
Abstract
Purpose
All current recommendations include calcium and vitamin D (Ca–D) as an integrated part of osteoporosis treatment. The purpose of this pilot study was to analyze compliance with a fixed combination of Ca–D in women persistent with the treatment.
Patients and methods
An observational study was carried out in three osteocenters in the Czech Republic. Women with osteoporosis ≥55 years of age concurrently treated with oral ibandronate were eligible. Compliance was evaluated in a period of 3 months by Medication Event Monitoring System (MEMS), tablet count, and self-report. Nonpersistence was defined as a MEMS-based gap in the use of Ca–D to be 30 days or more.
Results
A total of 73 patients were monitored, of which 49 patients were analyzed (target population). Based on MEMS, mean overall compliance was 71%; good compliance (≥80%) was observed in 59% of the patients. As many as 71% of the patients took drug holidays (≥3 consecutive days without intake); overall compliance of these patients was 59% and was slightly lower on Fridays and weekends. Patients without drug holidays were fully compliant (did not omit individual doses). Compliance differed according to daily time at which the patients mostly used the Ca–D. Afternoon/evening takers showed a mean overall compliance of 82% while morning/night takers only 51% (P=0.049). Based on MEMS, tablet count, and self-report, compliance ≥75% was observed in 59%, 100%, and 87% of the patients, respectively. Outcomes obtained by the three methods were not associated with each other. Undesirable concurrent ingestion of Ca–D and ibandronate was present only twice.
Conclusion
Despite almost perfect self-reported and tablet count-based compliance, MEMS-based compliance was relatively poor. Consecutive supplementation-free days were common; more than two-thirds of the patients took at least one drug holiday. This pilot study showed drug holiday to be the most important type of noncompliance with Ca–D in those who are persistent with the treatment.
Introduction
Osteoporosis is a silent systemic disease characterized by low bone mineral density and microarchitectural deterioration of bone tissue with increased fragility of bones. Osteoporosis and its consequences are a worldwide concern in the current aged society.Citation1
A variety of treatments are available to prevent and treat osteoporosis. The bisphosphonates alendronate, ibandronate, risedronate, and zoledronic acid; raloxifene; agents derived from parathyroid hormone; and denosumab and strontium ranelate are most commonly used in Europe.Citation1 All current recommendations include calcium and vitamin D (Ca–D) as an integrated part of osteoporosis treatment, which determines the success of antiresorptive and osteoanabolic therapy. Intakes of at least 1,000 mg/day of calcium and 800 IU of vitamin D can be recommended in the general management of patients with osteoporosis.Citation1
Despite ambiguities regarding the most appropriate supplementation doses and forms of supplements, combined Ca–D supplements in a daily dose of 0.5–1.2 g and 400–800 IU, respectively, are generally recommended in patients receiving bone protective therapy since the evidence for the efficacy of antiresorptives is mostly based on coadministration of Ca–D supplements.Citation1–Citation3 The use of a fixed combination of Ca–D in a single tablet should facilitate treatment adherence, especially if the patient also receives other treatments.Citation3,Citation4
Despite the availability of effective pharmacotherapy, approximately 50% patients with osteoporosis do not adhere to the treatment regimen and/or discontinue the treatment during the first year.Citation1,Citation5,Citation6 There is also a high prevalence of Ca–D insufficiency in the elderly.Citation7 Poor adherence to osteoporosis medication (compliance and persistence) is associated with smaller gains in bone mineral density and a significantly greater risk of fracture.Citation1,Citation8 While adherence to bisphosphonates has been extensively studied in common clinical practice,Citation5,Citation6 adherence to supplementation therapy escapes attention.
Supplementation with Ca–D was associated with a 12% reduction in the risk of fracture and 24% reduction in the risk of fracture in a population with a better adherence to the treatment.Citation3 However, adherence to supplementation therapy is low even in clinical trials.Citation9 Studies on adherence to Ca–D therapy in common practice are rare and are limited to persistence,Citation10 simple assessment by patient’s self-report,Citation11,Citation12 or database-based analysis of administrative data which rather reflect co-prescription rate.Citation13 In self-reported studies, patient compliance ranges between 30% and 75%.Citation11,Citation12,Citation14 Determinant factors of adherence to calcium and/or vitamin D treatment were patient’s attitude to the treatment, tolerability problems with the treatment, and the number of concurrent drugs.Citation12 Only one studyCitation14 used both objective and subjective methods, but it is limited to women initiating antiresorptive therapy. However, the character of noncompliance has not been studied in detail. Poor timing compliance such as concurrent ingestion of oral bisphosphonate and calcium can lead to adverse interaction resulting in significantly decreased absorption of the bisphosphonate.Citation1 We have previously pointed out that compliance with a postdose fasting interval could be a particular problem in patients treated with ibandronateCitation15 in which the interval of 60 minutes is twice as long as in other oral bisphosphonates, alendronate and risedronate. Further, taking into account the moderate overestimation of adherence by self-report,Citation16 it is important to study if self-reported adherence can be used in common practice to estimate compliance since it is practical, cheap, and suitable to realize in most settings.
The aim of the present analysis was therefore to study compliance with a fixed combination of Ca–D in women at risk of fracture who are persistent with such treatment. The primary objective was to study the character of noncompliance. The secondary objectives were to compare compliance obtained from the three methods, Medication Event Monitoring System (MEMS), tablet count, and self-report, and to study undesirable concurrent ingestion with oral ibandronate.
Methods
Study design
An observational pilot study was performed in consecutive secondary care female patients at risk of osteoporosis-related fracture.
Setting
Study participants were recruited from three outpatient osteocenters providing specialized care to patients with osteoporosis in the Czech Republic from May 2013 to October 2014. The osteoporosis centers were units of the following hospitals: University Hospital in Hradec Kralove, Institute of Rheumatology Prague, and Pardubice Regional Hospital.
Duration of the study
Patients were monitored for 3 months.
Participants
All patients fulfilling the eligibility criteria were asked to participate in the study. The inclusion criteria were as follows:
postmenopausal woman older than 55 years;
diagnosis of osteoporosis (measured by dual energy X-ray absorptiometry, bone mineral density measurement, T-score ≤−2.5 in the lumbar spine and/or hip region);
current treatment of osteoporosis with oral ibandronate;
treatment with oral bisphosphonate in an osteocenter for at least 2 years;
supplementation with a fixed combination of Ca–D, preparation Caltrate 600 mg/400 IU of vitamin D3 (start or continuation with the preparation). Only patients indicated for the calcium supplementation at the dose contained in one tablet, that is, 600 mg of calcium a day, were eligible.
Exclusion criteria were as follows:
use of a drug dispenser;
failure to adhere to the study protocol;
noninitiation with the Ca–D treatment;
nonpersistence with the Ca–D treatment.
These patients were not the target population of the study and were intended to be excluded from the analysis.
Outcome measures
In osteoporosis field, the term adherence is understood as both compliance (proximity to treatment recommendation often simplified as the number of doses taken divided by the number of prescribed doses) and persistence (how long the medication is taken).Citation1,Citation17 Based on this concept, we studied compliance-related outcomes in persistent patients. Based on MEMS data, nonpersistence was defined as a gap in the use of Ca–D to be 30 days or more.Citation18,Citation19
Primary outcome
The primary outcome was the character of noncompliance which was studied using MEMS. The MEMS is an electronic monitoring device intended for providing records on dosing history of drugs. The MEMS container consists of a bottle and a cap with a microprocessor. The cap registers the date and time of each opening of the container. The MEMS-based measures were adopted from literature and (if needed) adjusted to our scenario.Citation20–Citation23
Overall compliance: ratio of the number of container openings to the number of prescribed doses. The overall compliance can exceed 100%.
Correct dosing (days with correct number of doses, ie, one a day): percentage of the treatment days with one container opening. The correct dosing can reach a maximum of 100%.
Variability in time of drug intake: Ca–D was used in a regular time interval if 75% or more doses were used in the same time period, that is, regular takers. Among regular takers, we defined four categories. Morning takers took more than 75% of doses between 6 am and 12 am, afternoon takers between 12 am and 6 pm, evening takers between 6 pm and 12 pm, and night takers between 12 pm and 6 am. Participants who could not be classified as regular takers were referred to as variable takers.
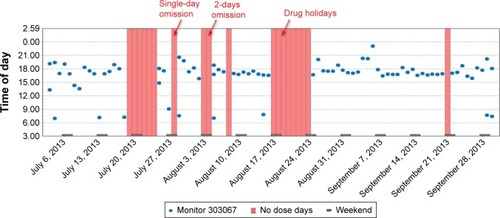
Single or sequentially missed multiple dosesCitation21 were classified as omissions of a dose on a single day, 2 consecutive days, and drug holidays. We defined the omission of a dose on a single day (24 hours) as Ca–D-free interval from 3 am to 3 pm. A similar rule was used to define the omission of more than 1 day ().
Drug holidays were defined as a sequence of at least 3 consecutive days without taking the drug.
Figure 1 Medication Event Monitoring System-based record of drug use in a particular patient covering a period of 3 months.
Secondary outcomes
We compared compliance (proportion of doses taken) using MEMS, tablet count, and patient’s self-report. Further, we examined potential concurrent ingestion of ibandronate and Ca–D.
Tablet count
After returning the MEMS container, the remaining tablets were counted by the researchers. Tablet count was defined as the number of tablets taken (not present in the container) expressed as the percentage of the correct number of tablets advised by the physician for the study period, that is, 90 tablets.Citation24,Citation25
Self-report
Patients responded the following questions in a one-page questionnaire:
How often did you take the Caltrate formula in the last 3 months? Response alternatives were: very often (more than 75% of the days), often (51%–75% of the days), sometimes (25%–50% of the days), and rarely or not at all (less than 25% of the days).
How many times did you miss a dose of Caltrate in the last month? (Open question).
Besides the questions on adherence, the questionnaire included also questions on the handling of the MEMS container, calcium-related gastrointestinal disorders, and the knowledge of the recommended daily intake of calcium.
Concurrent ingestion of Ca–D with ibandronate
Oral ibandronate should be taken after an overnight fast and 1 hour before the first food or drink (other than water) of the day or any other oral drugs or supplementation (including calcium). Calcium supplements are likely to interfere with the absorption of ibandronate. Therefore, patients should not take other oral drugs for 1 hour following the intake of ibandronate. The evaluation of concurrent ingestion of ibandronate and Ca–D was based on MEMS time of the use of Ca–D and self-reported time of ibandronate use recorded in the calendar. The concurrent ingestion was defined as use of Ca–D within 1 hour after the use of ibandronate.
Procedure
At baseline, each patient got a MEMS bottle containing 90 tablets of Ca–D (amount for 3 month-treatment) and a simple calendar for recording the use of oral ibandronate (the date and time of each use). All patients were instructed to take one tablet each day directly from the package and to bring the container with the rest of the tablets at the next visit. The day after the baseline visit, the patients started to be monitored.
At the check-up 3 months later, the patients returned the MEMS container, the calendar, and completed the short questionnaire. One day before the check-up visit, researchers sent a telephone reminder.
Data processing and statistical analysis
Data from the MEMS were transferred into a computer at the end of the study periods and processed using the PowerView 3.5.1 program (Aardex, Zug, Switzerland). All recorded container openings were considered to represent a single dose event.Citation26
Most variables did not follow a normal distribution and therefore nonparametric statistics were applied. The associations between variables were assessed using the following tests:
Kendall correlations for two continuous (ordinal) variables.
Mann–Whitney test for dichotomous and continuous (ordinal) variables.
Statistical analyses were calculated using PASW software (version 18.0). P<0.05 was considered statistically significant.
Ethics
The study protocol was approved by the ethical committees of the respective hospitals. Informed consent was required from all participants. Neither physicians nor patients were informed about individual study outcomes.
Results
Study population
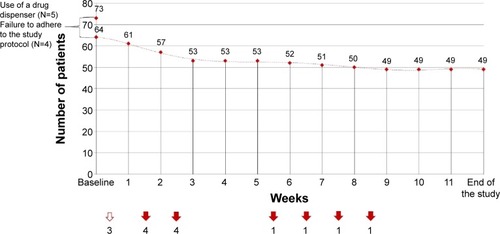
Five patients refused participation in the study. A total of 73 patients (94% of the target population) were recruited and monitored. As many as 24 patients were excluded due to prespecified exclusion criteria (), and 49 patients were available for the analysis.
Figure 2 Patients excluded from the study and reasons for their exclusion.
Basic characteristics of the studied population are summarized in .
Table 1 Characteristics of the study population (N=49)
Character of noncompliance
No multiple openings within a period of ≤15 minutes were observed. The overall compliance was 71% and the other compliance-related outcomes based on MEMS are summarized in . Characteristics of dosing omissions are presented in .
Figure 3 Omitted doses within single-day omission, 2-day omission, and drug holidays (%); all omitted doses represent 100%.
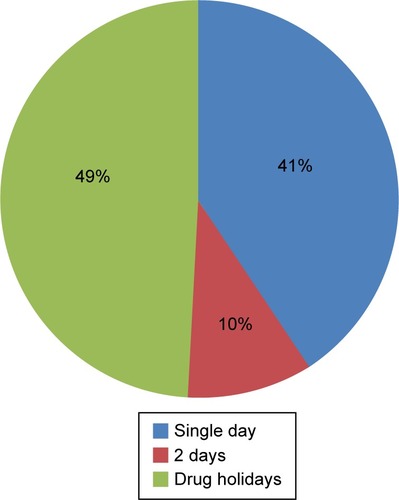
Table 2 Compliance-related outcomes based on Medication Event Monitoring System (N=49)
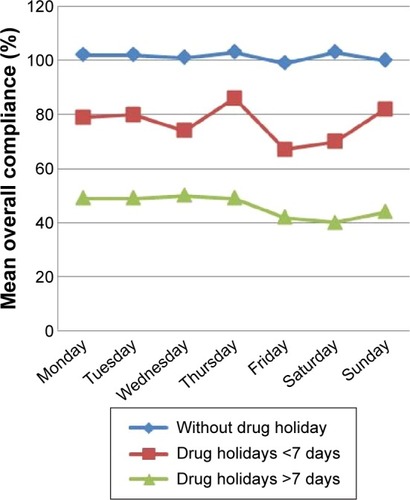
Patients without drug holidays were fully compliant (overall compliance was 101%), which means they practically did not omit doses. Overall compliance in patients with drug holidays was 59% and was slightly lower on Fridays and on weekends ().
Figure 4 Mean overall compliance according to presence of drug holidays at individual weekdays and weekends (%).
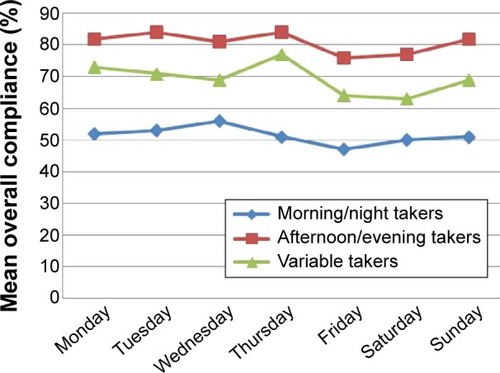
Periodic patterns in the execution of a dosing regimen were also analyzed. Overall compliance differed according to the daily time during which patients mostly used the drug (in 75% of cases or more). The subgroup of afternoon/evening takers (N=4/17) showed a mean overall compliance of 82% while the subgroup of morning/night takers (N=10/0) only 51% (P=0.049). Mean overall compliance in variable takers (N=18) was 70% ().
Figure 5 Mean overall compliance according to the category of takers at individual weekdays and weekends.
Comparison of compliance using MEMS, tablet count, and self-report
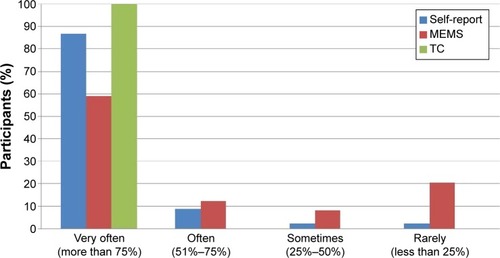
Categories of overall compliance based on the three methods in the whole study period are compared in . Mean overall compliance in the last month of the study was 72% and 97% when using MEMS and self-report, respectively. Compliance-related outcomes derived from the three methods were not associated with each other.
Figure 6 Categories of overall compliance with calcium/vitamin D supplementation in the cohort of 49 participants in the whole study period (3 months).
Concurrent ingestion of ibandronate and Ca–D
The concurrent ingestion was recorded only in two patients, once in each patient.
Discussion
This was a 3-month prospective study on electronically monitored compliance with osteoporosis supplementation therapy with retrospective self-evaluation of the compliance. The study was designed to be very close to common clinical practice and was focused on compliance with fixed combination of Ca–D in persistent female patients only. Despite almost perfect self-reported and tablet count-based compliance, MEMS-based compliance was relatively poor, which stresses the importance of objective methods in the measurement of compliance. Compliance better than 80%, often referred as cut point of good compliance,Citation5 was achieved in 60% of participants only. This number seems particularly low in the light of the fact that the study focused specifically on the implementation component of compliance; noninitiation and early discontinuation which can further decrease adherence to the treatment were not studied.Citation20 More than two-thirds of patients took at least one drug holiday (3 or more consecutive days without intake) and 43% took drug holiday longer than a week. This shows the implementation of the dosing regimen, that is, habit of taking once daily one tablet is not fixed well in most participants. About half of all dose-free days were part of drug holidays. These findings made drug holidays a leading problem in compliance with Ca–D in persistent patients in our pilot study. Bioavailability of oral ibandronate is reduced in the presence of calcium which interferes with absorption of ibandronate. Patients are probably very well informed and aware of this since undesirable concurrent ingestion of ibandronate and Ca–D, which can cause an interaction and potentially decrease the effect of ibandronate, was rare.
To our knowledge, this is the first study in which patient compliance with Ca–D was evaluated by a combination of both objective and subjective methods. Electronic medication-event monitoring which consists of automatic compilation of the time history of each patient’s entry into the drug package has been considered to provide the most reliable data on compliance.Citation27 However, it is relatively expensive and difficult to be used in common clinical practice. Therefore, methods that correlate with MEMS and are easier to perform can be of great importance for clinical practice.
However, appropriateness of the use of questionnaire instruments is sometimes questionable. The differentiation between an effect indicator model (all items in an instrument measure the same construct) and causal indicator model (the items measure unique, additive components of adherence) is crucial. Current multi-item tools, that is, validated questionnaires, can raise a question on what is actually measured (adherence only or a mixture of adherence, attitudes to the treatment, beliefs, preferences, and intentions).Citation28 Our particular interest was to formulate simple questions which express exactly the same measure as MEMS, that is, behavior (not intentions or attitudes) and omission of doses in the study period. Our questionnaire besides other items contained two simple questions on compliance with four response alternatives to avoid central tendency.
Discrepancy between MEMS and the other methods (the self-evaluation and tablet count) raises considerations regarding bias. Self-reported questionnaires usually overestimate adherence. Based on works of Shi et al,Citation16,Citation29 self-report compared to MEMS overestimates adherence by 10%–20%, but the methods are at least moderately correlated with each other.Citation16,Citation24 The over-reporting is generally attributed to social desirability bias and poor recall (for forgotten events). However, our difference between MEMS and other methods used (self-report and tablet count) is even higher, more than 25%. This can be explained as follows: 1) social desirability bias regarding self-report and tablet count is larger than in other similar studies and 2) MEMS measurement was free of Hawthorne bias.
Most studies comparing MEMS and self-report are from the USA or focused on the treatment of HIV.Citation16,Citation29 Social desirability bias can vary according to the setting, health care system, and cultural background. It could be more remarkable in post-communist countries and associated with perceived paternalism in medical decision making. Our present findings are in accordance with former Czech studies evaluating patient compliance with chronic conditions directly at clinics. Despite anonymity of the respondent, self-reported quantitative compliance (questions on doses used or missed) was almost always very high.Citation15,Citation30–Citation32 Social desirability is probably the dominant reason why our participants not only overrated their compliance by the questionnaire, but also spilled tablets out of MEMS and returned empty containers in most cases.
Hawthorne effect refers to those patients who overestimate their adherence when they know they are monitored.Citation33 This is apparent in the study on compliance with cardiovascular medication; correct dosing was 77% versus 59% in patients with and without information on the purpose of the electronic pillbox, respectively.Citation34 In most MEMS-based studies, participants were informed they are electronically monitored on medication adherence.Citation23,Citation24,Citation34,Citation35 MEMS-based adherence in most of these studies was relatively close to self-reported adherence.Citation16,Citation23,Citation24 We did not arouse the impression of electronically-mediated monitoring of compliance, so we believe the Hawthorne effect was practically absent in our study. Two studies in which monitoring of adherence was not suspectedCitation34,Citation35 also found out larger difference between MEMS-based and self-reported adherence; correct dosing of 59% versus 79%Citation34 and 90% versus 100%,Citation35 respectively.
Our almost perfect self-reported and tablet count-based compliance resulted in the uniformity of the respective variables; therefore, the impact of correlation, which showed no relationship among the methods, was weak.
The question remains how to easily and accurately estimate quantitative compliance in common practice. Social desirability seems to be a leading problem even in anonymous questionnaires completed directly at clinics.
In most MEMS-based studies on chronic treatment, patient compliance was higherCitation16,Citation23,Citation24,Citation34 than in our study. In a few studies, compliance was lower.Citation16,Citation34 Nevertheless, our study included persistent patients only.
In the study by Vrijens et al,Citation21 almost 5,000 hypertensive patients were monitored for 12 months. As much as 43% of doses were omitted within drug holidays. Our participants possibly considered their treatment less important, like supplementary therapy, and therefore even more, half of all doses, were omitted within drug holidays. As observed in the study on adherence with mesalazine in patients with ulcerative colitis,Citation24 our adherence was slightly higher before the check-up visit in the third month compared to the second.
In MEMS-based studies, lower adherence to long-term treatment is observed on weekends and possibly on Fridays.Citation21,Citation24,Citation26 In our study, slightly lower overall compliance was also observed on Fridays and Saturdays. We suppose that Fridays do not fit into the common daily routine, but Sundays do, because the patients used Ca–D in the afternoon/evening based on their physician’s recommendation.
Patients are usually instructed to use the Ca–D supplementation in the afternoon or evening by a prescribing physician. Our MEMS-based data are in accordance with the recommendation. Almost a half of patients used the supplementation mostly at this daily time; this subgroup, not surprisingly, showed better overall compliance. Similarly, considering the fact that antihypertensives are mostly recommended to be used in the morning, morning takers were most compliant with their treatment in the above mentioned study on adherence in patients with hypertension.Citation21
Our pilot study was relatively small, limited by the effort to capture as much homogeneous sample of patients as possible. To limit potential bias, we tried to keep the “naturalistic” character, that is, to organize the study in a way that is as much close to common clinical routine as possible.
Although it is still possible that patients did open the cap but did not actually take their medication, the MEMS may be less vulnerable to social desirability particularly when patients do not suspect they are monitored.
As the participants were recruited directly from the osteocenters, they may be more motivated to cooperate with physicians. The participants are likely to comply better with the treatment regimen than those who refuse participation in studies; therefore, patient compliance could be even slightly overestimated. Further, the participants were recruited from large osteocenters where the most specialized care and intensive counseling is provided.
Conclusion
Good compliance with a fixed combination of Ca–D was observed in 60% of persistent participants; consecutive supplementation-free days were common making drug holidays the most important type of noncompliance in our pilot study. In common clinical practice, emphasis should be placed on adequate support of compliance and ensuring the recommended daily intake of Ca–D in patients at risk of osteoporotic fracture. Self-reported evaluation of missed doses was highly overestimated and did not provide a real picture of patient compliance. A larger study is needed to confirm these preliminary findings.
Acknowledgments
We are grateful to Dr Bernard Vrijens for consultation on electronically-compiled dosing histories and sharing his profound, wide-ranging experience in medication adherence research. The authors would like to thank the physicians for patient recruitment: Prof Karel Pavelka, MUDr Olga Ruzickova, and MUDr Tomas Hala; further, thanks to Prof Jiri Vlcek for support of the MEMS method, Vera Holkova who assisted in study organization and data collection, and Mgr Michal Urbanek for English editing. The study was supported by Charles University in Prague, project SVV 260 187, and Program MH CZ – DRO (UHHK, 00179906).
Disclosure
The authors report no conflicts of interest in this work.
References
- KanisJAMcCloskeyEVJohanssonHCooperCRizzoliRReginsterJYEuropean guidance for the diagnosis and management of osteoporosis in postmenopausal womenOsteoporos Int2013241235723079689
- StromOBorgstromFKanisJAOsteoporosis: burden, health care provision and opportunities in the EU. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA)Arch Osteoporos201161–25915522886101
- TangBMEslickGDNowsonGDSmithCBensoussanAUse of calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years or older: a meta-analysisLancet200737065766617720017
- BangaloreSKamalakkannanGParkarSMesserliFHFixed-dose combinations improve medication compliance: a meta-analysisAm J Med2007120871371917679131
- CramerJAGoldDTSilvermanSLLewieckiEMA systematic review of persistence and compliance with bisphosphonates for osteoporosisOsteoporos Int20071881023103117308956
- KothawalaPBadamgaravERyuSSystematic review and meta-analysis of real-world adherence to drug therapy for osteoporosisMayo Clin Proc2007821493150118053457
- BruyèreOMalaiseONeuprezAColletteJReginsterJYPrevalence of vitamin D inadequacy in European postmenopausal womenCurr Med Res Opin2007231939194417631697
- RossSSamuelsEGairyKIqbalSBadamgaravESirisEA meta-analysis of osteoporotic fracture risk with medication nonadherenceValue Health20111457158121669382
- BrunnerRDunbar-JacobJLeboffMSPredictors of adherence in the women’s health initiative calcium and vitamin D trialBehav Med200934414515519064373
- GiustiA1BaroneARazzanoMPersistence with calcium and vitamin D in elderly patients after hip fractureJ Bone Miner Metab20092719510019018453
- Castelo-BrancoCCortésXFerrerMTreatment persistence and compliance with a combination of calcium and vitamin DClimacteric201013657858419951084
- Sanfelix-GenovésJGil-GuillénVFOrozco-BeltranDDeterminant factors of osteoporosis patients’ reported therapeutic adherence to calcium and/or vitamin D supplements: a cross-sectional, observational study of postmenopausal womenDrugs Aging2009261086186919761279
- ReymondierACailletPAbbas-ChorfaFMENOPOST – calcium and vitamin D supplementation in postmenopausal osteoporosis treatment: a descriptive cohort studyOsteoporos Int201324255956622588183
- DíezACarbonellCCalafJCalotoMTNoceaGObservational study of treatment compliance in women initiating antiresorptive therapy with or without calcium and vitamin D supplements in SpainMenopause2012191899521934533
- VytrisalovaMTouskovaTLadovaKAdherence to oral bisphosphonates: 30 more minutes in dosing instructions matterClimacteric20151819
- ShiLLiuJFonsecaVWalkerPKalsekarAPawaskarMCorrelation between adherence rates measured by MEMS and self-reported questionnaires: a meta-analysisHealth Qual Life Outcomes2010819920836888
- DeziiCMPersistence with drug therapy: a practical approach using administrative claims dataManag Care200110424511236643
- SchousboeJTDowdBEDavisonMLKaneRLAssociation of medication attitudes with non-persistence and non-compliance with medication to prevent fracturesOsteoporos Int2010211899190919967337
- HadjiPClausVZillerVIntorciaMKostevKSteinleTGRAND: the German retrospective cohort analysis on compliance and persistence and the associated risk of fractures in osteoporotic women treated with oral bisphosphonatesOsteoporos Int20122322323121308365
- VrijensBDe GeestSHughesDAA new taxonomy for describing and defining adherence to medicationsBr J Clin Pharmacol201273569170522486599
- VrijensBVinczeGKristantoPUrquhartJBurnierMAdherence to prescribed antihypertensive drug treatments: longitudinal study of electronically compiled dosing historiesBMJ200833676531114111718480115
- KardasPCompliance, clinical outcome, and quality of life of patients with stable angina pectoris receiving once-daily betaxolol versus twice daily metoprolol: a randomized controlled trialVasc Health Risk Manag2007323524217580734
- ZellerASchroederKPetersTJAn adherence self-report questionnaire facilitated the differentiation between nonadherence and nonresponse to antihypertensive treatmentJ Clin Epidemiol200861328228818226752
- GillespieDHoodKFarewellDStensonRProbertCHawthorneABElectronic monitoring of medication adherence in a 1-year clinical study of 2 dosing regimens of mesalazine for adults in remission with ulcerative colitisInflamm Bowel Dis2014201829124284414
- FiniganJNaylorKPaggiosiMAPeelNFEastellRAdherence to raloxifene therapy: assessment methods and relationship with efficacyOsteoporos Int201324112879288623695420
- CalsJWHopstakenRMLe DouxPHDriessenGANelemansPJDinantGJDose timing and patient compliance with two antibiotic treatment regimens for lower respiratory tract infections in primary careInt J Antimicrob Agents200831653153618457936
- OsterbergLBlascheTAdherence to medicationN Engl J Med2005353548749716079372
- VoilsCIHoyleRHThorpeCTMaciejewskiMLYancyWSJrImproving the measurement of self-reported medication nonadherenceJ Clin Epidemiol20116425025421194887
- ShiLLiuJKolevaYFonsecaVKalsekarAPawaskarMConcordance of adherence measurement using self-reported adherence questionnaires and medication monitoring devicesPharmacoeconomics201028121097110721080735
- HendrychovaTVytrisalovaMSmahelovaAVlcekJKubenaAAAdherence in adults with type 1 diabetes mellitus correlates with treatment satisfaction but not with adverse eventsPatient Prefer Adherence2013786787624043930
- VytrisalovaMBlazkovaSPalickaVSelf-reported compliance with osteoporosis medication – qualitative aspects and correlatesMaturitas200860322322918774663
- LadovaKMatoulkovaPZadakZSelf-reported adherence by MARS-CZ reflects LDL cholesterol goal achievement among statin users: validation study in the Czech RepublicJ Eval Clin Pract201420567167724917035
- McCambridgeJWittonJElbourneDRSystematic review of the Hawthorne effect: new concepts are needed to study research participation effectsJ Clin Epidemiol201467326727724275499
- ZellerARamseierETeagtmeyerABattegayEPatients’ self-reported adherence to cardiovascular medication using electronic monitors as comparatorsHypertension Res2008311120372043
- NieuwenhuisMMJaarsmaTvan VeldhuisenDJvan der WalMHSelf-reported versus ‘true’ adherence in heart failure patients: a study using the medication event monitoring systemNeth Heart J2012207–831331922527915