
Abstract
Purpose
To evaluate adverse drug reactions (ADRs) experienced by chronic myeloid leukemia (CML) patients during per oral tyrosine kinase inhibitor (TKI) treatment and correlation of ADR symptoms with medication adherence and perceived quality of life (QoL).
Patients and methods
Eighty-six adult, chronic-phase CML patients who had been on TKI treatment (79% on imatinib, 10.5% dasatinib, and 10.5% nilotinib) for at least 6 months participated in the study (mean age: 57.8 years, 52% males). The mean time from diagnosis was 5.1 years. All patients were interviewed, and patient-reported ADRs were obtained using a structured list. Adherence was assessed using Morisky’s 8-item Medication Adherence Scale (MMAS). The symptoms’ interference with patient’s daily QoL was measured by asking patients about the influence of symptom(s) on their mood, general condition, enjoyment of life, walking, relationships, and work.
Results
Ninety-seven percent of the patients were suffering from at least one ADR. The mean number of different symptoms was seven (range: 0–15, median 6). The most commonly perceived ADRs were muscle soreness or cramp (69/86, 80%); swelling of hands, legs, feet, or around the eyes (59/86, 69%); and fatigue (43/86, 50%). No correlation was found between adherence and ADRs, because symptoms were equally common in each MMAS adherence class. Half of the patients felt that the ADRs had a negative influence on their daily QoL. A quarter of the patients reported that ADRs affected either their mood, general condition, or enjoyment of life. The incidence of almost all ADRs was much higher among patients reporting negative influence of ADRs on their daily life compared to total study population (P=0.016).
Conclusion
TKI-related ADRs were common among CML patients irrespective of patient’s adherence level. Patients who reported that ADRs had a negative influence on their daily QoL perceived more ADRs than those who did not experience a negative influence.
Introduction
Chronic myeloid leukemia (CML) is a clonal disease of hematopoietic stem cells and is characterized by the presence of the Philadelphia chromosome and its oncogenic product p210 (Bcr-Abl).Citation1 The treatment of CML has dramatically changed over the last decade with the development of targeted therapy tyrosine kinase inhibitors (TKIs). CML patients treated with TKIs have good survival rates: patients treated with imatinib have been shown to have an estimated overall survival rate of 85% after 8-years’ follow-up.Citation2 Patients treated with TKIs need to continue treatment on a daily basis for their entire life to control the disease.Citation3 With current TKI therapies, the average rate of progression is approximately 1% per year.Citation2,Citation4–Citation7 This means that the symptom burden associated with TKI therapy generally has a greater effect on the patients’ daily life than the symptom burden of this progressive disease.Citation8 Several adverse drug reactions (ADRs) related to TKI therapy in CML are common to all TKIs, including myelosuppression, rash, nausea, diarrhea, fatigue, and musculoskeletal pain/arthralgia/myalgia, which occur at varying frequencies depending on the TKI in question.Citation4–Citation6
The need for continuous, potentially lifelong treatment with TKIs requires a high degree of patient perseverance for long-term disease control. The levels of adherence to TKI therapy among patients with CML have been found to be low.Citation9–Citation13 When asked about their poor adherence to imatinib therapy, CML patients report numerous reasons, both unintentional (forgetfulness, prescribing error, drug availability), and intentional (side effects, social events, travel, temporary illness, negative feelings, medication taste).Citation14 Eliasson et alCitation14 have also found that patients who reported intentional reasons for nonadherence had greater symptom severity than patients who reported unintentional reasons. Marin et alCitation10 found significantly lower rates of adherence to imatinib among patients who reported ADRs.
A standardized collection of health-related quality of life (QoL) data and other patient-reported outcomes (PROs) has contributed to a better understanding of overall treatment effectiveness in patients with solid tumors,Citation15,Citation16 but such evidence is lacking in patients with leukemia.Citation17,Citation18 PROs are defined by the FDA as “a measurement of any aspect of a patient’s health status that comes directly from the patient” (ie, without the interpretation of the patient’s responses by a physician or anyone else).Citation19 Documenting QoL and the adverse effects of CML treatments from the patients’ perspective is necessary to evaluate overall treatment effectiveness and the net clinical benefits of newer therapeutic strategies.Citation20 A patient-centered approach to determining the symptoms most relevant to patients with CML is supported by recent findings showing that health-care providers tend to underestimate the intensity of symptoms felt by patients with advanced cancer.Citation21 While the impact of TKIs from the patient’s perspective has been little investigated, PROs could be critical for making more informed treatment decisions, as all TKIs seem to provide similar excellent clinical outcomes.Citation4,Citation6 More attention has been placed on understanding the impact of symptom burden on patient QoL. At the moment, however, validated instruments to measure QoL in CML patients are not widely available or regularly used in clinical research or routine practice.
The aim of this study was to investigate patient-reported ADRs and their influence on adherence and QoL among CML patients on per oral TKI treatment.
Patients and Methods
Patient population
The study period was from June 2012 to September 2013. Eighty-six adult chronic-phase CML patients who had been on TKI treatment for at least 6 months were enrolled from eight secondary and tertiary care hospitals in Finland. All recruited patients gave their written informed consent before participating in the study. The study protocol was approved by HUS Ethics Committee of Medicine, and the ethics committees of the other concerned hospitals.
Patient interviews
All patients were interviewed in person by one of the researchers (MK), using a structured interview form. Each patient’s demographic data were collected during the interview. The interviews were digitally recorded, transcribed verbatim, and the results analyzed.
Adherence
Patient adherence was measured at the beginning of the interview using Morisky’s 8-item Medication Adherence Scale (MMAS)Citation22 validated for Finnish speakers.Citation12 MMAS is a structured questionnaire validated to estimate adherence to treatment and is widely used in chronic diseases.Citation22 The 8-item scale consists of seven questions with “yes” or “no” alternatives and one item (the last one) with a 5-point Likert scale. MMAS evaluates items addressing the circumstances surrounding adherence behavior.Citation22 Each item measures a specific medication-taking behavior and not a determinant of adherence behavior. MMAS scores can range from 0 to 8 and have been classified into three levels of adherence: high adherence (score 8), medium adherence (score 6–7.75), and low adherence (score <6).Citation22 MMAS questions related to intentional adherence and symptoms were separately analyzed.
ADRs
Patient-reported ADRs were assessed during the interview using a structured questionnaire. The questionnaire consisted of a list of 19 CML and TKI treatment-specific symptoms, and six items assessing the symptoms’ interference with the patient’s daily life (QoL). Patients were asked about the ADRs they experienced at the time of the study using a list of symptoms collected from the most common ADRs caused by TKIs in Phase III studies. The interviewer followed the standardized symptom inventory questionnaire, and every symptom was investigated by asking, “After the start of the TKI treatment have you suffered or are you currently suffering from the (mentioned) symptom?” The following alternatives were given: 1) not applicable; 2) has suffered before, but not at the moment (these answers were not included in the analysis); or 3) yes, I am currently suffering from this symptom (included in the analysis). The number of patient-reported ADRs was considered as a “symptom score”, each reported symptom yielding one score (score range: 0–1).
QoL
The patient interview also included six structured questions assessing functional impairment associated with TKI treatment (QoL). QoL was assessed as a negative influence of patient-reported ADRs on six items: mood, general condition, enjoyment of life, walking, relationships, and work in general. Each item scored one point (ie, the patient answered “yes”), leading to a maximum score of 6. This was considered as a QoL measure. If the patient did not report any negative influence on his/her daily QoL, then the score was “0”. The correlation between “QoL score” and “symptom score” was measured.
Statistical analysis
Each patient’s MMAS score was compared with the QoL score and symptom score. The statistical analysis was performed using IBM SPSS Statistics for MAC version 21.0 (IBM Corporation, Armonk, NY, USA). Spearman’s rho test was used to evaluate the difference between adherence, QoL, and ADRs. For statistical analysis, an α-value of 0.05 was considered statistically significant. Descriptive statistics were calculated as frequencies, percentages, means, and medians.
Results
Patients
A total of 120 chronic-phase CML patients were contacted between June 2012 and September 2013 in eight secondary or tertiary care hospitals in Finland. Of these, 86 participated in the study. The mean age was 57.8 years and 52% were male. Of the patients, 79.1% were using imatinib, 10.5% dasatinib, and 10.5% nilotinib. Patient characteristics are shown in .
Table 1 Characteristics of the CML patients on TKI medication involved in the study (n=86)
Patient-reported ADRs and their influence on medication adherence
The incidence of patient-reported ADRs was high (). At the time of the study, 97% of the patients reported suffering from at least one ADR which had started after the start of TKI treatment. The most commonly experienced ADRs were muscle soreness or cramp (69/86, 80%), swelling of hands, legs, feet, or around the eyes (59/86, 69%), and fatigue (43/86, 50%). There were also differences in ADR profiles between the three different therapies (). The incidence of different ADRs at different adherence levels is shown in . No correlation was found between adherence and patient-reported ADRs, because symptoms were equally common in each MMAS adherence class (high, medium, and low).
Figure 1 Prevalence of each patient-reported ADR in the study population (% of the patients, n=86).
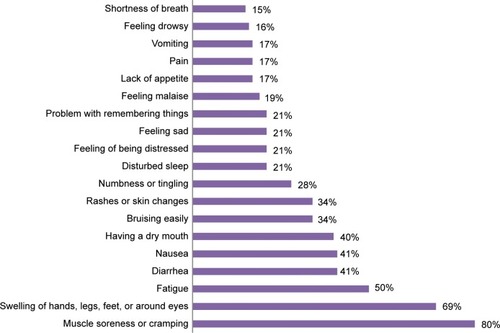
Table 2 CML patients’ self-reported ADRs with regard to the TKI in use
Table 3 CML patients’ self-reported ADRs compared to their adherence to TKIs measured by MMAS (n=86)
Influence of ADRs on patients’ QoL
More than half of the patients felt that the ADRs had a negative influence on their daily QoL (). A quarter of the patients reported that the symptoms had a negative influence either on their mood, general condition, or enjoyment of life. Patients who felt that their symptoms negatively affected their QoL suffered from an average of eight different symptoms (range: 3–15, median 8).
Table 4 The negative influence of ADRs to patients’ quality of life in different adherence levels
Compared with the total study population, the incidence of all symptoms other than nausea and vomiting was higher among patients who said that their symptoms negatively affected their daily life than among those who reported no such influence (). More men reported their symptoms to have a negative influence on their daily life than women (53% vs 44%). More than half of the imatinib users (54%), one-third of the dasatinib users (33%), and one-fifth of the nilotinib users (22%) experienced symptoms that had an unwanted influence on their daily life.
Table 5 ADRs of the patients who reported that symptoms had negative influence to daily life (n=44) vs ADRs of all patients (n=86)
Ceased medication or reduced dose
Nine (10%) patients spontaneously reported that ADRs had influenced their medication taking, ie, they had stopped taking the medication or reduced the dose when feeling worse (MMAS Question no 3). These patients also sometimes unintentionally forgot to take their medication. All of them reported that they were suffering from disturbed sleep, 89% (n=8) reported swelling, and 89% (n=8) cramp. Five (56%) of them felt that the symptoms influenced their daily life. Four patients had low adherence and five had medium adherence according to MMAS. Eight of them were using imatinib and one, dasatinib. The knowledge of the disease and its treatment was poor in this patient group,Citation12 except for one patient who scored 4 out of 5 points. Six of these patients scored 0 and two patients scored 1 in the knowledge test.
Intentional nonadherence and patient-reported symptoms
Twenty-six (30%) patients in the study reported intentional nonadherence (ie, not taking medication for some reason other than forgetting). On average, these patients suffered from six different symptoms (range: 0–11, median 7). Intentional nonadherence was more common among women than men (37% vs 24%), and among dasatinib and nilotinib users than imatinib users (44%, 44% vs 26%). Half of the patients taking the medication twice daily reported intentional nonadherence compared with 26% of patients taking the medication on a single daily dose.
Discussion
In this study, the prevalence of patient-reported ADRs during TKI treatment was high and much higher than in clinical trials, which in most cases study the efficacy and safety of treatments. Even though the ADRs did not influence adherence, they had a significant influence on patients’ QoL.
It has been reported in previous studies that symptom burden is cited as a primary reason for poor adherence to TKI therapy, and poor adherence has been linked to unsatisfactory treatment response and increased health-care resource utilization.Citation9,Citation10,Citation14 Only 10% of the patients in the present study spontaneously reported that ADRs had influenced their medication taking, ie, they had stopped taking the medication or reduced the dose when feeling worse. Patients were willing to take the medication even though they were reporting ADRs. We were unable to find a clinical correlation between these symptoms and patient adherence, but there was a significant correlation between higher number of symptoms and a negative impact on the patient’s QoL.
Results from previous randomized controlled trials suggest that treatment decisions influenced by QoL considerations may be beneficial in some patients.Citation23 It has been shown in a previous study that treatment with TKIs generally does not adversely affect – and may even improve – patient QoL.Citation24 As stated by the FDA, some “treatment effects are known only to the patient”, and such information can be lost when the patient’s perspective “is filtered through a clinician’s evaluation of the patient’s response to clinical interview questions”.Citation19 Thus, it is likely that robust QoL evidence in this area will help physicians to make more tailored treatment decisions. In some therapeutic areas, symptom-specific rating scales have been found to be valuable tools for assessing the effects of an intervention on treatment-related symptoms. In general, patients report symptoms earlier and more frequently than clinicians. From these studies, it appears that clinicians may be better at recognizing ADRs with potentially serious consequences, whereas patients may be better at assessing more subtle changes that affect their overall QoL.Citation25
The emergence of treatment-related ADRs, although potentially detrimental to patient QoL, can be effectively managed in most cases because ADRs are mostly mild to moderate in severity and generally consistent (ie, predictable) over time and across lines of therapy. Furthermore, the number of TKIs currently approved increases the likelihood that patients found to be intolerant to one TKI can switch to another, better tolerated alternative.
As CML patients come to expect increasingly longer survival with TKI therapy, the importance of managing symptom burden related to the disease and its treatment will also increase. The complex interplay between symptom burden, adherence, response to TKI therapy, and health-care utilization highlights the need for regular symptom burden assessment in CML as a means to identify potential adherence problems before they affect the patients’ response to TKI treatment. Information on disease and treatment-related effects from the patient’s perspective crucially provides the additional knowledge needed for both patients and physicians to make informed treatment decisions. Many patients do not exhibit disease symptoms at diagnosis and therefore may be irritated by the ADRs caused by the treatment. The ADRs which had the most negative effect on patients’ QoL in the present study were swelling, rashes, disturbed sleep, feeling sad or depressed, a problem with remembering things, and a feeling of malaise. Identifying these symptoms could help in treatment follow-up designed to manage the ADRs and patients to be able to successfully continue their treatment. QoL is necessary to support the proper use of TKI therapy in CML.
Limitations
The present study has some limitations. The instruments used for assessing ADRs and QoL were not validated. At the time this study was started, no validated QoL assessment instruments specific to leukemia or CML were available. Recently, three leukemia- and CML-specific QoL instruments have been validated: the Functional Assessment of Cancer Therapy – Leukemia,Citation15 the M.D. Anderson Symptom Inventory-CML,Citation26,Citation27 and the EORTC QLQ-CML24.Citation28 Further development and validation of leukemia- or CML-specific QoL measurement tools could improve the overall management of CML.
The study was a cross-sectional study (only one interview done). The ADRs were only reported by the patient and not compared with the physician’s assessment. It would be interesting to evaluate the severity of the symptoms in future studies. It may also be argued whether ADRs are the reason for a deterioration in QoL. ADRs may affect QoL, but it may also be argued that persons reporting impaired QoL may be those experiencing ADRs more frequently than others.
Conclusion
TKI-related ADRs were common among CML patients irrespective of patients’ adherence level. Patients who reported that ADRs had a negative influence on their daily QoL perceived more ADRs than those who did not experience a negative influence.
Acknowledgments
We are grateful to all the patients who participated in this study. We thank Dr Kimmo Talvensaari, MD, PhD; Professor Anne Juppo; Perttu Koskenvesa, MD; and Professor Kimmo Porkka for their help in making the study design. We would like to thank Professor Kari Remes; Dr Marjut Kauppila, MD, PhD; Dr Venla Terävä, MD, PhD; Dr Hanna Ollikainen, MD, PhD; Dr Sakari Kakko, MD, PhD; Antti Koponen, MD; Dr Maija Mikkola, MD, PhD; Anu Kutila MD; and Kirsi Launonen, MD for their help in recruiting the patients for the study. Our warm thanks go to study nurses Minna Pajuportti, Raija Aaltonen, Marjut Yrjönen, Ulla Pietilä, Erja Silventoinen, Leena Lahdenmaa, and Riitta Saavalainen for their help with patient contacts.
Disclosure
Meri Kekäle has received a grant from University Pharmacy, Helsinki, for this research. The authors report no other conflicts of interest in this work.
References
- GoldmanJMeloJChronic myeloid leukemia – advances in biology and new approaches to treatmentN Engl J Med2003349151451146414534339
- DeiningerMWO’BrienSGGuilhotFInternational randomized study of interferon vs STI571 (IRIS) 8-year follow-up: sustained survival and low risk for progression or events in patients with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) treated with imatinib [abstract 1126]Blood2009114
- BaccaraniMDeiningerMWRostiGEuropean LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013Blood2013122687288423803709
- LarsonRAHochhausAHughesTPNilotinib vs imatinib in patients with newly diagnosed Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase: ENESTnd 3-year follow-upLeukemia2012262197220322699418
- KantarjianHMShahNPCortesJEDasatinib or imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: 2-year follow-up from a randomized phase 3 trial (DASISION)Blood20121191123112922160483
- HochhausAO’BrienSGGuilhotFSix-year follow-up of patients receiving imatinib for the firstline treatment of chronic myeloid leukemiaLeukemia2009231054106119282833
- KantarjianHShahNPHochhausADasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemiaN Engl J Med20103622260227020525995
- CellaDNowinskiCJFrankfurtOThe impact of symptom burden on patient quality of life in chronic myeloid leukemiaOncology20148713314725012261
- NoensLvan LierdeMADe BockRPrevalence, determinants, and outcomes of nonadherence to imatinib therapy in patients with chronic myeloid leukemia: the ADAGIO studyBlood20091135401541119349618
- MarinDBazeosAMahonFXAdherence is the critical factor for achieving molecular responses in patients with chronic myeloid leukemia who achieve complete cytogenetic responses on imatinibJ Clin Oncol2010282381238820385986
- IbrahimAREliassonLApperleyJFPoor adherence is the main reason for loss of CCyR and imatinib failure for chronic myeloid leukemia patients on long-term therapyBlood20111173733373621346253
- KekäleMTalvensaariKKoskenvesaPPorkkaKAiraksinenMChronic myeloid leukemia patients’ adherence to per oral tyrosine kinase inhibitors compared with adherence as estimated by their physiciansPatient Prefer Adherence201481619162725473270
- YoodMUOliveriaSACzirakyMAdherence to treatment with second-line therapies, dasatinib and nilotinib, in patients with chronic myeloid leukemiaCurr Med Res Opin201228221321922168217
- EliassonLCliffordSBarberNMarinDExploring chronic myeloid leukemia patients’ reasons for not adhering to the oral anticancer drug imatinib as prescribedLeuk Res20113562663021095002
- TraskPCCellaDPowellCHealth related quality of life in chronic myeloid leukemiaLeuk Res20133791323116602
- PhillipsKMPinilla-IbarzJSotomayorEQuality of life outcomes in patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors: a controlled comparisonSupport Care Cancer20132141097110323179489
- EfficaceFBrecciaMSausseleSWhich health-related quality of life aspects are important to patients with chronic myeloid leukemia receiving targeted therapies and to health care professionals? GIMEMA and EORTC quality of life groupAnn Hematol2012911371138122543826
- AzizZIqbalJAaqibMAssessment of quality of life with imatinib mesylate as first-line treatment in chronic phase-chronic myeloid leukemiaLeuk Lymphoma2011521017102321534871
- US Food Drug Administration: Guidance for IndustryPatient-reported Outcome Measures: Use in Medical Product Development to Support Labeling ClaimsWashington, DCU.S. Department of Health and Human Services, Food and Drug Administration2009
- EfficaceFCocksKBrecciaMTime for a new era in the evaluation of targeted therapies for patients with chronic myeloid leukemia: inclusion of quality of life and other patient-reported outcomesCrit Rev Oncol Hematol20128112313521435899
- LaugsandEASprangersMABjordalKHealth care providers underestimate symptom intensities of cancer patients: a multicenter European studyHealth Qual Life Outcomes2010810420858248
- MoriskyDEAngAKrousel-WoodMPredictive validity of a medication adherence measure in an outpatient settingJ Clin Hypertens200810348354
- GuyattGHFerransCEHalyardMYExploration of the value of health-related quality-of-life information from clinical research and into clinical practiceMayo Clin Proc2007821229123917908529
- HahnEAGlendenningGASorensenMVQuality of life in patients with newly diagnosed chronic phase chronic myeloid leukemia on imatinib versus interferon alfa plus low-dose cytarabine: results from the IRIS StudyJ Clin Oncol2003212138214612775739
- BaschEJiaXHellerGAdverse symptom event reporting by patients vs clinicians: relationships with clinical outcomesJ Natl Cancer Inst20091011624163219920223
- M.D. Anderson Cancer Center: The MD Anderson Symptom Inventory Chronic Myeloid Leukemia Module (MDASI-CML) Available from: http://www.mdanderson.org/education-and-research/departments-programs-and-labs/departments-and-divisions/symptom-research/symptom-assessment-tools/mdasi-cml.htmlAccessed March 18, 2014
- WilliamsLGarcia GonzalezAAultPMeasuring the symptom burden associated with the treatment of chronic myeloid leukemiaBlood2013122564164723777764
- EfficaceFBaccaraniMBrecciaMInternational development of an EORTC questionnaire for assessing health-related quality of life in chronic myeloid leukemia patients: the EORTC QLQ-CML24Qual Life Res201423382583624026634