
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose
The purpose of this study was to evaluate a novel online education and coaching program to promote self-care among patients with heart failure. In this program, education and coaching content is automatically tailored to the knowledge and behavior of the patient.
Patients and methods
The evaluation of the program took place within the scope of the HeartCycle study. This multi-center, observational study examined the ability of a third generation telehealth system to enhance the management of patients recently (<60 days) admitted to the hospital for worsening heart failure or outpatients with persistent New York Heart Association (NYHA) Functional Classification III/IV symptoms. Self-reported self-care behavior was assessed at baseline and study-end by means of the 9-item European Heart Failure Self-care Behavior scale. Adherence to daily weighing, blood pressure monitoring, and reporting of symptoms was determined by analyzing the system’s database.
Results
Of 123 patients enrolled, the mean age was 66±12 years, 66% were in NYHA III and 79% were men. Self-reported self-care behavior scores (n=101) improved during the study for daily weighing, low-salt diet, physical activity (P<0.001), and fluid restriction (P<0.05). Average adherence (n=120) to measuring weight was 90%±16%, to measuring blood pressure was 89%±17% and to symptom reporting was 66%±32%.
Conclusion
Self-reported self-care behavior scores improved significantly during the period of observation, and the objective evidence of adherence to daily weight and blood pressure measurements was high and remained stable over time. However, adherence to daily reporting of symptoms was lower and declined in the long-term.
Introduction
Heart failure (HF) is highly prevalent and linked to increased incidence of hospital readmissions, poor quality of life, and mortality.Citation1 Management of HF is challenging and resource intensive. Encouraging patients and their caregivers to play a more active role in the management of the condition may be a cost-effective solution.Citation2 There is growing support for the concept and value of key self-care behaviors in HF, namely taking medication as prescribed, engaging in physical activity and exercise, monitoring signs and symptoms, and, where appropriate, following a low-salt diet and restricting fluid intake.Citation1 Effective self-care is associated with lower readmission and mortality rates.Citation3 It follows therefore that the promotion of self-care behaviors should benefit patients and health care systems alike.
To promote active participation in self-care management, patients and their caregivers should be provided with education on HF and ways to manage their condition themselves.Citation4 Education can be delivered in several settings: during the hospital stay, in outpatient clinics, in primary care, or at home. Usually, this is carried out in face-to-face sessions by health care professionals supported by leaflets or digital resources (eg, CD-ROM,Citation5 websites,Citation6 telehealth systems,Citation7 and tablet computersCitation8).
Nevertheless adherence to self-care behaviors in HF is low.Citation9,Citation10 There are several factors that may account for this. First, despite current guidelines, hospital/service provision of training and staff for HF education is insufficient to meet demands.Citation11–Citation13 Second, many patients with HF may have impaired cognitive function.Citation1,Citation14,Citation15 This makes learning new self-care skills problematic.Citation16 Third, some patients with HF are clinically depressed or experience depressive symptomsCitation17 that can undermine their motivation and ability to adopt new self-care routines.Citation1 Fourth, knowledge itself may not provide enough impetus and support to negotiate the considerable challenges of initiating and maintaining health behavior change.Citation18,Citation19
The aim of the HeartCycle project funded by the European Commission Seventh Framework program was to examine how telehealth systems can be employed to increase adherence to self-care behaviors in HF. The first stage of the HeartCycle project surveyed the provision of support for self-care among patients with HF. This revealed that, although education is often provided, there is little follow-up to support implementation of self-care skills. The main thrust of tele-health systems has been the monitoring of vital signs rather than patient motivation. Although some systems provided education,Citation20 no system incorporated a coaching program to support behavior change actively. Counseling of patients via telephone increases adherence but is time-consuming and may not be cost effective.Citation21–Citation23
With the aim of producing a less resource intensive approach, the HeartCycle project developed an innovative automated education and coaching (E&C) program integrated within a telehealth system. The rationale behind the program was to tailor the provision of information to the needs of the patient and offer an interactive coaching program to support them in the choice, adoption and maintenance of self-care behavior, and freeing the health care professional to deal with more complex issues arising from HF.
In this paper, we report the results of the component dealing with adherence to self-care behaviors and symptom reporting among HF patients using the HeartCycle E&C program in a multi-center observational study.
Patients and methods
Program summary
A detailed description of the E&C program has been published previously.Citation24 Briefly, based on the 2008 guidelines for the diagnosis and treatment of HF from the European Society of Cardiology,Citation25 we chose to offer education and coaching for daily monitoring of signs, physical activity, fluid restriction, low-salt diet, and medication intake. Other topics were addressed by education only (eg, alcohol consumption) or were left out of the program (eg, sexual activity and prognosis).
The program was offered to the patients via the Motiva Telehealth System (Philips, Böblingen, Germany). This system enables patients to measure vital signs (weight, blood pressure, heart rate), to answer symptoms questions, and to view trend-charts of vital signs and educational videos on their TV. Via a secure Internet connection, data are made available to the HF nurses, who assisted by decision support software, may adapt the care plan or call the patient.
The program’s behavior change model was based on the Heart Manual, a well-established, face-to-face, home-based cardiac rehabilitation approach.Citation26,Citation27 In this model, education and coaching are tailored to the knowledge and behavior of the individual patient. Coaching is offered for the self-care behaviors the patient is not engaged in, and education is provided when the patient has little knowledge of these behaviors. Coaching starts with assessing the patient’s readiness for change by letting the patient express how important self-care behaviors are, and how confident he or she is to engage in these behaviors. Patients are then guided through a goal-setting process that they conduct at their own pace through the support of the system. To raise commitment, patients set their own goals and make their own action plans. They report their progress in an electronic diary, allowing the system to provide appropriate weekly feedback. Only when patients repeatedly fail in adopting self-care behaviors do HF nurses intervene to offer help.
Coaching for daily monitoring of signs and symptoms was further tailored to the characteristics of these self-care behaviors. In particular, assessing the patient’s readiness for change was deemed not necessary since, based on previous experience with the Motiva system, adoption of these daily tasks was expected to be relatively easy. Furthermore, the goals of these behaviors were predefined: the patients were asked to measure weight and blood pressure and to answer a short questionnaire on breathlessness and edema every day. Finally, the patients did not need to self-report their progress on these behaviors in an electronic diary, since signs and symptoms data were stored automatically in the telehealth system.
Eligibility and study design
The E&C program was evaluated within the scope of the HeartCycle study that took place at three hospitals in the United Kingdom, Germany, and Spain. The aim of this multi-center, observational study was to investigate whether the management of patients with HF can be enhanced by a third generation telehealth system. Target doses of medicines were based on European Society of Cardiology guidelines, modified for the individual patient by an experienced clinician if necessary, after taking into account blood pressure, serum potassium, and renal function. Details of the phases of the study have been published elsewhereCitation24 but are not relevant to this report on self-care adherence.
The inclusion and exclusion criteria are shown in . Patients had been recently (<60 days) admitted for HF or were outpatients with persistent New York Heart Association (NYHA) III/IV symptoms. We did not formally screen for depression or cognitive dysfunction but as patients had to consent to participate in a relatively complex clinical study, patients with marked depression or obvious cognitive dysfunction will have been excluded. Moreover, patients were excluded from the study if in the investigators’ opinion, they were unable to operate or comply with the telehealth system.
Table 1 Inclusion and exclusion criteria for the HeartCycle study
The protocol was reviewed and approved by the ethics committee of each participating center. All patients provided written voluntary informed consent.
Data collection, instruments
Self-care behavior was measured at baseline and study end with the 9-item European Heart Failure Self-care Behavior Scale (EHFScB-9), which is a reliable and valid scale to measure self-care behavior.Citation28,Citation29 The items are rated on a 5-point scale between 1 (“I completely agree”) and 5 (“I completely disagree”).
Adherence to the three daily tasks (measuring weight, measuring blood pressure, and reporting of breathlessness, and edema) was determined by analyzing a de-identified copy of the telehealth system database. If patients measured their weight (or blood pressure) more than once per day, only one of these measurements was counted. The symptom questionnaire could be answered only once per day. The official enrollment and closure dates were used to determine the start and end of the patient’s monitoring period.
Statistical methods
The EHFScB-9 scores at baseline and study end were analyzed at an item level using a paired Student’s t-test. For each item, patients who answered “I completely agree” or “I agree” were considered adherent.Citation30
For each daily task, the objectively measured adherence was calculated as follows:
The number of expected data elements has been corrected for death, hospitalization, and other absence from home (eg, holidays). The overall adherence of all patients during the entire study was obtained by dividing the total number of received data elements (of all patients) by the total number of expected data elements (of all patients). For each patient, we calculated the adherence of the entire monitoring period, and per month. In the latter case, for each month, we used the number of received data elements in that month and the number of expected data elements in that month in the above formula.
Matlab 2013a and R version 3.1.2 were used for statistics and making illustrations.
Results
Patients’ characteristics
Of 123 patients enrolled (mean age 66±12 years, 79% men) (), most (66%) were in NYHA class III, indicating that they had marked limitation of physical activity.
Table 2 Baseline characteristics of the study population
Measured system usage
The patients were enrolled between January 2012 and March 2013. They were asked to use the system until the end of the study (June 30, 2013). Hence, patients enrolled in January 2012 could use the system for 18 months, but those enrolled in March 2013 only for 4 months.
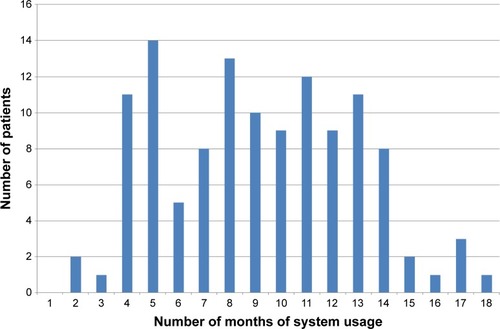
Of the 123 patients enrolled, three did not activate the system. The remaining 120 patients used the system for 9 months on average with a range of 2 to 18 months () with a total system usage of 1,101 patient-months. Ninety-seven patients used the system until the end of the study, and 23 patients discontinued before the end of the study due to death, increasing debility, or loss of interest.
Figure 1 The number of patients per number of months of system usage.
Self-reported self-care behavior at baseline and study end
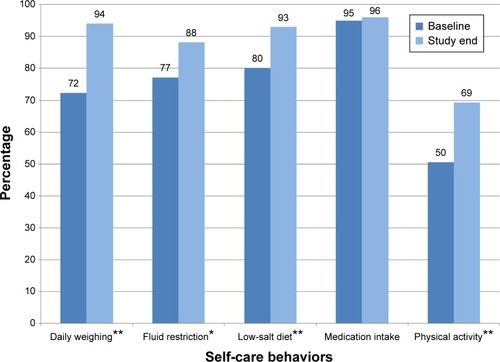
Data from the 101 patients with paired data from the EHFScB-9 questionnaire at baseline and study end showed improved adherence of all self-care behaviors except for medication intake (). The relative increase of adherence was 31% for daily weighing, 14% for fluid restriction, 16% for low-salt diet, and 38% for physical activity but only 1% for medication intake.
Figure 2 Percentage of adherent patients in the EHFScB-9 self-care behavior scale at baseline and study end (n=101).
Abbreviation: EHFScB-9, 9-item European Heart Failure Self-care Behavior Scale.
Differences in responses at baseline and study end per individual patient are shown in . For example, for daily weighing, 30 patients showed an adherence improvement from baseline to study end, the adherence of 61 patients remained the same, five patients showed a decline in adherence, and five patients gave an invalid answer at baseline or study end. All 61 patients who gave the same answer at baseline and study end for daily weighing, were adherent at both moments.
Table 3 Differences between the answers at baseline and study end for self-care behaviors measured with the EHFScB-9 scale (n=101)
Measured adherence to daily tasks
The overall and the average adherence of measuring weight and blood pressure was about 90% (). For daily reporting of symptoms, the overall and the average adherence was about 67%. The percentage of patients performing the daily task on ≥80% of the expected days was 88% for measuring weight, 85% for measuring blood pressure, and 50% for symptoms reporting.
Table 4 Objectively measured adherence per daily task (n=120)
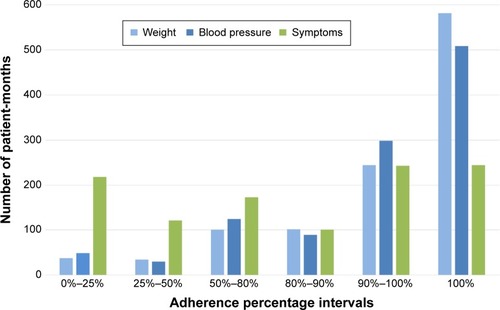
For measuring weight, adherence was 100% in 582 (of the 1,101) patient-months and between 90% and 100% in a further 244 patient-months (). For symptoms reporting, adherence was 100% in 244 patient-months, but between 0% and 25% in 218 patient-months.
Figure 3 Number of patient-months per adherence percentage interval (total number of patient-months =1,101).
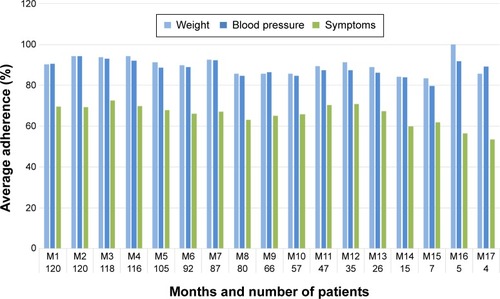
shows the average adherence over time of the three daily tasks. For example, 120 patients used the system for at least 1 month. The average adherence of measuring weight and blood pressure in the first month was 90%. For symptoms reporting the average adherence in the first month was 70%. A total of 92 patients used the system for at least 6 months. The average adherence percentage for measuring weight and blood pressure in month 6 was still about 90% but for symptoms reporting at month 6 this had dropped slightly to 66%.
Figure 4 Average adherence over time for weight, blood pressure, and symptoms reporting. The numbers at the horizontal axis denote the number of patients who were using the system in that month. Since month M18 had only one patient, this month has been excluded from the figure.
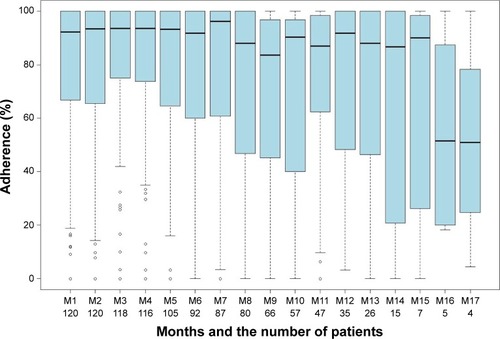
For measuring weight and blood pressure, adherence remained stable over time ( and ; the percentile details can be found in ). For symptoms reporting, adherence was stable for 6 months with a median of about 93%, and then started to decline (). After half a year, the variability for symptoms reporting became wider compared to both the variability in the preceding months and the variability for measuring weight and blood pressure.
Figure 5 Box-and-whisker plot for measuring weight. Vertical axis shows adherence. Horizontal axis shows the months and the number of patients who were using the system in that month. Month M18 has been excluded from the figure since only one patient was using the system for 18 months.
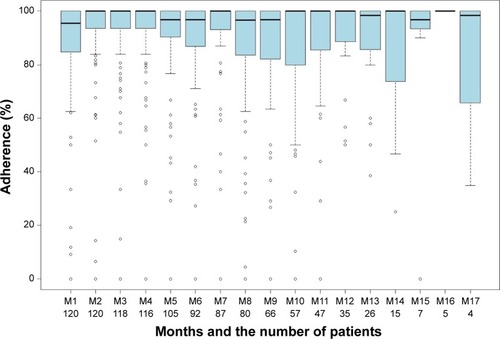
Figure 6 Box-and-whisker plot for measuring blood pressure. Vertical axis shows adherence. Horizontal axis shows the months and the number of patients who were using the system in that month. Month M18 has been excluded from the figure since only one patient was using the system for 18 months.
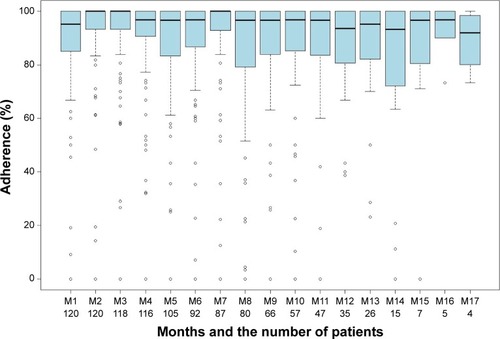
Figure 7 Box-and-whisker plot for symptoms reporting. Vertical axis shows adherence. Horizontal axis shows the months and the number of patients who were using the system in that month. Month M18 has been excluded from the figure since only one patient was using the system for 18 months.
Discussion
For all self-care behaviors except medication intake, self-reported, and self-care behavior scores improved significantly from baseline to study end (n=101). We assume that the automated coaching was the likely mechanism for this improvement; proof of this assumption in a randomized trial is the logical next step. The results are promising, especially when taking into account that most patients already received substantial conventional education preceding enrollment in the HeartCycle study, and that self-reported adherence of daily weighing, fluid restriction, and low-salt diet was already high at baseline (72%, 77%, and 80%, respectively).
Adherence to medication intake was very high in our study. This is in line with other studies that use self-report as a measure of medication adherence. Depending on the way of measurement, adherence levels for medication intake can vary between 10% and 98%.Citation10 More sensitive scales such as ProMASCitation31 or medication event monitoring systemsCitation32 may be used.
The objectively measured adherence of weight and blood pressure measurements is very high. It is encouraging that of the 1,101 patient-months of system usage, about half showed an adherence of 100% for weight and blood pressure monitoring.
Adherence to symptoms monitoring was lower compared to monitoring of weight and blood pressure, and started to decline after half a year. We did not systematically investigate the reasons for this. However, feedback provided by the study nurses revealed that some patients did not see the point in answering the short questionnaire on breathlessness and edema every day, especially when the intensity of their symptoms had not changed. Another reason could be that our program did not emphasize the value of symptoms reporting sufficiently and that patients perceived that there was no benefit in making the effort. When measuring weight or blood pressure, the system gives immediate feedback by providing information that the patient does not know yet. However, when reporting on symptoms, the patient has to enter information that he or she already knows into the system, but does not receive feedback on this. Receiving (personalized) feedback is essential in changing health behavior.Citation33
For daily weighing self-reported adherence at study end (94%) is only slightly higher than the objectively measured adherence. It should be noted that we used a conservative approach to determine the objectively measured adherence. In particular, we used the official enrollment and closure dates to determine the start and end of the monitoring period. However, in practice some patients started a few days later, or stopped a few days earlier. Three of our 123 patients (2.4%) did not activate the system. This is a considerably lower proportion of non-participation than reported in previous studies; for example in the Tele-HF study 14.4% of the patients never used the telemonitoring system.Citation34
In our study, 66% of the patients were in NYHA class III and 34% in NYHA class II. Since daily monitoring of signs and symptoms allows for the early detection of deterioration, it can be expected that with this program patients in NYHA class IV would show similar adherence to signs and symptoms monitoring. For the other self-care behaviors, it can be expected that the effectiveness of our program for class IV patients depends on the behavior. For example, since NYHA class IV patients have severe limitations with physical activity and are mostly bedbound, it can be expected that for these patients it will be difficult to increase their physical activity level.
Only a few studies have used the EHFScB-9 to study the effect of telehealth interventions on self-care behavior.Citation20,Citation35,Citation36 Two of these studies used the Motiva telehealth system offering vital signs monitoring, education, and motivational messages, but without the coaching program as described in this paper. The first study, with 214 patients and a mean follow-up of 288 days, found no differences in self-care behavior between the control group and the intervention group.Citation20 The RECAP study, in which 108 patients used the Motiva system during 42 days, found a significant difference between the EHFScB-9 total score at baseline and after 42 days.Citation35 For the individual items, significant differences were found for daily weighing, fluid restriction, and low-salt diet, but not for medication intake and physical activity. The TEHAF study investigated the effects of a telemonitoring system that offered dialogues and questions with variable emphasis on symptoms, knowledge, and behavior.Citation36 After 12 months, the total score of the intervention group had improved whereas the control group remained at the same level, which was a significant difference.
Several studies have reported on HF signs and symptoms monitoring adherence based on objective data collected by a telehealth system. Unfortunately, these studies use different adherence criteria. The TEMA-HF 1 study only reported overall adherence: 86% for measuring weight and 82% for measuring blood pressure on a daily basis.Citation37 In our study, these were 91% and 90%, respectively.
Most studies report an average adherence to a standard deviation ().Citation38–Citation42 For example, the TIM-HF study found an average adherence of 90.6% for blood pressure monitoring and 88.0% for symptoms reporting.Citation38 Another approach is to mention the percentage of patients monitoring signs or symptoms at least x% of the time. For example, in the CARME study 52.2% and 44.4% of the patients monitored weight and blood pressure respectively at least 80% of the time.Citation39 In both cases, the HeartCycle results are among the highest adherence percentages of measuring weight and blood pressure.
Table 5 Studies reporting on HF signs and symptoms monitoring adherence using telehealth system data
Four studies report on the combination of signs and symptoms monitoring.Citation34,Citation38,Citation43,Citation44 In the TEN-HMS study, where patients were asked to measure weight and blood pressure twice per day, 81% of the patients using the telehealth system had >80% adherence to at least one daily measurement (weight or blood pressure), and 55% had >80% adherence to twice daily measurements.Citation44 Worth mentioning is that in the Tele-HF study, by week 26 only 55% of the patients were still using the system at least three times per week (ie, 43% of the time).Citation34
The HeartCycle program is characterized by the fact that it provides automated coaching in the home context. Patients receive not only education about self-care behaviors, but also explicit support in adopting these behaviors. Furthermore, the HeartCycle program takes into account the dynamics of health behavior change by specifically addressing relapse. Patients who have relapsed are offered the opportunity to do the coaching program again.
So far, remarkably few programs offering automated coaching of HF self-care behaviors have been developed. We believe only one other study (CHF-CePPORT) designs and evaluates an e-platform for behavioral counseling and education to facilitate long-term adherence to self-care among patients with HF.Citation45 Similar to our program, it is based on motivational interviewing and cognitive-behavioral therapy.
Study limitations
This study has several limitations. HeartCycle was primarily designed to develop a novel telehealth system in collaboration with patients and a multi-disciplinary team of engineers and clinicians rather than to run a large randomized controlled trial. Development and evaluation of the education and coaching program was not the only objective of the study but this was also considered an iterative learning process followed by a pilot concept observational study that did not have a control group. Ideally, a control group receiving usual education on self-care should be compared with a group receiving only online education, and a group receiving both online education and coaching. The sample size for the HeartCycle study was calculated based on the number of patients required for one of the study phases.Citation24 Using three groups would require additional participants, which was beyond the available budget.
Second, this study did not assess whether the observed improvement in self-care adherence translated into improved outcome. This would require a larger randomized controlled trial.
Another limitation is that the patients were in the study for varying lengths of time. In particular, the time between the EHFScB-9 assessments at baseline and study end varied between 3 and 18 months.
Conclusion
Self-reported self-care behavior scores improved significantly from baseline to study end. Objectively measured adherence of daily weight and blood pressure measurements was very high and remained stable over time. Adherence to daily reporting of symptoms was lower and declined in the long-term.
The findings demonstrate that an automated education and coaching program, which is more scalable than human coaching, can be effective in improving self-care. A suggested next step is to compare this program with a control group receiving usual self-care education and a group receiving online education only, and to study the effect on clinical outcomes.
Acknowledgments
The authors gratefully thank W Armitage and M Clark for their contribution to the design of the program; B Schulte, K van Gelder, M Spanbroek, M van de Kamp, M Allmark, and A Tesanovic for the implementation of the program; and K Slottje, R Flockton, C Whitehead, P Atkin, P Gastelurrutia, M Domingo, and B Gonzalez Fernandez for performing the study. The authors thank H Reiter, C Westerteicher, A Bruege, U Goldbach, NK Bui, GJ de Vries, and A Rigby for their assistance. This research was supported by the European Commission under grant FP7-216695.
Supplementary material
Table S1 The details corresponding to the box-and-whisker plots in –
Disclosure
WS is employed by Philips. JGC has received research funding and honoraria for advice from Philips. CD and TJ report no conflicts of interest in this work.
References
- RiegelBMoserDKAnkerSDState of the science: promoting self-care in persons with heart failure: a scientific statement from the American Heart AssociationCirculation2009120121141116319720935
- ClelandJGEkmanIEnlisting the help of the largest health care workforce – patientsJAMA2010304121383138420858885
- LeeCSMoserDKLennieTARiegelBEvent-free survival in adults with heart failure who engage in self-care managementHeart Lung2011401122020561885
- McDonaghTABlueLClarkALEuropean Society of Cardiology Heart Failure Association Standards for delivering heart failure careEur J Heart Fail201113323524121159794
- StrömbergAAhlenHFridlundBDahlströmUInteractive education on CD-ROM – a new tool in the education of heart failure patientsPatient Educ Couns2002461758111804773
- OrlowskiJLOermannMHShaw-KokotJEvaluation of heart failure websites for patient educationAdv Emerg Nurs J201335324024623899948
- InglisSCClarkRAMcAlisterFAStructured telephone support or telemonitoring programmes for patients with chronic heart failureCochrane Database Syst Rev20108CD00722820687083
- Oosterom-CaloRAbmaTAVisseMAStutWTe VeldeSJBrugJAn interactive-technology health behavior promotion program for heart failure patients: Experiences and needs of patients and nurses in the hospital settingJMIR Res Protoc201432e3224945160
- JaarsmaTStrömbergABen GalTComparison of self-care behaviors of heart failure patients in 15 countries worldwidePatient Educ Couns201392111412023579040
- van der WalMHJaarsmaTAdherence in heart failure in the elderly: problem and possible solutionsInt J Cardiol2008125220320818031843
- JaarsmaTStrömbergADe GeestSHeart failure management programmes in EuropeEur J Cardiovasc Nurs20065319720516766225
- CawthonCWaliaSOsbornCNiesnerKJSchnipperJLKripalaniSImproving care transitions: the patient perspectiveJ Health Commun201217Suppl 331232423030579
- ManningSBridging the gap between hospital and home: a new model of care for reducing readmission rates in chronic heart failureJ Car-diovasc Nurs2011265368376
- SauvéMJLewisWRBlankenbillerMRickabaughBPresslerSJCognitive impairments in chronic heart failure: a case controlled studyJ Card Fail200915111019181287
- HarknessKHeckmanGAAkhtar-DaneshNDemersCGunnEMcKelvieRSCognitive function and self-care management in older patients with heart failureEur J Cardiovasc Nurs201413327728423733350
- PaulSHospital discharge education for patients with heart failure: What really works and what is the evidence?Crit Care Nurse200828668218378729
- FreedlandKERichMWSkalaJACarneyRMDávila-RománVGJaffeASPrevalence of depression in hospitalized patients with congestive heart failurePsychosom Med200365111912812554823
- MillerWRRollnickSMotivational Interviewing: Preparing People for ChangeNew YorkGuilford Press2002
- GollwitzerPMSheeranPImplementation intentions and goal achievement: a meta-analysis of effects and processesAdv Exp Soc Psychol20063869119
- BalkAHDavidseWDommelenPvTele-guidance of chronic heart failure patients enhances knowledge about the disease. A multi-centre, randomised controlled studyEur J Heart Fail200810111136114218790668
- GrancelliHVariniSFerranteDRandomized Study of Telephone Intervention in Chronic Heart Failure (DIAL): study design and preliminary observationsJ Card Fail20039317217912815566
- DunaganWCLittenbergBEwaldGARandomized study of a nurse-administered, telephone-based disease management program for patients with heart failureJ Card Fail200511535836515948086
- CourtneyMEdwardsHChangAParkerAFinlaysonKHamiltonKFewer emergency readmissions and better quality of life for older adults at risk of hospital readmission: a randomized controlled study to determine the effectiveness of a 24-week exercise and telephone follow-up programJ Am Geriatr Soc200957339540219245413
- StutWDeighanCArmitageWClarkMClelandJGJaarsmaTDesign and usage of the HeartCycle Education and Coaching Program for patients with heart failureJMIR Res Protoc201434e7225499976
- DicksteinKCohen-SolalAFilippatosGESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of CardiologyEur Heart J200829192388244218799522
- LewinBRobertsonIHCayELIrvingJBCampbellMEffects of self-help post-myocardial-infarction rehabilitation on psychological adjustment and use of health servicesLancet19923398800103610401349062
- ClarkMKellyTDeighanCA systematic review of the heart manual literatureEur J Cardiovasc Nurs201110131320451459
- JaarsmaTStrömbergAMårtenssonJDracupKDevelopment and testing of the European Heart Failure Self-Care Behavior ScaleEur J Heart Fail20035336337012798836
- JaarsmaTArestedtKFMårtenssonJDracupKStrömbergAThe European Heart Failure Self-care Behaviour scale revised into a nine-item scale (EHFScB-9): a reliable and valid international instrumentEur J Heart Fail20091119910519147463
- UchmanowiczILoboz-RudnickaMJaarsmaTLoboz-GrudzieńKCross-cultural adaptation and reliability testing of Polish adaptation of the European Heart Failure Self-care Behavior Scale (EHFScBS)Patient Prefer Adherence201481521152625382973
- KleppeMLacroixJHamJMiddenCThe development of the ProMAS: a Probabilistic Medication Adherence ScalePatient Prefer Adherence2015935536725784791
- NieuwenhuisMMJaarsmaTvan VeldhuisenDJvan der WalMHSelf-reported versus ‘true’ adherence in heart failure patients: a study using the Medication Event Monitoring SystemNeth Heart J2012207–831331922527915
- DiClementeCCMarinilliASSinghMBellinoLEThe role of feedback in the process of health behavior changeAm J Health Behav200125321722711322620
- ChaudhrySIMatteraJACurtisJPTelemonitoring in patients with heart failureN Engl J Med2010363242301230921080835
- VaronCAlaoMMinterJEffect of telehealth on self-care behavior of heart failure patientsComput Cardiol201441473476
- BoyneJJVrijhoefHJSpreeuwenbergMEffects of tailored telemonitoring on heart failure patients’ knowledge, self-care, self-efficacy and adherence: a randomized controlled studyEur J Cardiovasc Nurs201413324325223630403
- DendalePDe KeulenaerGTroisfontainesPEffect of a telemonitoring-facilitated collaboration between general practitioner and heart failure clinic on mortality and rehospitalization rates in severe heart failure: the TEMA-HF 1 (TElemonitoring in the MAnagement of Heart Failure) studyEur J Heart Fail201214333334022045925
- PrescherSDeckwartOKoehlerKWill telemonitoring be adopted by patients with chronic heart failure?Dtsch Med Wochenschr201413916829834 German24722932
- DomingoMLupónJGonzálezBEvaluation of a telemedicine system for heart failure patients: feasibility, acceptance rate, satisfaction and changes in patient behavior: results from the CARME (CAtalan Remote Management Evaluation) studyEur J Cardiovasc Nurs201211441041821402493
- LedwidgeMTO’HanlonRLalorLCan individualized weight monitoring using the HeartPhone algorithm improve sensitivity for clinical deterioration of heart failure?Eur J Heart Fail201315444745523204211
- LyngåPPerssonHHägg-MartinellAWeight monitoring in patients with severe heart failure (WISH). A randomized controlled studyEur J Heart Fail201214443844422371525
- de LusignanSWellsSJohnsonPMeredithKLeathamECompliance and effectiveness of 1 year’s home telemonitoring. The report of a pilot study of patients with chronic heart failureEur J Heart Fail20013672373011738225
- SetoELeonardKJCafazzoJABarnsleyJMasinoCRossHJMobile phone-based telemonitoring for heart failure management: a randomized controlled studyJ Med Internet Res2012141e3122356799
- ClelandJGLouisAARigbyASJanssensUBalkAHNoninvasive home telemonitoring for patients with heart failure at high risk of recurrent admission and death: the Trans-European Network-Home-Care Management System (TEN-HMS) studyJ Am Coll Cardiol200545101654166415893183
- NolanRPPayneAYMRossHAn Internet-based counseling intervention with email reminders that promotes self-care in adults with chronic heart failure: randomized controlled study protocolJMIR Res Protoc201431e524480783