
Abstract
Objective
The purpose of this study was to prospectively investigate the degree of pain experienced by the patients receiving transrectal ultrasonography (TRUS) of the prostate by applying a visual analog scale. We also identified the clinical parameters influencing pain during the TRUS examination.
Materials and methods
Records were obtained from a prospective database for male patients who received TRUS of prostate in the outpatient department of Chang Gung Memorial Hospital, Taiwan, from January 2014 to June 2014. The patients underwent a detailed physical examination and medical history review. Immediately after the TRUS examination, the patients completed questionnaires based on a ten-point visual analog pain scale. The variables of interest were age, body mass index, prostate volume, prostate sagittal length, prostate-specific antigen, previous TRUS experience, external hemorrhoids, anal surgical history, prostate calcification, and image artifact caused by stool in the rectum. All variables were correlated to the visual analog scale by applying multivariate regression analysis.
Results
By using linear regression analysis, we identified the independent factors that affected the pain score during the TRUS examination. The patients who received the examination for the first time or had longer prostate sagittal lengths, external hemorrhoids, anal surgical history, or stool stored in the rectum experienced more pain during the TRUS examination. Furthermore, the pain was reduced when we provided the patients with a detailed explanation before the procedure and allowed them to observe the real-time images during the examination.
Conclusion
Although a TRUS examination is uncomfortable for patients, after having identified the factors affecting pain, physicians can assist patients in reducing pain during the procedure, thus providing higher quality examinations.
Introduction
The first clinically applicable images of the prostate obtained through transrectal ultrasonography (TRUS) were described in 1967 by Watanabe et al.Citation1 Because ultrasound technology has become more refined over the years, the use of TRUS to evaluate prostatic disease has increased. By the mid-1980s, the 7 MHz ultrasound probe, which clearly delineates the architecture of the prostate, had become a standard diagnostic instrument.Citation2 TRUS can be used to detect prostate abnormalities such as benign prostatic hyperplasia, carcinoma of the prostate, prostatitis, prostatic abscess, and prostatic calculi.Citation3 However, a TRUS examination of the prostate is uncomfortable,Citation4 and some patients at Chang Gung Memorial Hospital have claimed that they experienced severe pain when receiving this invasive procedure. Although the degree of and factors influencing pain during TRUS-guided biopsy have been discussed in the literature,Citation5–Citation7 based on our research, no study has focused on the pain experienced by patients receiving TRUS of the prostate. The purpose of this study was to determine the manner in which patients experience the pain, and to identify the clinical parameters influencing the pain during a TRUS examination.
Materials and methods
This study was approved by the Institutional Review Board at Chang Gung Memorial Hospital, Taiwan. Records were obtained from a prospective database for male patients who received TRUS of the prostate in the outpatient department from January 2014 to June 2014. The patients underwent a detailed medical history review and physical examination. The patient’s age, body mass index, prostate-specific antigen level, previous anal operative history, and TRUS experience were recorded. When routine digital rectal examinations were performed, the anus was carefully inspected and the presence of external hemorrhoids was recorded. Patients with dementia, disabilities that interfered with verbal communication or neurological diseases that potentially influenced pain assessment, as well as patients who had prostatitis or who had received transurethral resection of the prostate were excluded. A total of 498 patients were enrolled in the study.
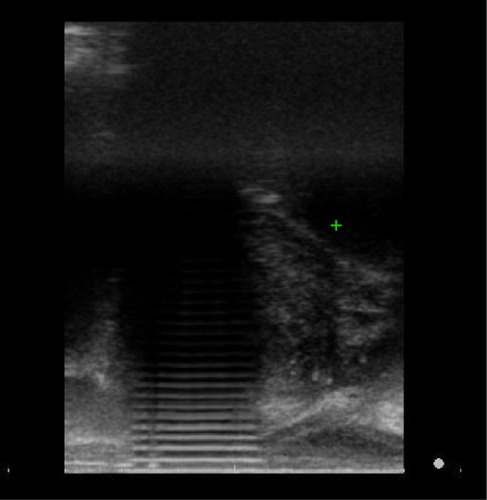
The patients were randomized into two groups according to medical chart number (odd, group 1; even, group 2). The group 1 patients received the TRUS examination according to the routine procedure of the hospital. By contrast, the group 2 patients received a detailed explanation of the examination procedure immediately before the examination began. In addition, a monitor was placed next to them, enabling them to observe the real-time images during the entire examination. Transrectal ultrasound was performed on the patients by a single urologist using an ultrasound machine (Prosound Alpha 6, Hitachi Ltd., Tokyo, Japan) fitted with a 7.5 MHz biplanar transrectal probe. The prostate volume was measured using the ellipse formula (sagittal length × width × height ×0.52). Whether the patients had stool stored in the rectum that interfered with the image quality () was recorded. Immediately following the examination, the patients completed a visual analog scale (VAS) questionnaire, evaluating the pain experienced during the TRUS on a scale of 0–10. After the patients rated the pain by marking a line to indicate pain level, a rounding method was used to obtain an integer.
Figure 1 Image shows artifact caused by stool stored in the rectum and interfered with the image quality. The examiner cannot easily measure the prostate sagittal length.
The pain score distribution was examined using the Kolmogorov–Smirnov test. The χ2 test was applied to test qualitative data, and the Mann–Whitney U-test was used to test numerical variables. All aforementioned variables were analyzed through linear regression analysis to identify the independent factors influencing the pain experienced during the procedure.
Results
The clinical characteristics of the patients are summarized in . The median patient age, prostate volume, and mean pain score was 63 years (range: 43–87), 32.40 g (range: 10.3–162.00), and 2.87 (range: 0–9), respectively. The distribution of the pain score is presented in . No pain (VAS =0) was reported by 53 patients (10.64%), mild pain (VAS =1–3) was described by 318 patients (63.86%), and moderate pain (VAS =4–5) was indicated by 107 (21.49%) patients. However, 60 patients (12.05%) reported experiencing severe pain (VAS =6–10) during the examination. The normal distribution of this result was confirmed through the Kolmogorov–Smirnov test ().
Figure 2 Distribution of pain score.
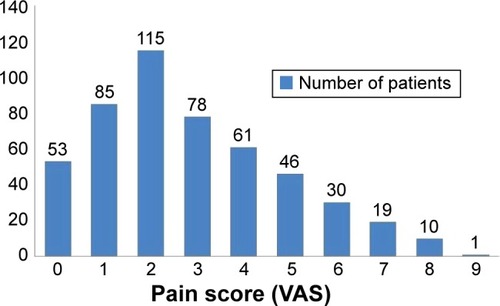
Figure 3 Kolmogorov–Smirnov test results showing that the pain score was normally distributed.
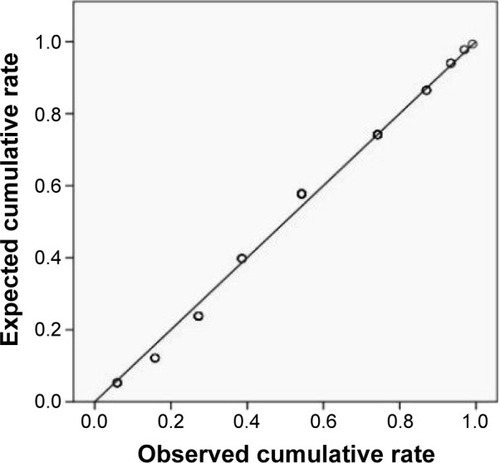
Table 1 Characteristics of the study population
When the patients were further subgrouped into two groups: VAS ≤3 and VAS ≥4, as shown in , we found that the patients who indicated VAS scores ≥4 were younger (63.04 vs 65.79, P=0.0293), had a larger prostate volume (43.04 g vs 37.41 g, P=0.0161), and longer prostate sagittal length (4.69 cm vs 4.56 cm, P=0.0415). The data also revealed that a lower percentage of patients whose VAS scores were ≥4 had TRUS experience (13.33% vs 23.85%, P=0.0427) and were randomly assigned to group 2 (34.91% vs 60.48%, P<0.0001), compared with patients with VAS scores of ≤3. By contrast, a higher percentage of patients with VAS scores of ≥4 had external hemorrhoids (59.09% vs 26.67%, P<0.0001), anal surgical experience (31.63% vs 6.96%, P<0.0001), and image artifact caused by stool (22.85% vs 11.79%, P=0.0068), as shown in .
Table 2 Comparison of patients’ numerical variables between pain score ≤3 and pain score ≥4
Table 3 Comparison of patients’ qualitative variables between pain score ≤3 and pain score ≥4
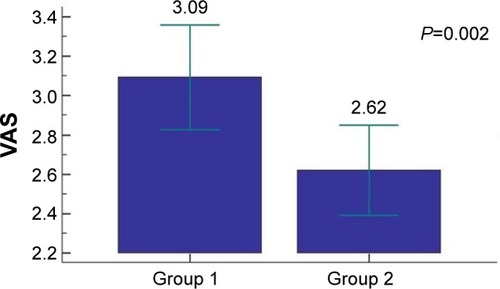
The group 2 patients had lower VAS scores than group 1 patients (2.62 vs 3.09, P=0.002), as shown in . In other words, the patients who received a detailed explanation of the procedure and were allowed to observe real-time images experienced less pain compared with the patients who did not.
Figure 4 Significantly lower pain scores of group 2 patients compared with those of group 1 patients.
Clinical parameters associated with TRUS that influenced VAS scores were analyzed (). Multivariate analysis revealed that the prostate sagittal length was the continuous variable influencing the level of pain. Assignment to group 2 and TRUS experience were negatively associated with the VAS score, whereas external hemorrhoids, anal surgical history, and image artifact caused by stool were independent factors that increased the VAS score.
Table 4 Multivariate analysis for the pain associated with TRUS using linear regression analysis
Discussion
The VAS is a simple assessment tool consisting of a 10 cm line with 0 on one end and 10 on the other.Citation8 Patients rate their pain by placing a mark on the line that corresponds to their current level of pain. The scale can be used as a baseline assessment of pain and to evaluate treatment effectiveness.Citation8 This scale has been widely used in many fields of pain research because it is easy to understand, requires less than 1 minute to complete, and has high validity and reliability.Citation9 Therefore, we applied the VAS in our study. Evaluating the degree of pain by using VAS and exploring the factors influencing pain during TRUS-guided biopsy have been discussed in the literature.Citation5–Citation7 However, based on our research, no study has focused on the pain experienced by the patients receiving TRUS of the prostate. Although the examination is considered an easy procedure by urologists and requires no local anesthesia, some patients claim to have experienced severe pain during the examination. Therefore, we focused on determining the pain scale distribution of the patients and identifying the factors influencing the pain. Our data revealed that the pain scores experienced by the patients were in a normal distribution, and the mean VAS score was only 2.87. This indicated that most of the patients tolerated the pain well and required no anesthesia during the procedure.
Our study revealed that patients with VAS scores of ≥4 were younger than the patients with VAS scores of ≤3 (63.04 vs 65.79, P=0.0293). Although multivariate analysis showed that the age was not a strong factor influencing the pain (P=0.0671; ), we maintain that age plays an influential role. Philips et alCitation10 and Rodriguez et alCitation11 have reported that older patients can tolerate pain more during a TRUS-guided prostate biopsy because of a relatively low anal resting tone. The internal anal sphincter provides approximately 60%–70% of the anal resting tone, whereas the external anal sphincter is responsible for 20%–30%; the remaining 10%–15% is attributed to expansion of the anal cushions, call hemorrhoids.Citation12–Citation15 Young patients have a relatively high resting anal tone and low anorectal compliance during probe insertion and withdrawal.Citation10–Citation11 Consequently, younger patients experience more pain during the procedure. Prostate configuration also played a crucial role in the pain during TRUS. Our results revealed that the prostate sagittal length, rather than the prostate volume, affected the pain level. Patients who had a longer prostate sagittal length experienced more pain because when measuring the prostate volume, the probe of the ultrasonography had to be inserted deeper in the rectum, causing more discomfort.
Patients with external hemorrhoids accounted for approximately 33.33% of the entire study population. Hemorrhoids are categorized as external hemorrhoids (distal to the dentate line), internal hemorrhoids (proximal to the dentate line), and mixed hemorrhoids (both proximal and distal). External hemorrhoids are more sensitive to pain, itching, and irritation than are internal hemorrhoids located proximal to the dental line.Citation16 During the TRUS examination, the external hemorrhoids of patients are irritated and are painful. According to our analysis, a higher VAS score was reported by patients with external hemorrhoids, which was an independent factor influencing the pain (). In addition, patients who had anal surgical history also reported a higher degree of pain during TRUS examination. Delayed anal scar tissue, fibrosis, asymptomatic stenosis, or even symptomatic stricture may occur after anal surgical procedures. The incidence of late anal stenosis is not too low and occurs in 4%–5% of patients receiving hemorrhoidectomy.Citation17 A previous study reported that fistulectomy can also induce anal fibrosis.Citation18 Although none of our patients mentioned having the aforementioned surgical complications, we determined that an anal surgical history reduced the compliance of the anal sphincter and, consequently, caused more pain during the probe insertion and withdrawal. Therefore, we suggest using a digital finger insertion with ample lubricant to rinse the dry anal canal, gradually dilating the anal sphincter to prevent anal sphincter spasms. The probe can be inserted slowly and gently after the resting anal tone decreases. Using this technique enables reducing the pain experienced during a TRUS examination by patients with external hemorrhoids or anal surgical history. Our study also revealed that patients experienced more pain when they had stool stored in the rectum that caused image artifact, possibly because the examiner had to obtain a higher quality image by shifting and adjusting the ultrasound probe position in the rectum. Therefore, we suggest that patients who have chronic constipation receive an enema before the procedure.
Czarnecki et al mentioned that pain is based on patient perceptions, which may be influenced by interrelated factors including the patient’s emotional and psychological state, level of anxiety, previous pain experience, understanding of the procedure, and medical condition and environmental factors.Citation19 This may explain why the patients who had previous TRUS experience experienced less pain during the procedure. Furthermore, explaining the examination and allowing patients to observe real-time images during the procedure reduced patient anxiety; thus, they experienced less pain. The study of Tarhan et al also revealed that video-based education about the procedure of TRUS biopsy can diminish patient anxiety.Citation20 Therefore, we suggest that a detailed explanation and the ability to observe real-time images of the procedure can significantly reduce the pain of an anxious patient.
There were some flaws and limitations in our study that are worth mentioning. First, some of the patients who received the examination potentially had prostate cancer. We did not further discuss whether prostate cancer would affect the degree of pain experienced by the patients. Second, although our study confirmed that anal surgical history was one of the independent factors influencing the pain associated with TRUS, some of the given history mainly relied on self-reporting rather than an accurate medical chart review. We were unable to understand how the pain associated with TRUS was affected by different anal surgical procedures, for example, hemorrhoidectomy, hemorrhoid ligation, fistulectomy, or fistulotomy. Last but not least, the diagnosis of external hemorrhoids was made by the inspection of an urologist rather than an anorectal specialist. As a result, the high incidence of external hemorrhoids among our patients was questionable.
Conclusion
Although a TRUS examination is uncomfortable for patients, we revealed that most of the study patients tolerated the pain and required no anesthesia during the procedure. However, 21.49% and 12.05% of the patients reported moderate pain and severe pain, respectively. Our study identified various independent factors influencing the pain associated with TRUS: prostate sagittal length, previous TRUS experience, external hemorrhoids, anal surgical history, and stool accumulation in the rectum. The aforementioned methods enable reducing discomfort. Furthermore, alleviating patient anxiety by providing a detailed explanation before the procedure and allowing patients to observe real-time images can reduce the pain.
Acknowledgments
This research was supported by grants from the Chang Gung Memorial Hospital (CMRPG3D0311, CMRPG392163, BMRP260) and the National Science Council, Taiwan (NSC 101-2314-B-182A-099-MY3).
Disclosure
The authors report no conflicts of interest in this work.
References
- WatanabeHIgariDTanahasiYDevelopment and application of new equipment for transrectal ultrasonographyJ Clin Ultrasound1974291984136630
- AlkanITürkeriLBirenTVolume determinations by transrectal ultrasonography in patients with benign prostatic hyperplasia: correlation with removed prostate weightInt Urol Nephrol1996285175239119637
- TerrisMKStameyTADetermination of prostate volume by transrectal ultrasoundJ Urol19911459849872016815
- Van PraetCDecaesteckerKHoebekePCorrelation between prostate volume measured by transrectal and suprapubic ultrasound: can we do without TRUS?Global congress on Prostate CancerMarseille, France13–14 June 2013
- SeymourHPerryMJALee-ElliotCPain after transrectal ultrasonography-guided prostate biopsy: the advantages of periprostatic local anaesthesiaBJU Int20018854054411678747
- von KnoblochRWeberJVargaZFeiberHHeidenreichAHofmannRBilateral fine-needle administered local anaesthetic nerve block for pain control during TRUS-guided multi-core prostate biopsy: a prospective randomised trialEur Urol20024150851412074792
- IraniJFournierFBonDGremmoEDoreBAubertJPatient tolerance of transrectal ultrasound-guided biopsy of the prostateBr J Urol1997796086109126093
- HuskissonECMeasurement of painLancet19742112711314139420
- HawkerGAMianSKendzerskaTFrenchMMeasures of adult pain: visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap)Arthritis Care Res201163S11S240S252
- PhilipJMcCabeJERoySDSamsudinACampbellIMJavlePSite of local anaesthesia in transrectal ultrasonography-guided 12-core prostate biopsy: does it make a difference?BJU Int200697226326516430625
- RodriguezAKyriakouGLerayELobelBGuilleFProspective study comparing two methods of anaesthesia for prostate biopsies: apex periprostatic nerve block versus intrarectal lidocaine gel: review of the literatureEur Urol200344219520012875938
- BennettRCDuthieHLThe functional importance of the internal sphincterBr J Surg19645135535714153389
- LestarBPenninckxFKerremansRThe composition of anal basal pressure. An in vivo and in vitro study in manInt J Colorectal Dis1989421181222746132
- FrencknerBEulerCVInfluence of pudendal block on the function of the anal sphinctersGut19751664824891150119
- GibbonsCPTrowbridgeEABannisterJJReadNWRole of anal cushions in maintaining continenceLancet1986184868868882870357
- JacobsDClinical practice. HemorrhoidsN Engl J Med20143711094495125184866
- SayfanJBeckerAKoltunLSutureless closed hemorrhoidectomy: a new techniqueAnn Surg20012341212411420479
- TheerapolASoBYNgoiSSRoutine use of setons for the treatment of anal fistulaeSingapore Med J200243630530712380728
- CzarneckiMLTurnerHNCollinsPMDoellmanDWronaSReynoldsJProcedural pain management: a position statement with clinical practice recommendationsPain Manag Nurs20111229511121620311
- TarhanHCakmakOUnalEThe effect of video-based education on patient anxiety in men undergoing transrectal prostate biopsyCan Urol Assoc J201481112