
Abstract
Purpose
To identify the distinct profiles of psychosocial adaptation of Chinese inflammatory bowel disease (IBD) patients and the predictive factors.
Patients and Methods
A cross-sectional survey method was used to recruit 263 IBD patients who were treated in a tertiary hospital in Shandong Province from July 2022 to April 2023. The general information questionnaire, Inflammatory Bowel Disease Psychosocial Adaptation Questionnaire, Resilience Scale for Inflammatory Bowel Disease, Chinese Benefit Finding Scale, and Stigma Scale for Chronic Illnesses, Medical Coping Modes Questionnaire and Inflammatory Bowel Disease-Disk were used as the instruments for investigation. Latent profile analysis was conducted with the six dimensions of the IBD Psychosocial Adaptation Questionnaire as the explicit indicators. The predictors of profile membership were analyzed by multinomial logistic regressions.
Results
Four profiles of psychosocial adaptation in IBD patients were identified: Low level psychosocial adaptation (14.1%), Medium level psychosocial adaptation – High body image distress (25.5%), Medium level psychosocial adaptation – Low body image distress (30.0%) and High level psychosocial adaptation (30.4%). Compared with Low level psychosocial adaptation group, High level psychosocial adaptation group had a higher level of positive cognition (OR=2.930, 95%IC 0.017–0.305, p< 0.001) and overall psychological resilience (OR=1.832, 95%IC 0.000–0.016, p < 0.001), more health behaviors (OR= 2.520, 95%IC 0.191–1.358, p=0.001), a lower level of internal stigma (OR=0.135, 95%IC 0.043–0.420, p < 0.001) and overall stigma (OR=0.010, 95%IC 0.003–0.118, p=0.001), less acceptance-resignation coping style (OR=0.055, 95%IC 0.209–3.200, p < 0.001) and lower disease burden (OR=0.407, 95%IC 0.298–0.698, p=0.006).
Conclusion
About a half of IBD patients had a medium level of psychosocial adaptation. Psychological resilience, benefit finding, stigma, medical coping styles and disease burden predicted psychosocial adaptation profiles. Healthcare providers need to focus on the heterogeneity of psychosocial adaptation of IBD patients and formulate personalized intervention programs for patients with different profiles to improve their psychosocial adaptation.
Introduction
Inflammatory bowel disease (IBD) is a chronic and life-threatening inflammatory disease of the gastrointestinal tissue.Citation1 There are two main subtypes of IBD, ie, ulcerative colitis (UC) and Crohn’s disease (CD). IBD causes intestinal (e.g, abdominal pain, diarrhea, and rectal bleeding) and extra-intestinal symptoms (eg, fatigue, anemia, and arthritis).Citation2 The global disease burden of IBD has been increasing over the past few decades.Citation3 The incidence is currently stable in Western countries.Citation4,Citation5 However, over the past decade, the incidence of IBD in the East has gradually increased, led by Asia and other recently developed and developing countries such as China, Korea and India.Citation3,Citation6 In China, the number of IBD cases increased by 911, 000 from 1990 to 2019. Due to the large population and the serious aging problem, the burden of IBD in China is expected to continue to grow in the next 25 years, and the number of IBD-related deaths will rise to about 7.57 million in 2044.Citation7 According to the latest statistics, the hospitalization rate of IBD patients in China showed an upward trend from 2013 to 2018.Citation8 In 2018, there were 166,000 hospitalized IBD patients in China, and the total hospitalization cost was US $426.37 million.Citation8 This greatly increases the financial and psychological stress of patients and imposes a huge financial and resource burden on the Chinese healthcare system.Citation5,Citation9 In addition, IBD is usually diagnosed in early adulthood and is currently incurable with characteristics of prolonged disease duration as well as alternating remission and recurrence, which negatively affects patients’ physical function, psychosocial health, and compromises their quality of life.Citation10–12
The impacts of IBD on psychosocial health involve disease-related and general stress, depressive and anxiety symptoms, impaired daily functioning, work disruption, and social withdrawal.Citation13 A systematic review showed that the pooled prevalence of anxiety symptoms and depressive symptoms in IBD patients was 1.95% and 2.22%, respectively.Citation14 In addition, IBD patients are prone to experience a combination of abnormal psychological symptoms such as obsessive-compulsive disorder, paranoia, and hostility.Citation15 These symptoms may lead to decreased psychosocial adaptation of IBD patients and affect their quality of life.Citation16 Psychosocial adaptation was described by Londono & McMillanCitation17 as a continuous process in which internal and external interactions reflect the changes individuals experience in adapting to their situation. Research suggests that psychosocial adaptation is crucial for patients’ active involvement in chronic disease managementCitation18 and exerts influence on their well-being in intrapersonal, interpersonal and extrapersonal domains.Citation19 Current studies about psychosocial adaptation were mainly conducted among cancer patients,Citation20,Citation21 adolescents,Citation16,Citation22 patients after surgeryCitation23,Citation24 and patients with chronic illnesses.Citation25 Nevertheless, there are relatively few studies on the psychosocial adaptation of IBD patients.Citation26
Based on the characteristics of IBD, WangCitation27 defined the psychosocial adaptation to IBD as the emotional experience, self-evaluation and attitude of IBD patients after diagnosis, as well as the process of adjusting individual behaviors to adapt to various social groups and norms. Different IBD patients may experience various patterns of psychosocial adaptation that suggests heterogeneity. Nevertheless, the majority of previous studies employed a variable-centered approach and measured the level of psychosocial adaptation as a composite score, which could not accurately reflect the differences between groups with various levels of psychosocial adaptation, and thus provide limited insights into related interventions. By contrast, latent profile analysis (LPA) is a person-centered approach that can classify individuals in a heterogeneous population into smaller and more homogeneous subgroups based on their values on continuous variables.Citation28 In addition, LPA can simplify the otherwise complex higher-order interactions among variables in the variable-centered analyses into a brief and simple representation.Citation29,Citation30 For this reason, LPA analysis results provide better referential value than variable-centered approach when developing tailored interventions for sub-populations to better match their needs.Citation31 Accordingly, this study selected LPA to identify patterns of psychosocial adaptation among IBD patients.
LivnehCitation19 proposed the psychosocial adaptation to chronic illness and disability framework which asserted that biophysiological status (eg, age, gender, and course of disease), psychological characteristics (eg, resilience, benefit finding, stigma, and coping strategies), and environmental features (eg, socioeconomic status) are the key factors in the process of psychosocial adaptation. Previous studies revealed the predictive effects of marriage, occupation, social support, stigma, medical coping styles and self-efficacy on psychosocial adjustment among Chinese nasopharynx cancer survivors, and head and neck cancer survivors after radiotherapy.Citation32,Citation33 In relation to IBD, a systematic review demonstrated that personality traits (eg, neuroticism and perfectionism), interpersonal traits (eg, attachment style), stress and coping strategies, emotional processing, and IBD-related cognition (eg, feeling stigmatized) were significantly associated with psychosocial adjustment among adults with IBD.Citation34 Personal resilience, family functioning and disease conditions were reported as the contributing factors of psychosocial adaptation in Chinese IBD patients.Citation26 These studies shed light on the associated factors of psychosocial adaptation in IBD patients, whereas the majority focused on a limited range of psychological factors. Furthermore, most studies used a variable-centered approach and thus probably cannot represent the influencing factors of psychosocial adaptation patterns in IBD patients.
Given limited research on a person-centered approach to explore psychosocial adaptation, this study aimed to identify the distinct profiles of psychosocial adaptation in Chinese IBD patients using LPA. Furthermore, based on the psychosocial adaptation to chronic illness and disability framework,Citation19 this study also aimed to analyze predictors of psychosocial adaptation latent profile membership in IBD patients by including biophysiological, psychological and environmental factors. Specifically, these factors consist of sociodemographic and disease-related information, resilience, benefit finding, stigma, medical coping styles and disease burden. The findings are expected to provide implications for healthcare providers to formulate targeted intervention programs for improving psychosocial adaptation of patients.
Materials and Methods
Design, Participants and Procedure
This study used a cross-sectional design with latent profile analysis. From July 2022 to April 2023, patients receiving treatment in the IBD specialist clinic of a tertiary hospital in Shandong Province were consecutively selected as the participants. The inclusion criteria were: (1) aged ≥18 years old, (2) diagnosed as IBD according to “Chinese Consensus on the diagnosis and treatment of inflammatory bowel disease”,Citation35 and (3) being conscious and able to complete the questionnaire independently or with the assistance of researchers. Exclusion criteria were: (1) duration of IBD < 3 months, (2) complicated with other serious diseases of heart, brain, kidney and other organs; and (3) was participating in other research.
By using G*Power 3.1.9 software and based on multiple regression analysis, the minimum sample size was calculated as 198, with effect size of 0.15, significance level of 0.05, power of 0.90 and 22 variables. With consideration of 20% non-response rate, the target sample size was 248. In addition, previous studies suggested a minimum sample size of 250 for LPA studies,Citation36 and a minimum profile in a large sample needs to include enough individuals (30–60) to support generalizations.Citation37 Finally, 263 patients were included in this study.
After obtaining permission from the IBD specialist clinic, two trained researchers recruited IBD patients who met the inclusion and exclusion criteria on the spot and used consistent instructions to explain the purpose and process of the study to the patients. With informed consent of the patients, the paper questionnaires were distributed and retrieved on the spot. In the meantime, with the consent and support of IBD specialized healthcare professionals, the researchers approached the potential participants online through sending a recruitment poster in the IBD patient Wechat group that was established and managed by IBD specialized healthcare professionals. The researchers distributed an electronic questionnaire via Wechat and followed the same steps with paper questionnaires to guide patients to fill out the questionnaire. When the questionnaires were returned, the researchers checked the completeness and eliminated invalid questionnaires that were featured with response time < 10 minutes and regular response patterns.
Measures
Socio-Demographic and Disease Related Questionnaire
The study collected demographic information, including sex, age, education level, marital status, permanent residence, lifestyle, occupational status, annual household income, and health care payment method. IBD-related information were also gathered, including disease type, course of disease, number of hospitalizations, history of surgery, current disease status, presence or absence of associated complications, current drug therapy, and presence or absence of comorbidity.
Inflammatory Bowel Disease Psychosocial Adaptation Questionnaire
The questionnaire developed by Chinese scholarsCitation38 includes 29 items in six dimensions to specifically assess psychosocial adaptation of IBD patients. The dimensions are anxiety/depression (10 items), sleep disorder (4 items), self-efficacy (5 items), body image (3 items), social support (3 items) and attitude (4 items). The response options were quantified using a 5-point Likert scale, ie, “never”, “ rarely”, “sometimes”, “often” and “always”. Higher total scores represent better overall psychosocial adaptation in IBD patients. To be noted, higher scores in anxiety/depression, sleep disorder and body image dimensions indicate lower levels of anxiety and depression, sleep disorder and body image distress, respectively. The Cronbach’s α of the questionnaire was 0.941 in the present study.
Resilience Scale for Inflammatory Bowel Disease
The scale compiled by LuoCitation39 was used to measure the psychological resilience level of IBD patients during the process of coping with the disease. The scale consists of 25 items in six dimensions of disease management, active coping with difficulties, positive cognition, emotional regulation, family support and peer support. The scale used 5-point Likert scoring method, with responses of “never” to “always” being assigned 1 to 5 points, respectively. The total score ranges from 25 to 125 points, and a higher score indicates a higher level of psychological resilience. The Cronbach’s α coefficient of the scale in this study was 0.935.
Chinese Benefit Finding Scale
The scale was adapted by Weaver et alCitation40 and was translated into Chinese version by Liu et alCitation41 to evaluate patients’ perceived positive benefits as a result of experiencing adversity during disease diagnosis and treatment. The scale includes six dimensions: acceptance (3 items), family relationship (2 items), world outlook (4 items), personal growth (7 items), social relationship (3 items) and health behavior (3 items). The total score ranges from 22 to 110, with a higher score signifying the stronger benefit finding. The Cronbach´s α coefficient of the scale in this study was 0.949.
Stigma Scale for Chronic Illnesses
The scale was developed by Rao et alCitation42 to measure the stigma of patients with chronic illnesses. It includes two parts: extrinsic stigma (11 items) and internal stigma (13 items). Each item was rated by 5-point Likert scale of “never”, “rarely”, “sometimes”, “often” and “always”. The total score ranges from 24 to 120 points, with a higher score suggesting a higher level of perceived stigma. The Cronbach’s α coefficient of the scale in this study was 0.950.
Medical Coping Modes Questionnaire
The questionnaire was compiled by Feifel,Citation43 and was adapted into Chinese versionCitation44 to assess the characteristics of coping styles that patients applied in the face of diseases. The questionnaire consists of three subscales: confrontation (8 items), avoidance (7 items) and acceptance-resignation (5 items). The higher score of the subscale indicates the more likelihood of the patients adopting a certain coping style. The Cronbach’α coefficients of the three subscales in the present study were 0.740, 0.404 and 0.875, respectively.
Inflammatory Bowel Disease-Disk
The scale was developed by Ghosh et alCitation45 and translated into Chinese by Liu.Citation46 It contains 10 items to assess the burden of IBD in ten domains, namely joint pain, abdominal pain, defecation-related problems, interpersonal communication, education and work, sleep, energy, mood, body image, and sexual function. Each item was assessed on a visual analogue scale from 0 to 10, with 0 indicating “strongly disagree”, 5 indicating “neither agree nor disagree”, and 10 indicating “strongly agree”. The total score of the scale is 0–100, with a score greater than 40 indicating a greater burden of disease and a lower quality of life. The Cronbach’s α coefficient of the scale in this study was 0.840.
Data Analyses
SPSS 26.0 and Mplus8.3 software was applied to analyze the data. For scales with several dimensions that contain different items, the mean score of items was calculated for analysis. Enumeration data were described by the number of cases and percentage. The chi-squared test or Fisher exact probability method was used for comparing classified disordered variables, and the Kruskal–Wallis H-test was used for comparing ordered variables. Continuous data were described as mean (M) ± standard deviation (SD). In the post hoc multiple comparisons of chi-squared test, the test level was corrected by chi-square segmentation, and p < 0.017 was considered statistically significant. By using Mplus 8.3 software, LPA was conducted to identify subgroups of psychological adaptation of IBD patients, with the item mean scores in the six dimensions of psychosocial adaptation as the explicit variables. The model fitting indices including Akaike information criterion (AIC), Bayesian information criterion (BIC), adjusted BIC (aBIC) and Entropy (0–1) were used to evaluate the accuracy of classification. In the LPA, the values of AIC, BIC and aBIC were smaller, and the entropy value is closer to 1, indicating a better fit of the model. Entropy >0.800 suggests that the accuracy of classification is 90%. The Lo-Mendell-Rubin (LMR) and the Bootstrap Likelihood Ratio test (BLRT) were applied to evaluate the fitting differences of the latent profile model. If all p-values reached the significant level (p < 0.05), it indicates that the model with k categories was significantly better than the model with k−1 categories.Citation36 Apart from the indices, the actual meaning of the profile was also considered when determining the number of profiles. Subsequently, Three-step (R3STEP) command in Mplus was performed to model the predictors of profile membership. This command enables a series of multinomial logistic regressions that assess whether an increase in an independent variable results in a higher probability of a person belonging to one profile over another.Citation47,Citation48
Ethical Considerations
The study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Medical College of Qingdao University (approval No.: QDU-HEC-2022195). All the participants signed informed consent.
Results
Tests for Common Method Bias and Multicollinearity
Given that the data were collected by self-report methods, Harman’s univariate test was performed prior to data analysis using exploratory factor analysis to detect common method bias. The results showed that five factors had eigenvalues greater than 1, explaining 68.05% of the variance. The first factor explained 37.89% of the variance, which was below the critical value of 40%.Citation49 Therefore, there was no significant common method bias in this study.
For predictive analysis, multicollinearity diagnosis among observed variables was performed. The results showed that the tolerance index of each model was less than 1, and the variance inflation factors (VIF) of independent variables (ie, psychological resilience, benefit finding, stigma, medical coping and IBD burden) were 1.283–5.464. According to the common rule of thumb that a VIF of 10 or above as a cutoff value for a large multicollinearity problem,Citation50 the results indicate that there is no significant multicollinearity problem among the independent variables involved in the five scales in the present study.
Participant Characteristics
In this study, a total of 270 questionnaires were distributed while seven invalid questionnaires were removed, and thus 263 valid questionnaires were retained, with an effective response rate of 97.41%. The age of 263 IBD patients was (43.71±14.60) years old. The majority of the patients were diagnosed as UC (74.9%) and 25.1% were CD. At investigation, 71.1% of the patients reported that they were in remission stage and 28.9% were in recurrence stage. The other information is shown in .
Table 1 General Information of Patients with Inflammatory Bowel Disease and Their Differences in Psychosocial Adaptation Latent Profile [N=263, Cases (Percentage, %)]
Item Mean Score, Standard Deviation and Correlation of Variables
The item mean scores, standard deviations, and correlations of the studied variables are shown in . Except medical coping style and its two dimensions (ie, confrontation and avoidance), other variables including psychological resilience and its dimensions, benefit finding and its dimensions, stigma, acceptance-resignation coping, and IBD burden were significantly correlated with overall psychosocial adaptation as well as its six dimensions (p< 0.01). Of these correlations, psychological resilience and benefit finding were positively correlated with psychosocial adaptation.
Table 2 Item Means, Standard Derivations, and Correlations of All Variables (N = 263)
Selection of Profile
The fitting indices for the different latent profile structures are shown in . As the number of profiles increased, lower Loglikelihood (LL), AIC, BIC, aBIC and significant BLRT were presented until the number reached 8. The 4-profile categories were selected because it provided lower LL, AIC, BIC, and aBIC, along with significant LMR and BLRT values, which indicated a significant improvement in the fit index compared to the k-1 categories (ie, the three-profile). Simultaneously, its Entropy value was >0.8, suggesting that the model containing 4 potential profiles can fully describe the category information of psychosocial adaptation in IBD patients with high reliability. Although five or more profiles have better fitting indices in terms of LL, AIC, BIC, aBIC, and entropy with significant BLRT values, their LMR values were insignificant. In addition, within five or more profiles, some profile sizes were less than 30 and accounted for below 5% of the total sample, which influenced their representation. Therefore, four-profile model of psychosocial adaptation was the best categorization.
Table 3 The Fitting Indices of Latent Profile Model of Psychosocial Adaptation in Patients with Inflammatory Bowel Disease
Profile Characteristics
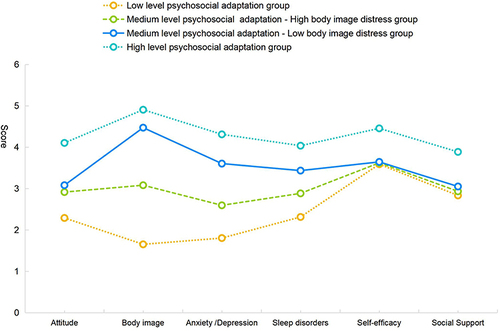
The profile characteristics of psychosocial adaptation in IBD patients are shown in . The four profiles were labeled based on their characterizing patterns of psychosocial adaptation. The “Low level psychosocial adaptation” profile accounted for the smallest proportion of the participants (14.1%) and exhibited the lowest level of psychosocial adaptation across the six dimensions. The “High level psychosocial adaptation” profile comprised 30.4% of the participants, which was featured by the highest scores in the six dimensions. The other two profiles were at medium level of psychosocial adaptation. Because the two profiles differed the most in the body image dimension, they were labeled as “Medium level psychosocial adaptation - High body image distress” group and “Medium level psychosocial adaptation-Low body image distress” group, respectively. The two profiles accounted for 25.5% and 30.0% of the participants, respectively.
Figure 1 Characteristics of four latent profiles of psychological adaptation in patients with inflammatory bowel disease.
Comparison of Different Profiles in Sociodemographic and Disease Data
As displayed in , whether suffering from complications and comorbidities showed significant difference among the four profiles of IBD patients.The results of post hoc multiple comparisons evinced a significant difference between “High level psychosocial adaptation” profile and “Medium level psychosocial adaptation-High body image distress” profile with respect to whether patients having complications or not (p=0.001). Simultaneously, “Medium level psychosocial adaptation – Low body image distress” profile and “Medium level psychosocial adaptation – High body image distress” profile were significantly different in the presence or absence of comorbidities (p=0.002).
Predictors of Latent Profile Membership
presents the R3STEP results of predictive factors of psychosocial adaptation profile membership. Using the “Low level psychosocial adaptation” profile as the reference group, the “Medium level psychosocial adaptation-High body image distress” profile had a higher level of overall psychological resilience and positive cognition, while “Medium level psychosocial adaptation – Low body image distress” profile had a higher level of overall psychological resilience, family support, and positive cognition, lower internal stigma, less avoidance coping mode and acceptance-resignation coping mode, and a lower degree of disease burden. In the meantime, the “High level psychosocial adaptation” profile had a higher level of overall psychological resilience and positive cognition, more health behaviors, a lower level of overall stigma and internal stigma, less acceptance-resignation coping mode and a lower degree of disease burden. Compared with the “Medium level psychosocial adaptation-High body image distress” profile, the “Medium level psychosocial adaptation – Low body image distress” profile had fewer comorbidities, a higher level of overall psychological resilience and family support, a lower degree of overall stigma and internal stigma, less acceptance-resignation coping mode and a lower degree of disease burden. The “High level psychosocial adaptation” profile had fewer IBD complications, a higher level of overall psychological resilience, and positive cognition, more health behaviors, a lower degree of overall stigma and internal stigma, less acceptance-resignation coping mode and a lower degree of disease burden. Compared with the “Medium level psychosocial adaptation – Low body image distress” profile, the “High level psychosocial adaptation” profile had a higher level of overall psychological resilience and disease self-management, more acceptance and health behaviors, a lower degree of overall stigma, and less acceptance-resignation coping style.
Table 4 Three-Step Results of Predictors of Latent Profiles
Discussion
The psychosocial adaptation of IBD patients was classified into four distinct latent profiles, revealing significant heterogeneity in the level of psychosocial adaptation of IBD patients. The study showed that 14.2% of the patients belong to the Low level psychosocial adaptation profile while the remaining were in the High level or Medium level profiles, indicating that most IBD patients had a moderate-high level of psychosocial adaptation. In particular, two profiles were characterized by body image. These results suggest that healthcare providers including nurses need to identify the heterogeneity of psychosocial adaptation among IBD patients and take a personalized approach to promoting their psychosocial adaptation in practice.
The Relationship Between Comorbidities, Complications, Body Image, Stigma and Psychosocial Adaptation in IBD
Comorbidities and complications were the significant variables in profile comparisons by using chi-squared tests. In particular, the results of R3STEP showed that IBD patients with complications were more likely to be classified into the Medium level psychosocial adaptation-High body image distress profile, which is consistent with the findings of Archer et al.Citation51 This suggests that most IBD patients with complications had a moderate level of psychosocial adaptation, while they were greatly troubled by body image. This may be related to the side effects of long-term medications, including immunosuppressants and hormones, leading to impaired body image in patients, such as weight gain, alopecia, and moon face.Citation52 Hypogonadism, gastrointestinal fistula, permanent stoma, short bowel syndrome, gastrointestinal and extra-intestinal dysplasia or cancer are also complications that cause body image disturbance in IBD patients.Citation53–55 In addition, studies have shown that comorbidities such as surgery and obesity can cause impaired body image of IBD patients, leading to patients’ poor psychosocial adaptation.Citation56,Citation57 Furthermore, the four profiles of psychosocial adaptation in IBD patients differed most prominently in the dimension of body image, suggesting that the levels of body image distress in IBD patients substantially affect their psychosocial adaptation.Citation58 Besides, the body image distress partially contributed to feelings of stigma in IBD patients, along with the embarrassing symptoms of IBD (eg, urgency of defecation and hyperactivity of bowel sounds) and perceived public awareness of the disease.Citation59 In the present study, patients in the “High level psychosocial adaptation” profile had a lower level of IBD disease stigma especially internal stigma, compared to the other three profiles. Research showed that more body image dissatisfaction increased higher levels of perceived stigmaCitation60 that can lead to poor psychosocial adjustment of patients.Citation61
Supported by previous research, the present study demonstrate that the psychosocial adaptation profile of IBD patients is closely related to comorbidities, complications, body image distress and stigma, which need to be recognized early for timely taking effective measures. To be specific, focus on addressing body image distress and stigma for IBD patients in the Low level psychosocial adaptation profile and Medium level psychosocial adaptation-High body image distress profile could be the intervention target for improving psychosocial adaptation in these patients. One study showed that more knowledge about the symptoms and complications of IBD was positively associated with reduced stigma.Citation62 In addition, emotional control, social support, and disease control are conducive to reducing stigma.Citation59 Therefore, healthcare providers can make efforts to enable IBD patients in the Low level psychosocial adaptation profile and Medium level psychosocial adaptation-High body image distress profile to obtain a well understanding of IBD to attenuate associated stigma. For instance, for patients with impaired body image due to long-term hormone intake, healthcare providers including nurses could timely deliver health education around management of medication side effects, such as supply of high-quality protein food and high potassium fruits and vegetables to reduce edema.Citation63 Additionally, prevention of complications for IBD patients is recommended through a multidisciplinary approach involving surgeons, dietitians, radiologists, pathologists and consultants in infectious diseases.Citation64 Studies have shown that early diagnosis and prompt treatment are the cornerstone for improving outcomes and maximizing mental health status for IBD patients.Citation10 Importantly, the risk stratification of IBD disease severity according to clinical symptoms, complications and comorbidities is beneficial to guiding the selection of first-line treatment,Citation10 and addressing the factors causing body image disturbance promptly, which could effectively reduce patients’ stigma and thus improve their psychosocial adaptation.
The Relationship Between Anxiety/Depression, Psychological Resilience and Psychosocial Adaptation in IBD
The latent profile analysis showed that anxiety/depression were predictors of the level of psychosocial adaptation in IBD patients, which aligns with the findings of Bannon et al.Citation65 Compared with the general population, there is an increased risk of anxiety and depression among IBD patients,Citation66 whereas high psychological resilient IBD patients had lower incidences of anxiety and depression.Citation67 Psychological resilience serves as a protective factor against the development of anxiety and depression.Citation68 In the present study, patients in the “High level psychosocial adaptation” profile had a higher level of overall psychological resilience and positive cognition compared to the other three profiles. In view of this, promoting psychological resilience could benefit IBD patients with low levels of psychosocial adaptation and anxiety/depression. Furthermore, family support and positive cognition of IBD were the predictors of Low level psychosocial adaptation profile and the Medium level psychosocial adaptation – high body image distress profile. Research reported that the implementation of family-centered intervention effectively improved the negative emotions of IBD patients and improved their psychological resilience.Citation69 Therefore, healthcare providers need to encourage family members to actively participate in the patient’s treatment decision-making, and equip family members to be competent caregivers for boosting IBD patients’ psychosocial adaptation. Furthermore, positive disease cognition and disease self-management ability were predictors of Medium level psychosocial adaption-Low body image distress profile. In the digital health times, Young et alCitation70 reported that the use of mobile e-health technology can effectively improve the self-management ability of patients with type 2 diabetes. This provides implications for healthcare professionals to offer remote health guidance for IBD patients through mobile electronic health information technology to improve their cognition of the disease and self-management ability, that help patients achieve a high level of psychosocial adaptation.
The Predictive Effects of Benefit Finding, Medical Coping Modes, Disease Burden on Psychosocial Adaptation Profiles
IBD patients in the Medium psychosocial adaptation-Low body image distress profile, Medium psychosocial adaptation-High body image distress profile and Low level psychosocial adaptation profile had less health behaviors, more avoidance as well as acceptance-resignation medical coping styles, and higher levels of disease burden than those in the High level psychosocial adaptation profile. Studies have shown that cognitive behavioral therapy (CBT) can improve avoidance behavior and benefit finding in patients with Parkinson’s disease.Citation71 CBT can effectively improve the coping ability and psychosocial adaptation of patients with gastrointestinal diseases.Citation72 Bennebroek et alCitation73 illustrated that IBD-specific CBT encompassing a cognitive intervention on illness beliefs, dysfunctional attitudes, and relapse-prevention plans, was effective in improving quality of life by reducing disease burden among IBD patients. Healthcare professionals could draw on these evidence to apply CBT to help IBD patients in the Low level psychosocial adaptation profile and Medium psychosocial adaptation-High body image distress profile to understand the nature of IBD from a positive perspective, to enhance disease-related health behaviors and correct medical coping styles, in order to strengthen their psychosocial adaptation. However, some research suggested that the positive psychological effects of CBT on IBD patients are short-term, and there is insufficient evidence to prove that CBT can continuously improve the psychosocial status of IBD patients.Citation74 Consequently, multiple digital interventions including web-based, computer-based, telephone, video conferencing, automated self-management systems, mobile applications, and text messaging can be adopted in the future to achieve long-term effects in improving psychosocial adaptation of IBD patients.Citation75
Limitations
There are several limitations to be recognized in the present study. Firstly, most of the patients in this study were young and middle-aged patients, and largely recruited from one tertiary hospital that may result in a Berkson bias. These limit the generalization of the study results. In future research, multi-center and larger sample investigation from community settings could be carried out to reduce the limitations of the single-center design and Berkson bias. In addition, no dose–response relationship was present across the different profiles in the horizontal direction of the two influencing factors of complication and comorbidity in this study due to their dichotomous attribute.Citation76 Future studies could refine the variables in terms of including complication and comorbidity in the criteria of disease severity to compare the differences between profiles to show a dose–response gradient and more specific results. Furthermore, the study was cross-sectional and thus could not measure the change of psychosocial adaptation over time. Given that IBD is a progressive and complex immune-mediated disorder, a longitudinal research design deserves to be employed to explore trajectory of psychosocial adaptation by following IBD patients over a period to uncover the dynamics of psychosocial adaptation profiles. Moreover, although certain bio physiological and psychological characteristics were measured as antecedents of psychosocial adaptation profiles in the study, some objective indicators such as validated biomarkers (eg, faecal calprotectin, C-reactive protein, oncostatin M)Citation77 need to be included in future research for analyzing their predictive effects on the psychosocial adaptation profile of IBD patients to supplement patient-reported outcomes.
Conclusion
From a person-centered perspective, latent profile analysis revealed four distinct profiles of psychosocial adaptation among IBD patients. Given the significant heterogeneity in the level of psychosocial adaptation in IBD patients, healthcare providers need to attend to the patterns of psychosocial adaptation of IBD patients, and formulate personalized intervention programs to improve their psychosocial adaptation. Simultaneously, it is worthy for healthcare providers to recognize the predictors influencing the profile membership including psychological resilience, benefit find, stigma, medical coping styles and disease burden when implementing tailored interventions.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors would like to sincerely thank the patients for their participation in this study. The authors also appreciate the support and assistance from chief physicians (Dr. Ding and Dr. Wu) and nurses in the Department of Gastroenterology of the Hospital during the process of approaching patients.
References
- Guan Q. A comprehensive review and update on the pathogenesis of inflammatory bowel disease. J Immunol Res. 2019;2019:7247238. doi:10.1155/2019/7247238
- Gelech J, Desjardins M, Mazurik K, Duerksen K, McGuigan-Scott K, Lichtenwald K. Understanding gut feelings: transformations in coping with inflammatory bowel disease among young adults. Qual Health Res. 2021;31(10):1918–1936. doi:10.1177/10497323211011442
- Agrawal M, Jess T. Implications of the changing epidemiology of inflammatory bowel disease in a changing world. United Eur Gastroenterol J. 2022;10(10):1113–1120. doi:10.1002/ueg2.12317
- Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769–2778. doi:10.1016/S0140-6736(17)32448-0
- Windsor JW, Kaplan GG. Evolving Epidemiology of IBD. Curr Gastroenterol Rep. 2019;21(8):40. doi:10.1007/s11894-019-0705-6
- Mak WY, Zhao M, Ng SC, Burisch J. The epidemiology of inflammatory bowel disease: east meets west. J Gastroenterol Hepatol. 2020;35(3):380–389. doi:10.1111/jgh.14872
- Shao B, Yang W, Cao Q. Landscape and predictions of inflammatory bowel disease in China: china will enter the Compounding Prevalence stage around 2030. Front Public Health. 2022;10:1032679. doi:10.3389/fpubh.2022.1032679
- He YM, Mao R, Yuan G, et al. The hospitalization burden of inflammatory bowel disease in China: a nationwide study from 2013 to 2018. Therap Adv Gastroenterol. 2022;15:17562848221102307. doi:10.1177/17562848221102307
- Ge L, Liu S, Li S, et al. Psychological stress in inflammatory bowel disease: psychoneuroimmunological insights into bidirectional gut-brain communications. Front Immunol. 2022;13:1016578. doi:10.3389/fimmu.2022.1016578
- Agrawal M, Spencer EA, Colombel JF, Ungaro RC. Approach to the management of recently diagnosed inflammatory bowel disease patients: a user’s guide for adult and pediatric gastroenterologists. Gastroenterol. 2021;161(1):47–65. doi:10.1053/j.gastro.2021.04.063
- Bisgaard TH, Allin KH, Keefer L, Ananthakrishnan AN, Jess T. Depression and anxiety in inflammatory bowel disease: epidemiology, mechanisms and treatment. Nat Rev Dis Primers. 2022;19(11):717–726.
- Byron C, Cornally N, Burton A, Savage E. Challenges of living with and managing inflammatory bowel disease: a meta-synthesis of patients’ experiences. J Clin Nurs. 2020;29(3–4):305–319. doi:10.1111/jocn.15080
- Halloran J, McDermott B, Ewais T, et al. Psychosocial burden of inflammatory bowel disease in adolescents and young adults. Intern Med J. 2021;51(12):2027–2033. doi:10.1111/imj.15034
- Barberio B, Zamani M, Black CJ, Savarino EV, Ford AC. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(5):359–370. doi:10.1016/S2468-1253(21)00014-5
- Bao S, Liu W, Liu L, Jiang G, Chen H. Analysis of factors related to spiritual psychology and quality of life in patients with inflammatory bowel disease based on artificial intelligence IBD nursing technology. J Healthc Eng. 2022;2022:7702432. doi:10.1155/2022/7702432
- Ma C, Ma Y, Wang Y, Lan X. Empathy and psychosocial adjustment in Tibetan and Han adolescents: a person-centered approach. Front Psychol. 2019;10:1896. doi:10.3389/fpsyg.2019.01896
- Londono Y, McMillan DE. Psychosocial adaptation: an evolutionary concept analysis exploring a common multidisciplinary language. J Adv Nurs. 2015;71(11):2504–2519. doi:10.1111/jan.12723
- Graffigna G, Bosio C, Pagnini F, et al. Promoting psycho-social wellbeing for engaging inflammatory bowel disease patients in their care: an Italian consensus statement. BMC Psychol. 2021;9(1):186. doi:10.1186/s40359-021-00692-6
- Livneh H. Psychosocial adaptation to chronic illness and disability: an updated and expanded conceptual framework. Rehabil Couns Bull. 2022;65(3):171–184. doi:10.1177/00343552211034819
- Chen YW, Lin TR, Kuo PL, et al. Psychosocial adjustment changes and related factors in postoperative oral cancer patients: a longitudinal study. Biomedicines. 2022;10(12):3231. doi:10.3390/biomedicines10123231
- Kang NE, Kim HY, Kim JY, Kim SR. Relationship between cancer stigma, social support, coping strategies and psychosocial adjustment among breast cancer survivors. J Clin Nurs. 2020;29(21–22):4368–4378. doi:10.1111/jocn.15475
- Sugimura K, Hihara S, Hatano K. Emotional separation, parental trust, and psychosocial adjustment in preadolescence and early adolescence. J Adolesc. 2020;84:165–170. doi:10.1016/j.adolescence.2020.09.001
- Xiao X, Su J, Su IJ. Psychosocial adjustment in young and middle-aged adults after coronary stent implantation: a mixed-method study. Heart Lung. 2022;52:86–94. doi:10.1016/j.hrtlng.2021.11.012
- Pedras S, Vilhena E, Carvalho R, Pereira MG. Psychosocial adjustment to a lower limb amputation ten months after surgery. Rehabil Psychol. 2018;63(3):418–430. doi:10.1037/rep0000189
- Reynolds N, Mrug S, Wolfe K, Schwebel D, Wallander J. Spiritual coping, psychosocial adjustment, and physical health in youth with chronic illness: a meta-analytic review. Health Psychol Rev. 2016;10(2):226–243. doi:10.1080/17437199.2016.1159142
- Xu Y, Liu T, Jiang Y, et al. Psychosocial adaptation among inflammatory bowel disease patients and associated factors: a cross-sectional study. Psychol Res Behav Manag. 2022;15:2157–2167. doi:10.2147/PRBM.S376254
- Wang YQA. Research progress of psychosocial adaptation in patients with inflammatory bowel disease. J Clin Med Prac. 2018;22(20):139–142.
- Berlin KS, Williams NA, Parra GR. An introduction to latent variable mixture modeling (part 1): overview and cross-sectional latent class and latent profile analyses. J Pediatr Psychol. 2014;39(2):174–187. doi:10.1093/jpepsy/jst084
- Lanza ST, Rhoades BL, Nix RL, Greenberg MT. Modeling the interplay of multilevel risk factors for future academic and behavior problems: a person-centered approach. Dev Psychopathol. 2010;22(2):313–335. doi:10.1017/S0954579410000088
- Leung CLK, Li KK, Wei VWI, et al. Profiling vaccine believers and skeptics in nurses: a latent profile analysis. Int J Nurs Stud. 2022;126:104142. doi:10.1016/j.ijnurstu.2021.104142
- Roeser RW, Eccles JS, Sameroff AJ. Academic and emotional functioning in early adolescence: longitudinal relations, patterns, and prediction by experience in middle school. Dev Psychopathol. 1998;10(2):321–352. doi:10.1017/S0954579498001631
- Yan MH, Fan Y, Chen M, Zhang J. The mediating role of self-efficacy in the association between perceived stigma and psychosocial adjustment: a cross-sectional study among nasopharyngeal cancer survivors. Psychooncology. 2022;31(5):806–815. doi:10.1002/pon.5865
- Wen L, Cui Y, Chen X, Han C, Bai X. Psychosocial adjustment and its influencing factors among head and neck cancer survivors after radiotherapy: a cross-sectional study. Eur J Oncol Nurs. 2023;63:102274. doi:10.1016/j.ejon.2023.102274
- Jordan C, Sin J, Fear NT, Chalder T. A systematic review of the psychological correlates of adjustment outcomes in adults with inflammatory bowel disease. Clin Psychol Rev. 2016;47:28–40. doi:10.1016/j.cpr.2016.06.001
- Wu KC, Liang J, Ran ZH, et al. Chinese consensus on diagnosis and treatment of inflammatory bowel disease(Beijing, 2018). Chin J Prac Int Med. 2018;38(09):796–813.
- Tein JY, Coxe S, Cham H. Statistical power to detect the correct number of classes in latent profile analysis. Struct Equation Model. 2013;20(4):640–657. doi:10.1080/10705511.2013.824781
- Sherman NW. Statistics in Kinesiology. Vincent, Brigham Young University, Weir, Des Moines University; 2015:100–102.
- Qi Y, Wang A. Development and psychometric evaluation of a psychosocial adaptation questionnaire for patients with inflammatory bowel disease. Chin Nurs Manag. 2020;20(01):44–48.
- Luo D. The development and psychometric assessment of the strength and resilience scale for inflammatory bowel disease [dissertation]. China: Nanjing Medical University; 2018.
- Weaver KE, Llabre MM, Lechner SC, Penedo F, Antoni MH. Comparing unidimensional and multidimensional models of benefit finding in breast and prostate cancer. Qual Life Res. 2008;17(5):771–781. doi:10.1007/s11136-008-9348-z
- Liu Z, Zhang L, Gudenkauf L. Cross-cultural adaptation of benefit finding scale for cancer patients. Chin J Nur. 2015;50(05):561–566.
- Rao D, Choi SW, Victorson D, et al. Measuring stigma across neurological conditions: the development of the stigma scale for chronic illness (SSCI). Qual Life Res. 2009;18(5):585–595. doi:10.1007/s11136-009-9475-1
- Feifel H, Strack S, Nagy VT. Degree of life-threat and differential use of coping modes. J Psychosom Res. 1987;31(1):91–99. doi:10.1016/0022-3999(87)90103-6
- Shen X, Jiang Q. Report on application of Chinese version of MCMQ in 701 patients. Chin J Behav Med Sci. 2000;2000(01):22–24.
- Ghosh S, Louis E, Beaugerie L, et al. Development of the IBD disk: a visual self-administered tool for assessing disability in inflammatory bowel diseases. Inflamm Bowel Dis. 2017;23(3):333–340. doi:10.1097/MIB.0000000000001033
- Liu J, Jiang Q, Liu A, Liu J, Ban C. Translation and test of validation and reliability of inflammatory bowel diseases disk scale. Chin J Nur. 2022;57(05):635–640.
- Asparouhov T, Muthen B. Auxiliary variables in mixture modeling: three-step approaches using mplus. Struct Equation Model. 2014;21(3):329–341. doi:10.1080/10705511.2014.915181
- Vermunt JK. Latent class modeling with covariates: two improved three-step approaches. Political Anal. 2017;18(4):450–469. doi:10.1093/pan/mpq025
- Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
- Kutner M, Nachtsheim C, Neter J. Applied Linear Regression Model; 2004.
- Archer S, Pinto A, Vuik S, et al. Surgery, complications, and quality of life: a longitudinal cohort study exploring the role of psychosocial factors. Ann Surg. 2019;270(1):95–101. doi:10.1097/SLA.0000000000002745
- Lamb CA, Kennedy NA, Raine T, et al. British society of gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106. doi:10.1136/gutjnl-2019-318484
- O’Toole A, Winter D, Friedman S. Review article: the psychosexual impact of inflammatory bowel disease in male patients. Aliment Pharmacol Ther. 2014;39(10):1085–1094. doi:10.1111/apt.12720
- Falconi M, Pederzoli P. The relevance of gastrointestinal fistulae in clinical practice: a review. Gut. 2001;49(Suppl 4):iv2–10. doi:10.1136/gut.49.suppl_4.iv2
- Le Berre C, Peyrin-Biroulet L, Sandborn WJ. selecting end points for disease-modification trials in inflammatory bowel disease: the SPIRIT consensus from the IOIBD. Gastroenterol. 2021;160(5):1452–1460.e1421. doi:10.1053/j.gastro.2020.10.065
- Bacha RA, Bouhnik Y, Serrero M, et al. Obesity in adult patients with inflammatory bowel disease: clinical features and impact on disability. A cross-sectional survey from the GETAID. Dig Liver Dis. 2023;55(12):1632–1639. doi:10.1016/j.dld.2023.05.008
- Spinelli A, Carvello M, D’Hoore A, Pagnini F. Psychological perspectives of inflammatory bowel disease patients undergoing surgery: rightful concerns and preconceptions. Curr Drug Targets Cardiovasc Haematol Disord. 2014;15(11):1074–1078.
- Demirdel S, Ö Ü. Body image disturbance, psychosocial adjustment and quality of life in adolescents with amputation. Disabil Health J. 2021;14(3):101068. doi:10.1016/j.dhjo.2021.101068
- Dibley L, Norton C, Whitehead E. The experience of stigma in inflammatory bowel disease: an interpretive (hermeneutic) phenomenological study. J Adv Nurs. 2018;74(4):838–851. doi:10.1111/jan.13492
- Wu YK, Berry DC. Impact of weight stigma on physiological and psychological health outcomes for overweight and obese adults: a systematic review. J Adv Nurs. 2018;74(5):1030–1042. doi:10.1111/jan.13511
- Xi Z, Rong CM, Ling LJ, et al. The influence of stigma and disability acceptance on psychosocial adaptation in patients with stoma: a multicenter cross-sectional study. Front Psychol. 2022;13:937374. doi:10.3389/fpsyg.2022.937374
- Rohde JA, Wang Y, Cutino CM, et al. Impact of disease disclosure on stigma: an experimental investigation of college students’ reactions to inflammatory bowel disease. J Health Commun. 2018;23(1):91–97. doi:10.1080/10810730.2017.1392653
- Cai X, Li X, Fan W, et al. Potassium and obesity/metabolic syndrome: a systematic review and meta-analysis of the epidemiological evidence. Nutrients. 2016;8(4):183. doi:10.3390/nu8040183
- Kaur M, Dalal RL, Shaffer S, Schwartz DA, Rubin DT. Inpatient Management of Inflammatory Bowel Disease-Related Complications. Clin Gastroenterol Hepatol. 2020;18(6):1346–1355. doi:10.1016/j.cgh.2019.12.040
- Bannon SM, Hopkins SW, Grunberg VA, Vranceanu AM. Psychosocial profiles of risk and resiliency in neurofibromatoses: a person-centered analysis of illness adaptation. J Neurooncol. 2022;156(3):519–527. doi:10.1007/s11060-021-03928-y
- Choi K, Chun J, Han K, et al. Risk of anxiety and depression in patients with inflammatory bowel disease: a nationwide, population-based study. J Clin Med. 2019;8(5). doi:10.3390/jcm8050654
- Philippou A, Sehgal P, Ungaro RC, et al. High levels of psychological resilience are associated with decreased anxiety in inflammatory bowel disease. Inflamm Bowel Dis. 2022;28(6):888–894. doi:10.1093/ibd/izab200
- Chen L, Wang Z, Liu D, et al. Anxiety, depression symptoms, and psychological resilience among hospitalized COVID-19 patients in isolation: a study from Wuhan, China. Brain Behav. 2023;13(12):e3274. doi:10.1002/brb3.3274
- Kang NN, Ma C, Wang Q, Wu YY. Effectiveness of family intervention on resilience, anxiety and depression in patients with inflammatory bowel disease. J Nurs Sci. 2018;33(13):70–72.
- Young HM, Miyamoto S, Dharmar M, Tang-Feldman Y. Nurse coaching and mobile health compared with usual care to improve diabetes self-efficacy for persons with Type 2 diabetes: randomized controlled trial. JMIR mHealth uHealth. 2020;8(3):e16665. doi:10.2196/16665
- Pachana NA, Egan SJ, Laidlaw K, et al. Clinical issues in the treatment of anxiety and depression in older adults with Parkinson’s disease. Mov Disord. 2013;28(14):1930–1934. doi:10.1002/mds.25689
- Bennebroek Evertsz F, Sprangers MAG, Sitnikova K, et al. Effectiveness of cognitive-behavioral therapy on quality of life, anxiety, and depressive symptoms among patients with inflammatory bowel disease: a multicenter randomized controlled trial. J Consult Clin Psychol. 2017;85(9):918–925. doi:10.1037/ccp0000227
- Keefer L, Palsson OS, Pandolfino JE. Best practice update: incorporating psychogastroenterology into management of digestive disorders. Gastroenterol. 2018;154(5):1249–1257. doi:10.1053/j.gastro.2018.01.045
- Chen J, Chen X, Sun Y, et al. The physiological and psychological effects of cognitive behavior therapy on patients with inflammatory bowel disease before COVID-19: a systematic review. BMC gastroenterol. 2021;21(1):469. doi:10.1186/s12876-021-02003-0
- Kiburi SK, Ngarachu E, Tomita A, Paruk S, Chiliza B. Digital interventions for opioid use disorder treatment: a systematic review of randomized controlled trials. J Subst Abuse Treat. 2023;144:108926. doi:10.1016/j.jsat.2022.108926
- Chalabi Hajkarim M, Karjalainen E, Osipovitch M, et al. Comprehensive and unbiased multiparameter high-throughput screening by compare finds effective and subtle drug responses in AML models. eLife. 2022;2022:11.
- Verstockt B, Noor NM, Marigorta UM, Pavlidis P, Deepak P, Ungaro RC. Results of the seventh scientific workshop of ECCO: precision medicine in IBD-disease outcome and response to therapy. J Crohns Colitis. 2021;15(9):1431–1442. doi:10.1093/ecco-jcc/jjab050