
Abstract
Background
Modern psychiatry focuses on self-stigma, coping strategies, and quality of life (QoL). This study looked at relationships among severity of symptoms, self-stigma, demographics, coping strategies, and QoL in patients with neurotic spectrum disorders.
Methods
A total of 153 clinically stable participants who met criteria for generalized anxiety disorder, social phobia, panic disorder, agoraphobia, mixed anxiety–depressive disorder, adjustment disorders, somatoform disorders, or obsessive–compulsive disorder were included in a cross-sectional study. Psychiatrists examined patients during regular psychiatric checkups. Patients completed the Quality of Life Satisfaction and Enjoyment Questionnaire (Q-LES-Q), Internalized Stigma of Mental Illness Scale (ISMI), a sociodemographic questionnaire, the Stress Coping Style Questionnaire (Strategie Zvládání Stresu [SVF] 78), and the Clinical Global Impression (CGI) scale.
Results
The diagnostic subgroups differed significantly in age and use of negative coping strategies, but not in other measured clinical or psychological variables. The findings showed that neither sex nor partnership played a role in perceived QoL. All Q-LES-Q domains correlated negatively with all ISMI domains, except school/study. Unemployed and employed groups of patients differed in QoL. Each of the coping strategies, except the need for social support, was related to self-stigma. The findings showed that sex, partnership, education, and employment played no role in self-stigma. No differences between sexes in positive coping strategies, severity of disorder, self-stigma, or QoL were found. QoL correlated significantly with all coping strategies, except for guilt denial. Multiple regression showed the most important factors to be positive coping, employment, and overall self-stigma rating, explaining 32.9% of QoL. Mediation analysis showed self-stigma level and negative coping strategies to be the most influential. The most substantial factors associated with self-stigma, as indicated by regression analysis, were Q-LES-Q total, subjective CGI, and positive coping strategies, which clarified 44.5% of the ISMI.
Conclusion
The study confirmed associations among self-stigma, quality of life, disorder severity, and coping strategies of outpatients with neurotic spectrum disorders.
Introduction
ICD10 category F40–48, specifically “Neurotic disorders, stress-induced disorders, and somatoform disorders”, covers a wide range of specific disorders, such as phobic anxiety disorders (social phobia), other anxiety disorders (generalized anxiety disorder [GAD], panic disorder), somatoform disorders, reaction to severe stress and adjustment disorders, obsessive–compulsive disorder (OCD), and dissociative disorders.Citation1 For brevity, we talk about neurotic spectrum disorders (NsDs). NsDs are accompanied by high health-care utilization, significant impairment, and considerable economic burden. According to epidemiological surveys, a third of the population suffers from an NsD during their lifetime, with higher incidence in women and especially the middle-aged.Citation2 They are the most common reason for the first visit to a psychiatrist or general practitioner for psychological problems in the Czech Republic.Citation3 NsDs are the most prevalent psychiatric problems connected with a high burden of disease.Citation1 Core manifestations of NsDs are tension, appraising situations as demanding, worries or ruminations, ineffective coping strategies, inability to control drives, a tendency to complain, and experiencing negative emotions, such as panic (immediate threat), anxiety (future threats), and depression (chronic stress).Citation4
The main reason for assessing quality of life (QoL) in different types of NsD is that most studies describe reduced QoL in connection with neuroticism or anxiety.Citation5,Citation6 Also, clinical practice advocates that anxiety symptoms are negatively related to QoL.Citation7,Citation8 Specific subtypes of NsD may differ in significantly various QoL domains.Citation9 However, there have not been many studies to measure differences in QoL in various subgroups of NsD or distinguish the effect of symptom severity on QoL.Citation9 In Cramer et al,Citation10 panic disorder, social phobia, and GAD had a negative effect on QoL, OCD had only a minor influence, and agoraphobia did not affect QoL at all.
According to Weidle et al,Citation11 QoL increased while anxiety symptoms decreased in children with OCD. Youth with social anxiety reported lower QoL in association with higher severity of anxiety symptoms.Citation12 Furthermore, lower socioeconomic status, ethnic minority, and female sex are described as predictors of reduced QoL and higher intensity of anxiety symptoms.Citation13,Citation14
While all NsDs seem to cause impairment through the distress connected with symptoms, avoidance, and self-stigma, there has been no description of which specific aspects of QoL are affected in different subtypes of NsD.Citation15 For example, those with social anxiety disorder are more likely to have reduced QoL in the social domain of the World Health Organization Quality of Life – brief assessment, which includes personal relationships, social support, and social relationships.Citation16
A standard definition of QoL has not been established. The World Health Organization outlines QoL as an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.Citation17 QoL is related to such conditions as life-threatening illness and chronic and long-term disorders, which lead to a noticeable decrease in QoL.Citation18,Citation19 Every area of a patient’s life affected by an illness, such as occupational and school functioning, household functioning, social functioning, emotional functioning, life satisfaction, and functional performance, may be included as a part of the multidimensional QoL model.Citation20 QoL assessment is based on a subjective observation of a patient’s life. This approach was built on several sociological surveys that demonstrated that objective life circumstances (such as income or education) have only a marginal effect on QoL.Citation21 Also, it is recommended to avoid the theoretical concepts and focus on personal observations associated with health.Citation5
QoL could be connected to other psychological or social processes. One of the most important is self-stigma.Citation22–Citation25 Self-stigma is a continuing process during which the patient accepts negative evaluations of the social milieu, which are based on social preconceptions of being socially inferior because of the psychiatric disorder.Citation26,Citation27 Given existing social prejudices and stereotypes about psychiatric disorders, patients may feel incompetent, weak-willed, not strong enough to manage their lives, inferior, and burdening those around them, due to their psychological problems.Citation28,Citation29 Patients who agree with common prejudices about psychiatric patients do not believe in their own symptom improvement, feel depressed, and suffer from negative self-esteem.Citation30–Citation33 The worries of prejudices may influence the patient’s efforts to find adequate treatment.Citation34
Ociskova et alCitation34 found that self-stigma was connected with the severity of depression, anxiety, and global evaluations of mental state at the beginning of treatment in individuals with NsD. Participants with a higher degree of self-stigma had lower progress during the therapy. Cinculova et alCitation35 showed no correlation between self-stigma and age of disorder onset, age, or duration of the posthospitalization period. However, there were links between self-stigma and number of previous hospitalizations, severity of the disorder, discontinuation of medication, antidepressant dosage, and the number of psychiatrists visited by the patient. Additionally, self-stigma was negatively associated with adherence to treatment.
Also, Kamaradova et al,Citation36 who inspected 332 patients with schizophrenia, bipolar disorders, depressive disorders, personality disorders, anxiety disorders, or substance-abuse disorders, found positive correlations between self-stigma, number of hospitalizations, severity of disease, lack of partnership, number of psychiatrists visited, doses of antidepressants, and nonadherence to treatment. A negative association was found with level of education.
Patients’ efforts to avoid social stigma may lead to their denial of the fact that they are mentally ill, prioritizing somatic explanation of the causes of the problem, and trying to avoid or delay seeking appropriate psychiatric or psychological treatment.Citation37–Citation39 People with certain coping strategies, such as dissociation, are more inclined to feelings of guilt and shame. These individuals may be vulnerable to developing self-stigma as well, because the primary emotional source of self-stigma is the feeling of shame.Citation40,Citation41
Other critical psychological variables that have a substantial impact on QoL are coping strategies.Citation22,Citation42,Citation43 Coping is a mental process of dealing with distress in different ways, with different approaches to the stressful situation, based on the individual’s resources. As a component of individual tools, coping strategies represent efforts made by a patient to deal with distress.Citation44 They should play an important role by connecting stressors and health consequences in both a physical and psychological way, and they could also relate to psychosocial factors, such as social support, subjective well-being, and resilience.Citation45,Citation46 Coping strategies can be divided according to different theories of stress management. In our study, we follow the parting of positive and negative management strategies in agreement with the authors of the Stress Coping Style Questionnaire (Strategie Zvládání Stresu [SVF] 78). Positive coping (Pos.Cop) and negative coping (Neg.Cop) mechanisms of patients reflected their maladaptive or adaptive problem-solving potential.Citation47
Efficient and flexible strategies for managing stressful situations are reflected positively. Neg.Cop strategies include less flexible strategies in the context of the situation.Citation48 Numerous maladaptive coping strategies are very effective in decreasing symptoms, at least in the short-term perspective. Unfortunately, after long-term use, they result in increased dysfunction and strengthening the disorder.Citation49 Coping strategies may affect well-being, and are closely linked with QoL in many psychiatric disorders.Citation50 The selection of coping strategies is influenced by the type of stressor, the individual’s perception of the threat, available personal resources, and the strategies’ effectiveness.Citation51 Negative cognitive biases, negative self-esteem, and disturbed self-perception in coping with life may significantly weaken the possibility of using adaptive coping strategies.Citation52
Models of NsD propose that inappropriate coping reactions to stressors play an essential part in their pathogenesis. Friedman et alCitation53 pointed out that a positive approach to life may have a promising impact on QoL in connection with Pos. Cop (eg, more considerable effort to seek and accept support from social environment), but the question is whether patients who develop neurotic symptoms, such as anxiety in reaction to stress, can cope with stressful life events adaptively or not. Ociskova et alCitation54 found that patients with an NsD who preferred maladaptive coping strategies profited from combined pharmacotherapy and psychotherapy considerably less than participants with more adaptive coping. Jacofsky et alCitation49 described specific maladaptive coping strategies in different anxiety disorders that inhibited the individual’s capability to disrupt paired associations between the situation and linked symptoms of anxiety, like sensitization, anxious avoidance, escape tendencies, negative reinforcement, and safety behavior.
Aim and hypotheses
This investigation was designed to measure self-stigma, QoL, and coping strategies of NsD outpatients as its first aim, followed by efforts to find out how self-stigma, QoL, and coping strategies are linked to one another, along with other clinical and demographic variables in outpatients with NsDs. Hypotheses were:
QoL will correlate negatively with self-stigma
QoL will correlate positively with Pos.Cop strategies, and negatively with Neg.Cop strategies
QoL will correlate negatively with the severity of the disorder
QoL will vary for different subgroups of NsD
QoL will be significantly related to demographic factors, such as education, partnership, and employment
self-stigma will correlate positively with the severity of the disorder
self-stigma will correlate positively with Neg.Cop and negatively with Pos.Cop strategies
Methods
A total of 25 outpatient psychiatrists confirmed the diagnoses, including and excluding criteria, and administered questionnaires. The investigation was carried out between March 2014 and November 2015. Inclusion criteria were adult age, diagnosis of anxiety disorder, adjustment disorder, somatoform disorder, or OCD according to the ICD10,Citation2 current mental state stabilized, and signing informal consent. Exclusion criteria were acute worsening of symptomatology, current hospitalization, current depressive disorder, mental retardation, substance-abuse disorder, and severe somatic illness. All patients attended the outpatient checkups and were treated with standard medication for anxiety and other NsDs according to the guidelines and principles of good clinical practice.
Assessment instruments
The participants filled out several questionnaires during the routine psychiatric checkup.
Quality of Life Satisfaction and Enjoyment Questionnaire
The Quality of Life Satisfaction and Enjoyment Questionnaire (Q-LES-Q) comprises 93 articles divided into eight sections.Citation55 Participants assess each section by picking out one number from a 5-point Likert scale according to agreement with the statement. Elaboration takes 20–30 minutes. Sections of the questionnaire are physical health, feelings, leisure, household, work, school/study, social relations, general, and a sum of QoL. The Czech version of the Q-LES-Q was validated by Müllerova.Citation56 Analyses indicated high internal consistency (Cronbach’s α=0.8–0.9) and proved the stability of answers over time (test–retest).Citation56 It is possible to get a total of 465 points from all domains together. The therapist guide contains average point values in individual domains, as well as the overall QoL of a healthy population for comparison with mentally ill patients. A healthy population in the therapist guide reached an average of 308 points, and 100% on total QoL corresponds to 465 points.Citation56
Internalized Stigma of Mental Illness scale
The Internalized Stigma of Mental Illness (ISMI) scale has 29 items that assess five domains of self-stigma: alienation, perceived discrimination, stereotype endorsement, social withdrawal, and resistance to stigma.Citation57,Citation58 Internal consistency of the questionnaire is excellent.Citation58 The Czech version (α=0.91) has excellent reliability (split-half method, Spearman–Brown coefficient 0.93) and test–retest consistency at 3 weeks after the initial assessment (r=0.90, P<0.001).Citation59 Therefore, when evaluating ISMI, total and partial scores are subtracted. Respondents can get a total of 116 points within the maximum number of self-stigmatizations.
Clinical Global Impression
The Clinical Global Impression (CGI) measure evaluates the global severity of psychopathology.Citation60 The score is grounded on signs, behaviors, and functioning over the last 7 days, both observed and reported. It is assessed on a 7-point scale from 1 (normal) to 7 (most extremely ill). Assessment is accomplished by an experienced rater via the objective version (ObjCGI). Participants also evaluate themselves with the subjective version (SubjCGI).Citation60 The scale has satisfactory internal consistency.Citation61 Intraclass correlations lie in the range 0.88–0.92.Citation61
Stress Coping Style Questionnaire
The Stress Coping Style QuestionnaireCitation47 (Strategie Zvládání Stresu [SVF] 78) contains 78 items distributed into 13 subscales, each representing a certain way of reacting to a stressful condition. The Czech version has a Cronbach’s α-value of 0.77–0.94.Citation62 Regular use of coping strategies is confirmed with t=40–60:Citation47 t>60 indicates increased usage of coping strategies, and t<40 means decreased usage of suitable strategies. Neg.Cop strategies include escape tendency, perseveration, resignation, and self-accusation. Pos. Cop strategies include underestimation, guilt denial, diversion, compensatory satisfaction, situation control, reaction control, and positive self-instruction (). Only need for social support and active avoidance are not recognized in the total score.Citation62
Table 1 Coping strategies according to the SVF78
Demographic questionnaire
This form contained age, sex, marital status, education, employment status, type of pension, heredity, number of siblings, number of psychiatric hospitalizations, age at disorder onset, duration of attendance at outpatient treatment center, and current medication.
Statistical evaluation and ethics
GraphPad Prism 3 and SPSS 24.0 were used for statistical analysis. Demographic data and mean total scores were calculated using descriptive statistics. The distribution of data, means, medians, and SDs were defined. Means were compared using the unpaired t-test and the Mann–Whitney test. Relationships between specific sets were examined using correlation coefficients (Pearson or Spearman, according to data distribution) and linear regression. Connections between alternative variables were calculated using χ2 or Fisher’s test (sex, marital status, partnership, education). Regression analysis was used to determine the significance of correlations of particular factors. For all statistical tests, a 5% level of significance was established. To evaluate correlation coefficients, the Cohen model of correlation force developed for psychological testing (1988) was used, with a very weak correlation being 0–0.09, weak correlation 0.09–0.29, moderate relationship 0.30–0.49, and strong relationship 0.50–1.00. The study was approved by the local ethics committee of the University Hospital Olomouc. All participants provided signed informed consent. The study was performed in accordance with the Declaration of Helsinki and guidelines for good clinical practice.Citation63
Results
Sample characteristics
A total of 153 outpatients with NsD diagnosed according to ICD10 criteria completed the scales (73.9% women) and questionnaires (150 SVF78, 152 ISMI, 153 Q-LES-Q). The mean age was 48.72±13.41 years. The majority of the patients were married (49.0%). Almost half the patients had secondary education (47.1%) and around a fifth university level (18.3%, ). Family psychiatric history was recognized in 29 participants (34.3%), and 57.5% of patients were employed. In total, 22.8% of participants received disability benefits (full disability benefits [7.8%] and partial disability benefits [14.4%]), 19.6% were retired, and 19.0% of the patients had been hospitalized ().
Table 2 Demographic and clinical characteristics of the patients
Patients with NsD were assessed by their psychiatrist as mildly mentally ill (2.67±1.19) [according ObjCGI]. Similarly, the severity of mental illness was also evaluated by patients (2.31±1.17, ) [according SubjCGI]. Of the total 465 points of the QoL, patient scores averaged 287.9±55.4 (62%, ). ISMI total score averaged 53.49±11.84 (t=43), with lower scores on ISMI – perceived discrimination (7.76±2.58, ). Use of Pos.Cop strategies showed t=50 (12.86±3.19), and Neg.Cop strategies t=60 (13.11±3.88, ).
Diagnostic subgroups
The sample was diagnostically heterogeneous in this category of mental illness, comprising six subgroups of NsD diagnoses: panic disorder and/or agoraphobia, social phobia, GAD and mixed anxiety–depression disorder, adjustment disorder, somatoform disorders, and OCD. The diagnostic subgroups differed significantly only in age and use of Neg. Cop strategies, but not in other measured clinical and psychological variables (). Considering Neg.Cop, in which the disease groups differed significantly, patients with social phobia used the highest use of Neg.Cop strategies from all NsD groups. Patients with panic disorder and agoraphobia had the lowest average use of Neg.Cop strategies ().
Table 3 Differences in assessment scales according to diagnoses
Treatment
A total of 147 patients used psychopharmacological drugs (96.1%), only six did not use any psychiatric medication (3.9%), while 139 (90.9%) reported using prescribed antidepressant medication. Most patients took the medication in prescribed dosages regularly (90.2%), and nine (6.0%) irregularly (occasionally forgetting to take it). Individual doses were not checked in this investigation.
Demographic factors, quality of life, self-stigma and coping strategies
There were no differences between the sexes in disorder severity (measured by ObjCGI or SubjCGI), Q-LES-Q total, ISMI total, or Pos.Cop and Neg.Cop strategies ().
Table 4 Differences according to demographic factors in assessment scales
No statistically significant differences were found among subgroups defined by education in connection with disorder severity evaluated by ObjCGI, SubjCGI, self-stigma measured by ISMI total, Pos.Cop, or Neg.Cop. Nevertheless, there was significant difference among educational subgroups in Q-LES-Q (one-way ANOVA, F148=3.11; P<0.05), more concretely among elementary and university education (). Partnership and employment have no significant influence on subjectively or objectively evaluated severity of the disorder assessed by SubjCGI and ObjCGI, self-stigma assessed by ISMI total, Pos.Cop, or Neg.Cop. QoL represented by Q-LES-Q total showed a statistically significant difference between unemployed and employed participants, while partnership had no significant effect on QoL ().
Quality of life
Subgroups of participants classified by diagnosis did not differ significantly in relation to the severity of the disorder (Kruskal–Wallis test), ISMI (one-way ANOVA), or Pos.Cop variables.
Relationships between QOL and demographic and clinical variables
Many correlations were found between domains of QoL and clinical and demographic factors (). Physical health and feelings correlated negatively with ObjCGI and SubjCGI. The work domain correlated negatively with age, onset of disorder, and ObjCGI. All domains of the Q-LES-Q correlated negatively with ObjCGI and SubjCGI, except for the domain school/study. The sum of Q-LES-Q correlated negatively with SubjCGI and ObjCGI, but not other demographic factors ().
Table 5 Correlations between QoL and demographic or clinical variables
Relationships between self-stigma and quality of life
All Q-LES-Q domains significantly negatively correlated with all ISMI domains, except school/study. Strong correlations were mainly between social withdrawal and the Q-LES-Q total score. The domain of feelings correlated strongly with alienation and stereotype endorsement. ().
Table 6 Relationships between Q-LES-Q domains and self-stigma
Relationships between coping strategies and quality of life
The sum of Pos.Cop significantly positively correlated with all Q-LES-Q domains except school/study. Q-LES-Q domains correlated negatively with Neg.Cop, except for the domains work and school/study (). Q-LES-Q total has either statistically significant positive/negative correlations with all domains, except for the strategy called guilt denial (not taking responsibility for burdens, emphasizes defensive approach).
Table 7 Relationships among Q-LES-Q domains and coping strategies
Self-stigma
Relationships between demographic or clinical variables and self-stigma\
Self-stigma measured by an overall score of ISMI significantly correlated positively with SubjCGI – severity, ObjCGI – severity, and number of hospitalizations. The onset of the disorder correlated only with alienation, duration of disease did not correlate with any ISMI domains, and number of hospitalizations correlated positively with alienation, stereotype endorsement, perceived discrimination, and social withdrawal, but did not correlate with stigma resistance (). SubjCGI and ObjCGI correlated significantly positively with all domains of ISMI except stigma resistance.
Table 8 Relationships between self-stigma and demographic, clinical variables, and coping strategies
Relationships between coping strategies and self-stigma
The sum of Pos.Cop strategies correlated negatively with all domains of self-stigma, just as Neg.Cop strategies correlated positively with all domains of self-stigma measured by ISMI ().
Regression analyses
Because several factors were related to the sum of the Q-LES-Q, multiple stepwise-regression analyses were performed to detect the major critical factors linked to QoL in outpatients with NsD. The dependent variable was Q-LES-Q total. The independent variables were partnership, diagnostic subgroup, number of hospitalizations, ObjCGI, SubjCGI, Pos. Cop, Neg.Cop, employment, and ISMI total. Six steps of backward-regression analysis identified the most significant factors connected with Q-LES-Q total. Those were Pos.Cop, employment, and overall ISMI rating, which explained 32.9% of Q-LES-Q total scores ().
Table 9 Multiple regression analysis with sum of Q-LES-Q or ISMI total as a dependent variable
According to the hypothesis, self-stigma was significantly related to many factors, so we performed the multiple-regression analyses for this as well. Independent factors included age, sex, partnership, education, employment, retirement, onset of disorder, duration of disorder, number of hospitalizations, Q-LES-Q total, Pos.Cop, and Neg.Cop. The most significant factors connected to self-stigma were SubjCGI, Pos.Cop, and Q-LES-Q total, which explained 44.5% of ISMI total (F88=18.673, P<0.001; ).
Mediation analysis
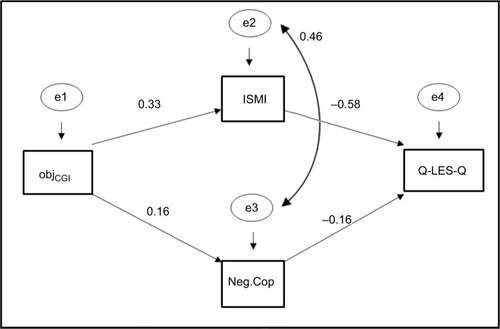
Previous analyses showed that QoL (Q-LES-Q total) might be significantly influenced by Pos.Cop, Neg.Cop, self-stigma (ISMI total), and ObjCGI. Amos software was used for the analysis. The specific method was maximum likelihood, as it is a golden standard in structural equation modeling and robust against normality violations.Citation38 shows standardized estimates of the pathways. The two paths linking ObjCGI with Q-LES-Q were significant. Fit indices also revealed a relatively appropriate model fit (χ21=4.463 [P=0.035], CFI 0.976, GFI 0.985, NFI 0.970, RMSEA 0.154). As such, levels of self-stigma and Neg.Cop strategies influenced QoL.
Figure 1 Mediation-analysis model.
Discussion
This study evaluated relationships among demographic and clinical data, self-stigma, QoL, and coping strategies. The demographic characteristics of the sample were comparable to other outpatient investigations on NsD for age, age at onset, sex, and marital and occupational status.Citation64–Citation66 In the first analysis, relationships between self-stigma and QoL, coping strategies, and demographic data were evaluated. The findings showed that sex, partnership, education, and employment played no role in self-stigma. Identical results were found in other studies where no differences of self-stigma in connection with sex, ethnicity, education, or occupation were shown.Citation36,Citation37,Citation67 Yen et alCitation68 did not confirm associations between age, sex, and self-stigma either. On the other hand, Girma et alCitation69 described higher self-stigma scores in women than in men. The level of self-stigma diminished with increasing levels of education. In the same way, participants who had a partner stigmatized themselves less than those without a partner. Also, the effect of education was important, as participants who had achieved higher education stigmatized themselves less. Marital status also influenced self-stigma. The differences in results could be attributed to different subpopulations of patients with various diagnostic and clinical conditions.
The findings showed that sex and partnership played no role in perceived QoL. However, QoL was different between patients with elementary education and patients with university education. Also, patients with a job displayed statistically significantly higher QoL than unemployed patients. These outcomes are similar to our results with patients with schizophrenia, where employed patients described higher QoL than unemployed patients.Citation70
Hypotheses
QOL will correlate negatively with self-stigma
As in our previous studies in other patient groups, this hypothesis was confirmed.Citation22,Citation24,Citation25,Citation70 All Q-LES-Q domains negatively correlated with all ISMI domains, except school/study (probably caused by the small number of studying participants). It seems that patients who feel more socially excluded because of stigma experience lower QoL to a greater extent. The same applies to feelings of alienation from one another or society because of experiencing stigma. The findings are also in agreement with Vrbova et al,Citation25 who also showed that self-stigma negatively predicted QoL in schizophrenic patients. Multiple-regression and mediation analyses confirm the results from correlations that self-stigma is one of the most powerful factors influencing QoL. Also, our previous studies showed that self-stigma correlated negatively with QoL in schizophrenia and depression.Citation22,Citation70
QOL will correlate positively with positive coping and negatively with negative coping
A hypothesis that QoL correlates positively with Pos.Cop was confirmed in correlation analysis and multiple regression. Pos.Cop strategies were significantly correlated with QoL. As Friedman et alCitation53 pointed out, a positive approach to life may cause a promising effect on QoL in connection with Pos.Cop. However, the question is if patients who develop neurotic symptoms, such as anxiety, in reaction to stress can cope with stressful life events adaptively or not. Patients with social phobia use more Neg.Cop than others in that diagnostic category, so we can assume that Neg.Cop strategies, such as avoidant and escape tendencies and resignations used in this group of NsD due to ill-fated fear of contact with the outside world, are represented to a more considerably maladaptive degree. On the other hand, patients with panic disorder and agoraphobia may be evasive somewhat selectively in certain situations or focus specifically rather than in general. Therefore, they may have the lowest degree of negative management. Jacofsky et alCitation49 pointed out that specific maladaptive coping strategies in different anxiety disorders affect the individual’s capability to break the paired link between circumstances and symptoms of anxiety. Escape tendencies are frequently used by individuals with panic attacks and (social) phobia. Negative reinforcement (social phobia), safety behavior (panic and GAD), sensitization (GAD), and anxious avoidance (GAD, panic disorder, social phobia). Gattino et alCitation71 posited that problem-focused approaches (positive reframing, active coping, using support) increase QoL in all its proportions, whereas emotion-focused coping (self-blame) reduces both psychological and physical QoL. Analogous outcomes were found in our previous studies on patients with schizophrenia and depression.Citation22,Citation43
On the other hand, mediation analysis indicated that QoL was mostly influenced by self-stigma and Neg.Cop strategies, which were both influenced by ObjCGI. It is interesting that according to the regression analysis, one of the main factors correlated with the Q-LES-Q were Pos.Cop strategies, but mediation analysis showed Neg.Cop strategies to be the main factor. In structural equation modeling, their interrelations are analyzed. Based on the theoretical background, several specific models explaining relationships between studied variables were selected. The significance of predictors of Q-LES-Q depends not only on isolated connections between each factor and the dependent variable but also on the structure of the model, ie, the associations among all these variables. As such, although Pos.Cop strategies were considered related to Q-LES-Q in multiple regression, they lost their impact in a model that tries to explain the relationships among the variables. Also, Neg.Cop strategies, which did not pass into the last step of the multiple regression (being pushed out by variables that showed a stronger isolated connection with the dependent variable) were meaningful in the supposed explanatory model. In this model, the factor of Neg.Cop strategies was a significant mediator. Therefore, it is not a strong dependent factor influencing Q-LES-Q, but significantly influences Q-LES-Q as a “middleman” between the severity of the disorder and Q-LES-Q.
QOL will correlate negatively with severity of disorder
Subjectively and objectively evaluated severity of the disorder correlated negatively in most of the Q-LES-Q domains, except school/study. The mean age of the patients in the sample was around 48 years. We also confirmed this hypothesis in our previous study in schizophrenia, where QoL and severity of disorder were significantly related as well.Citation70 Also, in another study, Q-LES-Q total and most Q-LES-Q domains correlated negatively with subjective and objective evaluation of the severity of the disorder in patients with depression.Citation42
When subjectively and objectively evaluated severity of the disorder were put into multiple-regression analysis, they were removed by other more influential factors, such as self-stigma, employment, and Pos.Cop. However, in the mediation-analysis model, which considers interactions between factors, objective assessment of the severity of the disorder was a factor that impacted QoL indirectly through self-stigma and Neg.Cop strategies, as is visible in .
QOL will vary for different groups of neurotic illnesses\
The diagnostic subgroups differed significantly only in age and using Neg.Cop strategies, but not in other measured clinical or psychological variables. As such, such variables as severity of disorder, self-stigma, Pos.Cop, and QoL did not play a significant role in connection with the type of diagnosis. Norberg et alCitation72 showed that patients diagnosed with anxiety disorders stated lower QoL than healthy controls. Reviews by Mogotsi et alCitation73 and Mendlowicz and SteinCitation5 about QoL in different anxiety disorders gave a practically identical portrait of anxiety disorders as disorders that noticeably decrease QoL and psychosocial functioning. A meta-analysis by Olatunji et alCitation74 evaluated dissimilarities in QoL between individuals suffering from anxiety disorders and nonclinical controls. No anxiety-disorder diagnosis was linked with significantly poorer QoL than in any other diagnosis of anxiety disorder. On the contrary, Cramer et alCitation10 investigated the influence of specific anxiety disorders on specific QoL indicators in a typical population. The outcomes indicated that panic disorder and social phobia within the past year, lifetime, and GAD within the past year had an independent influence on QoL when controlling for some sociodemographic variables, physical health, and other DSM-III-R Axis I psychiatric disorders. OCD and specific phobias had only an insignificant effect, and agoraphobia displayed no impact.
QOL will be significantly related to demographic factors, such as education, partnership, and employment
Employment is recognized as an essential factor in QoL. It is such a substantial factor that it passed the regression analysis as an independent factor. However, a connection between QoL and partnership was not found: patients with a partner had the same level of QoL as patients without a partner. Patients with elementary education had significantly lower QoL than university-graduated patients, but education was not a strong enough factor to pass the multiple regression analysis and did not show an effect in the mediation-analysis model.
QoL assessed by Q-LES-Q total showed a statistically significant difference between unemployed and employed patients. Employment was such a substantial factor that it passed the multiple-regression analysis as one of the three most powerful individual factors influencing QoL (with self-stigma and Pos.Cop). Having a job is quite an essential factor in QoL. Being employed was positively related to QoL in schizophrenia patients.Citation75 However, the causal direction of this link is uncertain: employment did not show up as an essential factor in the mediation-analysis model. Our study did not show a correlation of QoL with partnership status of the patient, in opposition to many previous studies.Citation75–Citation77
Self-stigma will correlate positively with severity of disorder
Disorder severity, especially in connection with subjective perception of severity, was significantly associated with self-stigma in all domains. Subjective evaluation of the severity of the disorder also passed multiple-regression analysis as one of the most influential factors influencing self-stigma. Self-stigma is typically greater in participants with more severe symptoms of psychiatric disorder.Citation22,Citation24,Citation35,Citation36,Citation54,Citation67,Citation70,Citation78 It can also relate to the finding that patients with greater self-stigma tend to experience more serious signs of anxiety and depression.Citation58,Citation79
Self-stigma will correlate positively with negative coping and negatively with positive coping strategies
This hypothesis was confirmed in this study. Each of the coping strategies, whether positive or negative, except need for social support, which is considered a neutral strategy, was significantly related to self-stigma and its domains (except stigma resistance, in which most coping strategies were not associated). In the case of avoiding social contact within a self-stigma, positive self-instruction and resignation positively and negatively impacted the positive and negative effects of whether or not a particular individual was looking for a connection and could gain a positive experience with people and environment or whether the patient avoided social contact and hence could stigmatize themselves to a greater extent. Rüsch et alCitation80 showed that persons who stigmatize themselves have a tendency to experience social anxiety. Social anxiety produces and is strengthened by safety and avoidant behavior. Persons with internalized stigma have a tendency to isolate themselves from society.Citation81 In our previous investigation of schizophrenia-spectrum-disorder patients, we also found significant associations between coping strategies and self-stigma. The capacity to use Pos.Cop is linked to decreasing self-stigma, and using Neg.Cop strategies mainly increases the self-stigma.Citation70 We cannot answer questions about causality in this cross-sectional study. Positive self-instruction and resignation are also essential strategies relating to alienation and stereotype agreement.
The regression analysis indicated that the most important aspects associated with QoL were Pos.Cop strategies, employment, and total self-stigma score. Other factors were not strong enough to pass the regression analysis. According to many studies, these factors are important in QoL.Citation5,Citation10,Citation22,Citation53,Citation72–Citation75 It seems that there could exist a significant interaction between having a job as an essential part of QoL and good life feeling, which can be associated with positive management of life events and reduced self-stigma because of a positive perception of one’s self. A cross-sectional study cannot answer questions on interactions and causality among these variables.
Limitations
The study had several shortcomings. The information was derived primarily from self-assessment. The use of such methods is limited by the ability of self-reflection of participants and willingness to be open with their information. Another limitation was the broad range of the NsD and comorbidities that the probands experienced. We did not assess the level of depression in this cross-sectional study, because “current depressive episode” was in the exclusion criteria. Serious somatic illness was also in the exclusion criteria. The patients were also treated with different medications, but the exact doses of the drug used were not monitored in this study.
Conclusion
Self-stigma, QoL, and coping strategies were revealed as important factors for people with NsD. The study confirmed links between self-stigma, QoL, severity of disorder, and coping strategies of outpatients with NsD. Self-stigma was not affected so much by the particular diagnosis. However, participants with higher severity of disorder, higher self-stigma, and Neg.Cop described a lower QoL. Future investigations should focus on paths of self-stigma and the impact of coping strategies on QoL in longitudinal studies of NsD.
Suggestions for practice include conveying the message to clinical workers that self-stigma, coping strategies, and QoL are interconnected. Speaking with patients about their understanding of being a psychiatric patient and being “cured”, understanding their fears of changes in life roles and their self-stigma directly, and encouraging them to change this opinion of themselves can be reasonably central for patients and their recovery.
Acknowledgments
The authors are grateful for the willing cooperation of Dr Jiří Rozkoš from Prostějov, Dr Jan Flídr from Kralupy nad Vltavou, Dr Jana Matějková from Prague, Dr Simona Papežová from Prague, Dr Pavel Tautermann from Prague, Dr Markéta Zemanová from Havlíčkův Brod, Dr Markéta Dobrá from Hrabyně, Dr Zuzana Kozáková from Trutnov (RIAPS association), Dr Tibor Miklóš from Prague, Dr Michaela Zapletalová from Chomutov, Dr Jana Novosadová from Blansko, Dr Jiří Trska from Týn nad Vltavou, Dr Zdeněk Holoubek from Nymburk, Dr Iva Ondráčková from Prague, Dr Andrea Bryčková from Hořice, Dr Jindřiška Masnerová from Beroun, Dr Petr Pastucha from Prostějov, and Dr Hana Lemanová from Brno.
Disclosure
The authors report no conflicts of interest in this work.
References
- International Classification of Disorders (1996) 10th revision. Mental and behavioural disorders: research diagnostic criteriaPraguePrague Psychiatric Centre1996179
- BandelowBMichaelisSEpidemiology of anxiety disorders in the 21st centuryDialogues Clin Neurosci201517332733526487813
- ÚŽIS ČRActivity in branch of psychiatryInstitute of Health Information and StatisticsCzech Republic200527 Available from: https://www.uzis.cz/system/files/zdrroccz2005.pdfAccessed January 30, 2019
- OrmelJJeronimusBFKotovRNeuroticism and common mental disorders: meaning and utility of a complex relationshipClin Psychol Rev2013l33568669723702592
- MendlowiczMVSteinMBQuality of life in individuals with anxiety disordersAm J Psychiatry2000157566968210784456
- AnsseauMDierickMBuntinkxFHigh prevalence of mental disorders in primary careJ Affect Disord2004781495514672796
- StevanovicDImpact of emotional and behavioral symptoms on quality of life in children and adolescentsQual Life Res201322233333722437546
- RaphaelJPaulKPsychological well-being, and anxiety among adolescents analysis along wellness: illness continuumInt J Innov Res Dev20143395401
- RaknesSPallesenSHimleJAQuality of life in anxious adolescentsChild Adolesc Psychiatry Ment Health2017112017133
- CramerVTorgersenSKringlenEQuality of life and anxiety disorders: a population studyJ Nerv Ment Dis2005193319620215729110
- WeidleBJozefiakTIvarssonTThomsenPHQuality of life in children with OCD with and without comorbidityHealth Qual Life Outcomes201412111224382363
- HoffALKendallPCLangleyADevelopmental differences in functioning in youth with social phobiaJ Clin Child Adolesc Psychol201746568669426630122
- LohDAMoyFMZaharanNLMohamedZDisparities in health-related quality of life among healthy adolescents in a developing country - the impact of gender, ethnicity, socio-economic status and weight statusChild Care Health Dev20154161216122625873448
- HollyLELittleMPinaAACaterinoLCAssessment of anxiety symptoms in school children: a cross-sex and ethnic examinationJ Abnorm Child Psychol201543229730924993313
- PantolGSchneierFRQuality of life in anxiety disordersQual Life Ment Disord1997149164
- Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL groupPsychol Med1998285515589626712
- World Health Organization Quality of Life assessment (WHOQOL)Position paper from the World Health OrganizationSoc Sci Med1995411014031498560308
- TaghipourHMoharamzadYMafiARQuality of life among Veterans with war-related unilateral lower extremity amputation: a long-term survey in a prosthesis center in IranJ Orthop Trauma200923752553019633463
- RahimiAMousaviBSoroushMMasumiMMontazeriAPain and health-related quality of life in war veterans with bilateral lower limb amputationsTrauma Mon201217228228624350107
- KatschnigHQuality of life in mental disorders: challenges for research and clinical practiceWorld Psychiatry20065313914517139340
- PowdthaveeNLekfuangfuWNWoodenMWhat’s the good of education on our overall quality of life? A simultaneous equation model of education and life satisfaction for AustraliaJ Behav Exp Econ201554102128713668
- HolubovaMPraskoJMatousekSComparison of self-stigma and quality of life in patients with depressive disorders and schizophrenia spectrum disorders – a cross-sectional studyNeuropsychiatr Dis Treat2016123021303027920539
- PiccoLPangSLauYWInternalized stigma among psychiatric outpatients: associations with quality of life, functioning, hope and self-esteemPsychiatry Res201624650050627821360
- VrbovaKPraskoJOciskovaMQuality of life, self-stigma, and hope in schizophrenia spectrum disorders: a cross-sectional studyNeuropsychiatr Dis Treat20171356757628260904
- VrbovaKPraskoJOciskovaMHolubovaMComorbidity of schizophrenia and social phobia - impact on quality of life, hope, and personality traits: a cross sectional studyNeuropsychiatr Dis Treat2017132073208328831256
- BrookOHvan HoutHPNieuwenhuyseaHde HaanMEffects of coaching by community pharmacists on psychological symptoms of antidepressant users; a randomised controlled trialEur Neuropsychopharmacol200313534735412957333
- CorriganPWRafaczJRüschNExamining a progressive model of self-stigma and its impact on people with serious mental illnessPsychiatry Res2011189333934321715017
- ParcesepeAMCabassaLJPublic stigma of mental illness in the United States: a systematic literature reviewAdm Policy Ment Health201340538439922833051
- OvertonSLMedinaSLThe stigma of mental illnessJ Couns Dev2008862143151
- SireyJABruceMLAlexopoulosGSPerceived stigma as a predictor of treatment discontinuation in young and older outpatients with depressionAm J Psychiatry2001158347948111229992
- TsangHWFungKMChungRCSelf-stigma and stages of change as predictors of treatment adherence of individuals with schizophreniaPsychiatry Res20101801101520493552
- PadurariuMCiobicaAPerssonCStefanescuCSelf-stigma in psychiatry: ethical and bio-psychosocial perspectivesRom J Bioeth2011917682
- UstündağMFKesebirSInternalized stigmatization in bipolar patients: relationship with clinical properties, quality of life and treatment complianceTurk Psikiyatri Derg201324423123924310089
- OciskovaMPraskoJKamaradovaDGrambalALatalovaKSigmundovaZRelationship between internalized stigma and treatment efficacy in mixed neurotic spectrum and depressive disordersNeuro Endocrinol Lett201435871171725702300
- CinculovaAPraskoJKamaradovaDSelf-stigma and discontinuation of pharmacotherapy in patients with anxiety disorders - cross-sectional studyNeuro Endocrinol Lett201738642942629298284
- KamaradovaDLatalovaKPraskoJConnection between self-stigma, adherence to treatment, and discontinuation of medicationPatient Prefer Adherence2016221012891298
- CampDLFinlayWMLLyonsEIs low self-esteem an inevitable consequence of stigma? An example from women with chronic mental health problemsSoc Sci Med200255582383412190273
- FinneySJDiStefanoCNon-normal and categorical data in structural equation modelingHancockGRMuellerRDStructural Equation Modeling: A Second CourseGreenwichInformation Age Publishing2008269314
- BarneyLJGriffithsKMChristensenHJormAFExploring the nature of stigmatising beliefs about depression and help-seeking: implications for reducing stigmaBMC Public Health2009916119228435
- LinkBGPhelanJCStigmaCConceptualizing stigmaAnnu Rev Sociol2001271363385
- AlonsoJBuronABruffaertsRWorld Mental Health ConsortiumAssociation of perceived stigma and mood and anxiety disorders: results from the world mental health surveysActa Psychiatr Scand2008118430531418754833
- HolubovaMPraskoJOciskovaMQuality of life and coping strategies of outpatients with a depressive disorder in maintenance therapy – A cross-sectional studyNeuropsychiatr Dis Treat201714738229339924
- HolubovaMPraskoJHrubyRCoping strategies and quality of life in schizophrenia: cross-sectional studyNeuropsychiatr Dis Treat2015113041304826677331
- Marquez-ArricoJEBenaigesIAdanAStrategies to cope with treatment in substance use disorder male patients with and without schizophreniaPsychiatry Res2015228375275926073284
- FolkmanSMoskowitzJTCoping: pitfalls and promiseAnnu Rev Psychol200455174577414744233
- SkinnerEAEdgeKAltmanJSherwoodHSearching for the structure of coping: a review and critique of category systems for classifying ways of copingPsychol Bull2003129221626912696840
- JankeWErdmannGSVF 78: Eine Kurzform des Stressverarbeitungs-fragebogen SVF 120 [A short form of stress management questionnaire SVF 120]GöttingenGermanHogrefe Verlag für Psychologie2002
- AldwinCMStress, Coping, & Development: An Integrative Perspective2nd ed.New York, NYGuildford Press2007
- JacofskyMDSantosMTNezirogluFThe Maintenance Of Anxiety Disorders: Maladaptive Coping StrategiesMentalHelp.net [online]San DiegoCentersite2009 [cit. 2018-07-02]. Available from: https://www.mentalhelp.net/articles/the-maintenance-of-anxiety-disorders-maladaptive-coping-strategies/Accessed January 15, 2019
- BchKArnoldRRodriguez-RubioBMediating effects of coping in the link between spirituality and psychological distress in a culturally diverse undergraduate sampleMent Health Relig Cult2014172173184
- FolkmanSPersonal control and stress and coping processes: a theoretical analysisJ Pers Soc Psychol19844648398526737195
- ScheierMFMatthewsKAOwensJFDispositional optimism and recovery from coronary artery bypass surgery: the beneficial effects on physical and psychological well-beingJ Pers Soc Psychol1989576102410402614656
- FriedmanLCKalidasMElledgeROptimismEROptimism, social support and psychosocial functioning among women with breast cancerPsychooncology200615759560316287209
- OciskovaMPraskoJKamaradovaDGrambalASigmundovaZIndividual correlates of self-stigma in patients with anxiety disorders with and without comorbiditiesNeuropsychiatr Dis Treat2015111767177926229471
- RitsnerMKursRGibelARatnerYEndicottJValidity of an abbreviated Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-18) for schizophrenia, schizoaffective, and mood disorder patientsQual Life Res20051471693170316119181
- MüllerovaHTranscultural transmission and validation of the quality life questionnaire Q-LES-Q. (in Czech: Mezikulturní přenos a validace dotazníku kvality života Q-LES-Q.)Psychiatrie200158087
- RitsherJBOtilingamPGGrajalesMInternalized stigma of mental illness: psychometric properties of a new measurePsychiatry Res20031211314914572622
- BoydJEAdlerEPOtilingamPGPetersTInternalized stigma of mental illness (ISMI) scale: a multinational reviewCompr Psychiatry201455122123124060237
- OciskováMPraškoJKamarádováDSelf-stigma in psychiatric patients-standardization of the ISMI scaleNeuro Endocrinol Lett201435762463225617887
- GuyWECDEU assessment manual for psychopharmacologyRockvilleU.S. DHEW1976
- ZaiderTIHeimbergRGFrescoDMSchneierFRLiebowitzMREvaluation of the clinical global impression scale among individuals with social anxiety disorderPsychol Med200333461162212785463
- SvancaraJCoping StrategiesTestcentrumPrague2003
- EMEA2002 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500002874.pdfAccessed March 20, 2009
- MichaelTZetscheUMargrafJEpidemiology of anxiety disordersPsychiatry200764136142
- PraskoJKamaradovaDCakirpalogluSPredicting the therapeutic response to intensive psychotherapeutic programs in patients with neurotic spectrum disordersActivitas Nervosa Super Rediviva2015571–23039
- OciskovaMPraskoJLatalovaKKamaradovaDGrambalAPsychological factors and treatment effectiveness in resistant anxiety disorders in highly comorbid inpatientsNeuropsychiatr Dis Treat2016121539155127445474
- LivingstonJDBoydJECorrelates and consequences of internalized stigma for people living with mental illness: a systematic review and meta-analysisSoc Sci Med201071122150216121051128
- YenCFChenCCLeeYTangTCYenJYKoCHSelf-stigma and its correlates among outpatients with depressive disordersPsychiatr Serv200556559960115872170
- GirmaETesfayeMFroeschlGMöller-LeimkühlerAMDehningSMüllerNFacility based cross-sectional study of self stigma among people with mental illness: towards patient empowerment approachInt J Ment Health Syst2013712124004512
- HolubovaMPraskoJHrubyRCoping strategies and self-stigma in patients with schizophrenia-spectrum disordersPatient Prefer Adherence2016101151115827445463
- GattinoSRolleroCDe PiccoliNApplied research quality life: the influence of coping strategies on quality of life from a gender perspective201510689
- NorbergMMDiefenbachGJTolinDFQuality of life and anxiety and depressive disorder comorbidityJ Anxiety Disord20082281516152218424062
- MogotsiMKaminerDSteinDJQuality of life in the anxiety disordersHarv Rev Psychiatry20008627328211133822
- OlatunjiBOCislerJMTolinDFQuality of life in the anxiety disorders: a meta-analytic reviewClin Psychol Rev200727557258117343963
- BouwmansCDe SonnevilleCMulderCLHakkaartvan RoijenLEmployment and the associated impact on quality of life in people diagnosed with schizophreniaNeuropsychiatr Dis Treat2015112125214226316759
- ÜçokAGorwoodPKaradayGEGOFORSEmployment and its relationship with functionality and quality of life in patients with schizophrenia: EGOFORS StudyEur Psychiatry201227642242521592736
- RaY-AKimWHImpact of employment and age on quality of life of individuals with disabilities: a multilevel analysisRehabil Couns Bull2016592112120
- LatalovaKPraskoJKamaradovaDSelf-stigma and suicidality in patients with neurotic spectrum disorder - a cross sectional studyNeuro Endocrinol Lett201435647448025433850
- RitsherJBPhelanJCInternalized stigma predicts erosion of morale among psychiatric outpatientsPsychiatry Res2004129325726515661319
- RüschNCorriganPWPowellKA stress-coping model of mental illness stigma: II. emotional stress responses, coping behavior and outcomeSchizophr Res20091101-3657119237266
- VauthRKleimBWirtzMCorriganPWSelf-efficacy and empowerment as outcomes of self-stigmatizing and coping in schizophreniaPsychiatry Res20071501718017270279