
Abstract
Delayed hematopoietic recovery and increased rate of engraftment failure limit the use of umbilical cord blood transplantation (UCBT). We describe a case of severe aplastic anemia treated by UCBT combined with mesenchymal stem cells. Our case reveals that infusing mesenchymal stem cells early (about 40 days) after UCBT may promote hematopoietic recovery. This experience will guide clinical scientists, especially hematologists, to deal with similar situations and encourage them to widen this strategy.
Introduction
The first successful case of umbilical cord blood transplantation (UCBT) was reported in the 1980s.Citation1 Nowadays, UCBT is recognized as one of the most significant branches of the hematopoietic stem cell transplantation (HSCT) field. However, the delay of hematopoietic reconstruction and increasing probability of engraftment failure resulting from relatively low counts of hematopoietic stem cells contained in a single cord blood (CB) unit prevent the UCBT from widespread use.Citation2–Citation4 Many strategies such as double-unit unrelated mismatched UCBT,Citation4–Citation8 direct bone marrow infusion,Citation9–Citation11 and ex vivo expansionCitation12–Citation14 have been studied to overcome the above-mentioned limitations.Citation15 The first description of mesenchymal stem cells (MSCs) by Friedenstein in 1966Citation16,Citation17 drew the attention of the biologic field, and the properties of supporting hematopoiesis of MSCs were also shown by Friedenstein in 1974.Citation18,Citation19 MSCs are multipotent stromal cells that can differentiate into a variety of cell types, including osteoblasts, chondrocytes, adipocytes, and so on.Citation20–Citation22 Due to their multilineage differentiation capacity, hematopoiesis-supporting nature, immunomodulation, and secretion of proregenerative factors,Citation23,Citation24 MSCs have been in the focus of intense research for decades.Citation21,Citation25 Here we report a case of severe aplastic anemia (SAA) successfully treated by UCBT combined with MSCs.
Case presentation
A 13-year-old Chinese girl who presented with repeated petechia and ecchymoses for 3 days accompanied by nasal bleeding once was admitted to a local hospital. Routine examination of blood revealed that the white blood cell (WBC) count was 2.64×109/L, hemoglobin (HGB) was 66.4 g/L, platelet (PLT) count was 9×109/L, neutrophil count was 0.18×109/L, and reticulocyte was 0.3%. Bone marrow examination showed that the bone marrow was extremely hypoplastic, megakaryocytes were absent, non-hematopoietic cells including plasmocyte, fibrocyte, and lymphocyte were increased, fat cells were increased significantly, hematopoietic cells were rare, and the chromosome karyotype was unremarkable; myelodysplastic syndrome (MDS) was not considered. There was no typical hemoglobinuria, Ham test was negative, and paroxysmal nocturnal hemoglobinuria (PNH) was not considered. She was diagnosed as suffering from SAA. After receiving antithymocyte globulin (ATG), cyclosporin, androgen, and component blood transfusion for 8 months, her condition did not improve.
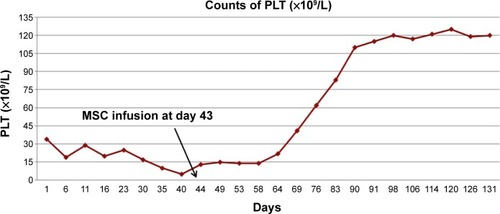
She was then transferred to our hospital. Bone marrow examination showed that the bone marrow was hypoplastic, pancytopenia was noted, megakaryocytes were absent, and the chromosome karyotype was unremarkable. She matched with her sister’s umbilical CB (HLA-A, HLA-B, HLA-DR). She was preconditioned with FC regimen (fludarabine 34 mg/m2, day 1 to day 6; cyclophosphamide 53 mg/kg, day 5 to day 6, with day 1 defined as the first day before UCBT day, and so on). She received 33 mL umbilical CB from her sibling sister with mononuclear cell 9.8×106/kg and WBC count 14.1×109/L on October 15, 2013. After transplantation, cyclosporin and mycophenolate mofetil were administered to prevent graft-versus-host disease (GVHD), alprostadil to prevent hepatic vein occlusion disease, and acyclovir to prevent cytomegalovirus (CMV) infection. Fluid infusion, alkalization of urine, and mesna were administered to prevent hemorrhagic cystitis. After transplantation, GVHD manifestation such as diarrhea, skin rash, and liver damage did not occur. Intermittent composition blood transfusion was needed. Routine blood examination on day 1 (day 1 is defined as the first day after UCBT day, and so on) showed WBC 0.15×109/L, HGB 57 g/L, and PLT 34×109/L; other blood analysis results from day 2 to day 41 are shown in . Routine blood examination on November 25, 2013 showed WBC 0.62×109/L, HGB 62 g/L, and PLT 6×109/L. She was still not grafted, and her condition did not improve. She received MSCs (total number 2×107, 4.35×105/kg, from umbilical cord; Alliancells Bioscience Co., Ltd., People’s Republic of China) on November 27, 2013. She had no obvious discomfort during the process or adverse reaction after the process. Routine blood examination before she was discharged showed WBC 3–5×109/L, HGB 80–90 g/L, and PLT 100–124×109/L. The shimeric state showed complete donor phenotype. The changing trends of her WBC counts before and after MSC infusion are shown in , the HGB counts in , and PLT counts in . The figures show that after MSC infusion, counts of WBC, HGB, and PLT increased and fluctuated around their normal levels; she was at complete remission and followed up.
Figure 1 Counts of WBC from day 1 to day 131.
Abbreviations: WBC, white blood cell; MSC, mesenchymal stem cell.
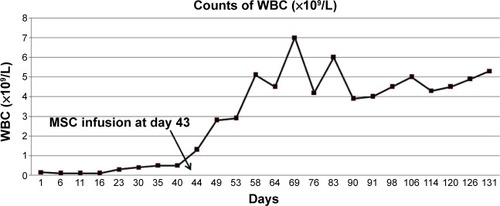
Figure 2 Counts of HGB from day 1 to day 131.
Abbreviations: HGB, hemoglobin; MSC, mesenchymal stem cell.
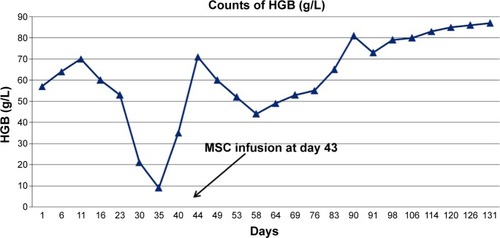
Figure 3 Counts of PLT from day 1 to day 131.
Abbreviations: PLT, platelet; MSC, mesenchymal stem cell.
Discussion
Compared to bone marrow transplantation (BMT), UCBT provides many advantages. The acquisition of CB is easy, and the collection is harmless both to the mother and the newborn infant. Also, HSCs from the CB graft can be cryopreserved and transplanted to the host after thawing without losing its reproducing ability. Broxmeyer’s study found no significant differences of nucleated cells, granulocyte-macrophage (CFU-GM), erythroid (BFU-E), and multipotential (CFU-GEMM) progenitors after cryopreservation of CB for 10 years.Citation26 Yamamoto et al reported that the recovery rate of total nucleated cell (TNC) count, CD34+ cell count, and CFU-GM number was not significantly different between the study group (18 CB units, collected between April 1998 and September 1998) and control group (18 CB units, collected between May 2008 and June 2008).Citation27 The latest study by Mitchell et al showed that UCB units after cryopreservation for at least 10 years had no impact on the clinical outcome.Citation28 The incidence of GVHD related to UCBT is generally lower than in BMT. According to Hwang et al GVHD incidence in unrelated UCBT is not higher than unrelated-donor BMT in pediatric patients: chronic GVHD (cGVHD) is lower in UCBT, and acute GVHD (aGVHD) (III–IV) is no different.Citation29 Zhang et al reported that the incidence rates of both aGVHD and cGVHD were significantly lower in the UBMT group compared with the BMT group in acute leukemia patients.Citation30 But Chen et al reported that the incidence of Grade 2–4 and 3–4 aGVHD was increased in the UBMT group compared with the BMT group and that the incidence of extensive cGVHD was significantly lower in UCBT.Citation31 Another obvious advantage of UCBT compared with BMT is the relatively low human leukocyte antigen (HLA)-matching requirements. A high degree of HLA matching is generally required in BMT, namely 6 of 6 (HLA-A, HLA-B, and HLA-DR loci), and only 30% of patients needing allogeneic HSCT can have access to a matched sibling donor.Citation2 For UCBT, a minimum 4 of 6 HLA allele matching is required, but 5 of 6 is ideal.Citation32
While hematopoiesis recovery is slow,Citation2–Citation4 and infectious complication incidence is high in CB recipients.Citation33,Citation34 Delayed hematopoietic recovery and increased rate of engraftment failure limit the use of UCBT. Delayed hematopoietic recovery could result in infection complication and increased transplantation-related mortality (TRM). UCBT outcomes have been proven to be closely associated with CD34+ dose or TNC dose.Citation35 Wagner et alCitation36 reported that the dose of CD34+ cells was a significant factor related to the rate of engraftment, TRM, and survival in Cox regression analyses. Eapen et alCitation37 found that with the TNC >3.0×107/kg, the overall outcome significantly improved in children with acute leukemia. The CD34+ dose in a CB graft is on average 1–2 log smaller than in an unrelated BM or peripheral blood stem cell graft.Citation38 Many strategies mentioned in the Introduction are utilized to overcome the low dose limitation in CB.
MSCs can be found in various tissues, such as peripheral blood, umbilical cord and placenta, bone marrow. Because of their properties such as multilineage differentiation capacity, hematopoiesis-supporting nature, immunomodulation, and secretion of proregenerative factors, MSCs have been regarded as potential therapeutic agents in many clinical diseases, in particular for the treatment of hematologic and immunological disorders. MSCs are used to treat autoimmune diseases as well. Constantin et alCitation39 reported that MSCs derived from adipose administered intravenously before onset of the disease significantly mitigated the severity of autoimmune encephalomyelitis (EAE) due to their immunomodulation properties. As regard to hematological disorders, MSCs are reported to be studied and used in various disorders, maybe due to their properties of hematopoiesis support and immunomodulation. Robinson et alCitation40 showed that a 10–20-fold increase in TNCs, a 7–18-fold increase in progenitor cells, and a 16–37-fold increase in CD34+ cells could be achieved by coculturing CB cells with MSCs. Nauta et alCitation41 reported that significant enhancement of long-term engraftment with better tolerance to host and donor antigens was achieved by the addition of host MSCs. The underlying mechanism of the immunomodulation of MSCs is not very clear, but growing evidence reveals that MSCs exhibit immunosuppressive activity on T cells,Citation42–Citation46 B cells,Citation47,Citation48 and natural killer (NK) cells.Citation49–Citation51 The underlying mechanism of hematopoiesis support of MSCs is supposed to be the effect of supporting the reconstruction of hematopoietic microenvironment in addition to direct hematopoiesis.Citation52–Citation54
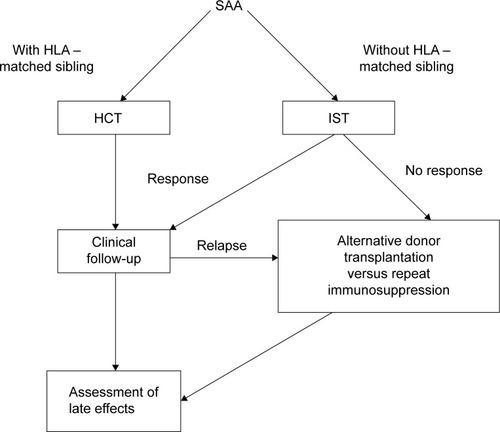
Aplastic anemia (AA) is a disease in which the bone marrow and the blood stem cells are damaged, which causes pancytopenia, including anemia, leukopenia, and thrombocytopenia. Its causes are various, and it is regarded as an autoimmune disorderCitation55 in which immune cells (mainly T cells)Citation56 attack the bone marrow and cause pancytopenia. Its first-line treatment consists of hematopoietic cell transplantation and administration of immunosuppressive drugs. SAA is life-threatening and needs immediate treatment. Adolescents and young adults (age <30 years) with SAA who have an HLA-matched sibling donor should proceed directly to hematopoietic cell transplantation;Citation57–Citation59 the treatment schemeCitation57 is shown in . But this treatment scheme does not consider the situation in which the patients do not respond to hematopoietic cell transplantation.
Figure 4 Treatment schema of SAA.
There have been reports in the literature on the use of MSCs during allogeneic transplantation to enhance engraftment.Citation60–Citation62 Our patient was an SAA case. She matched with her sister’s umbilical CB and was without transplantation-associated contraindications, but she did not respond to immunosuppressive therapy (IST) or UCBT. After failure of the initial UCBT treatment, considering AA is of pancytopenia and an immunity-related disease and the limitation of delayed hematopoietic recovery and increased rate of engraftment failure of UCBT discussed above, we decided to apply MSCs to this patient for its hematopoiesis-supporting properties and immunomodulation. After MSC infusion, the WBC count increased and fluctuated around the normal level; she was on complete remission and followed up.
Before this case, our department had handled four cases of UCBT and they all failed. Their basic clinical parameters are listed in . The first patient died of central nervous system infection and intracranial hemorrhage. The second one died of septic shock and disseminated intravascular coagulation. The third died of respiratory failure, severe pneumonia, and acute renal failure. The fourth died of interstitial pneumonia and acute left heart failure. Infection was a common cause of death of the four patients after receiving UCBT, and the mean interval between UCBT and death was 47.5 days.
Table 1 Basic clinical parameters of the other four UCBT patients
It is still challenging to deal with delayed hematopoietic recovery and to increase the rate of engraftment after UCBT. As discussed above, delayed hematopoietic recovery easily results in infection, and it is hard to control infection if hematopoietic recovery is delayed.
Our case reveals that infusing MSCs early (about 40 days) after UCBT may promote hematopoietic recovery. However, as this is a single case study without a controlled trial, we cannot be sure whether the MSC infusion had any effect in promoting hematopoietic recovery, or whether the initial CB engraftment was just delayed or infusion of MSC with engraftment was just coincidental. Further studies such as controlled trials and more cases are needed to prove the effect of MSC infusion to promote hematopoietic recovery in UCBT. But surely, the hematopoietic-supporting and immunomodulation properties of MSC are increasingly attracting the attention of scientists and clinicians, and our experience will encourage clinical scientists, especially hematologists, to elaborate this strategy while dealing with a similar situation or another.
Acknowledgments
This work was supported by the National Natural Science Foundation of People’s Republic of China (Grant no 81170492, 81370673), the National High Technology Research and Development Program 863 of People’s Republic of China (Grant no 2012AA022703), the National Key Basic Research Program 973 of People’s Republic of China (Grant no 2010CB732404), the Key Medical Projects of Jiangsu Province (Grant no BL2014078), and the Key Discipline of Jiangsu Province (2011–2015).
Disclosure
The authors declare no conflicts of interest in this work.
References
- GluckmanEBroxmeyerHAAuerbachADHematopoietic reconstitution in a patient with Fanconi’s anemia by means of umbilical-cord blood from an HLA-identical siblingN Engl J Med198932117117411782571931
- OranBShpallEUmbilical cord blood transplantation: a maturing technologyHematology Am Soc Hematol Educ Program2012201221522223233584
- RochaVGluckmanEImproving outcomes of cord blood transplantation: HLA matching, cell dose and other graft- and transplantation-related factorsBr J Haematol2009147226227419796275
- De LimaMSt JohnLSWiederEDDouble-chimaerism after transplantation of two human leucocyte antigen mismatched, unrelated cord blood unitsBr J Haematol2002119377377612437658
- SideriANeokleousNBrunet De La GrangePAn overview of the progress on double umbilical cord blood transplantationHaematologica20119681213122021546497
- YinYRenHYCenXALong-term outcomes in adults with leukemia treated with transplantation of two unrelated umbilical cord blood unitsChin Med J (Engl)2011124162411241621933579
- HuangSLZhouDH非血缘异基因脐血造血干细胞移植现状: 问题与对策 [Unrelated allogeneic umbilical cord blood transplantation: present status, problems and countermeasures]Zhongguo Shi Yan Xue Ye Xue Za Zhi200917117 Chinese19236736
- HashemHLazarusHMDouble umbilical cord blood transplantation: relevance of persistent mixed-unit chimerismBiol Blood Marrow Transplant201521461261925230381
- RochaVLabopinMRuggeriAUnrelated cord blood transplantation: outcomes after single-unit intrabone injection compared with double-unit intravenous injection in patients with hematological malignanciesTransplantation201395101284129123507699
- FrassoniFGualandiFPodestaMDirect intrabone transplant of unrelated cord-blood cells in acute leukaemia: a phase I/II studyLancet Oncol20089983183918693069
- BrunsteinCGBarkerJNWeisdorfDJIntra-BM injection to enhance engraftment after myeloablative umbilical cord blood transplantation with two partially HLA-matched unitsBone Marrow Transplant2009431293594019139736
- Flores-GuzmanPFernandez-SanchezVMayaniHConcise review: ex vivo expansion of cord blood-derived hematopoietic stem and progenitor cells: basic principles, experimental approaches, and impact in regenerative medicineStem Cells Transl Med201321183083824101670
- GeJCaiHLiQDuZTanWSEffects of telomerase activity and apoptosis on ex vivo expansion of cord blood CD34(+) cellsCell Prolif2013461384423240888
- HorwitzMEFrassoniFImproving the outcome of umbilical cord blood transplantation through ex vivo expansion or graft manipulationCytotherapy201517673073825778757
- YuXGuZWangYWangHNew strategies in cord blood cells transplantationCell Biol Int201337986587423589409
- FriedensteinAJPiatetzkyS2ndPetrakovaKVOsteogenesis in transplants of bone marrow cellsJ Embryol Exp Morphol19661633813905336210
- ChaoYHWuHPChanCKTsaiCPengCTWuKHUmbilical cord-derived mesenchymal stem cells for hematopoietic stem cell transplantationJ Biomed Biotechnol2012201275950323093863
- FriedensteinAJChailakhyanRKLatsinikNVPanasyukAFKeiliss-BorokIVStromal cells responsible for transferring the microenvironment of the hemopoietic tissues. Cloning in vitro and retransplantation in vivoTransplantation19741743313404150881
- ResnickIStepenskyPElkinGMSC for the improvement of hematopoietic engraftmentBone Marrow Transplant201045360560619718072
- HarrisDTUmbilical cord tissue mesenchymal stem cells: characterization and clinical applicationsCurr Stem Cell Res Ther20138539439923895058
- SharmaRRPollockKHubelAMcKennaDMesenchymal stem or stromal cells: a review of clinical applications and manufacturing practicesTransfusion20145451418143724898458
- SoleymaninejadianEPramanikKSamadianEImmunomodulatory properties of mesenchymal stem cells: cytokines and factorsAm J Reprod Immunol20126711821951555
- SerakinciNFahriogluUChristensenRMesenchymal stem cells, cancer challenges and new directionsEur J Cancer20145081522153024613620
- VanikarAVTrivediHLKumarAGopalSCKuteVBMesenchymal stem cells and transplant toleranceNephrology (Carlton)201419736937424698403
- BiebackKWuchterPBesserDMesenchymal stromal cells (MSCs): science and f(r)ictionJ Mol Med (Berl)201290777378222648521
- BroxmeyerHECooperSHigh-efficiency recovery of immature haematopoietic progenitor cells with extensive proliferative capacity from human cord blood cryopreserved for 10 yearsClin Exp Immunol1997107suppl 145539020936
- YamamotoSIkedaHToyamaDQuality of long-term cryopreserved umbilical cord blood units for hematopoietic cell transplantationInt J Hematol20119319910521207212
- MitchellRWagnerJEBrunsteinCGImpact of long-term cryopreservation on single umbilical cord blood transplantation outcomesBiol Blood Marrow Transplant2015211505425262882
- HwangWYSamuelMTanDKohLPLimWLinnYCA meta-analysis of unrelated donor umbilical cord blood transplantation versus unrelated donor bone marrow transplantation in adult and pediatric patientsBiol Blood Marrow Transplant200713444445317382250
- ZhangHChenJQueWA meta-analysis of unrelated donor umbilical cord blood transplantation versus unrelated donor bone marrow transplantation in acute leukemia patientsBiol Blood Marrow Transplant20121881164117322289799
- ChenYHXuLPLiuDHComparative outcomes between cord blood transplantation and bone marrow or peripheral blood stem cell transplantation from unrelated donors in patients with hematologic malignancies: a single-institute analysisChin Med J (Engl)2013126132499250323823825
- WangFHeJChenSHLA-A, HLA-B, HLA-DRB1 allele and haplotype frequencies in 6,384 umbilical cord blood units and transplantation matching and engraftment statistics in the Zhejiang cord blood bank of ChinaInt J Immunogenet2014411131923731569
- ParodyRMartinoRRoviraMSevere infections after unrelated donor allogeneic hematopoietic stem cell transplantation in adults: comparison of cord blood transplantation with peripheral blood and bone marrow transplantationBiol Blood Marrow Transplant200612773474816785063
- DanbyRRochaVImproving engraftment and immune reconstitution in umbilical cord blood transplantationFront Immunol201456824605111
- GluckmanERochaVArceseWFactors associated with outcomes of unrelated cord blood transplant: guidelines for donor choiceExp Hematol200432439740715050751
- WagnerJEBarkerJNDeForTETransplantation of unrelated donor umbilical cord blood in 102 patients with malignant and nonmalignant diseases: influence of CD34 cell dose and HLA disparity on treatment-related mortality and survivalBlood200210051611161812176879
- EapenMRubinsteinPZhangMJOutcomes of transplantation of unrelated donor umbilical cord blood and bone marrow in children with acute leukaemia: a comparison studyLancet200736995771947195417560447
- LindemansCAVan BesienKTopping it up: methods to improve cord blood transplantation outcomes by increasing the number of CD34+ cellsCytotherapy201517672372925791069
- ConstantinGMarconiSRossiBAdipose-derived mesenchymal stem cells ameliorate chronic experimental autoimmune encephalomyelitisStem Cells200927102624263519676124
- RobinsonSNNgJNiuTSuperior ex vivo cord blood expansion following co-culture with bone marrow-derived mesenchymal stem cellsBone Marrow Transplant200637435936616400333
- NautaAJWesterhuisGKruisselbrinkABLurvinkEGWillemzeRFibbeWEDonor-derived mesenchymal stem cells are immunogenic in an allogeneic host and stimulate donor graft rejection in a nonmyeloablative settingBlood200610862114212016690970
- Di NicolaMCarlo-StellaCMagniMHuman bone marrow stromal cells suppress T-lymphocyte proliferation induced by cellular or nonspecific mitogenic stimuliBlood200299103838384311986244
- ZhaoKLouRHuangFImmunomodulation effects of mesenchymal stromal cells on acute graft-versus-host disease after hematopoietic stem cell transplantationBiol Blood Marrow Transplant20152119710425300866
- YanZZhuansunYChenRLiJRanPImmunomodulation of mesenchymal stromal cells on regulatory T cells and its possible mechanismExp Cell Res20143241657424681107
- BartholomewASturgeonCSiatskasMMesenchymal stem cells suppress lymphocyte proliferation in vitro and prolong skin graft survival in vivoExp Hematol2002301424811823036
- AbumareeMAl JumahMPaceRAKalionisBImmunosuppressive properties of mesenchymal stem cellsStem Cell Rev20128237539221892603
- CorcioneABenvenutoFFerrettiEHuman mesenchymal stem cells modulate B-cell functionsBlood2006107136737216141348
- DengWHanQLiaoLYouSDengHZhaoRCEffects of allogeneic bone marrow-derived mesenchymal stem cells on T and B lymphocytes from BXSB miceDNA Cell Biol200524745846316008514
- WangHFShiYJRenHY骨髓间充质干细胞对异体自然杀伤细 胞调节作用的研究 [Bone marrow-derived mesenchymal stem cells regulate the proliferation and activity of natural killer cells]Zhongguo Shi Yan Xue Ye Xue Za Zhi2012202438442 Chinese22541115
- LiYQuYHWuYFBone marrow mesenchymal stem cells suppressing activation of allogeneic cytokine-induced killer/natural killer cells either by direct or indirect interactionCell Biol Int201539443544525492047
- SpaggiariGMCapobiancoABecchettiSMingariMCMorettaLMesenchymal stem cell-natural killer cell interactions: evidence that activated NK cells are capable of killing MSCs, whereas MSCs can inhibit IL-2-induced NK-cell proliferationBlood200610741484149016239427
- PontikoglouCDeschaseauxFSensebeLPapadakiHABone marrow mesenchymal stem cells: biological properties and their role in hematopoiesis and hematopoietic stem cell transplantationStem Cell Rev20117356958921249477
- HuoSWZhangY间充质干细胞在造血调控中的作用 [Mesenchymal stem cells in hematopoietic regulation – review]Zhongguo Shi Yan Xue Ye Xue Za Zhi2006141187190 Chinese16584622
- HaoLSunHWangJWangTWangMZouZMesenchymal stromal cells for cell therapy: besides supporting hematopoiesisInt J Hematol2012951344622183780
- YoungNSCurrent concepts in the pathophysiology and treatment of aplastic anemiaHematology Am Soc Hematol Educ Program20132013768124319166
- WestonWGuptaVAdkinsRJurecicRNew therapeutic approaches for protecting hematopoietic stem cells in aplastic anemiaImmunol Res2013571–3344324203441
- DeZernAEGuinanECAplastic anemia in adolescents and young adultsActa Haematol20141323–433133925228559
- HartungHDOlsonTSBesslerMAcquired aplastic anemia in childrenPediatr Clin North Am20136061311133624237973
- KurrePJohnsonFLDeegHJDiagnosis and treatment of children with aplastic anemiaPediatr Blood Cancer200545677078015706582
- BallLMBernardoMERoelofsHCotransplantation of ex vivo expanded mesenchymal stem cells accelerates lymphocyte recovery and may reduce the risk of graft failure in haploidentical hematopoietic stem-cell transplantationBlood200711072764276717638847
- Le BlancKSamuelssonHGustafssonBTransplantation of mesenchymal stem cells to enhance engraftment of hematopoietic stem cellsLeukemia20072181733173817541394
- MacmillanMLBlazarBRDeForTEWagnerJETransplantation of ex-vivo culture-expanded parental haploidentical mesenchymal stem cells to promote engraftment in pediatric recipients of unrelated donor umbilical cord blood: results of a phase I-II clinical trialBone Marrow Transplant200943644745418955980