
Abstract
Purpose
The impact of the COVID-19 pandemic on the working, personal and health conditions of health professionals has been highlighted, although it is necessary to verify whether certain instruments used in research on this topic have sufficient psychometric support for their use. This need was the main motivation for undertaking the present study. We aimed to analyse the psychometric properties of the Utrecht Work Engagement Scale (UWES-9) in a sample of active health care workers during the pandemic.
Patients and Methods
A cross-sectional study was conducted from March to August 2020 with 2326 active health care workers (78.7% women). The instruments that were applied included the UWES-9 scale, the Sense of Coherence scale (SOC-13), the Goldberg General Health Questionnaire (GHQ-12) and an item on self-perceived health.
Results
The three-factor structure related to the correlation of pairs of errors presented the best fit. The reliability of the UWES-9 was highlighted by the adequate internal consistency of the items, the existence of invariance according to gender, and its convergent and discriminant validity.
Conclusion
The findings of this work support the use of the UWES-9 to assess the work engagement of health personnel during the COVID-19 pandemic and identify it as an adequate measure of this psychological variable and the constructs that comprise it.
Introduction
The global labour market has suffered a considerable shock since the declaration of the COVID-19 pandemic in March 2020, and the impacts have varied among economic sectors, geographical areas, and labour sectors.Citation1
The pandemic has affected other work aspects and organizations. Thus, among the workers that experienced the most significant impact of the pandemic on their working, personal and health conditions, health personnel undoubtedly stand out. They were positioned in the front line against COVID-19 and faced a high risk of infection due to intense and long work hours, psychological discomfort, exhaustion, and fatigue, among other factors.Citation2 Research conducted throughout the pandemic showed the impact on the mental health of health professionals, especially female health workers, providing evidence of the anxiety, depression, worry, sleep disorders and stress that they experienced.Citation3,Citation4
A variable that has been related to the state of mental health in the work environment during the COVID-19 crisis is work engagement (WE).Citation5 This construct refers to “a positive, fulfilling, affective-motivational state of work-related well-being that can be seen as the antipode of job burnout”.Citation6 It is conceived as a persistent affective-cognitive state that is related to three concepts: Vigour, or high levels of energy, will and mental resistance; Dedication, or feeling enthusiastic about and challenged at work; and Absorption, that is, full and exclusive concentration on the tasks to be performed.Citation7
To measure this construct, a self-report questionnaire was designed: the Utrecht Work Engagement Scale (UWES). The UWES initially consisted of 24 items (UWES-24) answered with a seven-point response scale. However, after a psychometric evaluation with two types of samples (university students and Spanish workers), items were reduced to 17 (UWES-17).Citation7,Citation8 The authors concluded that the three-factor structure adequately fit the data of both samples, although a high correlation was detected between the latent factors, especially between vigour and absorption.Citation7 Since the publication of this scale, which is available in 21 languages, proposals for shorter versions have emerged, including that of a nine-item version, the UWES-9.Citation9–11
The UWES-9 scale has been widely used in the scientific literature with samples from several countries worldwide: Europe, Asia, Africa, the Americas and Oceania.Citation11–15 Among other issues, the psychometric properties of this instrument were studied, providing different models of its internal structure. A one-factor model has been proposed that shows a single dimension of WE that has been applied in various labour and geographical contexts, including Serbian workers, community health workers in Sierra Leone, teachers in the Dominican Republic, and other Spanish-speaking areas of the Caribbean, and working women in Sweden.Citation16–19 Similarly, studies have provided evidence of a better fit of the three-factor modelCitation10,Citation13,Citation20,Citation21 based on the original proposal of 17 items.Citation7 Later, this same author conducted a psychometric study with workers in different industries from Finland, Japan, the Netherlands, Spain and Belgium.Citation13 Analyses of other structures have also been carried out, such as a model of two correlated factors (dedication and vigour forming one factor and absorption forming a second factor) and a model with a second-order latent factor.Citation10,Citation20
Thus, the present study arises from the lack of consensus in the scientific literature regarding the factorial structure of the UWES-9 and the need to extract evidence of its validity when used in a particular historical moment, such as during a health crisis. Therefore, we aim to study the UWES-9 in health workers, as there is special concern about this situation during the pandemic for being working close to patients and living potentially distressing and hazardous situations. Thus, the objective of this work was to analyse the psychometric properties of the UWES-9 in a sample of health care professionals who were active during the COVID-19 pandemic in Spain. For this purpose, this study was intended to cover the following four aims: to examine the factorial structure of the scale; to determine the model with the best fit; to analyse the reliability; to study the factorial invariance (FI) and the differential functioning of the items as a function of gender and analyse the relationship of WE with the sense of coherence, psychological distress, and perceived health for trying to provide evidence of convergent validity.
Materials and Methods
Participants
The sample was taken from a research project conducted in Spain which aimed to assess the impact of the COVID-19 pandemic on the emotional well-being and psychological adjustment of the general population and health professionals.Citation22,Citation23 The inclusion criteria were: (i) being an active health care professional at the time of their participation in the study; (ii) being of legal age; and (iii) having a 100% response rate for the total questionnaire. The sample of the present study consisted of 2326 participants (78.7% women). The mean age was 42.8 years (SD = 11.5). The majority marital status was married or living with a partner (67.2%) and most of the sample (60.2%) had university studies. The sample comprised nurses (59.1%), physicians (23.8%) and other health professionals (17.1%) with more than 10 years of experience in their work environment (68.8%).
Instruments
Sociodemographic variables; Questions about gender, age, marital status, educational level, professional profile, and years of experience in the sector were included.
Utrecht Work Engagement Scale (UWES-9)Citation11 in its Spanish version;Citation24 a self-administered scale composed of nine items that evaluate WE. Items are answered with a Likert-scale from 0 (never) to 6 (always/every day). The instrument provides three partial scores and a total score. The partial scores are obtained by adding the items corresponding to each subscale (vigour: Items 1, 2, 5; dedication: Items 3, 4, 7; absorption: Items 6, 8, 9) and dividing the result by the number of items that compose it. The total score ranges from 0 to 6 points. A higher score indicates greater WE.
Sense of Coherence Scale (SOC-13)Citation25,Citation26 in its Spanish version;Citation27 a self-administered scale composed of 13 items with semantic differences. A response scale ranging from 1 (least frequent) to 7 (most frequent) is used to evaluate the frequency with which participants encounter certain experiences. The items are grouped into three dimensions (meaningfulness, comprehensibility, and manageability). A higher score indicates a higher level of coherence. Cronbach’s alpha obtained in this study was 0.83 (0.58 for meaningfulness, 0.70 for comprehensibility and 0.62 for manageability).
General Health Questionnaire (GHQ-12)Citation28 in its Spanish version;Citation29 a self-administered scale composed of 12 items that evaluate psychological distress through a Likert-type scale with 4 response options. The first two options receive a score of 0, while the remaining two are scored as 1. A higher score is related to a higher level of psychological distress. The internal consistency obtained in this study was α = 0.83.
Self-perceived health; An item with five response options evaluated the participants’ self-perceived health (very bad, bad, not so good, good, very good). This indicatorCitation30 has been used in different studies related to the COVID-19 and other pandemics.Citation31–33
Procedure
Thirteen days after the start of the lockdown in Spain, data collection began with an online questionnaire administered through the Qualtrics® XM survey platform. Snowball sampling was employed to disseminate the study through the social networks and email lists of professional groups that were invited to participate (eg, the General Council of Physicians, Nursing and the Beturia Andalusian Foundation for Health Research, among others). When participants accessed the survey link, they were presented with the study information and an informed consent form, which they had to accept to access the questionnaire. The anonymous and voluntary nature of participation was indicated, as was the possibility of leaving the study at any time. The confidentiality and protection of the collected data were guaranteed. Data collection took place from March 26 to August 27, 2020. This study received approval from the Research Ethics Committee of Huelva, belonging to the Regional Ministry of Health of Andalusia, Spain (PI 036/20).
Data Analysis
Analyses were carried out with SPSS 26.0 and AMOS 25.0 software. Exploratory univariate and multivariate analyses of the data were carried out to detect extreme values and to study normality using the Kolmogorov–Smirnov test and the Mardia test. The asymmetry and kurtosis indicators of the UWES-9 items were also explored, as was the existence of a ceiling and floor effect for each of them. To study the evidence of validity based on the internal structure of the scale, confirmatory factor analysis (CFA) was performed to test the fit of the following models: (i) a global factor, (ii) two correlated factors, (iii) three correlated factors and (iv) three first-order factors and a second-order factor (WE). Given the non-normal nature of the data, the robust Maximum Likelihood method was used providing the following fit indices: Satorra-Bentler goodness-of-fit χ² statistic (χ²S-B), Comparative Fit Index (CFI), Goodness-of-Fit Index (GFI), Adjusted Goodness-of-Fit Index (AGFI), Non-Normalized Fit Index (NNFI), Akaike’s Information Criterion (AIC), Root Mean Square Error of Approximation (RMSEA) and the Standardized Root Mean Square Residual (SRMR). CFI, GFI and NNFI values above 0.90 are indicative of acceptable fit.Citation34 However, Hu and BentlerCitation35 recommend values ≥ 0.95. RMSEA values lower than 0.06 are also indicative of a good fit.
Considering the model with the best fit, internal consistency was studied by providing item-test correlations and Cronbach’s alpha coefficient. Additionally, we examined the FI by gender using multigroup analysis. Given the difference in the number of men (n = 495) and women (n = 1831) in the sample, a random sample of 495 women was drawn to match both subsamples for the factorial equivalence analysis. FI was progressively tested at different levels: configural, weak, strong, and strict. To accept the equivalence of the factors and compare nested models, a change in CFI ≥ 0.01 was considered to adopt the least limited model and reject the most restrictive model.Citation36 Furthermore, to provide more validity evidence based on the internal structure, differential item functioning (DIF) was analysed using EASY-DIFCitation37 to improve the validity of scale interpretations. Mantel–Haenszel statistical test was performed as a comparative criterion for the groupsCitation38 as well as the p-value and its standard deviation (SPD). Significant p-values (< 0.05) were considered evidence of the existence of a DIF. In addition, the SPD indicator was interpreted to compare the expected mean scores between groups on each item in relation to the total score of the scale. In this case, a negative value indicated that the mean score would be lower in women (focal group) than in men (reference group). Furthermore, for those items that showed DIF, we compared the mean scores of the two independent groups (men and women) by calculating the Student’s t. Finally, to provide evidence of convergent validity through the relationship with other relative variables, the associations between scores on the UWES-9 scale and the SOC-13, the GHQ-12 and the self-perceived health were studied.
Results
Item Analysis
shows the means, standard deviations, asymmetry, and kurtosis values obtained for each item on the UWES-9 scale. As shown in , Item 7 had the highest score (M = 4.8; SD = 1.3), while the lowest score was obtained for Item 5 (M = 3.4; SD = 1.7). The asymmetry values of the distribution of the scores ranged from −1.2 to −0.3, and the kurtosis values were between −1.0 and 0.9. Although none of the items presented a floor effect (percentages less than 15% in all cases), a ceiling effect was observed for Items 7, 8, 9.
Table 1 Descriptive Statistics of the UWES-9
Confirmatory Factor Analysis
The fit indices for each of them are provided in . The model with three correlated factors showed the best fit [χ²S-B = 981.04; CFI = 0.92; RMSEA = 0.13]. Considering the modification indices obtained in this structure, we proceeded to correlate errors 1–2 and 8–9 to improve the fit of the model [χ²S-B = 331.02; CFI = 0.97; RMSEA = 0.08]. The studied factorial models and the estimated parameters are depicted in .
Table 2 Fit Indices for the Confirmatory Analysis of the UWES-9
Figure 1 Illustration of the confirmatory factor analysis of the one-factor solution, UWES-9.

Figure 2 Illustration of the confirmatory factor analysis of the two correlated factors solution, UWES-9.
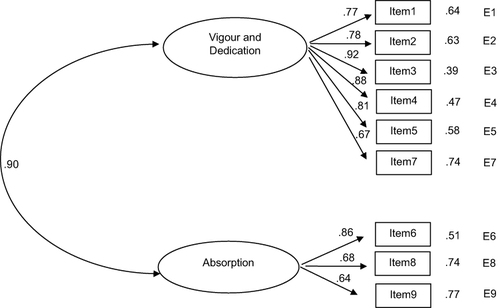
Figure 3 Illustration of the confirmatory factor analysis of the three correlated factors solution, UWES-9.
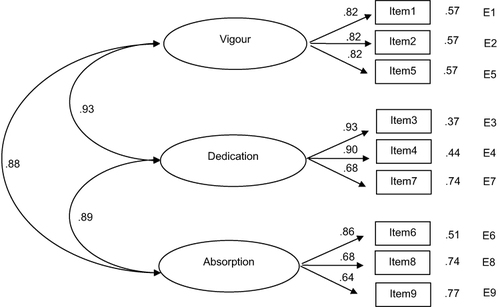
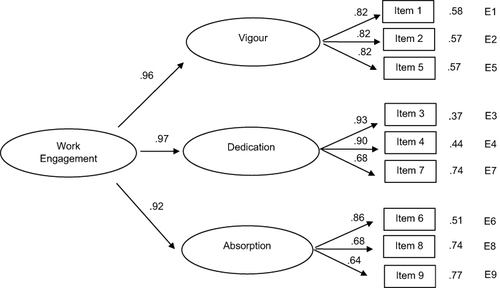
Figure 4 Illustration of the confirmatory factor analysis of the second order factor with three first order factors solution, UWES-9.
Reliability
In the analysis of the reliability of the scale scores, which were estimated with Cronbach’s alpha coefficient, a value of 0.93 was obtained for the total scale (α for men = 0.92; α for women = 0.93). The values obtained for the different dimensions were 0.79 for absorption, 0.87 for dedication and 0.85 for vigour. The item-test correlations () ranged between 0.58 (Item 9) and 0.85 (Item 3); in addition, Cronbach’s alpha values showed that the reliability of the scale would not increase significantly if some items were eliminated.
Table 3 Item-Test Correlations and Cronbach’s Alpha Coefficients
Factorial Invariance Across Gender
The CFI allowed the factorial invariance across gender in the three correlated factor solutions with and without the modification index to be accepted (). In both cases, the factorial structure of the UWES showed strict invariance by gender [RMSEA = 0.10 (0.09–0.10); CFI = 0.90] and [RMSEA = 0.06 (0.05–0.06); CFI = 0.97].
Table 4 Test of Factorial Invariance by Gender
Differential Item Functioning
Five of the 9 items on the UWES showed DIF when comparing men and women (). According to the SPD, scores from Items 1 and 6 were slightly higher in men in relation to the total score of the scale; scores from Items 7, 8, and 9 were higher in women. No indication of DIF was found when comparing genders in Items 2, 3, 4 and 5. Apart from suggesting the existence of DIF, we also found differences by gender in the mean scores of Items 1 (t = 5.171; p < 0.001), 6 (t = 4.662; p < 0.001), and 8 (t = 2.128; p < 0.05). However, although they showed DIF, there were no significant differences in the mean scores of Items 7 (t = 1.445; p = 0.074) and 9 (t = −0.304; p = 0.381).
Table 5 Differential Functioning of the Items Across Gender
Evidence of Construct Validity
In terms of validity in relation to other variables (), a greater sense of coherence (r = 0.42, p < 0.001) and higher dimension scores (meaningfulness r = 0.45, p < 0.001; comprehensibility r = 0.31, p < 0.001; and manageability r = 0.33, p < 0.001) were related to greater WE. Conversely, higher levels of psychological distress (on GHQ-12) were significantly related to lower WE (r = −0.38; p < 0.001). Finally, significant positive correlations were also obtained between WE and better self-perceived health (r = 0.26; p < 0.001).
Table 6 Correlations Between the UWES-9 and Related Constructs
Discussion
The main objective of the present study was to analyse the factorial structure of the UWES-9 scale for use with Spanish health professionals during the COVID-19 pandemic. In addition, we tried to extract data to support the invariance of the instrument according to the gender of the participants and provide evidence of convergent validity.
First, the analysis of the factorial structure of the instrument revealed that the model with the best fit indices among the five models studied was the model with three factors related to the correlation of pairs of errors 1–2 and 8–9, for which we observed CFI, GFI and NNFI values higher than 0.95, as recommended by Hu & Bentler.Citation35 Previous studies also suggest that the minimum number of dimensions presented by the UWES-9 scale with the capacity to explain the maximum amount of information collected by its items is equal to three.Citation10,Citation20,Citation21,Citation39
Although the initial model with three correlated factors showed an adequate CFI value (greater than 0.90), this was not achieved by the rest of the analysed parameters, which had higher results when pairs of errors were correlated following the indications of the modification indices. Other studies also applied this strategy with item pairs 1–2 and 8–9, such as the study by Lovakov et alCitation21 and the study by Schaufeli et al,Citation13 which is conceptually justified, according to Byrne.Citation40 Thus, Item 1 (“At my work, I feel bursting with energy”) would present a certain conceptual overlap with Item 2 (“At my job, I feel strong and vigorous”), and Item 8 (“I am immersed in my work”) would overlap with Item 9 (“I get carried away when I’m working”). Therefore, this work, in addition to providing evidence regarding the most appropriate factorial structure of the UWES-9, was interested in delving into other psychometric properties of the scale when the three-factor model is assumed.
Thus, the analyses that were performed indicated an adequate internal consistency of the UWES-9 instrument in terms of the three dimensions separately and the total scale, for both men and women. These results are similar to those of Sinval et alCitation10 in Portugal, or Schaufeli et alCitation13 in workers from five countries, including Spain. The items in each factor showed a high correlation among one another, indicating that the items in the dimensions of vigour, dedication and absorption measured the same construct.
Regarding the invariance according to the gender of the participants, the dimensions identified in the three-factor model did not show significant differences between men and women, indicating that the psychometric properties of this instrument are independent of the gender of the evaluated person. The invariance according to gender was also pointed out by Lovakov et alCitation21 in Russian workers and by Carmona-Halty et alCitation41 in Chilean university students, although there is a limitation in terms of studies that have explored this objective in health personnel with the model of three related factors. Greater consensus exists regarding the invariance of the scale according to other sample characteristics, such as its transcultural invariance.Citation10,Citation13,Citation42
DIF analyses should be an integral part of validity arguments.Citation43 In the present study, DIF was examined to explain the conditional differences in performance for two groups of participants (ie, man and woman) who were matched on the trait measured by the item.Citation44 After the functioning of the items of the UWES was analysed, five items showed different functioning in men and women. Some of these items also showed differences in mean scores according to gender. Following Arcos-Romero & Sierra,Citation45 the differences found in this study could be attributed to the following: (a) men and women truly differ regarding the variable; (b) items work differently across gender; and (c) there are real differences across gender, and the items do not work similarly for both. Thus, DIF analyses promote the validity and fairness in the interpretations of test scores that are planned as part of a larger validation effort.Citation43
Additionally, the results of this study showed evidence of convergent validity of the UWES-9 scale when applied to health personnel during the COVID-19 pandemic. Thus, the data indicated a statistically significant positive correlation between the UWES-9 and its factors concerning to the sense of coherence and perceived health. In contrast, a statistically significant negative relationship was observed between scores on this instrument and psychological distress. Before the COVID-19 pandemic, the literature already indicated that better self-perceived health status was related to greater WE among nursing personnelCitation46 and to present a greater sense of coherenceCitation47–49 and a better ability to face the challenges of life adaptively.Citation25 Mitonga-Monga and Hlongwane explained this relationship by arguing that workers with a high sense of coherence achieve their work objectives by perceiving the world as predictable, organized, and orderly.Citation50 A worse state of mental health, as occurs during psychological distress, is associated with a lower WE, as was observed in the study by García-Iglesias et alCitation51 with Spanish nurses and in papers such as Gorter and FreemanCitation52 and Holmberg et alCitation53 with health workers.
Between the possible limitations of the study, our data had a cross-sectional nature that could not happened with another design, such as longitudinal study. Another limitation lies in the sampling procedure which, although it is quite commonly used in research in this discipline and area of knowledge, does cannot guarantee that sample is representative of the health workers in this country, although the high sample number obtained might mitigate this effect.
A strong point of this study can be the inclusion of a significant number of workers from a sector that was vital in coping with a health crisis as complicated as was the first wave of the COVID-19 pandemic, which was marked by lockdown in Spain. With this regard, our study complements the existing literature analysing the psychometric properties of the UWES-9 instrument, providing results in favour of the use of this scale in the field of research to measure the WE of female and male Spanish health professionals based on three interrelated factors: vigour, dedication, and absorption by work.
Conclusion
The findings of this work support the use of the UWES-9 to assess the work engagement of health personnel during the COVID-19 pandemic and identify it as an adequate measure of this psychological variable and the constructs that comprise it.
Understanding the relationships between WE and sense of coherence, psychological distress, and perceived health among health care professionals may allow organizations to offer strategies to enhance those factors that improve the mental health of health care professionals in the performance of their duties. This, in turn, could improve the quality of life at work for these professions with the consequent improvement in quality of care and reduced accidents at work.
Implications
The UWE-9 questionnaire version validated in the population of health care professionals offers a new tool adapted to this group, which allows reporting on work engagement. In this sense, the data provided could be useful for health managers as they allow identifying areas of improvement which are specific to this population. This way, improvements in the work climate and, therefore, in the quality of health care could be achieved.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the Research Ethics Committee of Huelva, belonging to the Regional Ministry of Health of Andalusia, Spain (PI 036/20). Also, informed consent was obtained from all individual participants included in the study.
Disclosure
The authors report no conflicts of financial or non-financial interest in this work.
Additional information
Funding
References
- International Labour Organization. La COVID 19 y el mundo del trabajo [COVID-19 and the world of work]. Séptima edición. Estimaciones actualizadas y análisis; 2021. Séptima edición. Estimaciones actualizadas y análisis: https://cutt.ly/4ZseDDq. Accessed March 3, 2022.
- World Health Organization. Coronavirus disease (Covid-19) outbreak: rights, roles and responsibilities of health workers, including key considerations for occupational safety and health; 2020. Available from: https://cutt.ly/nmgTIsd. Accessed March 3, 2022.
- Pappa S, Ntella V, Giannakas T, et al. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:01–907. doi:10.1016/j.bbi.2020.05.026
- García-Iglesias JJ, Gómez-Salgado J, Martín-Pereira J, et al. Impact of SARS-CoV-2 (Covid-19) on the mental health of healthcare professionals: a systematic review. Rev Esp Salud Publica. 2020;94:e202007088.
- Hu J, He W, Zhou K. The mind, the heart, and the leader in times of crisis: how and when COVID-19-triggered mortality salience relates to state anxiety, job engagement, and prosocial behavior. J Appl Psychol. 2020;105(11):1218–1233. doi:10.1037/apl0000620
- Leiter MP, Bakker AB. Work engagement: introduction. In: Bakker B, Leiter P, editors. Work Engagement: A Handbook of Essential Theory and Research. London: Psychology Press; 2010.
- Schaufeli WB, Salanova M, González-Romá V, et al. The measurement of engagement and burnout: a two sample confirmatory factor analytic approach. J Happiness Stud. 2002;3(1):71–92. doi:10.1023/A:1015630930326
- Schaufeli M, Bakker A. Utrecht Work Engagement Scale. Preliminary Manual. Netherlands: Utrecht University; 2003.
- Schaufeli M, Bakker A. Defining and measuring work engagement: bringing clarity to the concept. In: Bakker B, Leiter P, editors. Work Engagement: A Handbook of Essential Theory and Research. London: Psychology Press; 2010.
- Sinval J, Marques-Pinto A, Queirós C, et al. Work engagement among rescue workers: psychometric properties of the Portuguese UWES. Front Psychol. 2018;8:2229. doi:10.3389/fpsyg.2017.02229
- Schaufeli WB, Bakker AB, Salanova M. The measurement of work engagement with a short questionnaire: a cross-national study. Educ Psychol Meas. 2006;66:701–716. doi:10.1177/0013164405282471
- Hallberg UE, Schaufeli WB. “Same” but different? Can work engagement be discriminated from job involvement and organizational commitment? Eur Psychol. 2006;11(2):119–127. doi:10.1027/1016-9040.11.2.119
- Schaufeli WB, Shimazu A, Hakanen J, et al. An ultra-short measure for work engagement: the UWES-3 validation across five countries. Eur J Psychol Assess. 2017;35(4):1–15.
- Shimazu A, Schaufeli WB, Kosugi S, et al. Work engagement in Japan: validation of the Japanese version of the Utrecht work engagement scale. Appl Psychol. 2008;57(3):510–523. doi:10.1111/j.1464-0597.2008.00333.x
- Klassen RM, Aldhafri S, Mansfield CF, et al. Teacher’ engagement at work: an international validation study. J Exp Educ. 2012;80(4):317–337. doi:10.1080/00220973.2012.678409
- Petrović IB, Vukelić M, Čizmić S. Work engagement in Serbia: psychometric properties of the Serbian version of the Utrecht work engagement scale (UWES). Front Psychol. 2017;8:1799. doi:10.3389/fpsyg.2017.01799
- Vallières F, McAuliffe E, Hyland P, et al. Measuring work engagement among community health workers in Sierra Leone: validating the Utrecht Work Engagement Scale. Eur J Work Org. 2017;33(1):41–46.
- Tomás JM, de Los Santos S, Georgieva S, et al. Utrecht work engagement scale in Dominican teachers: dimensionality, reliability, and validity. Eur J Work Organ Psychol. 2018;34(2):89–93.
- Willmer M, Jacobson JW, Lindberg M. Exploratory and confirmatory factor analysis of the 9-item Utrecht work engagement scale in a multi-occupational female sample: a cross-sectional study. Front Psychol. 2019;10:2771. doi:10.3389/fpsyg.2019.02771
- Kulikowski K. One, two or three dimensions of work engagement? Testing the factorial validity of the Utrecht work engagement scale (UWES) on a sample of Polish employees. Int J Occup Saf Ergon. 2019;25:241–249. doi:10.1080/10803548.2017.1371958
- Lovakov A, Agadullina ER, Schaufeli WB. Psychometric properties of the Russian version of the Utrecht Work Engagement Scale (UWES-9). Psychol Russ State Art. 2017;10(1):145–162. doi:10.11621/pir.2017.0111
- Gómez-Salgado J, Andrés-Villas M, Domínguez-Salas S, et al. Related health factors of psychological distress during the COVID-19 pandemic in Spain. Int J Environ Res Public Health. 2020;17(11):3947. doi:10.3390/ijerph17113947
- Domínguez-Salas S, Gómez-Salgado J, Andrés-Villas M, et al. Psycho-emotional approach to the psychological distress related to the COVID-19 pandemic in Spain: a cross-sectional observational study. Healthcare. 2020;8(3):190. doi:10.3390/healthcare8030190
- Valdez Bonilla H, Ron Murguía C. Escala Utrech de engagement en el trabajo [Utrech Scale of work engagement]. Jalisco: Occupational Health Psychology Unit Utrecht University; 2011.
- Antonovsky A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well. San Francisco: Jossey-bass; 1987.
- Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. 1993;36(6):725–733. doi:10.1016/0277-9536(93)90033-Z
- Virués-Ortega J, Martínez-Martín P, Del Barrio JL, et al. Validación transcultural de la Escala de Sentido de Coherencia de Antonovsky (OLQ-13) en ancianos mayores de 70 años [Cross-cultural validation of the Antonovsky Sense of Coherence Scale (OLQ-13) in the ederly over 70.]. Med Clin. 2007;128(13):486–492. doi:10.1157/13100935
- Goldberg DP, Gater R, Sartorius N, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. 1997;27(1):191–197. doi:10.1017/S0033291796004242
- Del Pilar Sánchez-López M, Dresch V. The 12-Item General Health Questionnaire (GHQ-12): reliability, external validity and factor structure in the Spanish population. Psicothema. 2008;20(4):839–843.
- Idler EL, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. 1997;38(1):21–37. doi:10.2307/2955359
- Ruiz-Frutos C, Ortega-Moreno M, Allande-Cussó R, et al. Health-related factors of psychological distress during the COVID-19 pandemic among non-health workers in Spain. Saf Sci. 2021;133:104996. doi:10.1016/j.ssci.2020.104996
- Tam CW, Pang EP, Lam LC, et al. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: stress and psychological impact among frontline healthcare workers. Psychol Med. 2004;34(7):1197–1204. doi:10.1017/S0033291704002247
- Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
- McDonald RP, Ho MHR. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64–82. doi:10.1037/1082-989X.7.1.64
- Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
- Putnick DL, Bornstein MH. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. 2016;41:71–90. doi:10.1016/j.dr.2016.06.004
- González A, Padilla JL, Hidalgo MD, et al. EASY-DIF: software for analyzing differential item functioning using the Mantel-Haenszel and standardization procedures. Appl Psychol Meas. 2011;35:483–484. doi:10.1177/0146621610381489
- Socha A, DeMars CE, Zilberberg A, et al. Differential item functioning detection with the Mantel-Haenszel procedure: the effects of matching types and other factors. Int J Test. 2015;15:193–215. doi:10.1080/15305058.2014.984066
- Hernandez-Vargas CI, Llorens-Gumbau S, Rodriguez-Sanchez AM, et al. Validación de la escala UWES-9 en profesionales de la salud en México [Validation of the UWES-9 scale in health professionals in Mexico]. Pensam psicol. 2016;14:89–100. doi:10.11144/Javerianacali.PPSI14-2.veup
- Byrne BM. Structural Equation Modelling with AMOS. 2nd ed. New York: Routledge; 2009.
- Carmona-Halty MA, Schaufeli WB, Salanova M. The Utrecht Work Engagement Scale for Students (UWES–9S): factorial validity, reliability, and measurement invariance in a Chilean sample of undergraduate university students. Front Psychol. 2019;10(1017):1–5. doi:10.3389/fpsyg.2019.01017
- Balducci C, Fraccaroli F, Schaufeli WB. Psychometric properties of the Italian version of the Utrecht Work Engagement Scale (UWES-9): a cross-cultural analysis. Eur J Psychol Assess. 2010;26(2):143–149. doi:10.1027/1015-5759/a000020
- Gómez-Benito J, Sireci S, Padilla JL, et al. Differential item functioning: beyond validity evidence based on internal structure. Psicothema. 2018;30(1):104–109. doi:10.7334/psicothema2017.183
- Muñiz J, Elosua P, Hambleton RK. International test commission guidelines for test translation and adaptation. Psicothema. 2013;25:151–157. doi:10.7334/psicothema2013.24
- Arcos-Romero AI, Sierra JC. Factorial invariance, differential item functioning, and norms of the Orgasm Rating Scale (ORS). Int J Clin Health Psychol. 2019;19:57–66. doi:10.1016/j.ijchp.2018.11.001
- Van Dorssen-Boog P, de Jong J, Veld M, et al. Self-leadership among healthcare workers: a mediator for the effects of job autonomy on work engagement and health. Front Psychol. 2020;11:1420. doi:10.3389/fpsyg.2020.01420
- Derbis R, Jasiński AM. Work satisfaction, psychological resiliency and sense of coherence as correlates of work engagement. Cogent Psychol. 2018;5(1):1–16. doi:10.1080/23311908.2018.1451610
- Garrosa E, Blanco-Donoso LM, Moreno-Jiménez B, et al. Evaluación y predicción del work engagement en voluntarios: el papel del sentido de la coherencia y la reevaluación cognitiva [Evaluation and prediction of work engagement in volunteers: the role of the sense of coherence and cognitive reappraisal]. An Psicol. 2014;30(2):530–540. doi:10.6018/analesps.30.2.148701
- Malagon-Aguilera MC, Suñer-Soler R, Bonmatí-Tomas A, et al. Relationship between sense of coherence, health and work engagement among nurses. J Nurs Manag. 2019;27:1620–1630. doi:10.1111/jonm.12848
- Mitonga-Monga J, Hlongwane V. Effects of employees’ sense of coherence on leadership style and work engagement. J Psychol Afr. 2017;27(4):351–355. doi:10.1080/14330237.2017.1347757
- García-Iglesias JJ, Gómez-Salgado J, Ortega-Moreno M, et al. Relationship between work engagement, psychosocial risks, and mental health among Spanish nurses: a cross-sectional study. Front Public Health. 2021;8:627472. doi:10.3389/fpubh.2020.627472
- Gorter RC, Freeman R. Burnout and engagement in relation with job demands and resources among dental staff in Northern Ireland. Community Dent Oral Epidemiol. 2011;39(1):87–95. doi:10.1111/j.1600-0528.2010.00568.x
- Holmberg J, Kemani MK, Holmström L, et al. Psychological flexibility and its relationship to distress and work engagement among intensive care medical staff. Front Psychol. 2020;11:603986. doi:10.3389/fpsyg.2020.603986