
Abstract
Background
There is a degree of affective interdependence that is considered normal and only becomes pathological if it causes excessive suffering, both for the subject and for those close to them. Our objective was to introduce and psychometrically validate a short and effective affective dependency scale, the Affective Dependence Scale (ADS-9).
Methods
We used a sample of 762 participants (clinical: emotional dependent subjects n = 212, comparison: non-emotionally-dependent addicted subjects n = 272, and general population n = 278) to assess the factor structure, the psychological construct validity and the measurement invariance for the ADS-9 by means of independent exploratory factor analyses for each sample group and subsequent multigroup confirmatory factor analyses.
Results
Our results confirm that ADS-9 is a psychometrically consistent instrument, with construct and clinical validity, as well as configural, metric and scalar invariance across different sample groups (clinical, comparison and general population). A hypothesized two-dimensional structure was confirmed by means of factor analyses. Both sub-scales of this abbreviated form, Submission and Craving, showed a good agreement with the previously validated Relationships and Sentimental Dependencies Inventory (IRIDS-100).
Conclusion
The ADS-9 is a brief instrument that appears to reliably detect the dependent and pathological components of affective dependence. It consists of two sub-scales, describing Submission (adaptation, accommodation, and subjugation) and Craving (imperative need for the other with the presence of disturbing states). We suggest that it is a versatile scale that may be useful for clinicians and researchers.
Introduction
Taking into account the conceptual differences between romantic love and affective dependence, we propose a multiaxial clinical description of affective dependence which includes the following criteria: (a) addictive criteria: extreme affective need with sentimental subordination, emotional emptiness, craving or intense longing for the partner, and withdrawal symptoms in the partner’s absence; (b) bonding criteria (pathology of the relationship): relational style (accommodation to the pathological status), and disabling attachment with impairment of one’s own autonomy; and (c) cognitive-affective criteria (associated psychopathology): mechanisms of denial and self-deception,Citation1 and negative feelings (emotional inescapability, abandonment, failure, and guilt).Citation2
Falling in love is a quasi-addictive phase of natural love, and, consequently, it is not a pathological process. Instead, it enhances the self, causing a greater diversity of self-concept domains along with greater self-efficacy and self-esteem.Citation3 The interdependence between members of every stable couple does not have negative consequences. Rather, marital satisfaction is positively correlated with attunement and dependence, while negatively correlated with idealization, persecution, and distrust.Citation4,Citation5 However, feelings of love can be more intense than desired, as it tends to happen after a breakup, or, contrarily, less intense than expected, as it is the case of long-term relationships.
Several authors assume a parallelism between love and dependence.Citation6–9 For instance, ReynaudCitation10 analyzed whether or not love could be considered a dependency by comparing clinical, neuropsychological, neurobiological, and neuroimaging data. He concluded that the neurophysiologic model for all dependencies applies to affective dependent subjects too, ie the desired object is overrated, the rewarding value and its memory trigger great motivation, simple desire becomes necessity, cortical control becomes insufficient, and, finally, dopamine encodes the value of pleasure in the case of both love and dependencies.
When considering infatuation as a passionate and transitory phase of love, its (pathological) perpetuation would be equivalent to affective dependence where subjects who think that they “care a lot” are actually “caring wrong”. They then turn joy into suffering, interrelation into servitude, and autonomy into dependence.Citation11,Citation12 In this way, we believe that there is a type of affective dependence that is clearly pathological, not so much because of its addictive nature, but because it generates excessive suffering for the subject and for those involved in the relationship. A fine and delicate border between close interdependence and affective dependence is assumed.
Romantic love usually generates psychosocial well-being, although one phase of it (passionate infatuation) can be painful. On the contrary, addiction to love is always painful for the members of the couple with relative intervals of pleasure that feed back into an evidently pathological interrelationship. The main difference between chemical addiction and the so-called love addiction lies in the psychophysical phenomena of drug tolerance, withdrawal, craving and addiction. For a person addicted to love, deprivation triggers devastating longing that can lead to self-destruction. A love addict subject will feel the loss of the loved one as a permanent affliction with sadness, emptiness, de-objectification and, ultimately, a disconsolate mourning. However, love addiction only occurs when the subject shows a repetitive attitude of dependence in successive relationships. The love addict subject does not know how to relate to their partner without establishing a bond of pathological and painful dependence for both of them.
Instruments That Measure Romantic Love and Affective Dependence
The meta-analysis by MasudaCitation13 on 33 empirical studies, and that by Graham and ChristiansenCitation14 on 127 studies and 38,132 participants, allow for an identification of various instruments to evaluate both romantic love and affective dependence. Other meta-analyses support the use of evolutionary and social psychological approaches to understand cognition in romantic relationships.Citation15–19
Among the tests that measure romantic love, Rubin’s Loving and Liking ScalesCitation20 ought to be mentioned first due to their historical value. This instrument consists of 26 items divided into two 13-item scales measuring liking and romantic love. Another instrument is the Individual Capacity To Love (CTL),Citation21 which consists of 41 items and evaluates the ability to love, considering cognition in romantic relationships as a personality trait related to various elements of mental health, such as depression, pathological narcissism, and conflicts. The Trait-Specific Dependence Inventory (TSDI)Citation15 consists of 34 items and six factors: Agreeable/Committed (nine items), Resource Accruing Potential (10 items), Physical Prowess (three items), Emotional Stability (four items), Surgency (five items), and Physical Attractiveness (three items). The Infatuation and Attachment Scales (IAS)Citation22 measure a two-dimensional construction of romantic love through two 10-item subscales: infatuation and attachment. Finally, Cannas et alCitation23 developed the Multidimensional Evaluation of Love Scale (MEVOL) which consists of 21 items.
Among the instruments that measure affective dependence, the Love Addiction Measure (LAS) consists of 20 items and was developed by Hunter et al.Citation24 The Interpersonal Dependency Inventory (IDI)Citation25 evaluates maladaptive dependence with 48 items. From the latter scale, McClintock et alCitation26 constructed a six-item reduced scale. The Emotional Dependence in Dating of young people and adolescents (DEN questionnaire)Citation27 consists of 12 items and 4 factors. The Relationships and Sentimental Dependencies Inventory (IRIDS-100)Citation28 consists of 100 items that measure three types of sentimental dependence: affective or emotional dependence, codependence, and bidependence. Finally, the Passionate Love Scale (PLS)Citation29 stands out as the instrument with the greatest inter-professional presence. With 30 items, the PLS locates the limit between passionate and addictive love according to the nature of some of the components it measures: intrusive thinking, concern for the partner, and negative feelings when things go wrong, among others.
Affective Dependence Components
The craving and submission components are nuclear factors in the conceptualization of affective dependence. However, particularly the craving construct has seen multiple uses and definitions in existing literature, although its most frequent meaning has been an “urgent need to consume”.Citation30–32 In other cases, craving has been equivalent to “longing” or “pain for the loss”.Citation33 Craving has also been associated with both psychological desire and with physical and psychological withdrawal,Citation34 with clear ethnic differences having been reported.Citation16,Citation35 The neurobiology of craving reveals an upregulation of the ventral tegmental dopaminergic pathwayCitation36 that would explain its physical-psychopathological components.
Various authors point out that submission (adaptation, accommodation and subjugation to the other) does not imply pathology.Citation37 However, symptomatic submission has been shown to correlate with depressive symptomsCitation38–40 and also appears to be related to attachment disorganization and/or control strategies.Citation41 It has additionally been related to associated behaviors of hostility,Citation38,Citation42 social anxiety,Citation43 guiltCitation44 and even paranoid beliefs.Citation45 In the area that concerns us here, affective dependence, submission has been associated with fearful attachment, pathological attachment and feelings of loneliness.Citation46
Craving remains an ambiguous concept for the scientific community, without any universally accepted definition, despite compulsive desire being a formal DSM-5 criterion.Citation47 Addictive craving is conceptualized as an “intrusive and overwhelming urge to use drugs”Citation48 while the relational craving is defined as “imperative need of the other with the presence of disturbing states”. It is a multidimensional phenomenon consisting of subjective, behavioral, physiological, and neurochemical correlates.Citation49
The main objective of this study is to develop the Affective Dependence Scale (ADS), a short and powerful instrument to detect and screen for affective dependence, and that allows for the subsequent clinical assessment of this phenomenon. Specifically, we aimed at (a) psychometrically validating the ADS, (b) testing the measurement invariance of the ADS across samples with differential psychopathological characteristics ie clinical (emotional dependent subjects), comparison (non-emotionally-dependent addicted subjects), and general population samples, and (c) determining if these three sample groups differ in their ADS scores.
Materials and Methods
Participants
The total sample used for the study consisted of 762 subjects divided into three groups: clinical, comparison, and general population (Supplementary Data S1).
The clinical group consisted of affective dependent subjects that were identified using the operational criteria that were described by Moral and SirventCitation2 and summarized in the introduction of the present study. To be included in the study, the subjects must had shown four or more of the following eight symptoms for a period of at least six months: extreme affective need with sentimental subordination, emotional emptiness, craving for the partner, withdrawal symptoms in the partner’s absence, accommodation to the pathological status, disabling attachment with impairment of one’s own autonomy, mechanisms of denial and self-deception, and negative feelings. Two subpopulations were included in the clinical population ie emotional dependent and bidependent (emotionally-dependent subjects with substance addiction) subjects. The emotional dependent subjects (those not addicted to psychoactive substances) were diagnosed among the subjects who responded to a press call by the researchers. The bidependent subjects in this group were under treatment at the Fundación Instituto Spiral care centers, in either Madrid or Oviedo (Spain). Each subject was selected by three judges consisting of members of the Fundatión’s multidisciplinary team of psychotherapists (psychologists, physicians and psychiatrist), through a differential diagnosis. There was a high degree of agreement among the three judges, whose decisions were unanimous in all cases. We attribute this agreement to their remarkable clinical experience. The clinical group consisted of 212 subjects (27.82% of the total sample), that were assigned to two different sub-populations: 55.66% bidependent and 44.34% emotional dependent subjects. This population consisted of 63.46% women and the remaining 36.54% men, ranging from 18 to 65 years (M = 39.77; SD = 9.93), 53.66% were single and 29.90% reported having had two partners. Regarding the psychopathological profile, 25.37% were diagnosed with depression, 23.88% with depression and anxiety and 8.96% with anxiety.
The comparison group consisted of 272 non-emotionally-dependent addicted subjects that were under treatment at the Fundación Instituto Spiral care centers, in either Madrid or Oviedo (Spain). They represented 35.70% of the total sample. The comparison population consisted of 50.28% women and the remaining 49.72% were men. Stratification by age yielded a mean of 37.88 years (SD = 10.14) with a range between 19 and 65 years, 54.80% were single and 23.08% declared having had one partner.
Finally, a group consisting of 278 subjects from the general population of the Principality of Asturias (Spain) was selected through random sampling without replacement. The subjects were contacted by the researchers that evaluated the sample frame and considered an age range similar to that of the subjects in the clinical group. The general population represented 36.48% of the total sample, 65.70% being women (34.30% men), within an age range between 18 and 62 (M = 32.65; SD = 12.42). Participants were predominantly single (65.09%), most had finished high school (28.62%) and university studies (higher degree, 23.91%; medium degree, 17.75%), and had lived their entire lives with one (43.54%) or two partners (26.20%).
Instruments
The study aims at evaluating the psychometric properties of an Affective Dependence Scale, which is made up of nine self-applied items extracted from the IRIDS-100 that have been selected after a double (clinical and experimental) decantation.
In a previous study,Citation2 the IRIDS-100 identified a psychological profile in respondents that differed from that of other sentimental dependent groups (codependent and bidependent subjects) as well as of comparison groups (non-emotionally-dependent addicted subjects, non-codependent relatives, and general populations). The IRIDS-100 inventory evaluates the types of sentimental dependence, offering subscales (Affective Dependence, Codependence and Bidependence) and factors of clinical relevance in the relational field. In particular, it identifies a factorial structure integrated by seven explanatory dimensions: Dependent triad, Accommodation, Self-deception, Negative feelings, Characterosis (personality anomaly related to factors of identity and relational boundaries: identification, interaction with the other, weak versus rigid personality boundaries, selfishness, control and domination), Personal history, and Codependent triad (Heterocontrol). The Dependent triad dimension is made up of three factors (Dependence, Sensation seeking, and the IRIDS Craving) and it represents most of the explained variance of the Emotional Dependence construct.Citation2 The process of adaptation of the IRIDS-100 to the Spanish population had adequate psychometric guarantees as well as an adequate internal consistency, with a value of 0.892 for the Dependent Triad dimension and 0.825 for the Characterosis dimension, and with a high Cronbach’s α for the overall test (α= 0.971). The items had saturations greater than 0.80. As a result, this shortened version evaluates the Cognitive-Affective Profile construct through two dimensions, ie Craving (imperious need of the partner with the presence of disturbing states, assessed in five items) and Submission (adaptation, accommodation, and subjugation to the partner, assessed in four items), measured using a five-point Likert scale (strongly disagree to strongly agree).
Procedure
The research was based on a quantitative cross-sectional non-experimental design of a correlational descriptive type.Citation50 The authors contacted the participants and requested their voluntary participation in the study. Informed consent was obtained from the participants, in accordance with the ethical provisions developed in the Declaration of Helsinki. The present study does not apply treatments that could be harmful or affect the fundamental rights of the participants. The Research Ethics Committees of the Principality of Asturias and of the Health Area of Palencia approved this study and the consent process (reference numbers 2022.193 and 2022/033, respectively), and the general recommendations by the Research Ethics Committee of the University of Oviedo (Principality of Asturias, Spain)Citation51 related to the promotion of good practices in research, from the training stage, and ensuring that research meets criteria of rigor, honesty, responsibility, freedom, respect and equality, risk prevention and protection of people, and promoting responsible research, have been followed. All participants were verbally informed of the use of their scoring in the administered self-reports as well as sociodemographic information (age, gender, marital status, education level, number of partners, and health and addiction histories) for research purposes only, and verbal informed consent was individually obtained from each participant before answering the questionnaires. As there were no participants under 18 years of age, it was not necessary to request consent from their parents and guardians. The information was collected by professionals of the therapeutic program of the Fundación Instituto Spiral, where the data were treated with the strictest confidentiality (including the assignment of an identification code). No personal information was used at any stage of the investigation. The risk level of the study was minimal and the study followed general principles associated with autonomy, the right to nonparticipation, confidentiality and right to information. No experimental manipulations of any kind were performed.
Data Analysis
Sex was compared among the study groups by means of a G test, and the age composition was compared among the study groups using a Kruskal Wallis test and subsequent posthoc tests where p-values were adjusted with the Bonferroni method.
Exploratory factor analysis (EFA) was used as a preliminary procedure to determine whether the nine items of the scale were grouped into theoretically significant factors. The EFAs were independently conducted for each of the three study groups (clinical, comparison and general population). Given the ordinal nature of the variables and their lack of uni- and multivariate normality, EFAs were based on the polychoric correlation matrices. In order to explain the structure of the covariances between variables, and after checking sample adequacy (index of determination, Kaiser-Meyer-Olkin index KMO, and Bartlett sphericity test), the robust diagonally weighted least squares estimator (RDWLS)Citation52 was used. Oblique rotation through the Normalized Direct Oblimin method was applied, using a delta value equal to zero for a moderate degree of correlation between the suggested factors. The number of factors to be retained was assessed according to both the Kaiser rule and the theoretically proposed structure. The measure invariance of the factorial structure of the scale was contrasted across samples by means of multigroup confirmatory factor analyses (CFA) using polychoric correlations and the RDWLS estimator. Three invariance levels were considered:Citation53 (1) configural invariance, which requires the factorial structure to be invariant across groups; (2) metric invariance, where factor loadings are forced to be equal across groups; and (3) scalar invariance, which requires the item intercepts to be equal across groups. We considered the more restricted model to fit the data when the CFI difference between more and less constraint models was equal or less than 01.Citation54,Citation55
Measures of central tendency, variability, skewness, kurtosis and percentile information were independently computed for each factor and study group.
The internal consistency of the scale and its subscales was verified using the ordinal alpha reliability coefficientCitation56 for each study group. The analysis of validity of the scale scores was carried out by means comparisons between the different study groups. We used linear models to evaluate the effect of the socio-demographic variables on the affective dependence measures for each study group. For all of these analyses, we used permutation-based approaches to assess statistical significance since heteroscedasticity violated assumptions for likelihood-based algorithms. The p-values of the post hoc comparisons were adjusted using the Bonferroni method.
The congruence between the shortened version proposed here and the IRIDS-100 Affective Dependence Subscale was explored using Spearman correlations corrected for the shared error variance between both scales due to the common items between them.Citation57,Citation58 Since correlation only considers the monotonicity between both forms, we additionally computed the Gower Agreement Index.Citation59,Citation60
Scores on both the general scale and the two subscales were calculated by averaging their item scores.
FACTOR version 10.10.3Citation61 was used for the EFAs; lavaan,Citation62 semToolsCitation63 and semPlotCitation64 R packages were used for the multigroup CFAs; and wPerm,Citation65 lmPermCitation66 and rcompanionCitation67 R packages were used to run comparisons and correlations based on permutation tests. We used R version 4.1.2.Citation68 Shortform 1.1Citation57 and the Gower Agreement Calculator v 1.1.1Citation59 were used to compute Levy’s correlation correction and Gower’s Agreement Indices, respectively, when determining the agreement between the shortened version and the IRIDS-100.
Results
Sample Adequacy and Factorial Structure
Sex ratios of the subjects differed significantly among the three study groups (χ2 = 11.585; df = 2; p = 0.003). Furthermore, the general population sample was significantly younger than the clinical and comparison ones (Kruskal–Wallis H = 50.588; df = 2; p = 0.001; clinical - general population: p = 0.001; comparison - general population: p = 0.001). We attribute these differences in sex and age among our study groups to the sociodemographic characteristics of the three types of populations under study. Addicted subjects, whether bidependent or non-emotionally-dependent addicted subjects, were under treatment at the Fundación Instituto Spiral and represent an intentional sample. In the case of pure emotional addicted subjects (those not addicted to psychoactive substances), they were diagnosed among the subjects who responded to a press call by the researchers, with a greater response from women who, as in similar studies, show to be more receptive and tend to get more involved. The age was lower for the general population due to the greater acceptance of young people to take part in the study.
The study of the dimensionality of the sample was carried out via EFAs independently conducted on each of the study samples. Prior to the analysis, the KMO sample adequacy was calculated and resulted adequate (clinical = 0.867; comparison = 0.895; general population = 0.855), the matrix determinant was significant (clinical = 0.005; comparison = 0.016; general population = 0.019) as was the Bartlett sphericity test (p < 0.001 in all samples).
Indices showed good model fit in all samples (). The factors reached an adequate explained variability in all three study samples, yielding a scale that consisted of nine items assigned to two dimensions or explanatory factors (Submission and Craving) that explained over 60% of the total variance both of them having high saturations (). The scale was, therefore, named Affective Dependence Scale-9 items (ADS-9).
Table 1 Fit Indices of the Exploratory Factor Analysis of the ADS-9 for the Three Study Samples
Table 2 Factorial Structure of the ADS-9 (Rotated Loading Matrix) in the Clinical, Comparison and General Population Samples
Measurement Invariance
We performed multigroup CFAs to assess whether the ADS-9 was invariant across groups of subjects with different psychopathological profiles. Three models were evaluated (ie configural, metric, and scalar), yielding invariance across samples for all the levels considered (configural-metric levels: χ2 difference = 19.876, p = 0.134, CFI scaled difference = 0.003; metric-scalar levels: χ2 difference = 45.068, p = 0.035, CFI scaled difference = 0.007).
The multigroup model had, for each sample, two correlated factors where all the elements loaded in their corresponding factors and the factors were correlated between them. shows the standardized parameter estimates for the final model, which fit was adequate (robust CFI = 0.996, TLI = 0.994, RMSEA = 0.030, SRMR = 0.046, χ2 = 96.146, df = 78, p = 0.080).
Figure 1 Standardized parameter estimates for the multigroup configural measurement model of the ADS-9. (A) clinical, (B) comparison, and (C) general population. All p < 0.001.
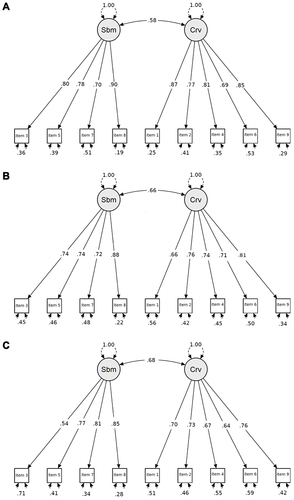
All factor loadings were statistically significant (p < 0.001), and the standardized estimated covariance between Submission and Craving was 0.577 for the clinical sample, 0.656 for the comparison sample, and 0.682 for the general population (all p < 0.001). Basic descriptive statistics for both explored factors and for each of the study samples are shown in .
Table 3 Basic Descriptive Statistics for the Three Study Samples
The matrices of bivariate polychoric correlations between each of the items that integrate both analyzed factors (Submission and Craving) in the clinical, comparison, and general population samples are shown in , respectively.
Table 4 Polychoric Correlations Between the ADS-9 Items for the (A) Clinical, (B) Comparison, and (C) General Population Samples
Internal Consistency
Reliability measured as ordinal alpha reached satisfactory levels both for the total scale (clinical = 0.892; comparison = 0.880; general population = 0.867) and for each of the factors (clinical: Submission = 0.873, Craving = 0.894; comparison: Submission = 0.843, Craving = 0.855; and general population: Submission = 0.822, Craving = 0.826).
Validity of the Scale Scores
Significant differences in both the Submission (F2,759 = 64.510, p < 0.001) and Craving (F2,759 = 26.200, p < 0.001) dimensions were found among the study samples in the expected direction. Specifically, both for the Submission and Craving dimensions, the clinical subpopulation scored higher (p < 0.001) than the other study samples. This shows a greater pathology in the clinical sample in relation to the comparison and general population samples.
Effect of Sex and Age on the ADS-9
We found no significant differences in the ADS-9 scores between men and women either for Submission or Craving in any of the three study groups (Submission: clinical sample F1,206 < 0.001, p = 0.990; comparison sample F1,177 = 2.328, p = 0.129; general population F1,275 = 0.204, p = 0.652; Craving: clinical sample F1,206 = 2.622, p = 0.107; comparison sample F1,177 = 0.307, p = 0.580; general population F1,275 = 3.610, p = 0.058). Submission and Craving scores were only statistically and positively related to age in the general population sample (Submission: clinical sample β = −0.002, p = 0.882; comparison sample β = 0.002, p = 1.000; general population β = 0.006, p < 0.001; Craving: clinical sample β = −0.005, p = 0.902; comparison sample β = 0.006, p = 0.172; general population β = 0.010, p = 0.005).
Agreement Between the ADS-9 and the IRIDS-100
Levy’s corrected correlation (r.adj) and the Gower Agreement Index revealed a high congruence between the ADS-9 and the IRIDS-100 Affective Dependence Subscale (clinical sample: r.adj = 0.756, Gower index = 0.919; comparison sample: r.adj = 0.780, Gower index = 0.916; general population: r.adj = 0.571, Gower index = 0.924).
Discussion
Our results indicate that the ADS-9 is an instrument through which the dependent and pathological components of affective dependence can be identified. This assessment is completed with the ADS-9 subscales (Submission and Craving) that offer a more specific clinical analysis of the associated psychopathology in an accurate and quick way. The ADS-9 has two undeniable merits: it is brief and it detects affective dependence well. However, it is not a test that disentangle the different aspects of affective dependence into subtle factors. In addition, its two sub-scales of Submission and Craving are indicators of psychological qualities of notable interest for the clinician, both to work on derived nosologies and to know the evolutionary state of the affected person.
The predictive capacity of submission has been shown in adult depressionCitation69 and in depression in adolescence through variables of social comparison and submissive behavior.Citation70 In the genral population, women have been found to score higher than men in depression, submissive behavior and external shame,Citation71 although in the affected population contrasting results have been reported. In a study by Zimmerman et al,Citation72 submissive behaviors mediated the relationship between social anxiety and shame in men but not in women, while Gilbert et alCitation73 found no difference in sensitivity to rejection, anger, anhedonia or anxiety between depressed men and women.
From a psychodynamic perspective, authors such as Kealy et alCitation74 unequivocally consider pathological narcissism to be destructive to love. Likewise, Day et alCitation75 point out that deficits in love are intertwined with maladaptive narcissistic problems.
The measurement of craving may be used to predict relapse,Citation76,Citation77 evaluate psychological and pharmacological treatments, predict readiness for discharge,Citation78 and test theories of addiction and desire.Citation79 Tiffany et alCitation80 attribute the relapse more to an automatically learned behavior than to craving. McHugh et al,Citation81,Citation82 instead, found that higher desire was associated with a higher likelihood of alcohol and prescription opioid use.
Limitations
We acknowledge some limitations of this study, being the first of them the collection of the study sample, since patients usually consult for symptoms of sequelae (depression reactive to a frustration in love, for instance). A second limitation has been the lack of awareness, or even lack of acceptance, of the “affective dependence” construct by clinicians, who perceive it as something alien. Patients themselves are also often unaware of a problem that mortifies them while ignoring its root cause. Fortunately, this is being rectified and professionals are gradually acknowledging the “affective dependence” construct which, despite not being included in the international classifications of mental illnesses, has an undoubted presence and is part of the common lexicon of mental health professionals that do not hesitate to identify it and – if necessary – treat it. Finally, this was a cross-sectional study and therefore we were unable to assess metrics such as reliability over time, predictive validity, and sensitivity to change.Citation83 In the same way, craving (and to some extent submission) is a dynamic process that cannot be fully captured in a single “snapshot” and should be further assessed with repeated measures in patients throughout their treatment.Citation84 This cross-sectional nature of the work precluded us from analyzing whether Craving can predict treatment outcome,Citation85 although this does not reduce its value to be considered from a diagnostic-therapeutic perspective.Citation80 As for Submission, although we consider submissive behavior to be an important factor in affective dependence, our research was limited due to its correlational nature.
Taking all of the above into account, the brief scale that we present here may be especially suitable for momentary evaluation studies to assess temporal fluctuations and, in addition, be useful both for research and clinical applications, since it has already been psychometrically validated here.
Conclusion
Given that the ADS-9 is a short, simple and reliable self-administered instrument, we believe that it represents a particularly useful and versatile scale both for clinicians and researchers, and that it may be applicable in studies aiming to detect affective or emotional dependence in a quick (only nine items), reliable and, therefore, practical way, being also suitable for both screening and extensive studies.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Sirvent C, Herrero J, Moral MV, Rodríguez FJ, Boyd RL. Evaluation of self-deception: factorial structure, reliability and validity of the SDQ-12 (self-deception questionnaire). PLoS One. 2019;14:e0210815. doi:10.1371/journal.pone.0210815
- Moral MV, Sirvent CM. Emotional or affective dependencies: aetiology, classification and assessment. Revista Española de Drogodependencias. 2008;33(2):150–167. Spanish.
- Chóliz M, Gómez C. Social emotions II (infatuation, jealousy, envy and empathy). In: Palmero F, Fernández-Abascal EG, Martínez F, Chóliz M, editors. Psychology of Motivation and Emotion. Madrid: McGrawHill; 2002:395–418. Spanish.
- Rimé B. Emotions at the service of cultural construction. Emot Rev. 2020;12(2):65–78. doi:10.1177/1754073919876036
- Solano L, Nicolò AM, Di Trani M, et al. The marital love relationship: construction and preliminary validation on 610 subjects of a psychoanalytically derived inventory. Psychoanal Psychol. 2012;29(4):408–428. doi:10.1037/a0030206
- Coppin G, Pool ER. Affect, “wanting” and relevance: commentary on Lutz et al (2020). Addict Behav. 2021;115:106792. doi:10.1016/j.addbeh.2020.106792
- Fisher HE. The tyranny of love: love addiction—An anthropologist’s view. In: Rosenberg KP, Curtiss Feder L, editors. Behavioral Addictions: Criteria, Evidence, and Treatment. Elsevier Academic Press; 2014:237–265.
- Kemp R, Butler A. Love, hate and the emergence of self in addiction recovery. Existent Anal. 2014;25(2):257–268.
- Stauffer CS, Woolley JD. Can we bottle psychosocial treatments for addiction? The role of oxytocin. J Clin Psychiatry. 2014;75(9):3–4. doi:10.4088/JCP.14ac09437
- Reynaud M. Does love addiction exist? Ann Med Psychol. 2010;168(7):516–523. French.
- Wegmann R, Brand M. Affective and cognitive processes involved in behavioral addictions. Addict Behav. 2021;118:106885. doi:10.1016/j.addbeh.2021.106885
- Sirvent CM. Does love addiction exist? In: Laespada MT, Estevez A, editors. Are There Addictions Without Substances? Serie Drogodependencias. Vol. 29. I. Deusto Publicaciones. Universidad de Deusto; 2014. Spanish.
- Masuda M. Meta-analyses of love scales: do various love scales measure the same psychological constructs? Jpn Psychol Res. 2003;45(1):25–37. doi:10.1111/1468-5884.00030
- Graham JM, Christiansen K. The reliability of romantic love: a reliability generalization meta-analysis. Pers Relatsh. 2009;16(1):49–66. doi:10.1111/j.1475-6811.2009.01209.x
- Ellis BJ, Simpson JA, Campbell L. Trait-specific dependence in romantic relationships. J Pers. 2002;70(5):611–659. doi:10.1111/1467-6494.05019
- Eriksson K, Strimling P. Using models to predict cultural evolution from emotional selection mechanisms. Emot Rev. 2020;12(2):79–92. doi:10.1177/1754073919890914
- Fisher HE, Brown LL, Aron A, Strong G, Mashek D. Reward, addiction, and emotion regulation systems associated with rejection in love. J Neurophysiol. 2010;104(1):51–60. doi:10.1152/jn.00784.2009
- Fletcher GJO, Kerr PSG. Through the eyes of love: reality and illusion in intimate relationships. Psychol Bull. 2021;136(4):627–658. doi:10.1037/a0019792
- Mashek D, Aron A, Fisher H. Identifying, evoking, and measuring intense feelings of romantic love. Represent Res Soc Psychol. 2000;24:48–55.
- Rubin Z. Measurement of romantic love. J Pers Soc Psychol. 1970;16(2):265–273. doi:10.1037/h0029841
- Kapusta ND, Jankowski KS, Wolf V, et al. Measuring the capacity to love: development of the CTL-inventory. Front Psychol. 2018;9:1115. doi:10.3389/fpsyg.2018.01115
- Langeslag SJE, Muris P, Franken IH. Measuring romantic love: psychometric properties of the infatuation and attachment scales. J Sex Res. 2013;50(8):739–747. doi:10.1080/00224499.2012.714011
- Cannas AF, Veneziani CA, Bisiacchi PS. The Multidimensional Evaluation of Love (MEVOL) Scale: development and preliminary validation. TPM Test Psychom Methodol Appl Psychol. 2019;26(2):249–269.
- Hunter MS, Nitschke C, Hogan L. A scale to measure love addiction. Psychol Rep. 1981;48(2):582. doi:10.2466/pr0.1981.48.2.582
- Hirschfeld RMA, Klerman GL, Harrison M, et al. A measure of interpersonal dependency. J Pers Assess. 1977;41(6):610–618. doi:10.1207/s15327752jpa4106_6
- McClintock AS, McCarrick SM, Anderson T, Himawan L, Hirschfeld R. Development and validation of a six-item version of the Interpersonal Dependency Inventory. Assessment. 2017;24(3):360–370. doi:10.1177/1073191115605178
- Urbiola I, Estévez A, Iraurgi I. Emotional dependence in dating of young people and adolescents (DEN): development and validation of an instrument. Ansiedad y Estrés. 2014;20(2–3):101–114. Spanish.
- Sirvent CM, Moral MV. Construction and validation of the Inventory of Interpersonal Relationships and Sentimental Dependencies (IRIDS-100). Salud Drogas. 2018;18(2):35–47. Spanish.
- Hatfield E, Sprecher S. Measuring passionate love in intimate relations. J Adolesc. 1986;9(4):383–410. doi:10.1016/S0140-1971(86)80043-4
- Billieux J, Van der Linden M, Ceschi G. Which dimensions of impulsivity are related to cigarette craving? Addict Behav. 2007;32(6):1189–1199. doi:10.1016/j.addbeh.2006.08.007
- Brockmeyer T, Hahn C, Reetz C, Schmidt U, Friederich H. Approach bias modification in food craving—A proof of concept study. Eur Eat Disord Rev. 2015;23(5):352–360. doi:10.1002/erv.2382
- Meadows A, Nolan LJ, Higgs S. Self-perceived food addiction: prevalence, predictors, and prognosis. Appetite. 2017;114:282–298. doi:10.1016/j.appet.2017.03.051
- Boddez Y. The presence of your absence: a conditioning theory of grief. Behav Res Ther. 2018;106:18–27. doi:10.1016/j.brat.2018.04.006
- Brousse G, de Chazeron I. Craving: keys to understanding. Alcoologie Et Addictologie. 2014;36(2):105–115. French.
- Williams M, Jayawickreme N, Sposato R, Foa EB. Race-specific associations between trauma cognitions and symptoms of alcohol dependence in individuals with comorbid PTSD and alcohol dependence. Addict Behav. 2012;37(1):47–52. doi:10.1016/j.addbeh.2011.08.008
- Johnson B. Psychological addiction, physical addiction, addictive character, and addictive personality disorder: a nosology of addictive disorders. Can J Psychoanal. 2003;11(1):135–160.
- Wismeijer AAJ, Van assen MALM. Psychological characteristics of BDSM practitioners. J Sex Med. 2013;10(8):1943–1952. doi:10.1111/jsm.12192
- Allan S, Gilbert P. Submissive behaviour and psychopathology. Br J Clin Psychol. 1997;36(4):467–488. doi:10.1111/j.2044-8260.1997.tb01255.x
- Gilbert P, Pehl J, Allan S. The phenomenology of shame and guilt - an empirical-investigation. Br J Med Psychol. 1994;67:23–36. doi:10.1111/j.2044-8341.1994.tb01768.x
- Troop NA, Allan S, Treasure JL, Katzman M. Social comparison and submissive behaviour in eating disorder patients. Psychol Psychother. 2003;76(3):237–249. doi:10.1348/147608303322362479
- Liotti G. Attachment disorganization and the controlling strategies: an illustration of the contributions of attachment theory to developmental psychopathology and to psychotherapy integration. J Psychother Integr. 2011;21(3):232–252. doi:10.1037/a0025422
- Bird T, Tarsia M, Schwannauer M. Interpersonal styles in major and chronic depression: a systematic review and meta-analysis. J Affect Disord. 2018;239:93–101. doi:10.1016/j.jad.2018.05.057
- Gilbert P, Allan S, Trent D. A short measure of social and separation anxiety. Br J Med Psychol. 1996;69:155–161. doi:10.1111/j.2044-8341.1996.tb01860.x
- O’Connor LE, Berry JW, Weiss J, Gilbert P. Guilt, fear, submission, and empathy in depression. J Affect Disord. 2002;71(1–3):19–27. doi:10.1016/S0165-0327(01)00408-6
- Pinto-Gouveia J, Matos M, Castilho P, Xavier A. Differences between depression and paranoia: the role of emotional memories, shame and subordination. Clin Psychol Psychother. 2014;21(1):49–61. doi:10.1002/cpp.1818
- Pincus AL, Gurtman MB. The 3 faces of interpersonal dependency - structural-analyses of self-report dependency measures. J Pers Soc Psychol. 1995;69(4):744–758. doi:10.1037/0022-3514.69.4.744
- Bergeria CL, Strickland JC, Justin C, Huhn AS, Strain EC, Dunn KE. A preliminary examination of the multiple dimensions of opioid craving. Drug Alcohol Depend. 2021;219:108473. doi:10.1016/j.drugalcdep.2020.108473
- Kakko J, Alho H, Baldacchino A, Molina R, Nava FA, Shaya G. Craving in opioid use disorder: from neurobiology to clinical practice. Front Psychiatry. 2019;10:592. doi:10.3389/fpsyt.2019.00592
- Mezinskis JP, Honos-Webb L, Kropp F, Somoza E. The measurement of craving. J Addict Dis. 2001;20(3):67–85. doi:10.1300/J069v20n03_07
- Hernández R, Fernández C, Baptista P. Research Methodology. Mexico DF: McGraw-Hill; 1998. Spanish.
- Consejo de Gobierno de la Universidad de Oviedo. Boletín Oficial Del Principado de Asturias. Resolution of June 25, 2019, of the Governing Council of the University of Oviedo, approving the regulations of the Research Ethics Committee; 2019. Spanish.
- Asparouhov T, Muthen B. Simple second order chi-square correction; 2010. Available from: https://www.statmodel.com/download/WLSMV_new_chi21.pdf. Accessed September 13, 2021.
- Milfont TL, Fischer R. Testing measurement invariance across groups? Applications in cross-cultural research. Int J Psychol Res. 2010;3:111–121. doi:10.21500/20112084.857
- Fischer R, Karl JA. A primer to (cross-cultural) multi-group invariance testing possibilities in R. Front Psychol. 2019;10:1507. doi:10.3389/fpsyg.2019.01507
- Hirschfeld G, von Brachel R. Improving Multiple-Group confirmatory factor analysis in R – a tutorial in measurement invariance with continuous and ordinal indicators. Pract Assess Res Evaluat. 2014;19:7.
- Zumbo BD, Gadermann AM, Zeisser C. Ordinal versions of coefficients alpha and theta for Likert rating scales. J Mod Appl Stat Methods. 2007;6(1):21–29. doi:10.22237/jmasm/1177992180
- Barrett P. Levy’s Short Vs. Long Form Corrected Correlation. Auckland: Advanced Projects R&D Ltd; 2015.
- Levy P. Correction for spurious correlation in evaluation of short-form tests. J Clin Psychol. 1967;23(1):84–86. doi:10.1002/1097-4679(196701)23:1<84::AID-JCLP2270230123>3.0.CO;2-2
- Barrett P. Gower Program Help File. Auckland: Advanced Projects R&D Ltd; 2012.
- Gower JC. A general coefficient of similarity and some of its properties. Biometrics. 1971;27:857–871. doi:10.2307/2528823
- Lorenzo-Seva U, Ferrando PJ. FACTOR A computer program to fit the exploratory factor analysis model. Behav Res Methods. 2006;38:88–91. doi:10.3758/BF03192753
- Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Softw. 2012;48(2):1–36. doi:10.18637/jss.v048.i02
- Jorgensen TD, Pornprasertmanit S, Schoemann AM, Rosseel Y. semTools: useful tools for structural equation modeling. R package version 0.5–5; 2021. Available from: https://CRAN.R-project.org/package=semTools. Accessed September 13, 2021.
- Epskamp S. semPlot: path diagrams and visual analysis of various SEM packages’ output. R package version 1.1.2; 2019. Available from: https://CRAN.R-project.org/package=semPlot. Accessed September 13, 2021.
- Weiss NA. wPerm: permutation tests. R package version 1.0.1; 2015. Available from: https://CRAN.R-project.org/package=wPerm. Accessed September 13, 2021.
- Wheeler B, Torchiano M. lmPerm: permutation tests for linear models. R package version 2.1.0; 2016. Available from: https://CRAN.R-project.org/package=lmPerm. Accessed September 13, 2021.
- Mangiafico S. Rcompanion: functions to support extension education program evaluation. R package version 2.4.1; 2021. Available from: https://CRAN.R-project.org/package=rcompanion. Accessed September 13, 2021.
- R Core Team. R: a language and environment for statistical computing. R foundation for statistical computing, Vienna, Austria; 2021. Available from: https://www.R-project.org/. Accessed September 13, 2021.
- Öngen DE. The relationships between self-criticism, submissive behavior and depression among Turkish adolescents. Pers Individ Dif. 2006;41(5):793–800. doi:10.1016/j.paid.2006.03.013
- Puissant SP, Gauthier JM, Van Oirbeek R. The contribution of social rank and attachment theory to depression in a non clinical sample of adolescents. Span J Psychol. 2011;14(2):832–842. doi:10.5209/rev_SJOP.2011.v14.n2.30
- Cheung MSP, Gilbert P, Irons C. An exploration of shame, social rank and rumination in relation to depression. Pers Individ Dif. 2004;36(5):1143–1153. doi:10.1016/S0191-8869(03)00206-X
- Zimmerman J, Morrison AS, Heimberg RG. Social anxiety, submissiveness, and shame in men and women: a moderated mediation analysis. Br J Clin Psychol. 2015;54(1):1–15. doi:10.1111/bjc.12057
- Gilbert P, Irons C, Olsen K, Gilbert J, McEwan K. Interpersonal sensitivities: their links to mood, anger and gender. Psychotherapy. 2006;79:37–51.
- Kealy D, Ogrodniczuk JS. Pathological narcissism and the obstruction of love. Psychodyn Psychiatry. 2014;42(1):101–120. doi:10.1521/pdps.2014.42.1.101
- Day JS, Townsend ML, Grenyer BFS. Living with pathological narcissism: core conflictual relational themes within intimate relationships. BMC Psychiatry. 2022;22(1):1–11. doi:10.1186/s12888-021-03660-x
- Doherty K, Kinnunen T, Militello FS, Garvey AJ. Urges to smoke during the first month of abstinence: relationship to relapse and predictors. Psychopharmacology. 1995;119:171–178. doi:10.1007/BF02246158
- Killen JD, Fortmann P. Craving is associated with smoking relapse: findings from three prospective studies. Exp Clin Psychopharmacol. 1997;5:137–142. doi:10.1037/1064-1297.5.2.137
- Anton RF, Drobes DJ. Clinical measurement of craving in addiction. Psychiatr Ann. 1998;28:553–560. doi:10.3928/0048-5713-19981001-06
- Hartz DT, Frederick-Osborne SL, Galloway GP. Craving predicts use during treatment for methamphetamine dependence: a prospective, repeated-measures, within-subject analysis. Drug Alcohol Depend. 2001;63:269–276. doi:10.1016/S0376-8716(00)00217-9
- Tiffany ST, Wray JM. The clinical significance of drug craving. Addict Rev. 2012;1248:1–17.
- McHugh RK, Fitzmaurice GM, Carroll KM, et al. Assessing craving and its relationship to subsequent prescription opioid use among treatment-seeking prescription opioid dependent patients. Drug Alcohol Depend. 2014;145:121–126. doi:10.1016/j.drugalcdep.2014.10.002
- McHugh RK, Fitzmaurice GM, Griffin ML, Anton RF, Weiss RD. Association between a brief alcohol craving measure and drinking in the following week. Addiction. 2016;111(6):1004–1010. doi:10.1111/add.13311
- McHugh RK, Trinh CD, Griffin ML, Weiss RD. Validation of the craving scale in a large sample of adults with substance use disorders. Addict Behav. 2021;113:106651. doi:10.1016/j.addbeh.2020.106651
- Livacic-Rojas P, Vallejo G, Fernández P. Analysis of type I error rates of univariate and multivariate procedures in repeated measures designs. Commun Stat Simul Comput. 2010;39(3):624–640. doi:10.1080/03610910903548952
- Kleykamp BA, De Santis M, Dworkin RH, et al. Craving and opioid use disorder: a scoping review. Drug Alcohol Depend. 2019;205:107639. doi:10.1016/j.drugalcdep.2019.107639