 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Introduction
Appropriate medical care seeking could prevent a significant number of child deaths and complications due to ill health. This study aims to determine factors affecting health seeking behavior (HSB) for childhood illnesses, thereby improving child survival.
Methods
A cross sectional study was carried out from January 11 to April 2, 2012. A total of 212 caretakers of children under the age of 5 years participated. Caretakers who visited the vaccination unit in the Shehair Health Center during the study period and had a child with a history of diarrhea, fever, cough, and/or difficulty of breathing during the last 14 days were included. The data were collected by interviewing caretakers and the answers were reported in pretested structured questionnaires.
Results
Medical care was sought for about half of the sick children (n=109, 51.42%). Seeking medical care was frequently initiated for illnesses that did not improve or worsened. The major reasons for not seeking medical care were “illness was mild” (n=40, 38.83%) and “illness is not for medical treatment” (n=32, 31.07%). The caretakers sought medical care significantly more when they had a higher level of school education (POR [prevalence odds ratio] 5.85, 95% CI [confidence interval]: 2.34–14.61), when the illness was perceived as severe (POR 5.39, 95% CI: 2.81–10.33), and when the child had difficulty of breathing (POR 2.93, 95% CI: 1.10–7.80).
Conclusion
For the preventable childhood illnesses with existing interventions, appropriate HSB prevalence is low. Symptom type, caretakers’ education, and perception of illness severity are the predictors of HSB. Educational improvement of the mothers, introduction of community based integrated management of childhood illness, and in-depth research are imperative to improve mothers’ HSB.
Introduction
Children represent the most vulnerable age group in any community; therefore, the child mortality rate is widely used as a demographic measure and an important indicator of the level of welfare in countries.Citation1
About 7 million children worldwide under the age of 5 years died in 2011. More than half of these deaths were due to preventable conditions where access to simple and affordable interventions was possible. Leading causes of death were pneumonia, preterm birth complications, diarrhea, birth asphyxia, and malaria.Citation2 Undernutrition contributed to more than a third of these deaths.Citation3
Overall, considerable progress has been made towards achieving Millennium Development Goal 4. Since 1990, the global under-5-year-old mortality rate (U5MR) has dropped from 87 deaths per 1,000 live births in 1990 to 51 deaths per 1,000 live births in 2011. But the rate of this reduction is still insufficient to reach the target of a two-thirds reduction of 1990 mortality levels by the year 2015.Citation2
However, success in reducing childhood mortality needs more than the availability of adequate health services with well-trained health professionals. As families are the first people responsible for child care, success requires a partnership between health workers and families with community support.Citation4
Epidemiologists and social scientists have focused their attention on studying the relationship between childhood illnesses and health seeking behavior (HSB).Citation5 Health or care seeking behavior has been defined as any action taken by someone in order to find an appropriate remedy for themselves or for the person whom they take care of, when they have a health problem or illness.Citation6
In some low-income settings, child health and survival was improved when parents selected qualified medical care providers rather than nonqualified ones.Citation7
Generally, there is a growing amount of literature on HSB and the predictors of health services utilization, especially in developing countries.Citation8 Unfortunately, HSB studies often describe patterns of behavior without clarifying causes for that behavior, thereby failing to give valuable recommendations.Citation9
Reviews of the global literature suggested that factors affecting HSB could be classified as cultural beliefs, sociode-mographic status, women’s autonomy, economic conditions, physical and financial accessibility, disease pattern, and health service issues.Citation8,Citation10–Citation14 But, in developing countries, cultural practices and beliefs were the most prevalent.Citation8 Cultural practices are prevalent in Yemen; these include massage, cauterization, and local herbal preparations. In addition, many people think that herbs are always useful and are never harmful (Bamatraf, unpublished data, 2008).
Unfortunately, no published quantitative studies have been found regarding the predictors of HSB for children in Yemen. In the last Yemen Family Health Survey (YFHS), data indicated that no medical care was sought for 53% and 61% of the children under five years of age with respiratory symptoms and diarrhea, respectively.Citation15 Another Yemeni study described HSB for children with diarrhea but did not quantitatively determine its predictors (Bamatraf, unpublished data, 2008).
U5MR in Yemen is one of the highest in the Middle East. The World Health Organization reported it as being 77/1,000 live births, with the average regional and global rate as 68 and 57/1,000, respectively, in 2012. Apart from neonatal fatal conditions, pneumonia, followed by diarrhea, was the most frequent cause of death.Citation16
This study therefore aims to determine the factors affecting HSB of caretakers when their children under the age of 5 years are suffering from common childhood illnesses such as diarrhea, fever, cough, and difficulty of breathing (DOB). Therefore, this study enables one to understand how to influence caretakers’ behavior by a rational policy in order to promote child health. The objectives of the current study are to describe the caretakers’ HSB, identify the rationale of HSB, and determine the relationship of HSB with subject, disorder, and service characteristics.
Methods
Study design
The study was carried out in Shehair city, which is an ancient city in Hadhramout Governorate, Yemen. It is classified as an urban city.Citation17 It is located on the Arabian Sea coast, about 36 km from Almukalla (the capital of Hadhramout Governorate). The population was estimated to be 11,196 in 2011. The study was cross sectional.
Participants
The study targeted caretakers of children under the age of 5 years. The caretakers of children under 5 years of age with a history of diarrhea, fever, cough, and/or DOB during the preceding 14 days were included. Caretakers that had problems that might have affected the reliability of the questionnaire scores and those who refused to participate in the study were excluded.
Sample
All caretakers who met the inclusion criteria and visited the vaccination unit in Shehair Health Center (SHC) from January 11, 2012 were conveniently included until the required sample was completed by April 2, 2012. The total number of participants was 212 caretakers.
The required sample size was calculated from the prevalence of HSB in literature. The following formula was used to calculate sample size:
where z is the z score (1.96 for 95% confidence level), p is the percentage picking a choice (it is substituted at 0.53 [avoiding seeking medical care in YFHS]),Citation15 c is the proportion of error we are prepared to accept (the current study set <0.07), and the required minimum sample size was 195. Five percent was added for the possibility of nonresponse, so the minimum sample size became 205 caretakers.
Study variables
There are many models for studying care seeking behaviors. Kroeger’s sociobehavioral model covers the major dimensions of HSB.Citation18 It is comprehensive and well-organized, so it enables the establishment of correlations with good predictability.Citation19 This study depended on Kroeger’s model in addition to the literature review in determining the study variables. shows the study variables.
Figure 1 Factors affecting HSB for common childhood illnesses; study variables.
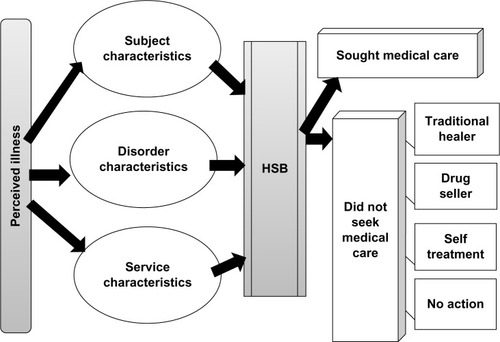
Subject characteristics of the caretakers and children. Caretakers’ data include age, marital status, education, occupation, and address. Children’s data are age, sex, number of siblings, and child birth order. Disorder characteristics mean the severity and symptom type, ie, fever, diarrhea, cough, and/or DOB. Service characteristics include accessibility, acceptability, attitude towards traditional and modern medicine, quality of medical care, and affordability of medical care cost.
Sought medical care means consulted a qualified medical professional. Traditional healers are nonqualified persons who treat the sick children using traditional nonmedical methods such as massage, herbs, and cauterization. Drug sellers are nonqualified persons who sell drugs without medical prescription.
For inferential statistics, the caretakers’ age and the number of siblings were classified into two categories according to the mean. The educational level was categorized according to the level of school education.Citation20
Similarly, respondents’ addresses were classified to three levels, one, two, and three, according to the geographic range and catchment area of the health facility for immunization activity (EPI-Program, unpublished data, 2011). Level two and three were merged into one category to avoid empty cells. Children were classified into infants and older. The birth order was divided into two categories based on the median.
Perception of severity of child illness was reported according to assessment using the caretakers’ subjective evaluation. Diarrhea was defined as watery stools that occurred more than three times during any 24-hour period.Citation21 DOB was defined as caretaker’s perception of breathing as rapid and/or difficult.Citation18 Cough was defined as a continuous cough.Citation18 Fever was reported according to the caretakers’ subjective evaluation.
Data collection
The data was collected by interviewing the respondents in SHC using a structured questionnaire formulated by the researcher and written in Arabic. A female community health worker was trained to assist in interviews. She was a native of the community and was deliberately chosen from the community to facilitate the flow of information.
The interviews were conducted in Arabic (Yemeni accent). The questionnaire covered the study objectives and variables and had five parts: subject characteristics; disorder characteristics; HSB patterns; HSB rationale; and services characteristics.
The questionnaire was validated by two steps. Firstly, a pilot survey of 30 caretakers from the target population was conducted before the beginning of data collection. The pilot survey questionnaires were not included in the study because the questionnaire was modified in the light of the study findings. Secondly, five academic members of staff were asked to review the draft questionnaire. Most of them had conducted a study on HSB previously.
Data analysis
The data were coded, checked, and processed with version 20 Statistical Package for the Social Sciences (SPSS; IBM Corporation, Armonk, NY, USA). Summary statistics, such as means, standard deviations (SD), frequencies, and proportions, were used to summarize variables. Chi-square tests were used to identify associations between categorical variables with P-value <0.05 as the significance level. Logistic regression analysis was conducted to determine significant predictors of outcomes with estimation of the POR (prevalence odds ratio) and 95% CI (confidence interval).
The Department of Family Medicine in Hadhramout University reviewed and approved the study protocol. A simple and clear explanation of the research aims and procedure was provided to the SHC manager and the staff involved in the study. Informed consents were obtained verbally from the manager and the staff who were included in the study. They were given feedback about the results of the study. Similarly, verbal consents were obtained from all of the caretakers who participated in the interviews. Respondents’ privacy and confidentiality were assured.
Results
Demographic characteristics
All caretakers were adults with a mean age of 28 years (SD ± 6). Age ranged from 18 to 45 years. Most of the caretakers were the mothers (98.58%) while the remaining 1.42% were grandmothers and aunts. Regarding the age of children, the mean was 18 months (SD ± 17) and it ranged from 10 days to 59 months. The median number of siblings was two; it ranged from 1 to 9. shows the demographic characteristics of caretakers and children. The most common reported symptom was fever (76.89%), followed by cough (35.85%), diarrhea (29.25%), and DOB (13.68%). Around 58% of the respondents (122) perceived their children’s illnesses as severe.
Table 1 Frequency distribution of caretakers and their sick children by demographic characteristics
Description of HSB
Out of 212 sick children, 109 (51.42%) sought medical care, while 21 (9.91%) caretakers did nothing in response to illnesses (). The mean duration before seeking medical care was 3 days (SD ± 2). Of the total number of medically treated children, care was sought on the first day of perceived onset of illness for only 19 subjects (17.43%). Although “sought medical care” was the most common pattern of HSB, it was the first action for only 56 (26.42%) of respondents. The most common first action was “purchased drugs” ().
Figure 2 Caretakers’ distribution by the source of care.
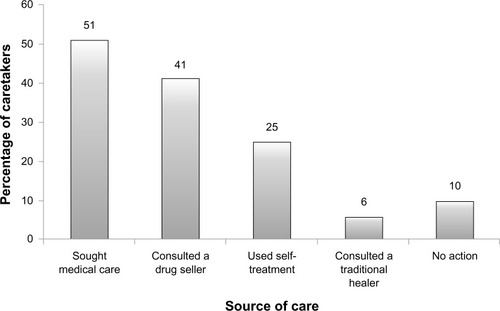
Table 2 Distribution of caretakers by the order of action
Decision was made by both parents for 75 (35.38%) children. Sixty two (29.25%) of the respondents stated that the decision was taken by the mother alone.
Rationale of HSB
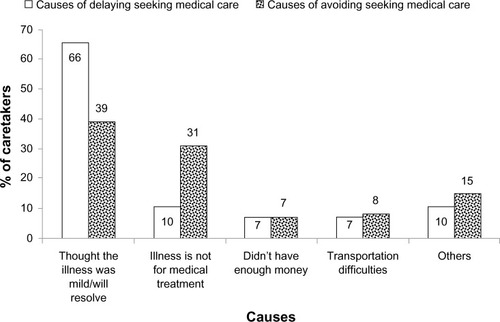
For those who did not seek medical care, the main reason was stated as being “illness was mild” (n=40, 38.83%), and the next most common cause was “illness is not for medical treatment” (n=32, 31.07%). The main reason for delaying seeking medical care for more than 3 days was “thought the illness was mild/will resolve” (66.32%) ().
Figure 3 Causes of delaying and avoiding seeking medical care.
Relationship of HSB with subject, disorder, and service characteristics
Regarding service characteristics, there was no statistically significant relationship between any of the services characteristics included in the questionnaire and HSB as P-values for all of them were >0.05 using Chi-square test. The respondents who agreed that the medical care cost was affordable sought medical care more frequently. For medical services acceptability and attitude towards modern medicine, it was impossible to find the correlation as all the respondents answered with “Yes.”
shows the associations between HSB with subject and disorder characteristics. According to the bivariate analysis, significant associations were observed between HSB and the educational level of caretakers (P=0.003), the presence of cough (P=0.047), having DOB (P=0.005), and illness perception (P<0.001). According to logistic regression analysis, caretakers with secondary school education were six times more likely to seek medical care than noneducated ones (POR =5.85, 95% CI: 2.34–14.61). Perceiving illnesses as severe was five times more likely to be associated with medical care seeking as compared to not severe (POR =5.39, 95% CI: 2.81–10.33). For those who had DOB, the caretakers were three times more likely to seek medical help than those who did not (POR =2.93, 95% CI: 1.10–7.80). Cough is no longer significant after adjustment of other variables using logistic regression analysis.
Table 3 Relationship between HSB and subject and disorder characteristics
Discussion
In studying HSB in Shehair city, the current study found that 51.42% of the respondents sought medical care, this being the most frequent action.
YFHS and other studies similarly showed that around half of the respondents sought medical care.Citation5,Citation22 Better results and higher rates of medical care seeking were reported in some countries,Citation23–Citation28 while others showed lower rates.Citation24,Citation29,Citation30
Variation in HSB could be attributed to differences in cultural and demographic features of the samples, because most of these studies are not based on national or regional samples. In addition, the spectrum of the illness used differed between some of the studies.
The least frequent action was consulting traditional healers followed by self-treatment. In the study in Almukalla, Yemen, consulting traditional healers was the most frequent action (Bamatraf, unpublished data, 2008). That study included diarrhea only, which was experienced by less than one third of the children in the current study. Promtussananon and PeltzerCitation31 concluded that most mothers used home remedies for the treatment of diarrhea and modern drugs for the treatment of fever and cough, which might explain the differences between these studies in Yemen.
Although seeking medical care was the most frequent HSB pattern in this study, it was not usually done as the first choice. The most frequent first response was purchasing over-the-counter drugs. Bamatraf (unpublished data, 2008), and a study in South Africa, found that treatment by home remedies was the most frequent first action by caretakers for children with diarrhea.Citation31
Mothers were the caretakers for nearly all the children and participated in decision making in more than 60% of cases, which corresponds with the study in Almukalla (Bamatraf, unpublished data, 2008). For most of the people in developing countries, and particularly for children, the type of treatment during illness cases is mainly decided by family members, especially the mothers.Citation1 Low decision-making power of women impacted negatively on HSB in the study areas.Citation32
Actually, it is difficult to determine the most appropriate time to take the sick child to medical providers because this depends on the illness itself, the health status of the child, the caretaker, and so forth; but, with no doubt, delay is not acceptable, especially in a country with a high U5MR like Yemen.
Uncomplicated illnesses could be managed at home, but severe illnesses should be treated by appropriate health providers without delay.Citation33 The current study documented that 122 caretakers perceived the illnesses as severe, but only 19 of them took their children for medical care during the first day of illness. Other studies similarly recorded some delay in medical care seeking.Citation22,Citation32,Citation34 In a Nepalese study, about 43% of those who sought medical advice did so within 24 hours.Citation29
Delay in care-seeking by caregivers contributes to the large number of child deaths in developing countries.Citation35 Factors such as pluralistic care-seeking practices, and the inability to recognize potentially life-threatening conditions, were found to be associated with the delay.Citation7 This delay could affect child health significantly and can lead to complications that make the medical care less effective and, in some cases, useless.
In 2008, Bamatraf stated that most of the children with diarrhea were taken to medical care only after home treatments and those of traditional healers failed (Bamatraf, unpublished data, 2008). During that time a child may become severely dehydrated. For that reason, it is very important to address and deal with the causes of delay.
In reviewing literature, studies rarely discussed the rationale of delayed medical care despite the fact that many mentioned the duration of illness before care seeking. Some studies have documented a popular belief that a patient has to be very ill to warrant taking him or her to the hospital as well as the reliance on traditional healers and the preference for trying self-medication prior to consulting medical professionals.Citation32
The main reason for not seeking medical care in the current study was “The illness was mild.” This is in agreement with several other studies.Citation15,Citation25,Citation36 The next common reason was “Illness is not for medical treatment.”Citation37 This pointed to the traditional illness concepts of childhood symptoms, which are believed to be a result of nonmedical mechanisms and preferably treated by traditional healers or home remedies.Citation38
A study in Burkina Faso showed that local illness concepts about manifestations of severe malaria in Africa were associated with avoidance or significant delay of effective biomedical treatment. Thus, they recommended considering these concepts when developing specific educational messages within national malaria control programs.Citation38
The findings of the current study are an indication that households seem to have shifted from making use of professional medical services as a trusted source of care to, instead, taking it as the last solution after trying other trusted methods. The situation here is dangerous for the general health of the population and, therefore, must be corrected.
AshornCitation1 in his study in Malawi found the variables that describe the type of the first treatment to be statistically significantly associated with childhood mortality. On the other hand, the analysis of the second treatment brought considerably fewer statistically significant relationships with childhood mortality.
Considering the factors affecting HSB, several studies have reported a positive relationship between maternal education and HSB, which is in agreement with the present study.Citation24,Citation27,Citation29,Citation30,Citation39,Citation40 Millennium Development Goals’ last report stated that, within countries, child mortality is higher in rural areas and among poorer and less educated families.Citation20
This study shows that caretakers with secondary school education were six times more likely to seek medical care than noneducated ones. This implies that the higher the level of school education, the better HSB. School education increases the mother’s knowledge about biological aspects of human beings, common health problems, and healthy habits as these are included in standard school curricula. Also, educated mothers are more likely to be able to read comprehensibly and thereby understand better. They are expected to understand health education messages presented in mass media and through other methods more than the less-educated ones. Other subject characteristics listed in the results were insignificant.
Regarding disorder characteristics, caretakers were more likely to seek medical treatment when a child experienced DOB. YFHS and another two studies reported similar findings.Citation15,Citation18,Citation31 This finding differs to that which Mbagaya and OdhiamboCitation30 and Taffa and ChepngenoCitation41 found among Kenyan mothers, who were much more likely to seek out a medical care provider when a child experienced fever and gastrointestinal symptoms than when suffering from respiratory symptoms.
These studies included a wider range of respiratory symptoms. Usually, little or no action is taken for upper respiratory symptoms because it is assumed they will heal in their own time.Citation30 Those studies were done in Kenya, so another explanation is that both the identification of and response to illnesses are closely linked to cultural beliefs.Citation1
Perceiving the illness as severe was strongly associated with seeking medical care in the current study. Many studies found it to be one of the main predictors of HSB.Citation1,Citation5,Citation24,Citation29,Citation36,Citation39 It has been maintained that, in general, people use first what is most easily available to them, but in cases of serious illnesses they are willing to make a greater effort in order to try something better.Citation1
None of the service characteristics significantly predicted HSB in this study, although mothers who could afford the cost of care sought medical care more frequently than others.
When comparing this finding with those of other published studies, many did not consider services characteristics, and others have contrasting results. Several studies reported distance from medical care facility, poor facilities, or inability to afford medical care cost as factors affecting HSB.Citation8,Citation27,Citation30,Citation32,Citation42,Citation43
Disagreement between studies regarding the significance of service characteristics could be explained by the sample differences, for example, studies in which samples were selected from large areas with a population of different characteristics, variable distances from health facilities, and multiple health service options would be more likely to prove the significance of association.
It is important to understand the limitations of the current study. It is known that the community based survey is a better choice for sampling in a study like this, but it requires team work and financial support that is beyond the scope of a study done by two researchers. Visitors of SHC vaccination unit were selected because all of them had children under 5 years old and were not coming for illnesses to gain medical care but for vaccination. Another point is that the vaccination coverage in SHC is more than 90%, which indicates that women come from almost all areas of Shehair, rendering the sample more representative.
There was a possibility of inaccurate responses regarding the disease characteristics as this largely depends on recall. The study included illnesses within 14 days before the interview to minimize the recall bias.Citation5,Citation26,Citation29,Citation40,Citation43
Furthermore, the present study did not address in depth the health and illness beliefs. To explore HSB of a population in depth, it needs a qualitative or mixed study with a team including anthropologists and/or social scientists to conduct ethnographic research. This is not available for the time being. The current study is an observational study. It could not prove any causal relationship between HSB and the factors affecting it.
In conclusion, for the preventable childhood illnesses with the existing interventions, appropriate HSB prevalence is low. Caretakers’ education, symptom type, and perception of illness severity are the predictors of HSB.
Educational improvement of mothers is recommended. We place emphasis on literacy programs because around 27% of the respondents had no school education. Messages in the mass media about the importance of schooling are mandatory. Further research to explore the barriers of school education are expected to help in solving the problem. Introduction of community-based Integrated Management of Childhood Illness programs could facilitate behavior change. Formal and nonformal medical care options have great potential for successful implementation to improve child health and should be explored by health policies. Local illness concepts could be explored and used effectively as a part of care seeking interventions as this is found to be one of the main causes of avoiding and delaying seeking medical care. In-depth research is imperative to visualize the real picture of the habits and practices of the people of our country, and to establish the causation of inappropriate HSB. More challenging would be the translation of research into policy and action.
Acknowledgments
This paper is based on a Masters thesis at Hadhramout University of Science and Technology. We thank the referees of the thesis, Dr Mosleh Ismail and Professor Abdullhakeem Lardhi, for their constructive comments. The authors are gratefully indebted to mothers and SHC’s staff who participated in and supported the study interviews. We additionally would like to thank Dr Fouziya Bamatraf, Dr Chandrashekhar Sreeramareddy, Dr Diana Sacke, and Anne-Laure Page for their helpful comments on the study methodology. We are thankful to the editor Dr Johnny Chen and the reviewers for insightful comments on the previous version of this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
- AshornUChild health-seeking in Lungwena, Malawi [academic dissertation]TampereUniversity of Tampere2003
- Children: reducing mortality [webpage on the internet]GenevaWorld Health Organization2012 Available from: http://www.who.int/mediacentre/factsheets/fs178/en/index.htmlAccessed October 12, 2012
- JohanssonEWCarvajalLNewbyHYoungMPneumonia and Diarrhoea: Tackling the Deadliest Diseases for the World’s Poorest ChildrenNew YorkUNICEF2012 Available from: http://www.unicef.org/media/files/UNICEF_P_D_complete_0604.pdfAccessed December 27, 2012
- Child health in the community – “Community IMCI”: briefing package for facilitators [webpage on the internet]GenevaWorld Health Organization2004 Available from: http://www.who.int/maternal_child_adolescent/documents/9241591951/en/index.htmlAccessed June 29, 2012
- GoldmanNHeuvelinePHealth-seeking behaviour for child illness in GuatemalaTrop Med Int Health20015214515510747275
- OlenjaJEditorial Health seeking behaviour in contextEast Afr Med J2003802616216167716
- D’SouzaRMRole of health-seeking behaviour in child mortality in the slums of Karachi, PakistanJ Biosoc Sci200335113114412537161
- ShaikhBTHatcherJHealth seeking behaviour and health service utilization in Pakistan: challenging the policy makersJ Public Health (Oxf)2005271495415590705
- GrundyJAnnearPHealth-Seeking Behaviour Studies: a Literature Review of Study Design and Methods with a Focus on CambodiaAustraliaUniversity of Melbourne, The Nossal Institute for Global Health201077 Available from: http://ni.unimelb.edu.au/__data/assets/pdf_file/0011/385967/HPHF_Hub_WP7_Health_Seeking_Behaviour.pdfAccessed June 11, 2012
- KatungPYSocio-economic factors responsible for poor utilization of PHC services in rural community in NigeriaNiger J Med200110282911705051
- NavaneethamKDharmalingamAUtilization of maternal health care services in Southern IndiaSoc Sci Med2002551849186912383469
- FatimiZAvanIDemographic, Socio-economic and Environmental determinants of utilization of antenatal care in rural setting of Sindh, PakistanJ Pak Med Assoc20025213814212174476
- UchudiJMCovariates of child mortality in Mail: does the health seeking behavior of the mother matter?J Biosoc Sci200133335411316394
- StephensonRHenninkMBarriers to family planning service use among the urban poor in PakistanAsia Pac Popul J200419526
- League of Arab States Republic of Yemen Ministry of Health and PopulationYemen Family Health Survey Principal ReportSanaaCentral Statistical Organization (CSO)2004
- Data from the Global Health Observatory: Country health profile [webpage on the internet]GenevaWorld Health Organization2013 Available from: http://www.who.int/gho/countries/yem.pdfAccessed May 21, 2012
- Social Fund for Development: Programming UnitEducational SurveyYemenMinistry of Education2008
- SakisakaKJimbaMHanadaKChanging poor mothers’ care-seeking behaviors in response to childhood illness: findings from a cross-sectional study in Granada, NicaraguaBMC Int Health Hum Rights20101011020515485
- Hausmann-MuelaSRiberaJMNyamongoIHealth-Seeking Behavior and the Health System Response: Disease Control Priorities Project8200337 DCPP Working Paper No 14. Available from: http://dcp2.org/file/29/wp14.pdfAccessed April 15, 2012
- Inter-Agency and Expert Group on MDG IndicatorsThe Millennium Development Goals Report 2012New YorkUnited Nations2012 Available from: www.undp.org/content/dam/undp/library/MDG/english/The_MDG_Report_2012.pdfAccessed December 24, 2012
- Diarrheal Disease [webpage on the internet]GenevaWorld Health Organization Available from: http://www.who.int/mediacentre/factsheets/fs330/en/index.htmlAccessed April 27, 2012
- AssefaTBelachewTTegegnADeribewAMothers’ health care seeking behaviour for childhood illnesses in Derra District, North-shoa Zone, Oromia Regional State, EthiopiaEthiop J Health Sci20081838794
- NdugwaRPZuluEMChild morbidity and care-seeking in Nairobi slum settlements: the role of environmental and socio-economic factorsJ Child Health Care200812431432819052189
- AbdulraheemISParakoyiDBFactors affecting mothers’ healthcare-seeking behaviour for childhood illnesses in a rural Nigerian settingEarly Child Dev Care20091795671683
- PageALHustacheSLuqueroFJDjiboAManzoMLGraisRFHealth care seeking behavior for diarrhea in children under 5 in rural Niger: results of a cross-sectional surveyBMC Public Health20111138921612640
- MotlaghMEHeidarzadehAHashemianHDosstdarMPatterns of Care Seeking During Episodes of Childhood Diarrhea and its Relation to Preventive Care Patterns: National Integrated Monitoring and Evaluation Survey (IMES) of Family Health. Islamic Republic of IranInt J Prev Med201231606722355479
- GaoWDangSYanHWangDCare-seeking pattern for diarrhea among children under 36 months old in Rural Western ChinaPLOS One201278e4310322912799
- Global health observatory: Care seeking for pneumonia: situation and trends [webpage on the internet]GenevaWorld Health Organization Available from: http://www.who.int/gho/child_health/prevention/pneumonia_text/en/index.htmlAccessed July 12, 2012
- SreeramareddyCTShankarRPSreekumaranBVSubbaSHJoshiHSRamachandranUCare seeking behaviour for childhood illness-a questionnaire survey in western NepalBMC Int Health Hum Rights20066716719911
- MbagayaGMOdhiamboMOOniang’oRKMother’s health seeking behaviour during child illness in a rural western Kenya communityAfr Health Sci20075432232716615844
- PromtussananonSPeltzerKHealth care-seeking behaviour for child illnesses among rural mothers in South Africa: a pilot studyHealth SA Gesondheid200382
- MazzilliCDavisAHealth Care Seeking Behaviour in Somalia – A Literature ReviewSomaliaUNICEF and the European Union200952 Available from: www.unicef.org/somalia/SOM_HealthcareseekingbehaviourReport_10-WEB.pdfAccessed March 2, 2012
- FujinoYSasakiSIgarashiKImprovement in mothers’ immediate care-seeking behaviors for children’s danger signs through a community-based intervention in Lusaka, ZambiaTohoku J Exp Med20092171738519155611
- NajninNBennettCMLubySPInequalities in Care-seeking for Febrile Illness of Under-five Children in Urban Dhaka, BangladeshJ Health Popul Nutr201129552353122106759
- KällanderKHildenwallHWaiswaPGaliwangoEPetersonSPariyoGDelayed care seeking for fatal pneumonia in children aged under five years in Uganda: a case-series studyBull World Health Organ200886533233818545734
- Amuyunzu-NyamongoMNyamongoIKHealth seeking behaviour of mothers of under-five-year-old children in the slum communities of Nairobi, KenyaAnthropol Med20061312540
- HillZKendallCArthurPKirkwoodBAdjeiERecognizing childhood illnesses and their traditional explanations: exploring options for care-seeking interventions in the context of the IMCI strategy in rural GhanaTrop Med Int Health20038766867612828551
- BeiersmannCSanouAWladarschEDe AllegriMKouyatéBMullerOMalaria in rural Burkina Faso: local illness concepts, patterns of traditional treatment and influence on health-seeking behaviourMalar J2007610617686147
- HongTKDibleyMJTuanTFactors affecting utilization of health care services by mothers of children ill with diarrhea in rural VietnamSoutheast Asian J Trop Med Public Health200334118719812971534
- AminRShahNMBeckerSSocioeconomic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: A cross-sectional analysisInt J Equity Health20109920361875
- TaffaNChepngenoGDeterminants of health care seeking for childhood illnesses in Nairobi slumsTrop Med Int Health200510324024515730508
- FeikinDRNguyenLMAdazuKThe impact of distance of residence from a peripheral health facility on pediatric health utilisation in rural western KenyaTrop Med Int Health2009141546119021892
- EwingVLLallooDGPhiriKSRoca-FeltrerAManghamLJSanJoaquinMASeasonal and geographic differences in treatment-seeking and household cost of febrile illness among children in MalawiMalar J2011103221303538