Prevalence of orthodontic malocclusion in schoolchildren in Slovenia. A prospective aepidemiological study. Eur J Paediatr Dent. 2022;23(1):39. doi:10.23804/ejpd.2022.23.01.07
- Silva RG, Kang DS. Prevalence of malocclusion among Latino adolescents. Am J Orthod Dentofacial Orthop. 2001;119(3):313–315. doi:10.1067/mod.2001.110985
- Agarwal SS, Jayan B, Chopra SS. An Overview of Malocclusion in India. J Dent Health Oral Disord Ther. 2016;3(3):00092.
- Zhang M, Mcgrath C, Hägg U. The impact of malocclusion and its treatment on quality of life: a literature review. Int J Paediatr Dent. 2006;16(6):381–387.
- Long H, Wang Y, Jian F, et al. Current advances in orthodontic pain. Int J Oral Sci. 2016;8(2):67–75. doi:10.1038/ijos.2016.24
- Trein MP, Mundstock KS, Maciel L, et al. Pain, masticatory performance and swallowing threshold in orthodontic patients. Dental Press J Orthod. 2013;18(6):117–123. doi:10.1590/S2176-94512013000600018
- Wu A, McGrath C, Wong RWK, et al. Comparison of oral impacts experienced by patients treated with labial or customized lingual fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2011;139(6):784–790. doi:10.1016/j.ajodo.2009.07.027
- Ren Y, Jongsma MA, Mei L, et al. Orthodontic treatment with fixed appliances and biofilm formation--a potential public health threat? Clin Oral Investig. 2014;18(7):1711–1718. doi:10.1007/s00784-014-1240-3
- Sunil PC, Michael T, Raju AS, et al. Evaluation of micro-organism in ligated metal and self-ligating brackets using scanning electron microscopy: an in vivo study. J Int Oral Health. 2015;7(7):58–62.
- Bignozzi I, Crea A, Capri D, et al. Root caries: a periodontal perspective. J Periodontal Res. 2014;49(2):143–163. doi:10.1111/jre.12094
- Lopez R, Smith PC, Göstemeyer G, et al. Ageing, dental caries and periodontal diseases. J Clin Periodontol. 2017;44(Suppl 18):S145–S152. doi:10.1111/jcpe.12683
- Ogaard B, Larsson E, Henriksson T, et al. Effects of combined application of antimicrobial and fluoride varnishes in orthodontic patients. Am J Orthod Dentofacial Orthop. 2001;120(1):28–35. doi:10.1067/mod.2001.114644
- Migliorati M, Isaia L, Cassaro A, et al. Efficacy of professional hygiene and prophylaxis on preventing plaque increase in orthodontic patients with multibracket appliances: a systematic review. Eur J Orthod. 2015;37(3):297–307. doi:10.1093/ejo/cju044
- Seidel CL, Gerlach RG, Weider M, et al. Influence of probiotics on the periodontium, the oral microbiota and the immune response during orthodontic treatment in adolescent and adult patients (ProMB Trial): study protocol for a prospective, double-blind, controlled, randomized clinical trial. BMC Oral Health. 2022;22(1):148. doi:10.1186/s12903-022-02180-8
- Hirota SK, Moreno RA, Dos Santos CHR, et al. Psychological profile (anxiety and depression) in patients with oral lichen planus: a controlled study. Minerva Stomatol. 2013;62(3):51–56.
- Lei J, Yap AU, Zhang M, et al. Temporomandibular disorder subtypes, emotional distress, impaired sleep, and oral health‐related quality of life in Asian patients. Community Dent Oral Epidemiol. 2021;49(6):543–549. doi:10.1111/cdoe.12643
- Suresh KV, Shenai P, Chatra L, et al. Oral mucosal diseases in anxiety and depression patients: hospital based observational study from south India. J Clin Exp Dent. 2015;7(1):e95. doi:10.4317/jced.51764
- Lamers F, van Oppen P, Comijs HC, et al. Comorbidity patterns of anxiety and depressive disorders in a large cohort study: the Netherlands Study of Depression and Anxiety (NESDA). J Clin Psychiatry. 2011;72(3):3397. doi:10.4088/JCP.10m06176blu
- Clarke DM, Currie KC. Depression, anxiety and their relationship with chronic diseases: a review of the epidemiology, risk and treatment evidence. Med J Aust. 2009;190(S7):S54–S60. doi:10.5694/j.1326-5377.2009.tb02471.x
- Azaripour A, Weusmann J, Mahmoodi B, et al. Braces versus Invisalign(R): gingival parameters and patients’ satisfaction during treatment: a cross-sectional study. BMC Oral Health. 2015;15(1):69. doi:10.1186/s12903-015-0060-4
- Thomas T, Robinson C, Champion D, et al. Prediction and assessment of the severity of post-operative pain and of satisfaction with management. Pain. 1998;75(2–3):177–185. doi:10.1016/S0304-3959(97)00218-2
- Hill KB, Hainsworth JM, Burke FJT, et al. Evaluation of dentists’ perceived needs regarding treatment of the anxious patient. Br Dent J. 2008;204(8):E13–E13. doi:10.1038/sj.bdj.2008.318
- Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. 2011;90(11):1264–1270. doi:10.1177/0022034511399918
- Boman UW, Wennström A, Stenman U, et al. Oral health-related quality of life, sense of coherence and dental anxiety: an epidemiological cross-sectional study of middle-aged women. BMC Oral Health. 2012;12(1):14. doi:10.1186/1472-6831-12-14
- Hassel AJ, Danner D, Freier K, et al. Oral health-related quality of life and depression/anxiety in long-term recurrence-free patients after treatment for advanced oral squamous cell cancer. J Craniomaxillofac Surg. 2012;40(4):e99–e102. doi:10.1016/j.jcms.2011.05.011
- Curto A, Alvarado-Lorenzo A, Albaladejo A, et al. Oral-health-related quality of life and anxiety in orthodontic patients with conventional brackets. Int J Environ Res Public Health. 2022;19(17):10767. doi:10.3390/ijerph191710767
- Wang J, Tang X, Shen Y, et al. The correlations between health-related quality of life changes and pain and anxiety in orthodontic patients in the initial stage of treatment. Biomed Res Int. 2015;2015:725913. doi:10.1155/2015/725913
- Wang J, Guo W-J, Zhang L, et al. The development and validation of Huaxi emotional-distress index (HEI): a Chinese questionnaire for screening depression and anxiety in non-psychiatric clinical settings. Compr Psychiatry. 2017;76:87–97. doi:10.1016/j.comppsych.2017.04.001
- Wang Y, Ye JL, Chen T, Zhang L. Assessment of psychometric properties of the Huaxi Emotional-distress. Gen Hosp Psychiatry. 2023;84:188–193. doi:10.1016/j.genhosppsych.2023.07.007
- Locker D, Allen F. What do measures of ‘oral health-related quality of life’ measure? Community Dent Oral Epidemiol. 2007;35(6):401–411. doi:10.1111/j.1600-0528.2007.00418.x
- Xin WN, Ling JQ. Validation of a Chinese version of the oral health impact profile-14. Zhonghua Kou Qiang Yi Xue Za Zhi. 2006;41(4):242–245.
- Yang GH, Feng Y, Xue L-X, et al. Factorial structure and measurement invariance of the Chinese version of the Oral Health Impact Profile-14 among clinical populations and non-clinical populations: an evidence for public oral investigations. BMC Oral Health. 2023;23(1):588. doi:10.1186/s12903-023-03310-6
- Chen M, Feng Z-C, Liu X, et al. Impact of malocclusion on oral health-related quality of life in young adults. Angle Orthod. 2015;85(6):986–991. doi:10.2319/101714-743.1
- He S, Wei S, Wang J. Chronic periodontitis and oral health-related quality of life in Chinese adults: a population-based, cross-sectional study. J Periodontol. 2018;89(3):275–284.
- Huang S, Liu Y, Li M, et al. Oral health knowledge, attitudes, and practices and oral health-related quality of life among stroke inpatients: a cross-sectional study. BMC Oral Health. 2022;22(1):410. doi:10.1186/s12903-022-02446-1
- Lin F, Ye Y, Ye S, et al. Effect of personality on oral health-related quality of life in undergraduates. Angle Orthod. 2018;88(2):215–220. doi:10.2319/051017-322.1
- Tang T, Zhang L, Hou Y-F, et al. A prospective study of changes in oral health-related quality of life during “all-on-four” immediate restoration for edentulous individuals. Shanghai Kou Qiang Yi Xue. 2018;27(1):52–55.
- Uzarevic Z, Bulj A. Oral health-related quality of life among Croatian university students. Int J Environ Res Public Health. 2021;18(12):6483. doi:10.3390/ijerph18126483
- Romero-Maroto M, Santos‐Puerta N, González Olmo MJ, et al. The impact of dental appearance and anxiety on self-esteem in adult orthodontic patients. Orthod Craniofac Res. 2015;18(3):143–155. doi:10.1111/ocr.12091
- Ireland AJ, Ellis P, Jordan A, et al. Chewing gum vs. ibuprofen in the management of orthodontic pain, a multi-centre randomised controlled trial–the effect of anxiety. J Orthod. 2017;44(1):3–7. doi:10.1080/14653125.2016.1277317
- Zhang F, Li F, Yang H, et al. Altered brain topological property associated with anxiety in experimental orthodontic pain. Front Neurosci. 2022;16:907216. doi:10.3389/fnins.2022.907216
- Vidigal M, Mesquita CM, De Oliveira MN, et al. Impacts of using orthodontic appliances on the quality of life of children and adolescents: systematic review and meta-analysis. Eur J Orthod. 2022;44(4):359–368. doi:10.1093/ejo/cjac003
- Mandava P, Singaraju GS, Obili S, et al. Impact of self-esteem on the relationship between orthodontic treatment and the oral health-related quality of life in patients after orthodontic treatment - a systematic review. Med Pharm Rep. 2021;94(2):158–169. doi:10.15386/mpr-1843
- Johal A, Alyaqoobi I, Patel R, et al. The impact of orthodontic treatment on quality of life and self-esteem in adult patients. Eur J Orthod. 2015;37(3):233–237. doi:10.1093/ejo/cju047
- Joanie Roy DDS. Dental anxiety associated with orthodontic care: prevalence and contributing factors. 2018.
- Wan-Jun Guo HWWD, Chun-Tao Shen TRWW, Zeng NCWL. Effects of anxiety and depression and early detection and management of emotional distress on length of stay in hospital in non-psychiatric inpatients in China: a hospital-based cohort study. Lancet. 2019;3:394.
- Choi SH, Cha J-Y, Lee K-J, et al. Changes in psychological health, subjective food intake ability and oral health-related quality of life during orthodontic treatment. J Oral Rehabil. 2017;44(11):860–869. doi:10.1111/joor.12556
- Agou S, Locker D, Muirhead V, et al. Does psychological well-being influence oral-health-related quality of life reports in children receiving orthodontic treatment? Am J Orthod Dentofacial Orthop. 2011;139(3):369–377. doi:10.1016/j.ajodo.2009.05.034
- Kaya Y, Alkan Ö, Kömüroglu AU, et al. Effects of ibuprofen and low-level laser therapy on orthodontic pain by means of the analysis of interleukin 1-beta and substance P levels in the gingival crevicular fluid. J Orofac Orthop. 2021;82(3):143–152. doi:10.1007/s00056-020-00254-2
- Lobre WD, Callegari BJ, Gardner G, et al. Pain control in orthodontics using a micropulse vibration device: a randomized clinical trial. Angle Orthod. 2016;86(4):625–630. doi:10.2319/072115-492.1
- Wang J, Wu D, Shen Y, et al. Cognitive behavioral therapy eases orthodontic pain: EEG states and functional connectivity analysis. Oral Dis. 2015;21(5):572–582. doi:10.1111/odi.12314
- Aly AE, Hansa I, Ferguson DJ, et al. The effect of alpha binaural beat music on orthodontic pain after initial archwire placement: a randomized controlled trial. Dental Press J Orthod. 2023;27(6):e2221150. doi:10.1590/2177-6709.27.6.e2221150.oar
- Sandhu SS, Sandhu J. Effect of physical activity level on orthodontic pain perception and analgesic consumption in adolescents. Am J Orthod Dentofacial Orthop. 2015;148(4):618–627. doi:10.1016/j.ajodo.2015.04.037
- Cozzani M. Self-reported pain after orthodontic treatments: a randomized controlled study on the effects of two follow-up procedures. Eur J Orthod. 2016;38(3):266–271. doi:10.1093/ejo/cjv032
- Huurre T, Lintonen T, Kaprio J, et al. Adolescent risk factors for excessive alcohol use at age 32 years. A 16-year prospective follow-up study. Soc Psychiatry Psychiatr Epidemiol. 2010;45(1):125–134. doi:10.1007/s00127-009-0048-y
- McCambridge J, McAlaney J, Rowe R, Lanphear BP. Adult consequences of late adolescent alcohol consumption: a systematic review of cohort studies. PLoS Med. 2011;8(2):e1000413. doi:10.1371/journal.pmed.1000413
- Silins E, Horwood LJ, Najman JM, et al. Adverse adult consequences of different alcohol use patterns in adolescence: an integrative analysis of data to age 30 years from four Australasian cohorts. Addiction. 2018;113(10):1811–1825. doi:10.1111/add.14263
- Wu Y, Xiong X, Fang X, et al. Psychological status of TMD patients, orthodontic patients and the general population during the COVID-19 pandemic. Psychol Health Med. 2021;26(1):62–74. doi:10.1080/13548506.2020.1858489
- Kang JM, Kang KH. Effect of malocclusion or orthodontic treatment on oral health-related quality of life in adults. Korean J Orthod. 2014;44(6):304–311. doi:10.4041/kjod.2014.44.6.304
- Tang X, Cai J, Lin B, et al. Motivation of adult female patients seeking orthodontic treatment: an application of Q-methodology. Patient Prefer Adherence. 2015;9:249–256. doi:10.2147/PPA.S78691
- Yi S, Zhang C, Ni C, et al. Psychosocial impact of dental aesthetics and desire for orthodontic treatment among Chinese undergraduate students. Patient Prefer Adherence. 2016;10:1037–1042. doi:10.2147/PPA.S105260
- Cotrin P, Peloso RM, Oliveira RC, et al. Impact of coronavirus pandemic in appointments and anxiety/concerns of patients regarding orthodontic treatment. Orthod Craniofac Res. 2020;23(4):455–461. doi:10.1111/ocr.12395
- Gao M, Yan X, Zhao R, et al. Comparison of pain perception, anxiety, and impacts on oral health-related quality of life between patients receiving clear aligners and fixed appliances during the initial stage of orthodontic treatment. Eur J Orthod. 2021;43(3):353–359. doi:10.1093/ejo/cjaa037
- Fujiyama K, Honjo T, Suzuki M, et al. Analysis of pain level in cases treated with Invisalign aligner: comparison with fixed edgewise appliance therapy. Prog Orthod. 2014;15(1):64. doi:10.1186/s40510-014-0064-7
- White DW, Julien KC, Jacob H, et al. Discomfort associated with Invisalign and traditional brackets: a randomized, prospective trial. Angle Orthod. 2017;87(6):801–808. doi:10.2319/091416-687.1