
Abstract
Background
Inhaled antibiotics (ABs) are recommended for use in the therapy of chronic Pseudomonas aeruginosa infection in patients with cystic fibrosis (CF). The aim of this systematic literature review was to identify level of adherence to inhaled ABs and to determine predictors and consequences of nonadherence in CF.
Methods
A systematic literature search of English-language articles was conducted in April 2015 using Medline and Embase. No publication date limit was applied. The literature screening was conducted by two independent reviewers. All of the included studies were assessed for quality.
Results
The search yielded 193 publications, of which ten met the inclusion criteria and underwent data extraction. Seven studies focused on inhaled tobramycin, one on inhaled colistimethate, one on inhaled levofloxacin, and one on inhaled aztreonam lysine. Medication adherence to inhaled ABs was analyzed by pharmacy refill history, daily phone diary, parent and child self-reports, vials counting, or electronic monitoring. In randomized controlled trials (n=3), proportion of adherent patients (>75%–80% of required doses taken) ranged from 86% to 97%; in prospective cohort studies (n=3), adherence rates ranged between 36% and 92%, and in retrospective studies (n=4) it ranged between 60% and 70%. The adherence to inhaled ABs in CF was found to be associated with the complexity of treatment, time of drug administration, age of patients, treatment burden (adverse events, taste), and patient satisfaction.
Conclusion
The high diversity of adherence data was because of the different study designs (randomized controlled trials vs real-world studies) and the lack of a commonly accepted consensus on the definition of adherence in the reviewed articles. Routine adherence monitoring during CF care, discussing the possible reasons of suboptimal adherence with the patient, and changing treatment regimens on the basis of patient burden can individualize CF therapy for patients and may improve the level of adherence.
Introduction
Cystic fibrosis (CF) is an inherited disease that affects particularly the lungs, pancreas, hepatobiliar system, reproductive tract, and sweat glands.Citation1,Citation2 It is caused by mutations in the gene encoding the CF transmembrane conductance regulator protein.Citation1,Citation2
Chronic infection with Pseudomonas aeruginosa (PA) impacts the progress of lung disease, which determines the life expectancy in CF. PA is one of the most common gram-negative bacteria causing acute exacerbation and progress of the lung disease in CF.Citation3 In the management of lung infection with PA, inhaled antibiotic (AB) therapy is recommended as maintenance therapy.Citation4 Aerosol delivery of ABs yields high concentration directly to the airways, where the bacterium persists while minimizing systemic exposure and toxicity.Citation5–Citation7 Colistimethate inhalation has been widely used in Europe, while current CF guidelines recommend chronic use of tobramycin inhalation solution (TIS) in the USA to improve lung function and to decrease exacerbations in chronic PA infection.Citation8 Use of inhaled aztreonam was approved by the US Food and Drug Administration in December 2009, and efficacy of inhaled levofloxacin has been studied in a clinical Phase III trial for chronic PA infection in CF patients.Citation9,Citation10
Medication adherence (compliance) “refers to the act of conforming to the recommendations made by the provider with respect of timing, dosage, and frequency of medication taking”.Citation11 In chronic diseases, such as in CF, medication nonadherence poses a significant barrier to optimal disease management. The daily therapy of CF, including chest physiotherapy, numerous oral and inhaled medications, nutritional supplements, and vitamins, involves a complex and time-consuming regimen for the patient,Citation12 which may be a significant predictor of nonadherence. In CF, previous studies reported somewhat higher adherence than for other chronic diseases (eg, asthma and allergic rhinitis).Citation12–Citation15 However, adherence is therapy-specific, and adherence rates may vary widely between different CF-related therapies. As it was identified in a cross-sectional study, higher treatment adherence to both respiratory (62%) and digestive treatment (88%), and lower adherence to physiotherapy (41%) and nutritional supplements (59%) were observed.Citation16
Although many studies evaluated adherence to CF-related medications, only few of those investigated adherence to inhaled ABs.Citation12,Citation13,Citation17 Nevertheless, evidence on prevalence and predictors of nonadherence to inhaled ABs would be highly valuable to the development of effective adherence-enhancing interventions and to improve disease management of CF patients with chronic PA infection. Therefore, the aim of this systemic review was to identify level of adherence to inhaled ABs for chronic PA infection in CF and to determine the possible predictors and consequences of nonadherence on the basis of the existing publications. To our knowledge, no systematic review encompassing this topic has been published to date.
Materials and methods
A systematic literature search of English-language articles was conducted in April 2015 using Medline and Embase (via Scopus) with the following search terms: (adheren* OR persisten* OR complian*) AND (“cystic fibrosis” OR mucoviscidosis) AND (“Pseudomonas aeruginosa”) AND (antibiotic*). No publication date limits were defined. The search results were processed in two steps: first, the titles and abstracts were screened; next, all the full text of all the potentially relevant articles were analyzed. The references of the included articles were screened for additional eligible studies. The literature screening was conducted by two independent reviewers; disagreements between reviewers were resolved by consensus.
The reasons for exclusion in both steps were the following: 1) the article reported no new evidence (ie, editorial, letter, case report, or review), 2) the article was a case study, 3) the article was not related to CF, and 4) the article had not assessed adherence to inhaled ABs for the treatment of chronic PA infection in CF. This review included only publications in which data on adherence to inhaled ABs were clearly separated from adherence data of other medications.
The data extraction was limited to findings relevant to the research topic. The following information was extracted from each included study: 1) the first author and year of publication, 2) the country, 3) the study design, 4) the study year, 5) study exclusion and inclusion criteria, 6) the study population characteristics, 7) the medication therapy, 8) the method of measuring and defining adherence, 9) adherence data, and 10) predictors and consequences of nonadherence to inhaled ABs in CF. In case of studies in which adherence rates were presented graphically only, WebPlotDigitizer 3.8 was used to extract numerical data accurately out of figures. The scope of this review was to give a systematic overview on the adherence to inhaled ABs in CF; therefore, results of adherence measures that were not applied to assess adherence to inhaled ABs were not abstracted from the included studies.
For the quality assessment of the included studies, the strengthening the reporting of observational studies in epidemiology (STROBE) checklistCitation18 was used. All the studies were independently assessed by two review authors; disagreements were resolved by consensus. The results of the quality assessment were summarized as the percentage of the fulfilled criteria for each study (criteria that were not applicable to a study were excluded from the quality assessment), ranging from 0% (none of the applicable STROBE criteria fulfilled) to 100% (all applicable STROBE criteria fulfilled).
Results
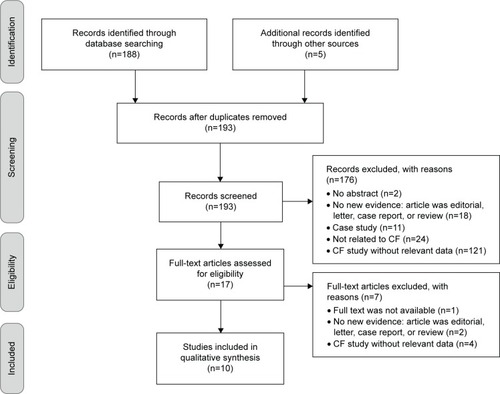
The literature search resulted in 188 hits, and five additional records were identified through hand search of the references of relevant articles. The screening of the titles and abstracts identified 17 potentially eligible studies. After the review of the relevant full texts, ten studies were finally included in the systematic review. The flow diagram of the systematic literature review process, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)Citation19 template, is presented in .
Figure 1 The flow diagram of the systematic literature review process.
Three studies were randomized controlled trials (RCTs),Citation20–Citation22 three were prospective cohort studies,Citation23–Citation25 and four retrospective studiesCitation26–Citation29 were also included. The population size varied between 28Citation28 and 832Citation29 subjects, with a mean age of 9.1Citation28 to 28.7Citation20 years. Seven studies focused on measuring adherence to inhaled tobramycin,Citation21–Citation24,Citation26,Citation27,Citation29 one on inhaled colistimethate,Citation28 one on inhaled levofloxacin,Citation20 and one on inhaled aztreonam lysine.Citation25 The general characteristics of the reviewed studies are summarized in .
Table 1 General characteristics and adherence to inhaled antibiotics results of the included studies
Medication adherence to inhaled ABs was analyzed by pharmacy refill history (30%),Citation26,Citation27,Citation29 daily phone diary (10%),Citation24 parent and/or child self-reports (20%),Citation23,Citation24 vials counting (30%),Citation20,Citation22,Citation25 or electronic monitoring (10%).Citation28 Regnault et alCitation21 were the only authors who did not describe the method for measuring adherence, while Modi et alCitation24 and Oermann et alCitation25 did not report how adherence was defined in their studies. Six studiesCitation20–Citation23,Citation26,Citation29 determined adherence as categorical variable only, five studiesCitation24,Citation25,Citation27,Citation28 as continuous only, and one study as both.Citation21 Measurement methods, results, and predictors/consequences of adherence to inhaled ABs are presented in .
Except for the studies conducted by Eakin et alCitation27 and Modi et al,Citation24 most studies assessed adherence to inhaled ABs only and did not evaluate adherence to other medications simultaneously ().
Table 2 Comparison of adherence to inhaled antibiotics and other medications in patients with cystic fibrosis
The included studies fulfilled the STROBE criteria between 52%Citation28 and 73%.Citation21,Citation29 Details of the quality assessment are provided in . The majority of the studies described their scope, study design, settings, participants, variables, measurements, and main results adequately. All but oneCitation28 of the reviewed studies described their statistical methods in detail; however, none of them undertook a sensitivity analysis to examine the robustness of the results. Furthermore, no study provided information on missing data and how they dealt with the same.
Discussion
Ten studies were identified and included in this systematic review.Citation20–Citation29 The majority of the studies focused on measuring adherence to inhaled tobramycin (n=7).Citation21–Citation26,Citation29 To our knowledge, this is the first systematic review of the adherence to inhaled ABs in CF. The results from the present study contribute to understanding the current status of adherence to inhaled ABs and for planning future research that can add to the global picture of adherence in CF.
Methodological issues: randomized controlled trials vs real-world studies
Most of the included publications were real-world studies (n=7)Citation23–Citation29 contrary to RCTs (n=3).Citation20–Citation22 From the viewpoint of health care professionals, real-world studies provide more reliable information about medication adherence in contrast with RCTs, which may overestimate adherence. As RCTs are mainly designed to assess safety and efficacy of pharmaceuticals, the study design emphasizes internal validity over generalizability. In these studies, because of protocol requirements, the data may not be applicable to the more heterogeneous patient group encountered in actual clinical practice. Effectiveness studies (eg, prospective cohort studies and retrospective studies), where treatment and/or disease management is studied under real-world conditions (eg, in unselected populations; patients are under routine care, taking open-label treatment, with no additional visits), remedy some of these limitations. This issue is especially relevant in case of adherence data. In RCTs, usually better treatment adherence is obtained due to the continuous, obligatory control visits or measurement of serum drug levels. Moreover, patients sometimes feel that they are in favored situation, because they are eligible to take part in the study and use a novel, not launched medication in CF. In addition, between regular visits, phone calls also remind patients to the use/administration of the drug, or they are asked about their experiences related to the new drug.
In the included RCTs,Citation20–Citation22 the proportion of adherent patients (>75%–80% of required doses taken) ranged between 86.4% (inhaled tobramycin, measurement method was not reported)Citation21 and 97.3% (inhaled levofloxacin, measured by vials counting).Citation20 In contrast, in the prospective cohort study conducted by Harrison et al,Citation23 only 44.9% of patients reported greater than 80% adherence to TIS and 77.5% to tobramycin inhalation powder (TIP) (measured by patient self-report). In the included retrospective studies, the proportion of highly adherent patients (>4 fills per 12 months) was found to be in the range of 7% (inhaled tobramycin, measured by pharmacy refill records)Citation26 to 29.6% (inhaled tobramycin, measured by pharmacy refill records)Citation29 ().
Adherence rates to inhaled antibiotics
Determining an overall rate for adherence to inhaled ABs in CF was difficult because different adherence definitions and measurement methods were applied in the reviewed studies; furthermore, two of the included studiesCitation24,Citation25 did not declare a clear definition for adherence. In prospective cohort studies, adherence rates ranged between 36% (inhaled tobramycin, measured by daily phone diary)Citation24 and 92% (inhaled aztreonam, measured by vials counting),Citation25 and in retrospective studies it ranged between 60% and 70% (inhaled colistimethate, measured by electronic monitoring)Citation28 (). Adherence to inhaled ABs did not differ significantly from adherence rates to other CF-related medications ().Citation27
Predictors of adherence
In the reviewed studies, adherence to inhaled ABs was found to be associated with the age of patients, patient’s satisfaction, treatment burden (ie, adverse events and taste), and time of drug administration (ie, morning vs evening inhalation).Citation21,Citation26,Citation28 McNamara et alCitation28 found that treatment adherence was better in those patients who were younger than 12 years of age (<12 years of age: 71% vs ≥12 years of age: 50%). A reasonable explanation may be the presence of parental supervision in this age group. This result is similar to the findings of Modi et al,Citation24 who reported that parental supervision of CF medical treatments can improve children’s treatment adherence. Furthermore, preadolescents and adolescents who spent more of their treatment time supervised by mothers had better adherence. Interestingly, Eakin et alCitation27 could not identify any relationships between age and treatment adherence. According to the findings of Regnault et al,Citation21 patient satisfaction with inhalation AB therapy was linked to patient adherence, and side effects seemed to be the key drivers of patients’ behavior regarding their inhaled ABs in CF. Patients’ self-perception about the efficacy of the drug,Citation30 clinical response,Citation30 cumulative toxicity,Citation30 drug intolerance,Citation26 treatment burden, and the time and frequency of administrationCitation24 could determine adherence to therapy. McNamara et alCitation28 found that evening adherence (75%) was significantly better than morning adherence (58%) to inhaled colistimethate.Citation28 A possible explanation of this phenomenon could be that children have to wake up early in the morning for complete airway clearance, chest physiotherapy, and inhalation before going to school. Unpleasant taste of the inhaled AB, delay in the improvement of lung function (FEV1 [forced expiratory volume in 1 second]), and respiratory symptoms may also lead to nonadherence.Citation20,Citation26,Citation31 Furthermore, adherence to a novel medication may be better than to an older one.Citation20
Real-world studies enable better understanding of the predictors of nonadherence from patients’ viewpoint compared with RCTs. However, since measuring adherence to inhaled ABs as a phenomenon is relatively new, many of its potential predictors have not yet been evaluated, such as relationship between treatment adherence and health-related quality of life, relationship between clinical parameters (eg, FEV1) and adherence, or direct comparison of adherence between various type of inhaled ABs in CF.
Consequences of nonadherence
In RCTs, high adherence was observed between artificial conditions compared to real-world studies. Therefore this analysis made conclusions about consequences of nonadherence on the basis of results published by real-world studies.Citation23–Citation29 Most studies concentrated on the level of adherence, on the identification of nonadherence, and on how adherence can be improved. However, only few (n=4) researches dealt with the consequences.Citation23,Citation26,Citation27,Citation29 Further studies are needed to understand the clinical consequences of nonadherence in CF.
Generally, the examination of financial impact, not the clinical impact, of poor adherence dominated in the reviewed articles. However, it was difficult to clarify the real effect of nonadherence on clinical outcomes because of the natural progression of the disease. There are many factors (eg, microbiological agents and CF-related complications), not only treatment adherence, in CF that may have an impact on the progression of the disease. Our analysis suggests that better adherence to inhaled ABs in patients with CF is significantly associated with decreased health care utilization, median outpatient costs, excluding drug costs, and decreased risk of hospitalization.Citation26,Citation29 Moreover, reductions in CF-related hospitalizations translated to significant reductions in CF-related inpatient costs. That could mean that low-adherence users may have more frequent pulmonary exacerbations and CF-related complications.Citation29 However, Eakin et alCitation27 found that adherence to inhaled tobramycin was not significantly associated with the occurrence of pulmonary exacerbation and change in FEV1% predicted slope.
Enhancing adherence
Only few of the authors of the reviewed articles developed suggestions on how adherence to inhaled ABs can be improved. McNamara et alCitation28 observed that changing treatment regimen from twice daily to once daily significantly improved adherence (26% vs 54%, in 1 month). In a real-world, prospective cohort study, Harrison et alCitation23 demonstrated that the use of a more rapid delivery system could result in increased adherence to inhaled ABs. In their research, TIP was associated with better adherence compared with TIS ().
In the recent years, some useful tools have been developed to improve medication adherence in patients with CF. Internet-based adherence interventions and mobile phone applications became more and more popular.Citation32 Besides telemedical patient management, it still seems important to improve patient education programs to provide home service programs in collaboration with social workers. However, the most important issue is to recognize the necessity of routine adherence monitoring during CF care. It is also important that physicians do not expect adherence to be the sole responsibility of patients, because improving treatment adherence is teamwork. Clinicians should understand their patients’ problems in relation to side effects or with time of administration and help patients to choose an inhaled AB that is the best for the patient. If adherence is routinely monitored and results are discussed openly with patients, then treatment regimens can be individualized for patients. This kind of interaction can result in sustainable levels of adherence during the CF care.
Limitations
The findings of this systematic review should be considered in light of the following limitations. The current systematic literature review involved searching only studies that were published in English and indexed in the selected databases; unpublished material and studies from other resources were precluded. The major limitation of the analysis is that because of the paucity of studies, small sample sizes, and diverse definitions of adherence, adherence measurement method results differ vastly, and it is difficult to make any generalizing statements regarding the general predictors of nonadherence. As a further effort, we screened the references of the included articles for additional eligible studies. STROBE checklist was developed for the quality assessment of observational studies. Specific issues related to research using routinely collected data are not addressed in STROBE; nevertheless, we also used this checklist for quality assessment of those studies in which retrospective analyses were performed.
Conclusion
Different adherence definitions and measurement methods made it difficult to determine an overall rate for adherence to inhaled ABs in CF based upon the reviewed studies. Our analysis suggests that probably because of their highly controlled conditions, RCTs provide higher adherence rate to inhaled ABs than real-world studies. Adherence to inhaled ABs was found to be associated with the complexity of treatment, time of drug administration, age of patients, treatment burden (ie, adverse events and taste), and patient satisfaction. Further research is needed to better understand the predictors of adherence to inhaled ABs, which would be critically important to the development of effective adherence-enhancing interventions. Routine adherence monitoring, discussing the possible reasons of nonadherence with the patient, and changing treatment regimens on the basis of patient burden may optimize patient management and hence improve adherence in patients with CF.
Supplementary materials
Table S1 The quality assessment of the included studies
Disclosure
The authors report no conflicts of interest in this work.
References
- KnowlesMRDuriePRWhat is cystic fibrosis?N Engl J Med2002347643944212167688
- SantisGBasic molecular geneticsHodsonMEGeddesDMCystic FibrosisLondon, UKChapman & Hall19951534
- RaidtLIdelevichEADubbersAIncreased prevalence and resistance of important pathogens recovered from respiratory specimens of cystic fibrosis patients during a decadePediatr Infect Dis J201534770070525851069
- DoringGConwaySPHeijermanHGAntibiotic therapy against Pseudomonas aeruginosa in cystic fibrosis: a European consensusEur Respir J200016474976711106223
- DoringGFlumePHeijermanHElbornJSTreatment of lung infection in patients with cystic fibrosis: current and future strategiesJ Cyst Fibros201211646147923137712
- CooneyGFLumBLTomaselliMFielSBAbsolute bioavailability and absorption characteristics of aerosolized tobramycin in adults with cystic fibrosisJ Clin Pharmacol19943432552598021334
- GellerDEPitlickWHNardellaPATracewellWGRamseyBWPharmacokinetics and bioavailability of aerosolized tobramycin in cystic fibrosisChest2002122121922612114362
- FlumePAO’SullivanBPRobinsonKACystic fibrosis pulmonary guidelines: chronic medications for maintenance of lung healthAm J Respir Crit Care Med20071761095796917761616
- FDA Briefing Document for Anti-Infective Drugs Advisory Committee MeetingAztreonam for inhalation solution (NDA 50-814) for improvement of respiratory symptoms in cystic fibrosis patients 2009 Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/Anti-InfectiveDrugsAdvisoryCommittee/UCM193023.pdfAccessed June 1, 2015
- Cystic Fibrosis FoundationDrug Development Pipeline2015 Available from: http://www.cff.org/research/DrugDevelopmentPipeline/Accessed June 1, 2015
- CramerJARoyABurrellAMedication compliance and persistence: terminology and definitionsValue Health2008111444718237359
- AbbottJDoddMBiltonDWebbAKTreatment compliance in adults with cystic fibrosisThorax19944921151208128399
- ConwaySPPondMNHamnettTWatsonACompliance with treatment in adult patients with cystic fibrosisThorax199651129338658364
- BenderBGMotivating patient adherence to allergic rhinitis treatmentsCurr Allergy Asthma Rep20151531025956611
- ChanAHStewartAWHarrisonJCamargoCAJrBlackPNMitchellEAThe effect of an electronic monitoring device with audiovisual reminder function on adherence to inhaled corticosteroids and school attendance in children with asthma: a randomised controlled trialLancet Respir Med20153321021925617215
- Arias LlorenteRPBousono GarciaCDiaz MartinJJTreatment compliance in children and adults with cystic fibrosisJ Cyst Fibros20087535936718304896
- WhiteTMillerJSmithGLMcMahonWMAdherence and psychopathology in children and adolescents with cystic fibrosisEur Child Adolesc Psychiatry20091829610418807223
- WhiteRGHakimAJSalganikMJStrengthening the reporting of observational studies in epidemiology for respondent-driven sampling studies: “STROBE-RDS” statementJ Clin Epidemiol201568121463147126112433
- MoherDLiberatiATetzlaffJAltmanDGPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementAnn Intern Med20091514264269 W26419622511
- GellerDEFlumePAStaabDLevofloxacin inhalation solution (MP-376) in patients with cystic fibrosis with Pseudomonas aeruginosaAm J Respir Crit Care Med2011183111510151621471106
- RegnaultABalpMMKulichKViala-DantenMValidation of the treatment satisfaction questionnaire for medication in patients with cystic fibrosisJ Cyst Fibros201211649450122583743
- RamseyBWPepeMSQuanJMIntermittent administration of inhaled tobramycin in patients with cystic fibrosis. Cystic Fibrosis Inhaled Tobramycin Study GroupN Engl J Med1999340123309878641
- HarrisonMJMcCarthyMFlemingCInhaled versus nebulised tobramycin: a real world comparison in adult cystic fibrosis (CF)J Cyst Fibros201413669269824815094
- ModiACLimCSYuNGellerDWagnerMHQuittnerALA multi-method assessment of treatment adherence for children with cystic fibrosisJ Cyst Fibros20065317718516679071
- OermannCMRetsch-BogartGZQuittnerALAn 18-month study of the safety and efficacy of repeated courses of inhaled aztreonam lysine in cystic fibrosisPediatr Pulmonol201045111121113420672296
- BriesacherBAQuittnerALSaimanLSaccoPFouayziHQuittellLMAdherence with tobramycin inhaled solution and health care utilizationBMC Pulm Med201111521251275
- EakinMNBilderbackABoyleMPMogayzelPJRiekertKALongitudinal association between medication adherence and lung health in people with cystic fibrosisJ Cyst Fibros201110425826421458391
- McNamaraPSMcCormackPMcDonaldAJHeafLSouthernKWOpen adherence monitoring using routine data download from an adaptive aerosol delivery nebuliser in children with cystic fibrosisJ Cyst Fibros20098425826319447080
- WertzDAChangCLStephensonJJZhangJKuhnRJEconomic impact of tobramycin in patients with cystic fibrosis in a managed care populationJ Med Econ201114675976821942462
- AppelGBAminoglycoside nephrotoxicityAm J Med19908816S20S discussion 38S–42S2180292
- ChuchalinAAmelinaEBiancoFTobramycin for inhalation in cystic fibrosis: beyond respiratory improvementsPulm Pharmacol Ther200922652653219616111
- HilliardMEHahnARidgeAKEakinMNRiekertKAUser preferences and design recommendations for an mHealth app to promote cystic fibrosis self-managementJMIR Mhealth Uhealth201424e4425344616