
Abstract
Purpose
Adherence to and persistence with antidepressants are often suboptimal. However, little is known about how patient knowledge and outcome expectations may influence antidepressant adherence and persistence.
Method
Individuals who had been prescribed their first antidepressant to treat depression in the preceding 6 months were recruited to an online survey via Facebook. Knowledge, education received, and initial outcome expectations were analyzed for associations with persistence and adherence.
Results
Two hundred and twenty surveys were analyzed. A total of 117 participants had taken their antidepressant for at least 3 months; another 25 had never started or stopped after <3 months without consulting their doctor. Differences in expectations and various educational messages among persistent and nonpersistent participants were identified. Having received the instruction “don’t stop it without checking with your doctor” was a significant independent predictor of persistence (odds ratio [OR] =5.9, 95% confidence interval [CI] =1.4–24.5). At the time of the survey, 82.7% of participants were taking an antidepressant and 77.9% were adherent. Significant independent predictors of adherence were a greater age (OR =1.1, 95% CI =1.0–1.2), knowledge (OR =1.6, 95% CI =1.1–2.3), being informed of common side effects (OR =5.5, 95% CI =1.1–29.0), and having discussed ways to solve problems (OR =3.9, 95% CI =1.1–14.5).
Conclusion
Improving outcome expectations and particular educational messages may increase adherence and persistence. Greater knowledge may enhance adherence. Further investigation is warranted to determine whether a focus on these simple educational messages will improve outcomes in patients who commence an antidepressant.
Keywords:
Introduction
Persistence with and adherence to antidepressants are typically poor, so there remain substantial opportunities for improvement.Citation1 Adherence is the extent that a person’s medication-taking behavior corresponds with agreed recommendations from a health professional in terms of timing, dosage, and frequency.Citation2 Persistence is a measure of how long a patient continues with the treatment, compared to the prescribed duration.Citation2 Discontinuing an antidepressant early or taking it inconsistently increases the risk of relapse or recurrence of depression.Citation3
There is usually a delay of 1–2 weeks before some response may be seen from an antidepressant and 6 weeks or more for full benefit.Citation4 The STAR*D trial found that, while approximately one-third of patients experienced remission with the first antidepressant prescribed, trials of up to four antidepressants were required to achieve a cumulative remission rate of 67%.Citation5 Patients starting on an antidepressant should be informed about the likely delay in efficacy and that a change in agent may be required. Patients should be reviewed regularly for efficacy, adverse effects, adherence, and persistence.
Once stabilized on an effective antidepressant, it is recommended that it should be continued for at least 6–12 months after the initial episode of depression.Citation4 However, one study found that only 44.3% of participants were still taking their antidepressant 6 months after the initial prescription.Citation1 Of these, 63.1% discontinued their antidepressant without involving their doctor, and only 55.6% of participants were considered adherent.Citation1 Another study found that only 19% of participants stayed within the guideline recommendations of how the antidepressant should be taken.Citation6 Some patients do not even start their antidepressant, with one-quarter in one study either not starting the medication or discontinuing within 2 weeks.Citation7
Possible factors that may influence adherence and persistence include patient knowledge about antidepressants and depression, and patient expectations about the treatment outcome. Patients seem to have varying beliefs, concerns, and misconceptions that may influence their use of antidepressants.Citation8–Citation13 For example, the study by Warden et al.Citation14 found that patients’ initial concerns about possible side effects affected persistence. Another study by this author found that negative attitudes about psychiatric medications were linked with poor persistence at 12 months.Citation15 A study by Anderson et al analyzed qualitative data on patient experiences of starting an antidepressant. The approach by the clinician and patients’ involvement were reported by patients as influencing whether they took their antidepressant.Citation13
Providing accurate and tailored education about antidepressants is likely to assist patients in taking their antidepressants correctly and safely. While educational interventions alone do not appear to result in improved adherence,Citation16,Citation17 patients do indicate a desire for more information than is currently being provided,Citation18–Citation20 and other studies have found a link between educational messages and persistence.Citation21,Citation22 Patient knowledge does not seem to have been studied explicitly in this context. Therefore, research investigating the effect patient knowledge on depression and antidepressants may have on persistence and adherence is warranted, along with further examination of the links that adherence and persistence have with educational messages. This information will assist health professionals to determine their approach when counseling.
There is also a paucity of studies focusing on patient outcome expectations regarding antidepressant treatment. Researchers have generally indicated a link between more positive initial outcome expectations and a greater response to treatment.Citation23–Citation25 However, they have not looked closely at adherence or persistence. Therefore, there is considerable value in studying the possible effect of pretreatment expectations on adherence and persistence in a clinical setting.
The aim of this study was to investigate the relationships outcome expectations, knowledge, and educational messages received may have with adherence to and persistence with antidepressants in patients who have recently initiated antidepressant therapy.
Methods
Participants were recruited to an online survey using Facebook, Inc™, from March 12, 2014 to June 15, 2014. A paid advertisement targeted Australian users over 18 years of age. A Facebook page was also created to generate a status in order to share the survey freely with the users. A prize of an Apple® iPad mini was used as an incentive to participate. Participants were eligible if they were aged over 18 years, residing in Australia, and had been prescribed their first antidepressant to treat depression in the preceding 6 months. This was regardless of whether they were currently taking an antidepressant.
The survey asked for the age, sex, current antidepressant taking status, the date on which the antidepressant was started, and, where relevant, the date it was stopped. If participants had switched, stopped, or never started their antidepressant, they were directed to extra questions.
Outcome expectations were measured using a modified version of the Credibility and Expectancy Questionnaire. This was first used in 1972Citation26 and validated in 2000, showing good internal consistency and test/retest reliability.Citation27 Rutherford et al modified this questionnaire for their study, choosing the two questions that measured expectancy.Citation24 One question measured the expected likelihood of improvement, and the other the expected magnitude of improvement.Citation24 The expectancy score was derived from the sum of these two questions.Citation24 Participants were asked to think back to when they were first prescribed their antidepressant and what they thought at this time so that the answers would approximate their initial outcome expectations.
Knowledge was measured using a shortened version of the patient multiple-choice knowledge test of depression and its treatments, developed and psychometrically tested by Gabriel and Violato.Citation28 The original questionnaire contained 27 questions; this was shortened to seven for the purposes of this study. The seven questions chosen included a question from each component of knowledge about depression and antidepressants that the original researchers assessed. The total number of correct answers gives a knowledge score.Citation28 Educational messages received by the participants were also assessed using a questionnaire used by Lin et al with slight modifications.Citation21 Participants were asked to think back to the information originally provided by their doctor or pharmacist and whether particular topics or instructions had been covered.
Adherence was measured by the Antidepressant Adherence questionnaire that Gabriel and Violato adapted from the Morisky Medication Adherence Questionnaire.Citation29 Participants currently taking an antidepressant were asked to think back over the past 4 weeks to determine the number of times he or she missed the medication.Citation29 Participants were classified as being nonadherent if they had missed their medication, for any reason, five or more times over the past 4 weeks.Citation29
It was estimated that at least 384 patients needed to be surveyed to ensure that the results were generalizable to the ~1 million Australians with depression.Citation30 This recruitment target was based on a sample size calculation, using data for the total Australian prevalence of depression, with a 95% confidence interval (CI) and a 5% margin of error.Citation30,Citation31
Variables were analyzed to identify predictors of adherence and persistence. Persistence was analyzed by considering participants who had taken their antidepressant for 3 months or more to be persistent and those who never started or who had stopped after <3 months without consulting their doctor to be nonpersistent. Participants who were still taking an antidepressant but who had been taking it for <3 months were excluded from this aspect of the analysis. Adherence was analyzed for participants currently taking an antidepressant who had an adherence classification.
All variables were entered into SPSS Version 21 (IBM Corporation, Armonk, NY, USA). Age and sex of the participant, expectation scores, knowledge scores, and educational messages were tested against adherence and persistence. Categorical variables were analyzed using the chi-square test for independence (with Yates continuity correction), parametric continuous variables were analyzed using independent-samples t-tests, and nonparametric continuous variables were analyzed using the Mann–Whitney U-test. Pearson correlation was used to compare two parametric continuous variables. Logistic regression models were performed on the univariate predictors, with P<0.1 used as a threshold for entry into the model. A significance level of P<0.05 was used for all statistical procedures. Any missing responses to questions were excluded from the applicable analyses.
This study was approved by the Tasmanian Social Sciences Human Research Ethics Committee on December 10, 2013 (reference number H0013623). An information page was included at the start of the survey. This informed potential participants about the risks and benefits of the study and explained that non-identifiable, combined results may be submitted for publication. All participants were 18 years of age or older. By submitting the survey, participants provided their implied consent.
Results
A total of 238 patients completed the online survey, of which 220 (92.4%) responses were usable (). The cost of the recruitment strategy through Facebook advertising averaged $6.25 per response.
Figure 1 Participant flowchart.
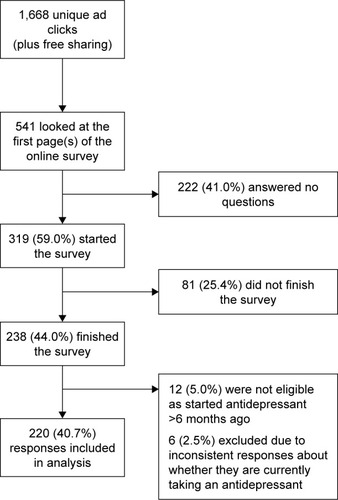
A high proportion of respondents were young (≤25 years old), and the majority of them were women, as shown in . The majority of participants were still taking an antidepressant (82.7%) at the time of the survey. Of the 181 participants with an adherence classification, 22.1% reported being nonadherent.
Table 1 Participant characteristics
details the reasons participants gave for switching, never starting, or stopping their antidepressant. Participants who had switched antidepressants frequently responded that they had experienced adverse effects (43.8%) or that the initial antidepressant was not working (75.0%). Participants who never started their antidepressant cited concerns about possible adverse effects (57.1%) and a belief that they did not think they needed to be on an antidepressant (57.1%), most commonly.
Table 2 Reasons given for switching, stopping, or never starting the prescribed antidepressant
Participants who had stopped taking an antidepressant did so because of feeling better (16.1%), experiencing adverse effects (35.5%), the lack of efficacy (48.8%), or concerns about dependence (19.4%). Only three (9.7%) discontinued their antidepressant with their doctor’s involvement, with two of these participants discontinuing after <3 months. Fourteen (45.2%) had since told their doctor, but the remainder had not informed their doctor that they had stopped their medication.
The responses of 142 participants were available for the analysis of persistence. One hundred and seventeen participants (82.4%) reported taking their antidepressant for at least 3 months, while 25 (17.6%) had never started or stopped after <3 months without consulting their doctor and were considered to be nonpersistent. Predictors of persistence from the analysis of these participants are shown in .
Table 3 Predictors of persistence
Participants who were classified as being persistent had significantly greater mean expectation scores than those who had poor persistence (11.5±3.6 vs 7.4±4.1, respectively; t=4.8, P<0.001). Seven educational messages were found to be significantly associated with persistence, and one showed a trend toward significance. Persistent participants had a greater median age than nonpersistent participants, with a trend toward significance (median age 23, range 18–71 vs 22, range 18–61, respectively; U=1,122.5, P=0.08). There was no significant association with persistence for knowledge scores (t=0.9, P=0.332) or sex (x2=0.03, df=1, P=0.86).
The multiple variable logistic regression model for persistence was statistically significant, x2 (10, N=108)=30.0, P=0.001, explained between 24.3% and 40.9% of variance in persistence, and correctly classified 88.0% of cases. The educational instruction “don’t stop it without checking with your doctor” was identified as a significant independent predictor of persistence (OR =5.9, 95% CI =1.4–24.5).
A total of 181 participants were still taking their antidepressant at the time of the survey and were assessed for adherence, with 22.1% of these classified as nonadherent. contains the predictors of adherence for these participants. Adherent participants were significantly older than nonadherent participants (median age 28, range 18–71 vs 21, range 18–57, respectively; U=1,872.5, P=0.002). Participants who were adherent also had significantly greater mean expectation scores than those who were nonadherent (11.9±3.6 vs 10.1±3.9, respectively; t=2.8, P=0.006), although the difference was small. Adherent participants had significantly better mean knowledge scores than those who were nonadherent (5.2±1.5 vs 4.7±1.6, respectively; t=2.0, P=0.042). Five educational messages were found to be significantly associated with adherence, and four showed a trend toward significance. There was no significant association between the sex of the participant and adherence (x2=0.85, df=1, P=0.36).
Table 4 Predictors of adherence
The multiple variable logistic regression model for adherence was statistically significant, x2 (12, N=148)=43.0, P<0.001, explained between 25.2% and 39.3% of variance in adherence, and correctly classified 81.8% of cases. Four independent predictors were identified: higher age (OR =1.1, 95% CI =1.0–1.2), knowledge score (OR =1.6, 95% CI =1.1–2.3), being informed of common side effects (OR =5.5, 95% CI =1.1–29.0), and having discussed ways to solve problems (OR =3.9, 95% CI =1.1–14.5).
No correlation was found between knowledge and expectation scores (r=0.005).
Discussion
Poor persistence with and nonadherence to antidepressants were common in our study participants. The results indicate that improving outcome expectations may increase adherence and persistence, and improving knowledge may improve adherence. Certain specific educational messages were also linked with persistence or adherence.
Persistence among the participants was better than in some studies.Citation1,Citation21,Citation32 For example, two other studies found that 38% and 57%, respectively, stopped within 3 months of initial prescription.Citation1,Citation32 Adherence was also greater than other studies have reported.Citation1,Citation33 Conversely, the proportion of patients who stopped their antidepressant without involving their doctor was similar to or greater than that reported in previous studies.Citation1,Citation6
This study provides new information on the effects of outcome expectations on adherence to and persistence with antidepressants. Previous research has focused more on the effects on treatment outcome from taking antidepressants, with little information on persistence and adherence.Citation24,Citation25 While the magnitude in the difference between the mean expectation scores was small, the results are promising. The associations between higher outcome expectations and both persistence and adherence indicate that interventions to improve patients’ outcome expectations could be worthwhile.
There has been limited research to date on factors that may influence a patient’s expectations about treatment outcome. The current study did not find a link between knowledge and expectations. Possible factors identified previously include more information about the offered treatment, past experiences with medications, and relationships with health care providers.Citation34–Citation36 However, the best ways to improve a patient’s expectations are unclear. For example, changing the doctor’s communication style has not always had an effect on expectations in past studies.Citation23 Further research is needed to identify the ways to influence patients’ outcome expectations.
Knowledge about depression and antidepressants was an independent predictor of adherence. Studies have found that greater education about antidepressants may give patients more confidence and is associated with an increased use of antidepressants, and that educational messages may be linked to adherence.Citation19,Citation21,Citation22 However, multiple studies show only minimal effect of educational interventions alone on adherence.Citation16,Citation17 Despite this, the link between knowledge and adherence in this study reiterates the importance of ensuring that patients are knowledgeable about depression and antidepressants as a component of promoting adherence.
This study supports the findings of Lin et al, who found specific educational messages to be linked with persistence (termed “adherence” in their study) after 1 month.Citation21 Three of the significant messages were in common with their study: how long the antidepressant should take to start having a noticeable effect and being told a couple of weeks or a month or so; what to do if the person had questions about the use of the medicine; and not to stop the medication without checking with the doctor. The message about time to effect being significant indicates that knowing it will take some time to work may help patients persevere. This aligns with a comment made by a patient in one study who explained that being told it would take 4–6 weeks to start working helped him to not give up on treatment.Citation13
The only independent predictor of persistence was advising patients not to stop without telling their doctor, which suggests that this message may effectively discourage patients from stopping on their own, without seeking support. How the medication works and three of the messages about side effects were also significant. Perhaps counter intuitively, the message about how long to expect to continue taking the medication was not related to persistence. Similarly, being told to keep taking the medicine even if starting to feel better was also not related. It could be that these messages play a greater role in persistence later into treatment.
In common with the analysis of persistence, three of the four educational messages about side effects were significantly related to adherence. In particular, communication about common side effects was an independent predictor. The links between communication about side effects and persistence and adherence support the findings from Bull et al,Citation12 who found discussion about adverse effects significantly reduced the odds of stopping antidepressant treatment. Similarly, patients in other studies had more confidence if they experienced adverse effects as described, or found adverse reactions more tolerable when they had been informed about them.Citation37,Citation38 Other significant messages associated with adherence included how the medication works and discussing ways to solve problems (an independent predictor). Interestingly, being told to take the medication on a daily basis without interruption was not related to adherence.
This analysis of educational messages emphasizes the value of a number of common counseling points to help with adherence, persistence, or both. However, not all of the messages that were or were not significant were predictable. This highlights the possible benefits of considering studies like this one in order to incorporate evidence-based counseling approaches into clinical practice.
There are some potential limitations to this study. The comparatively small proportion of nonpersistent or nonadherent participants may have been due to these individuals being less likely to participate. Advertising a prize of an iPad mini through Facebook also had the potential to influence participants and to encourage misleading responses. Additionally, the sample size was less than that calculated, and recruitment through Facebook may have led to a select population that may not fully represent the target population. The combination of these factors may have influenced the observed level of persistence.
There were more women responders, which may be partially explained by a greater rate of having a “depressive episode” in women and a greater utilization of mental health services, as measured in an Australian national survey in 2007.Citation30 However, the difference in the number of responders by sex is larger than this explanation alone can account for. Although there were more young responders, the age range responding was wide (18–71), meaning there were still a number of older participants. Location demographic data were not collected, so the spread of respondents across Australia was not analyzed. A possible strength of this novel recruitment strategy is that it may have reached individuals normally missed through standard methods, including those who may have limited contact with health care professionals.
In addition, there were limitations relating to the nature of the survey. The survey relied on participants self-reporting their adherence and persistence, looking at only the past 4 weeks. Furthermore, initial outcome expectations and education received were not measured at the start of treatment. Instead, participants were asked to think back on when they were first prescribed their original antidepressant. Some of the questionnaires were modified slightly. In particular, the knowledge questionnaire was shortened so that the survey would not be overly long. Additionally, clinical outcome was not measured in this study, which meant that the relationships between this and the observed adherence and persistence rates were not analyzed.
While recruitment was specific for patients with depression only, it is possible that patients with other diagnoses participated. Clinical variables such as the severity and duration of illness, specific medications and dosages prescribed, and other treatments patients are on could be looked at in future studies. Despite these potential limitations, a significant strength of this study is that it addresses areas that have received minimal prior study, especially in a clinical setting. Future research could aim to support the study results in other populations, with larger sample sizes.
Conclusion
In conclusion, given that poor persistence and adherence are often typical of patients taking an antidepressant, the results provide valuable information for researchers and health professionals alike. Future studies could further investigate what influences expectations, which could lead to the development of targeted interventions to improve patients’ initial outcome expectations. An immediate implication for clinical practice is guidance on key messages to include when counseling patients starting an antidepressant to attain greater persistence and adherence. Further investigation is warranted to determine whether a focus on these simple educational messages will improve patient outcomes. Overall, the results of this study are encouraging and indicate promising avenues to explore.
Acknowledgments
The abstract of this paper was presented at the Australasian Pharmaceutical Science Association conference in December 2014 as an oral presentation. The full program, with the abstract included on page 45, is available at http://apsa-online.org/files/2014ConferenceProceedings.pdf. The actual paper, however, has never been published and is not being considered for publication elsewhere.
Disclosure
The authors declare no conflicts of interest in this work.
References
- SawadaNUchidaHSuzukiTPersistence and compliance to antidepressant treatment in patients with depression: a chart reviewBMC Psychiatry200993819531229
- CramerJARoyABurrellAMedication compliance and persistence: terminology and definitionsValue Health2008111444718237359
- PompiliMSerafiniGDel CasaleAImproving adherence in mood disorders: the struggle against relapse, recurrence and suicide riskExpert Rev Neurother200997985100419589049
- Therapeutic Guidelines LimitedTreatment of DepressionMelbourneeTG complete2013
- RushAJTrivediMHWisniewskiSRAcute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D reportAm J Psychiatry2006163111905191717074942
- HunotVMHorneRLeeseMNChurchillRCA cohort study of adherence to antidepressants in primary care: the influence of antidepressant concerns and treatment preferencesPrim Care Companion J Clin Psychiatry200792919917607330
- van GeffenECGardarsdottirHvan HultenRvan DijkLEgbertsACHeerdinkERInitiation of antidepressant therapy: do patients follow the GP’s prescription?Br J Gen Pract200959559818719192372
- BrownCBattistaDRBruehlmanRSereikaSSThaseMEDunbar-JacobJBeliefs about antidepressant medications in primary care patients: relationship to self-reported adherenceMed Care200543121203120716299431
- ChakrabortyKAvasthiAKumarSGroverSAttitudes and beliefs of patients of first episode depression towards antidepressants and their adherence to treatmentSoc Psychiatry Psychiatr Epidemiol200944648248819011717
- van GeffenECHermsenJHHeerdinkEREgbertsACVerbeek-HeidaPMvan HultenRThe decision to continue or discontinue treatment: experiences and beliefs of users of selective serotonin-reuptake inhibitors in the initial months – a qualitative studyRes Social Adm Pharm20117213415021272543
- KessingLVHansenHVDemyttenaereKBechPDepressive and bipolar disorders: patients’ attitudes and beliefs towards depression and antidepressantsPsychol Med20053581205121316116946
- BullSAHuXHHunkelerEMDiscontinuation of use and switching of antidepressants: influence of patient-physician communicationJAMA2002288111403140912234237
- AndersonCKirkpatrickSRidgeDKokanovicRTannerCStarting antidepressant use: a qualitative synthesis of UK and Australian dataBMJ Open2015512e008636
- WardenDTrivediMHWisniewskiSRIdentifying risk for attrition during treatment for depressionPsychother Psychosom200978637237919738403
- WardenDRushAJCarmodyTJPredictors of attrition during one year of depression treatment: a roadmap to personalized interventionJ Psychiatr Pract200915211312419339845
- ChongWWAslaniPChenTFEffectiveness of interventions to improve antidepressant medication adherence: a systematic reviewInt J Clin Pract201165995497521849010
- GilbodySWhittyPGrimshawJThomasREducational and organizational interventions to improve the management of depression in primary care: a systematic reviewJAMA2003289233145315112813120
- GarfieldSFrancisSASmithFJBuilding concordant relationships with patients starting antidepressant medicationPatient Educ Couns200455224124615530761
- HaslamCBrownSAtkinsonSHaslamRPatients’ experiences of medication for anxiety and depression: effects on working lifeFam Pract200421220421215020393
- van GeffenECKruijtboschMEgbertsACHeerdinkERvan HultenRPatients’ perceptions of information received at the start of selective serotonin-reuptake inhibitor treatment: implications for community pharmacyAnn Pharmacother200943464264919318603
- LinEHVon KorffMKatonWThe role of the primary care physician in patients’ adherence to antidepressant therapyMed Care199533167747823648
- SunGCHsuMCMoyleWLinMFCreedyDVenturatoLMediating roles of adherence attitude and patient education on antidepressant use in patients with depressionPerspect Psychiatr Care2011471132221418069
- RutherfordBRWagerTDRooseSPExpectancy and the treatment of depression: a review of experimental methodology and effects on patient outcomeCurr Psychiatry Rev20106111024812548
- RutherfordBRMarcusSMWangPA randomized, prospective pilot study of patient expectancy and antidepressant outcomePsychol Med2013431822717127
- SotskySMGlassDRSheaMTPatient predictors of response to psychotherapy and pharmacotherapy: findings in the NIMH Treatment of Depression Collaborative Research ProgramAm J Psychiatry1991148899710081853989
- BorkovecTDNauSDCredibility of analogue therapy rationalesJ Behav Ther Exp Psychiatry197234257260
- DevillyGJBorkovecTDPsychometric properties of the credibility/expectancy questionnaireJ Behav Ther Exp Psychiatry2000312738611132119
- GabrielAViolatoCThe development of a knowledge test of depression and its treatment for patients suffering from non-psychotic depression: a psychometric assessmentBMC Psychiatry200995619754944
- GabrielAViolatoCKnowledge of and attitudes towards depression and adherence to treatment: the Antidepressant Adherence Scale (AAS)J Affect Disord2010126338839420708273
- Australian Bureau of StatisticsNational Survey of Mental Health and Wellbeing: Summary of Results, 2007 (43260)CanberraABS2008
- SurveyMonkey Inc [webpage on the Internet]Survey Sample Size2013 Available from: https://www.surveymonkey.com/mp/sample-size/Accessed July 22, 2013
- LuCYRougheadENew users of antidepressant medications: first episode duration and predictors of discontinuationEur J Clin Pharmacol2012681657121713518
- BullochAGPattenSBNon-adherence with psychotropic medications in the general populationSoc Psychiatry Psychiatr Epidemiol2010451475619347238
- DolovichLNairKSellorsCLohfeldLLeeALevineMDo patients’ expectations influence their use of medications? Qualitative studyCan Fam Physician200854338439318337533
- HorvathPTreatment expectancy as a function of the amount of information presented in therapeutic rationalesJ Clin Psychol19904656366422246373
- MosesTLeuchterAFCookIAbramsMWhat shapes depressed individuals’ pre-treatment expectation in antidepressant clinical trials?Internet J Ment Health200732112
- BadgerFNolanPConcordance with antidepressant medication in primary careNurs Stand20062052354016989339
- BolliniPTibaldiGTestaCMunizzaCUnderstanding treatment adherence in affective disorders: a qualitative studyJ Psychiatr Ment Health Nurs200411666867415544664