
Abstract
This study explored the influence of individual and social factors regarding intentions and behaviors related to prosthodontic treatment, using the theory of planned behavior (TPB). A cross-sectional study was designed with a sample of 225 individuals with some degree of tooth loss. A questionnaire was used containing factors that would have potential influence on the intentions and behaviors of individuals, as well as clinical and sociodemographic data. Descriptive statistics, internal consistency analysis, chi-square test for trend, and logistic regression were used for data analysis. The TPB components – attitude toward the behavior (ATB), subjective norm (SN), and perceived behavioral control (PBC) – showed good internal consistency (alpha = 0.60–0.78). Intention and behavior were associated with TPB components and the overall scale. Similarly, positive intentions and behaviors were associated with age, upper tooth loss, anterior tooth loss, and higher social status. Multiple logistic regression showed that intention was associated with PBC (OR =1.57; P<0.016), while behavior was associated with tooth loss in both arches (OR =9.3; P<0.001), anterior tooth loss (OR =5.13; P<0.001), higher social status (OR =3.06; P<0.03), and PBC (OR =1.38; P=0.03). The presence of anterior tooth loss was the most relevant factor for prosthodontic treatment demand and utilization, while socioeconomic status and an individual’s perceived ease or difficulty in undergoing treatment played a significant, but secondary, role in behavior toward prosthodontic care.
Introduction
Although preventive dentistry helps control the risk factors for tooth loss, and there has been a downward trend in edentulism in recent decades, the demand for prosthodontic treatment is expected to rise even in developed countries as a result of the rapid increase in elderly populations and the increasing numbers of adults retaining their natural teeth.Citation1 This background requires effective strategies from public and private oral health care systems to appropriately treat those with prosthodontics and diminish the existing inequalities in treatment access.
There is sound evidence about the effectiveness of several strategies for treatment of tooth loss using conventional and implant treatments for a wide range of prosthodontic needs and across a broad variety of clinical situations that go from uncomplicated single tooth loss to complex and extensive treatment for complete edentulism. However, there are also significant barriers regarding access to oral health care, which impair overall demand for treatment. These barriers also make the overall demand dependent on available treatment options and resources from both the care provider and society, as well as several social and psychological processes that transform need into demand and demand into effective utilization. These usually focus on oral reconstruction from a functional and esthetic point of view, rather than dealing with a life-threatening disease or oral condition that requires compulsory intervention.Citation2,Citation3
To identify and assess reliable factors that influence individual patterns of health services use, social cognition models and health behavior theories have been applied to oral health care, using concepts from behavioral science research. These models, such as the theory of planned behavior (TPB),Citation4 attempt to identify and explain how expectations, judgments, beliefs, and intentions lead to various behaviors concerning oral health care.Citation5,Citation6 A key starting point for the development of social cognition models of health behavior is the observation that although social structural factors such as age, sex, and socioeconomic status are reliably associated with health actions, it is usually difficult and sometimes impossible to modify these factors. Thus, cognition rather than social structure variables may be considered when modeling the determinants of health behaviors.Citation7
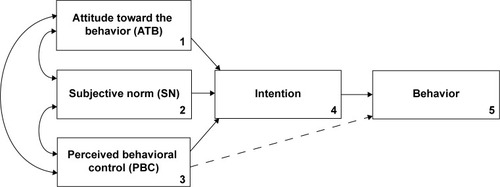
According to Ajzen,Citation4 TPB considers three independent determinants of intention, which in turn influence the consequent behavior (): (1) attitude toward the behavior (ATB) (ie, the favorable or unfavorable evaluation of the behavior), (2) subjective norm (SN) (ie, the perceived social pressures to perform or not to perform the behavior), and (3) perceived behavior control (PBC) (ie, the perception of the extent to which the behavior is within the individual’s control, measured in terms of self-efficacy and controllability in relation to the behavior). In prosthodontics, these factors match a corresponding set of behavior-related beliefs (behavioral, normative, and control beliefs) that refect the underlying cognitive structure of the TPB, as described elsewhere.Citation8
Figure 1 Conceptual framework of the theory of planned behavior.
Abbreviations: ATB, attitude toward the behavior; SN, subjective norm; PBC, perceived behavioral control.
We assumed that consumers of prosthodontic care are rational, make systematic use of information available to them, and consider the implications of their actions before making a decision about their treatment. We also hypothesized that patients’ behaviors can be somewhat predicted by the TPB model, but there is scarce systematic and sound information about patients’ intentions, attitudes, and behaviors concerning prosthodontic care on which to base predictions of decision-making in oral health. Hence, this study aimed to explore the influence of attitudes, social norms, and control beliefs, as well as clinical and socioeconomic variables, on patients’ intentions and behaviors for predicting willingness to undergo prosthodontic care.
Material and methods
This was a cross-sectional study that included a convenience sample of subjects over 18 years of age, with some degree of tooth loss, irrespective of sex, general dental conditions, and treatment needs. No subjects were under current dental treatment. All subjects were residents of two capital cities in the central region of Brazil (Goiania, Goiás and Palmas, Tocantins). Data collection occurred between January 2012 and March 2013. The study protocol was approved by the local ethical research committee.
A questionnaire was created based on 15 predictive factors of the TPB (ATB – n=6, SN – n=5, and PBC – n=4) proposed in a previous study.Citation8 Subsequently, a set of 42 raw items was created based on the subject’s likelihood of a prosthodontic treatment-seeking behavior, with affirmatives concerning attitudes and beliefs about tooth loss and prosthodontic treatment. Responses were measured using a 7-point Likert scale (1= strongly disagree, 2= moderately disagree, 3= slightly disagree, 4= neutral, 5= slightly agree, 6= moderately agree, and 7= strongly agree). Some items on the scale were reversed to achieve the same meaning from the overall direction of the scale (reversal items), and a mean score was calculated for each TPB component.
Further reliability analysis was performed to assess the properties of the component subscales (ATB, SN, and PBC) and overall scale scores using Cronbach’s alpha as a model of internal consistency based on the average inter-item correlation. Values of internal consistency were ATB =0.60, SN =0.71, PBC =0.61, and an overall scale =0.78. The affirmatives that comprise the final instrument used for analysis are listed in .
Table 1 Categories and items used for questionnaire construction, using the components of the TPB construct to explore opinions and attitudes toward prosthodontic treatment
The outcome components of TPB (intention and behavior) were also assessed in the questionnaire and regarded as separate dependent variables. The intention to undergo prosthodontic treatment (for substitution, repair, or new treatment) was measured as a response to the question, “If you had a new tooth loss or a problem with your existing prosthesis, would you intend to undergo treatment within 6 months?” Responses were measured using a 7-point Likert scale (1= definitely not, 2= probably not, 3= maybe not, 4= neutral, 5= maybe yes, 6= probably yes, and 7= definitely yes). Afterward, subjects were dichotomized using the median value of the distribution of scores.
Behavior was assessed through direct reporting and clinical examination for identification of replaced missing teeth and untreated edentulous spaces. Individuals were separated into two groups: (1) subjects with replaced missing teeth and no untreated edentulous spaces (positive behavior group) and (2) subjects with at least one untreated edentulous space for at least 6 months (negative behavior group).
ATB, SN, PBC, and the overall TPB scale were used as behavioral predictors of the subjects’ intentions and behaviors toward prosthodontic treatment. Additionally, sociodemographic variables were also assessed, such as age, sex, educational level, and socioeconomic status. Stratification of the subject’s socioeconomic status was based on the Brazilian government’s classification system that classifies its citizens by socioeconomic level (A1, A2, B1, B2, C1, C2, D, and E), where A1 is the highest level and E the lowest level, based on education and ownership of consumer durable goods.Citation9
Clinical data included the location of the edentulous spaces (maxillary and/or mandibular arch), site of tooth loss (anterior and/or posterior), presence and number of untreated and treated edentulous spaces, and types of previous prosthodontic treatment. Additionally, oral health-related quality of life impacts were measured using the Brazilian version of the Oral Health Impact Profile (OHIP-14) instrument.Citation10
Descriptive analysis was performed using frequency analysis for nominal variables and central tendency and dispersion measures for continuous variables. Simple and multiple logistic regressions were used to test the association between intention or behavior (dependent variables) and the independent variables (predictive factors of the TPB, clinical status, and socioeconomic status). All statistical analysis was performed using IBM-SPSS 20.0 software.
Results
A sample of 225 subjects completed the questionnaire; 52.0% were female and aged from 18 years to 84 years (mean = 42.8; standard deviation [SD] =13.4). Most of the respondents were classified in the middle-class socioeconomic stratum (classes B and C =82.7%). describes characteristics of the sample according to the occurrence of previous prosthodontic treatment. The most common configurations of tooth loss were only posterior edentulous space for both maxilla (45.2%) and mandible (74.6%). Cross-tabulation of upper and lower tooth loss revealed that the most common configurations were combined upper and lower posterior tooth loss (n=47; 21.6%) and lower posterior only (n=42; 19.3%). Only eleven subjects (4.9%) were fully edentulous.
Table 2 Distribution of sociodemographic and clinical variables according to the occurrence of previous prosthodontic treatment
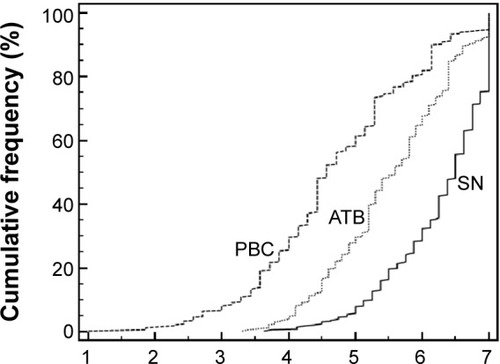
The cumulative frequency distribution of the scores on the ATB, SN, and PBC scales is shown in . Participants had positive attitudes, SNs, and self-control toward prosthodontic treatment. Lower scores were found for PBC compared to ATB and SN (P<0.001), and significant Pearson’s correlation coefficients (P<0.001) were found between all scales (ATB–SN =0.57, ATB–PBC =0.39, SN–PBC =0.38).
Figure 2 cumulative frequency distribution of the scores of scales: ATB, SN, and PBC.
shows descriptive values of the TPB and OHIP scales as well as the results of simple logistic regression for the association between intention/behavior and independent variables. The results showed that intention and behavior were associated with all of the TPB components (P<0.05) and the overall TPB scale (P<0.01). Similarly, positive intention and behavior were associated with age, upper tooth loss, anterior tooth loss, and higher social status.
Table 3 Results of simple logistic regression for the association between intention or behavior (dependent variables) and predictive factors of the TPB
The final multiple regression models are shown in . Positive intention was only predicted by PBC (odds ratio [OR] =1.57; 95% confidence interval [CI] =1.09–2.26), while positive behavior was associated with the position of tooth loss (maxillary and anterior tooth loss) (P<0.001), higher socioeconomic status (OR =3.06; 95% CI =1.11–8.44), and PBC (OR =1.38; 95% CI =1.03–1.84).
Table 4 Results of multiple logistic regression for factors predicting intention and behavior, including clinical, socioeconomic, and TPB components as independent variables
Discussion
This study aimed to investigate how attitudes, SNs, and PBC (as components of the TPB conceptual structure) are shaped and how they could ultimately enable a better understanding of the reasons that individuals demand and utilize prosthodontic care services.Citation8
Results revealed that treatment-seeking behavior might not be accurately explained or predicted by the three components of the TPB: ATBs, SN, and PBC. Conversely, behaviors about prosthodontic treatment may be strongly influenced by clinical features (extension and position of edentulous spaces), socioeconomic status, and the individual’s PBC, which encompass the ease or difficulty of performing this particular behavior, taking into account aspects such as time availability, management of financial costs, and access to health care services.
Previous evidence shows that the likelihood of demanding and utilizing prosthodontic care depends on the position of the edentulous spaces, since individuals are more likely to replace anterior than posterior missing teeth.Citation11 There is a positive association between missing tooth position and patient satisfaction with the mouth; also, the presence of an intact anterior sextant and at least three premolars in occlusion is the best predictor of satisfaction.Citation11,Citation12
Alternative strategies for the replacement of posterior missing teeth, such as the shortened dental arch concept, assure masticatory function, occlusal support, and dental arch stability for most elderly people.Citation13 This concept postulates that a dentition with preserved anterior teeth and premolars is sufficient for acceptable levels of satisfaction with appearance, functionality, comfort, improved oral hygiene, and reduced costs;Citation14,Citation15 and it has been proven that functionally oriented treatment is a more feasible and cost-effective approach for subjects with limited physical and/or financial resources.Citation16,Citation17 Treatment based on the shortened dental arch concept was 1.84 times more cost effective than conventional removable prostheses in a group of partially dentate older patients.Citation17 Satisfaction with oral condition is affected by the extent and position of edentulous spaces;Citation12 the higher the number of lost teeth (and lower occlusal units), the greater the impairment of oral health-related quality of life.Citation18 However, tooth replacement should not necessarily be regarded as the definitive therapy for posterior bounded edentulous spaces, although more robust studies are necessary to clarify the long-term effects of non-treatment.Citation19
Socioeconomic status such as education level, income, employment status, and place of residence are strong predictors of dental care service utilization.Citation20 Disadvantaged population groups are also more affected by barriers to accessibility, which increases inequalities regarding access to oral health services and worsens individuals’ attitudes toward treatment costs. All of these aforementioned aspects are important predictors of prosthodontic treatment-related behavior for specific population groups.
No previous clinical study used the TPB framework to try to explain the intention and behavior-related factors that influence prosthodontic treatment-seeking. The preliminary results of our study suggest that new investigations with other representative samples may be conducted to improve the validity of these findings. Future studies are also needed to attempt to create reliable and valid questionnaires in order to improve the accuracy of their assessment and evaluation. To increase the consistency of the scales, more related items testing the same concept should be added to the test. In addition, other new explanatory models may be proposed to identify other relevant psychosocial dimensions, since it has been shown that intentions and behaviors toward prosthodontic treatment cannot be fully explained by the TPB components unless clinical and socioeconomic features are included in the model.
Conclusion
The position of the edentulous spaces is the most relevant factor for prosthodontic treatment demand and utilization, while socioeconomic and an individual’s perceived ease or difficulty of undergoing treatment may play a significant but secondary role in behavior toward prosthodontic interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
- WuBLiangJPlassmanBLRemleCLuoXEdentulism trends among middle-aged and older adults in the United States: comparison of five racial/ ethnic groupsCommunity Dent Oral Epidemiol201240214515321974715
- NarbyBKronströmMSöderfeldtBPalmqvistSProsthodontics and the patient: what is oral rehabilitation need? Conceptual analysis of need and demand for prosthodontic treatment. Part 1: a conceptual analysisInt J Prosthodont2005181757915754898
- NarbyBKronströmMSöderfeldtBPalmqvistSProsthodontics and the patient. Part 2: need becoming demand, demand becoming utilizationInt J Prosthodont200720218318917455442
- AjzenIThe Theory of Planned BehaviorOrgan Behav Hum Decis Process1991502179211
- LuzziLSpencerAJFactors influencing the use of public dental services: an application of the Theory of Planned BehaviorBMC Health Serv Res200889318445298
- Buunk-WerkhovenYADijkstraAvan der SchansCPDeterminants of oral hygiene behavior: a study based on the Theory of Planned BehaviorCommunity Dent Oral Epidemiol201139325025921070323
- GodinGSheeranPConnerMBélanger-GravelAGallaniMCNolinBSocial structure, social cognition, and physical activity: a test of four modelsBr J Health Psychol201015799519321038
- VieiraAHLelesCRExploring motivations to seek and undergo prosthodontic care: an empirical approach using the Theory of Planned Behavior constructPatient Prefer Adherence201481215122125246777
- Associação Brasileira de Empresas de Pesquisa (ABEP)Critério de Classificação Econômica Brasil2011 Available from: http://www.abep.org/criterioBrasil.aspxAccessed 21 March, 2011
- OliveiraBHNadanovskyPPsychometric properties of the Brazilian version of the oral health impact profile – short formCommunity Dent Oral Epidemiol200533430731416008638
- EliasACSheihamAThe relationship between satisfaction with mouth and number and position of teethJ Oral Rehabil19982596496619758393
- EliasACSheihamAThe relationship between satisfaction with mouth and number, position and condition of teeth: studies in Brazilian adultsJ Oral Rehabil1999261537110080325
- GotfredsenKWallsAWWhat dentition assures oral function?Clin Oral Implants Res200718344517594368
- ArmelliniDvon FraunhoferJAThe shortened dental arch: a review of the literatureJ Prosthet Dent200492653153515583557
- KannoTCarlssonGEA review of the shortened dental arch concept focusing on the work by the Käyser/Nijmegen groupJ Oral Rehabil2006331185086217002745
- GerritsenAEWitterDJBronkhorstEMCreugersNHAn observational cohort study on shortened dental arches – clinical course during a period of 27–35 yearsClin Oral Investig2013173859866
- McKennaGAllenFWoodsNCost-effectiveness of tooth replacement strategies for partially dentate elderly: a randomized controlled clinical trialCommunity Dent Oral Epidemiol201442436637424251386
- BabaKIgarashiYNishiyamaAPatterns of missing occlusal units and oral health-related quality of life in SDA patientsJ Oral Rehabil200835862162818699971
- FaggionCMJrGiannakopoulosNNListlSHow strong is the evidence for the need to restore posterior bounded edentulous spaces in adults? Grading the quality of evidence and the strength of recommendationsJ Dent201139210811621093527
- GuineyHWoodsNWheltonHMorganKPredictors of utilisation of dental care services in a nationally representative sample of adultsCommunity Dent Health201128426927322320064