
Abstract
Purpose
The purpose of the study was to assess the sense of coherence and its relationship with oral health and other study variables among adult patients at university dental hospital.
Patients and Methods
This cross-sectional study included adult patients visiting the Dental Hospital of the College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam. Sense of coherence was determined by Antonovsky’s Sense of Coherence scale (SOC-13), which consists of 13 items on a 7-point Likert. DMFT index, plaque index, gingival index, and simplified oral hygiene index were used to evaluate the oral health of study participants. Bivariate and multivariable analyses were performed, and 0.05 level of significance was used in the study.
Results
The study included the data of 558 participants with a mean age of 32.19±10.11 years. The mean score of SOC was 52.77±13.11, which was significantly higher in high-income participants (P <0.001), participants without a medical condition (P=0.021), non-smokers (P <0.001), and those who visited the dentist in less than one year (P=0.028). Bivariate analysis showed statistically significant negative correlations between SOC and DMFT index (P=0.002), SOC and plaque index (P <0.001), SOC and gingival index (P=0.002), and SOC and simplified oral hygiene index (P=0.001). Multivariable analysis also showed that SOC was significantly correlated with DMFT index (P=0.001), plaque index (P <0.001), gingival index (P <0.001), and oral hygiene index (P=0.004) after controlling for age, gender, education, and monthly income.
Conclusion
This study found that high-income and healthy participants, non-smokers, and those who visited the dental office during the last one year demonstrated significantly higher SOC. In addition, there was a statistically significant correlation between SOC and oral health. These study findings highlight the importance of raising awareness about SOC to improve oral health outcomes in adult patients.
Introduction
Sense of Coherence (SOC) refers to a global orientation to one’s inner and outer environments which is hypothesized to be a significant determinant of location and movement on the health ease/disease continuum.Citation1 SOC is a health-promoting resource that enhances expectations for improved health, strengthens resilience, and develops and maintains a positive state of health.Citation2 This helps individuals cope with life stressors and enables them to perform healthy behaviors due to an increased sense of well-being.Citation3 Health promotion programs should include interventions to enhance SOC because individuals with high SOC perceive the world as more comprehensible, manageable, and meaningful, and are better equipped to use resources for better management of stressors.Citation4
Sense of Coherence is a determinant of oral health behavior such as tooth brushing, smoking, sugar consumption, and dental attendance.Citation3 Besides, it is also related to the oral-health-related quality of life and plays an important role in oral health promotion.Citation5 A study of Finnish adults by Bernabé et al reported a relationship between higher scores of SOC and improved oral health behaviors. The participants with increased SOC were more likely to visit the dentist for regular dental visits and brush their teeth twice daily, and they were less likely to consume sugar and smoke daily.Citation6
Researchers have investigated the relationship between SOC and oral health status.Citation7,Citation8 A previous study by Lindmark et al demonstrated that higher SOC scores were associated with lower plaque accumulation and periodontitis in the adult Swedish population.Citation7 In India, Shilpa et al reported a significant association between SOC and loss of attachment; however, no significant association was found between SOC and caries experience and plaque index.Citation8 On the contrary, a previous study failed to show that SOC could predict the incidence of periodontal disease in adults.Citation9 Hence, the literature on SOC and oral health shows conflicting results, highlighting the need for further exploration of this topic.
There is a lack of sufficient data regarding the sense of coherence and oral health in Middle Eastern countries, including Saudi Arabia. The study data may be used to inform the development of policies and programs to strengthen SOC to prevent and control oral diseases and improve quality of life. Therefore, the study aimed to assess the sense of coherence and its influences on oral health among adult patients attending the dental hospital College of Dentistry Imam Abdulrahman Bin Faisal University, Dammam. In addition, the study investigated the relationship of SOC with demographic factors.
Methods
Study Design and Sample
This cross-sectional study included adult patients who visited the dental hospital of the College of Dentistry Imam Abdulrahman Bin Faisal University (IAU), Dammam. The Institutional Review Board at the Deanship of Scientific Research IAU approved the study (IRB 2021–02-065). The study included adult patients (˃ 18 years) and those who provided written informed consent. Patients with psychological disorders, those who were mentally unstable, unable to complete a clinical oral examination, or taking some antipsychotic medications were excluded from the study. Sample size (N = 554) was calculated by using a 95% confidence level, 0.5 variability in population, ±5% margin of error (precision levels), and an approximate population (N= 10,000). A convenience sample of patients was used in the study. The researchers collected data from September 2022 till May 2023.
Procedures and Assessments
Clinical examination and questionnaire administration were carried out to measure study variables. The World Health Organization criteria were used to examine patients.Citation10 Oral health was measured by utilizing multiple indices, such as the DMFT (Decayed, Missing, Filled Teeth) index, the Simplified Oral Hygiene Index, the Plaque Index, and the Gingival Index. The DMFT index identified dental caries by examining the decayed teeth (D), missing teeth (M) due to caries, and filled teeth (F). DMFT index measures the prevalence and severity of dental caries and provides information on oral health status related to dental caries. The gingival index measures gingival health and looks for the presence or absence of gingival bleeding or inflammation. The plaque index was used to determine the severity and location of the soft debris that accumulates on the tooth surface due to poor oral health routines. A higher plaque index increases the risk of oral diseases due to poorer oral hygiene. The participant’s oral hygiene status was examined using the Simplified Oral Hygiene Index.Citation11 Six indexed teeth were used to measure plaque, gingival, and oral hygiene indices. Overall, DMFT, plaque, gingival and simplified oral hygiene indices provide a comprehensive evaluation of different aspects of oral health, including dental caries, plaque accumulation, gingival inflammation, and oral hygiene. To ensure the reliability of the clinical data, a training and calibration session was conducted. Inter-examiner consistency assessments were performed to get acceptable values (Kappa statistics > 0.70) before conducting the oral examination of study participants.Citation10
In addition to these clinical assessments, Antonovsky’s Sense of Coherence Scale (SOC-13) was used to measure the ability of people to cope with a stressful situation, and it consisted of 13 items rated on a 7-point Likert scale (always (1), very often (2), often (3), sometimes (4), rarely (5), seldom (6), never (7)).Citation1,Citation12 The SOC-13 instrument score ranges from 13 to 91, and a higher score indicates a stronger SOC.Citation13 The scale is reliable, valid, and cross-culturally applicable.Citation14 Both Arabic and English versions of SOC-13 were used among Arab and non-Arab study participants, respectively. The study also included participants’ responses about gender, nationality, education level, monthly family income, medical problems, smoking, and dental attendance. The self-administered questionnaire containing the SOC-13 scale and demographic information was pilot-tested before its final administration among study participants. A self-completion questionnaire was provided to the participants in the waiting area of the clinic. After returning the completed questionnaires to one of the researchers, the participants underwent an oral examination in dental hospital clinics. Ethical principles of the Declaration of Helsinki were followed during the study.
Statistical Analysis
Statistical analysis was conducted using SPSS (Statistical Package for the Social Sciences). Descriptive statistics (frequencies, proportions, means, and standard deviations) were used to summarize the demographic features of the research participants and each item of the SOC-13 scale. Inferential statistical approaches included bivariate and multivariable analyses to evaluate the relationship of the SOC with oral health. Non-parametric tests such as Mann–Whitney U, Kruskal–Wallis, and Spearman correlation tests were used in the study because the data did not follow a normal distribution. The Mann–Whitney U-test and the Kruskal–Wallis test were performed to investigate the relationship between SOC and study variables such as age, gender, family income, medical condition, smoking, and dental visits. The correlations between SOC and various oral health indices were assessed using Spearman correlation test. A significance level (alpha) of 0.05 was adopted to determine the statistical significance.
Results
The study included the data of 558 participants with a mean age of 32.19±10.11 years. The majority of participants were males (81.9%), Saudis (81.9%), and had a college/university education (63.1%). Cronbach’s α of SOC was 0.87, which reflects good internal consistency of the scale. The mean score of SOC was 52.77±13.11, which was significantly higher in high-income participants (P <0.001) compared with middle-income and low-income participants. Similarly, participants without medical conditions (P=0.021), non-smokers (P <0.001), and those who visited the dentist in less than one year (P=0.028) demonstrated significantly greater SOC ().
Table 1 Sense of Coherence (SOC) and Its Relationship with Study Variables Among Participants (N=558)
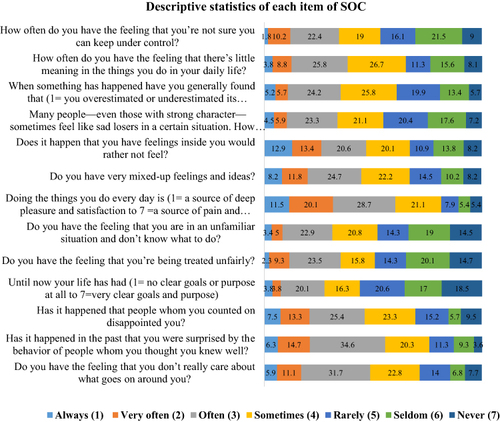
shows the descriptive statistics of each item of the SOC-13 Scale. Examining each item provides insight into the distribution of participants’ responses. Only 18.5% of participants reported that they had very clear goals and purpose in life. About one-third of participants (34.6%) reported that they were often surprised by the behaviour of someone they knew, 31.7% often did not care what went around them, and 24.7% often had very mixed feelings and ideas.
Figure 1 Distribution of participants’ responses about each item of SOC.
The study showed statistically significant negative correlations between SOC and DMFT index (P=0.002), SOC and plaque index (P <0.001), SOC and gingival index (P=0.002), and SOC and simplified oral hygiene index (P=0.001) (). Multivariable analysis shows that SOC significantly correlated with the DMFT index (P=0.001), plaque index (P <0.001), gingival index (P <0.001), and simplified oral hygiene index (P=0.004) after controlling for age, gender, education, and monthly income ().
Table 2 Bivariate Analysis: Correlation Between Sense of Coherence and Oral Health Indices Among Study Participants
Table 3 Multivariable Analysis: Relationship of Sense of Coherence with Oral Health Status Among Study Participants
Discussion
The present study evaluated the influence of the sense of coherence on oral health, smoking, dental visits, and general health. It was found that SOC significantly and negatively correlated with caries experience, emphasizing that greater SOC will result in reduced caries experience among adult patients. These findings are in line with the results of a study by Bernabé et al where Finnish adults with strong SOC exhibited a lower prevalence of caries and greater retention of teeth.Citation15 In another longitudinal study, Bernabé et al found that individuals in Finland with greater SOC had a significantly lower incidence of caries after adjusting for demographic factors.Citation16 According to a systematic review and meta-analysis of high quality studies, individuals with low scores of SOC have a greater likelihood of having high caries.Citation17 Wennström et al conducted a study on middle-aged women in Sweden, and reported a significant association between SOC and the number of teeth, demonstrating that low SOC was associated with more missing teeth.Citation18 On the contrary, in a recent study by Mathisen et al revealed no significant association between SOC and dental caries among general adults population in Norway.Citation19 Similar results were obtained in a study of preuniversity students (16–17 years), where authors showed no significant association between SOC and caries experience in India.Citation8 It is known that dental caries can eventually lead to tooth loss, therefore, having a strong SOC can predict low caries, which may result in a reduced number of missing teeth.
Furthermore, the present study found a significant negative relationship between SOC and plaque index, gingival index, and simplified oral hygiene index. These findings correspond to the results of previous studies related to SOC and oral health. Nagpal et al showed that adolescents with low SOC were at significantly greater risk (Relative Risk of 5.56) of gingival bleeding in India.Citation20 A study of Finnish adults by Savolainen et al reported that low SOC was independently and significantly related to a high score of plaque index, indicating poorer oral hygiene status.Citation21 However, Shilpa et al reported no significant relationship between SOC and plaque index among Indian students.Citation8 SOC is known as a strong predictor of oral health behaviours, which affect the oral health status of individuals,Citation22 and people with strong SOC exhibit better oral health behaviours and ultimately optimal oral health.Citation15
Our analysis showed that smokers had a significantly lower score of SOC compared to non-smokers, which corresponds with the results of a study by Bernabé et al who showed that higher levels of SOC were associated with lower odds of daily smoking after adjusting for demographic factors.Citation6 Similar findings of a strong relationship between higher SOC and non-smoking behaviour were reported by Peker et al.Citation23 Furthermore, in a study of hypertensive patients, Igna et al demonstrated a lower score of SOC among smokers.Citation24 Individuals with low levels of SOC are more likely to smoke because they may not be able to handle stressful situations, which may account for the association between low SOC and smoking behaviour.Citation3
In the present study, the participants who visited the dentist during the last year demonstrated significantly greater SOC than those who visited after a year. The role of SOC in the patterns of dental visits is supported by the results of a study by Freire et al who showed that participants with higher SOC frequently visited the dental office for routine dental check-ups.Citation25 On the other hand, studies by Mathisen et al and Lindmark et al did not find a significant association between SOC and regular dental appointments.Citation19,Citation26 Different patterns of dental visits and variations in the availability of oral health services in different countries may account for the observed differences in these results.
SOC, a health-promoting psychological resource, helps individuals cope with stresses in their environment, and individuals who belong to high socioeconomic status are known to have strong SOC.Citation9,Citation12,Citation18 Recently, the researchers reported that SOC was independently associated with income, indicating a higher SOC among high-income adults.Citation19 This is in line with the results of the present study, where participants with high income demonstrated significantly higher levels of SOC compared to those with low income. High income ensures the availability of financial resources to pay for basic needs and greater access to other resources such as social support, cultural stability, and preventive health orientation to mitigate psychological stresses, leading to strengthening SOC.Citation27,Citation28
It has been observed that there is a positive association between a strong SOC and subjective state of health and a negative association with the occurrence of disease.Citation29 In a recent longitudinal study, Dziuba et al reported long-term associations between SOC and self-reported health and physician-assessed health in Germany.Citation30 Previous studies have shown that high levels of SOC are associated with a low risk of mortalityCitation31 and lower odds of the onset of depressive symptoms.Citation32 In addition, there is a positive association between SOC and quality of life among patients with congenital heart diseases.Citation33 In accordance with the literature, the present study also found a significantly higher SOC among healthy participants compared with those with a medical problem.
Previous studies have investigated the association between age and SOC and provided conflicting results.Citation26,Citation34 Lindmark et al’s investigation revealed a lower mean SOC score in individuals aged 20–29 years compared to those within the 30–80 age range.Citation26 In contrast, Feldt et al found a higher mean score of SOC in participants over the age of 30 years than those under 30 years of age.Citation34 In the present study, no statistically significant difference in mean scores of SOC was observed between participants equal to or below 30 years of age and those above 30 years. These disparities could be attributed to variations in cultures, social support, life experiences, and coping abilities across study populations, in addition to differences in assessment methodologies.Citation22
Low SOC is related to poorer oral health, as demonstrated through negative correlations between oral health indices and SOC in our sample of patients. The study results may be used by dentists and other health professionals to enhance SOC among adult patients to promote oral health and achieve improved oral health outcomes. For example, the study results may suggest the need for targeted interventions to improve SOC in patients with low income, smoking habits, and a medical problem. Physical activity, healthy nutrition, mindfulness, social support and networking, and problem-solving skills can enhance SOC among these individuals, leading to optimal oral health.Citation35 In the present study, the participants with greater SOC showed reduced caries experience, improved gingival health, diminished plaque deposits, and better oral hygiene, and these individuals should maintain their activities and efforts to sustain high level of SOC and better oral health status.
The present study offers valuable data on the sense of coherence and oral health, utilizing a validated and reliable instrument and clinical examination of study variables. However, certain limitations to the study should be acknowledged. The use of a convenience sample and data collection from a university dental hospital may limit the generalizability of the study results. Additionally, the participants who conveniently participated in the study might have an inherently higher SOC, and this could limit the generalizability of the study findings. Therefore, care should be exercised when generalizing the results to other populations in different settings. The study did not collect information about smoking related factors such as types of smoking products, frequency of smoking, previous smoking status, etc., which may have an impact on SOC and eventually study results. Antonovsky developed the SOC scale based on the context of Western culture, and the scale may not capture cultural differences in how Saudi and non-Saudi participants perceive and handle stresses. Moreover, the cross-sectional study design is limited in establishing a cause-and-effect relationship; therefore, a temporal relationship between sense of coherence and oral health cannot be established. In the future, it is recommended that large longitudinal studies be undertaken to more effectively establish the impact of sense of coherence on the oral health of populations.
Conclusions
This study revealed that participants with higher income and good health, non-smokers, and those who had visited the dentist in the past year exhibited significantly higher SOC. Furthermore, a statistically significant negative correlation was observed between SOC and oral health, emphasizing that a higher SOC is related to improved oral health, such as reduced caries experience and improved gingival health and oral hygiene. These findings underscore the importance of establishing programs to enhance SOC and diagnosing oral diseases at early stages for positive oral health outcomes, including the reduction of oral complications.
Disclosure
The authors report no conflicts of interest in this work.
References
- Antonovsky A. The structure and properties of the sense of coherence scale. Soc sci med. 1993;36(6):725–733. doi:10.1016/0277-9536(93)90033-Z
- Eriksson M, Lindström B. Antonovsky’s sense of coherence scale and the relation with health: a systematic review. J Epidemiol Community Health. 2006;60(5):376–381. doi:10.1136/jech.2005.041616
- Elyasi M, Abreu LG, Badri P, et al. Impact of sense of coherence on oral health behaviors: a systematic review. PLoS One. 2015;10(8):e0133918. doi:10.1371/journal.pone.0133918
- Wainwright NW, Surtees PG, Welch AA, et al. Healthy lifestyle choices: could sense of coherence aid health promotion? J Epidemiol Community Health. 2007;61(10):871–876. doi:10.1136/jech.2006.056275
- Nammontri O, Robinson PG, Baker SR. Enhancing oral health via sense of coherence: a cluster-randomized trial. J Dent Res. 2013;92(1):26–31. doi:10.1177/0022034512459757
- Bernabé E, Kivimäki M, Tsakos G, et al. The relationship among sense of coherence, socio-economic status, and oral health-related behaviours among Finnish dentate adults. Eur J Oral Sci. 2009;117(4):413–418. doi:10.1111/j.1600-0722.2009.00655.x
- Lindmark U, Hakeberg M, Hugoson A. Sense of coherence and oral health status in an adult Swedish population. Acta Odontol Scand. 2011;69(1):12–20. doi:10.3109/00016357.2010.517553
- Shilpa M, Naik SP, Potdar S, et al. Sense of coherence and oral health status among 16 to 17-year-old preuniversity students of virajpet taluk: a cross-sectional study. J Contemp Dent Pract. 2016;17(5):388–393. doi:10.5005/jp-journals-10024-1860
- Kanhai J, Harrison VE, Suominen AL, et al. Sense of coherence and incidence of periodontal disease in adults. J Clin Periodontol. 2014;41(8):760–765. doi:10.1111/jcpe.12272
- World Health Organization. Oral health surveys: basic Methods: World Health Organization; 2013. Available from: https://www.who.int/publications/i/item/9789241548649. Accessed Nov 24, 2023.
- Malmo University. Methods and Indices; 2023. Available from: https://capp.mau.se/methods-and-indices/. Accessed July 8, 2024.
- Antonovsky A. Unraveling the mystery of health: how people manage stress and stay well. Joss Bass Google Schola. 1987;2:409–427.
- Stern B, Socan G, Rener-Sitar K, Kukec A, Zaletel-Kragelj L. Validation of the Slovenian version of short sense of coherence questionnaire (SOC-13) in multiple sclerosis patients. Zdr Varst. 2019;58(1):31–39.
- Eriksson M, Lindström B. Validity of Antonovsky’s sense of coherence scale: a systematic review. J Epidemiol Community Health. 2005;59(6):460–466. doi:10.1136/jech.2003.018085
- Bernabé E, Watt RG, Sheiham A, et al. Sense of coherence and oral health in dentate adults: findings from the Finnish Health 2000 survey. J Clin Periodontol. 2010;37(11):981–987. doi:10.1111/j.1600-051X.2010.01604.x
- Bernabé E, Newton JT, Uutela A, Aromaa A, Suominen AL. Sense of coherence and four-year caries incidence in Finnish adults. Caries Res. 2012;46(6):523–529. doi:10.1159/000341219
- Torres TAP, Corradi-Dias L, Oliveira PD, et al. Association between sense of coherence and dental caries: systematic review and meta-analysis. Health Promot Int. 2020;35(3):586–597. doi:10.1093/heapro/daz038
- Wennström A, Wide Boman U, Stenman U, Ahlqwist M, Hakeberg M. Oral health, sense of coherence and dental anxiety among middle-aged women. Acta Odontol Scand. 2013;71(1):256–262. doi:10.3109/00016357.2012.671362
- Mathisen KM, Holde GE, Torp S, Jönsson B. Sense of coherence in a general adult population in Northern Norway and its associations with oral health. BMC Oral Health. 2023;23(1):755. doi:10.1186/s12903-023-03430-z
- Nagpal R, Gupta A, Marya CM, Mushtaq I, Tandon S. Association of sense of coherence with oral health behaviors and gingival bleeding among adolescents. J Indian Soc Periodontol. 2021;25(2):150–155. doi:10.4103/jisp.jisp_165_20
- Savolainen JJ, Suominen-Taipale AL, Uutela AK, et al. Sense of coherence as a determinant of toothbrushing frequency and level of oral hygiene. J Periodontol. 2005;76(6):1006–1012. doi:10.1902/jop.2005.76.6.1006
- Poursalehi R, Najimi A, Tahani B. Effect of sense of coherence on oral health behavior and status: a systematic review and meta-analysis. J Educ Health Promot. 2021;10:361. doi:10.4103/jehp.jehp_1350_20
- Peker K, Bermek G, Uysal O. Factors related to sense of coherence among dental students at Istanbul University. J Dent Educ. 2012;76(6):774–782. doi:10.1002/j.0022-0337.2012.76.6.tb05313.x
- Igna CV, Julkunen J, Ahlström R. Sense of coherence relates with smoking. J Health Psychol. 2008;13(8):996–1001. doi:10.1177/1359105308097962
- Freire MC, Sheiham A, Hardy R. Adolescents’ sense of coherence, oral health status, and oral health-related behaviours. Oral Epidemiol. 2001;29(3):204–212. doi:10.1034/j.1600-0528.2001.290306.x
- Lindmark U, Stenström U, Gerdin EW, Hugoson A. The distribution of “sense of coherence” among Swedish adults: a quantitative cross-sectional population study. Scand J Public Health. 2010;38(1):1–8. doi:10.1177/1403494809351654
- Gupta E, Robinson PG, Marya CM, Baker SR. Oral Health Inequalities: relationships between Environmental and Individual Factors. J Dent Res. 2015;94(10):1362–1368. doi:10.1177/0022034515592880
- Antonovsky A. Unraveling the mystery of health: how people manage stress and stay well. San Francisco. 1987;1987:175.
- Suominen S, Helenius H, Blomberg H, Uutela A, Koskenvuo M. Sense of coherence as a predictor of subjective state of health: results of 4 years of follow-up of adults. J Psychosom Res. 2001;50(2):77–86. doi:10.1016/S0022-3999(00)00216-6
- Dziuba A, Krell-Roesch J, Schmidt SCE, Bös K, Woll A. Association between sense of coherence and health outcomes at 10 and 20 years follow-up: a population-based longitudinal study in Germany. Front Public Health. 2021;9:739394. doi:10.3389/fpubh.2021.739394
- Yamauchi K, Kato T, Saito I, Yamaizumi M. Relationship between mortality risk and health-related factors and sense of coherence in residents ofa rural area in Japan. J Rural Med. 2020;15(1):38–43. doi:10.2185/jrm.2019-001
- Ito M, Seo E, Maeno T, Ogawa R, Maeno T. Relationship between depression and stress coping ability among residents in Japan: a two-year longitudinal study. J Clin Med Res. 2018;10(9):715–721. doi:10.14740/jocmr3512w
- Moons P, Apers S, Kovacs AH, et al. Sense of coherence in adults with congenital heart disease in 15 countries: patient characteristics, cultural dimensions and quality of life. Eur J Cardiovasc Nurs. 2021;20(1):48–55. doi:10.1177/1474515120930496
- Feldt T, Lintula H, Suominen S, et al. Structural validity and temporal stability of the 13-item sense of coherence scale: prospective evidence from the population-based HeSSup study. Qual Life Res. 2007;16(3):483–493. doi:10.1007/s11136-006-9130-z
- Lindström B, Eriksson M. Contextualizing salutogenesis and Antonovsky in public health development. Health Promot Int. 2006;21(3):238–244. doi:10.1093/heapro/dal016