
Abstract
Background
Depressive symptoms are common among HIV-positive men who have sex with men (MSM). This study aims to explore (1) the relationship between family functioning and depressive symptoms and (2) the mediating roles of stigma and resilience in the relationship among HIV-positive MSM.
Methods
We used data from a cross-sectional study of a convenience sample in Hunan Province, China, conducted in 2019. The data analysis included 191 HIV-positive MSM with an average age of 26.98 years. All participants completed self-report questionnaires on demographic variables, family functioning, stigma, resilience, and depressive symptoms.
Results
Better family functioning was significantly associated with lower depressive symptoms. Both stigma (Indirect effect = −0.04, 95% CI, −0.10 ~ −0.001) and resilience (Indirect effect = −0.06, 95% CI, −0.12 ~ −0.01) were significant partial mediators in the relationship between family functioning and depressive symptoms. A parallel and chain mediating role of stigma and resilience in the relationship between family functioning and depressive symptoms was also supported (Indirect effect = −0.03, 95% CI, −0.08 ~ −0.01).
Conclusion
Improving family functioning is crucial for alleviating depressive symptoms among HIV-positive MSM in China. Depression assessment and reduction should be an integral part of prevention and treatment programs targeting stigma and resilience.
Introduction
Extensive evidence indicates a rising prevalence of HIV among men who have sex with men (MSM).Citation1 For example, although MSM accounts for 2% of the population in the United States, they represented a staggering 69.9% of new HIV diagnoses in 2017,Citation2 which are 87.9 times as likely as behaviorally heterosexual men to ever be diagnosed with HIV infection.Citation3 A recent review of 47 studies conducted in 17 countries in Latin America and the Caribbean revealed that MSM, especially young MSM, constitute high-risk groups for HIV infection, with a pooled prevalence ranging from 1.2% to 32.6%.Citation4 Liu et al summarized the positive rate of HIV antibodies to be 26% among older MSM in Western and Central Europe and North America. They also noted that the prevalence among this group has been continuously increasing over the past two decades, rising from 16% to 33%.Citation5 In China, a review of 355 surveys across 59 cities in 30 provinces and municipalities documented an overall prevalence of HIV among MSM of 5.7%, with rapid year-over-year increases.Citation6 This increasing number of HIV-positive MSM presents significant public health challenges, including, but not limited to, higher disease burden and risk of transmission, as well as greater incidence of mental illness. Depressive symptoms are one of the common mental disorders among HIV-positive MSM.Citation7 Previous studies suggested that compared with HIV-negative MSM, HIV-positive MSM have a higher risk of depressive symptoms (23.2% vs 33.1%).Citation8 Another study conducted with a Chinese sample has demonstrated that 36% of HIV-positive MSM suffer from depression, a significantly higher percentage compared to the general population.Citation9 Depressive symptoms not only impair the quality of life of HIV patients,Citation10 but also affect their adherence to antiretroviral therapy, increasing HIV-related morbidity and mortality.Citation11 Consequently, exploring influential factors of depressive symptoms can shed valuable insights into preventing mental disorders and improving the quality of life among HIV-positive MSM.
Family functioning reflects the extent to which a family operates as a unit to cope with stressorsCitation12 and may be a powerful protective factor against depression.Citation13 According to the Circumplex model of marital and family systems,Citation14 better family functioning means greater family cohesion and family resilience, which can effectively alleviate an individual’s post-traumatic psychological problems. A developing body of research supports the protective role of family functioning; for example, a cross-sectional study of 435 HIV-positive patients found that increased family functioning predicted a subsequent decrease in depression.Citation15 Influenced by traditional Chinese cultural values, prejudice from family members and rejection of family relationships might adversely affect MSM.Citation16 However, data remains limited regarding the relationship between family functioning and depression in the context of sexual minorities. It would be worthwhile, therefore, to examine the pathways that connect these two elements to understand their impacts among HIV-positive MSM. Finally, knowledge about various mediators could also provide useful information for targeted clinical interventions.
Stigma, herein conceptualized as “attributes that are deeply discrediting to an individual in society creating a deviant social persona”,Citation17 may be one of the risk factors in depression among HIV-positive MSM.Citation18,Citation19 Sexual minorities include lesbian, gay, bisexual, and transgender. HIV-positive MSM, as a part of sexual minorities, are strongly stigmatized within Chinese society. Based on the Minority Stress Model, sexual minorities experience excess stress because of their stigmatized social status compared with heterosexual individuals,Citation20 which in turn leads to depression. Several studies support the Minority Stress Model in understanding stigma and depression in Chinese sexual minorities. Gay and bisexual men who suffer from stigma were found to be at greater risk of developing depressive symptoms in four cities in northeastern China.Citation21 And in a longitudinal study of gay and bisexual men from Beijing, anticipated stigma predicted depression after 6 months.Citation22 Beyond China, empirical studies have likewise found stigma to be strongly associated with depression among people living with HIV (PLWH).Citation23,Citation24 Related to these findings, previous studies suggest that family support is negatively related to stigmaCitation25 and that strong family functioning and cohesion may have protective effects against feelings of stigma.Citation26 It is therefore plausible to hypothesize that poor family functioning increases the risk of stigma, which in turn increases the likelihood of depressive symptoms. There is, however, no study that has yet examined the mediating role of stigma in the poor family functioning to increased depressive symptoms link.
Resilience, as a modifiable characteristic and important mediator of depression, is further investigated in this article. It refers to a dynamic process wherein an individual presents a positive adaptation to stress, crisis, and adversity.Citation27 According to a typical construct of resilience,Citation28 resilience can be changed through supportive circumstancesCitation29 and person-environment interactions,Citation30 such as emotional bonds between family members.Citation31 Research has found that more resilient individuals tend to present with fewer depressive symptoms compared with less resilient ones.Citation32,Citation33 This echoes the findings of a meta-analysis showing that resilience is inversely related to depression.Citation34 Empirical studies with refugees have also found that family functioning could affect depressive symptoms through resilience.Citation35 To our knowledge, few studies have explored how resilience mediated the association of family functioning with depressive symptoms in the context of sexual minorities and HIV.
Furthermore, a developing body of research has highlighted how stigma might influence resilience.Citation36 As suggested by previous research,Citation37 resilience mediates stigma and self-esteem, which leads to depression among HIV-positive MSM. To date, the associations among family functioning, stigma, resilience, and depressive symptoms of HIV-positive MSM remain unexplored. Accordingly, the present study aimed to evaluate whether stigma and resilience served as underlying psychological mechanisms accounting for the relationship between family functioning and depressive symptoms. The first hypothesis was that higher levels of family functioning and resilience would be associated with a lower level of depressive symptoms, whereas greater stigma would be associated with elevated depressive symptoms. The second hypothesis was that stigma and resilience would mediate the association between family functioning and depressive symptoms. Identifying factors that mediate family functioning and depression should shed light on potential interventions and social policies to reduce mental health disparities among HIV-positive MSM.
Methods
Setting and Participants
The cross-sectional study was carried out between March and June of 2019. A sample of HIV-positive MSM was recruited in the patient waiting room at the institute for HIV/AIDS of the First Hospital of Changsha, China. Inclusion criteria for participants were (1) male, (2) over 16 years old, (3) diagnosed with HIV due to sexual contact with men, and (4) able to read and understand the questionnaire. Exclusion criteria were (1) illiteracy, (2) disability (3) current existing severe AIDS symptoms, and (4) had a prior diagnosis of a mental disorder. We distributed survey invitations to eligible patients in the outpatient clinic who met the inclusion criteria. Those who expressed willingness to participate were requested to complete a paper questionnaire with the face-to-face guidance of a researcher. All participants and their caregivers (if under 18 years old) provided written informed consent prior to the survey. Meanwhile, this survey was completed anonymously, and participants’ data was kept entirely confidential. Participants could stop participation at any time. In addition, all participants were given contact details for free mental health services and remuneration of 50 CNY. Finally, we approached 217 HIV-positive MSM, and 191 participants completed this survey voluntarily (response rate = 88.02%).
The investigation was carried out in accordance with the latest version of the Declaration of Helsinki and approved by the Ethics Committees of Xiangya School of Nursing of Central South University (No. 2018007).
Measure
Family Functioning
The family APGAR index was used to assess family functioning in this study.Citation38 It consists of 5 items, with five dimensions: adaptation, partnership, growth, affection, and resolve. Response options were based on a 3-point Likert scale, where 0 = never or rarely, 1 = sometimes, and 2 = most or all of the time. Higher scores indicated better family functioning. The family APGAR index has demonstrated acceptable reliability and validity in the Chinese population,Citation39 and the Cronbach’s alpha for the current sample was 0.88.
Stigma
The Social Impact Scale (SIS) was used to measure participants’ perceived stigma.Citation40 It consists of 24 items covering four dimensional constructs: social rejection, financial insecurity, internalized shame, and social isolation. The SIS uses a 4-point Likert scale, from 1 (strongly disagree) to 4 (strongly agree). Higher scores indicated greater perceived stigma. The Chinese version of SIS was tested to be reliable and valid.Citation41 In this study, its Cronbach’s alpha was 0.94.
Resilience
The 10-item Connor-Davidson Resilience Scale (CD-RISC-10) is a self-reported scale of resilience level, proposed by Campbell-Sills et alCitation42 and originating from the 25-item CD-RISC.Citation43 Each item was rated on a five-point Likert scale, from 0 (not true at all) to 4 (true nearly all the time). Higher scores indicated an increased level of psychological resilience. The Chinese version of CD-RISC-10 has satisfactory psychometric properties,Citation44,Citation45 and it showed a high Cronbach’s alpha in the current sample (alpha= 0.97).
Depressive Symptoms
The 9-item Patient Health Questionnaire (PHQ-9) was used to assess depressive symptoms over the past two weeks.Citation46 Responses to items range from 0 (not at all) to 3 (nearly every day); a higher total score indicated more frequent depressive symptoms. A cut-off score of 10 identified cases of clinical depression with acceptable sensitivity and specificity.Citation47 The PHQ-9 has been found to show good reliability and validity when used in the Chinese population,Citation48 and is widely employed in studies of HIV-positive MSM.Citation7 The Cronbach’s alpha was 0.93 in the current sample.
Demographic Variables
Demographic variables were collected by self-report, including age, duration of HIV infection, education level, ethnicity, residence location, marital status, single child status, caregiver’s education, and family monthly income.
Statistical Analysis
The mean (M) and standard deviation (SD) were estimated for continuous variables and the frequencies (N) and percentages (%) for categorical variables. A univariate analysis (eg, Mann–Whitney U-test and Chi-square test) was performed to examine the differences of demographic variables between depressed participants (PHQ-9 ≥ 10) and non-depressed participants (PHQ-9 < 10). Meanwhile, bivariate correlations were calculated among family functioning, stigma, resilience, depressive symptoms, and other relevant variables. We also tested for potential multicollinearity by variance inflation factor (VIF).Citation49 Finally, the mediating hypotheses were conducted with PROCESS macro, providing path coefficient estimates (b) and bootstrapped 95% confidence intervals (95% CI) for indirect effects based on 5000 bootstrapping resamples.Citation50 Before path analysis, Harman’s one factor test through exploratory factor analysis (EFA) was conducted to examine common method bias,Citation51 and all continuous variables were normalized. When the mediation effect (model 6) was tested, family functioning was entered as the predictor, stigma and resilience as the mediator, and depressive symptoms as the outcome. Statistically significant variables in the univariate analysis were screened and included in path analysis as covariates. All statistical analyses were performed using SPSS 23.0. A two-tailed p < 0.05 was employed to indicate statistical significance.
Results
Sample Characteristics
The total sample (N = 191) ranged in age from 16 to 50 years, with a mean age of 26.98 (SD=6.07) years old. Most participants were educated at or above the college level (76.4%) and were of Han ethnicity (95.3%). 57.6% (N =110) reported that their residency status is rural, 48.7% of participants (N = 93) were only child, while only 6.3% (N = 12) had married. The average time elapsed since their HIV diagnosis was 35.97 (SD = 30.30) months. Detailed sample demographic information can be found in .
Table 1 Descriptive Statistics of Participants (N = 191)
Group Differences by Depression
Of the 191 participants, approximately a quarter of the participants (N = 50, 26.2%) reported clinical depression. also illustrates the differences of sample characteristics between depressed participants and non-depressed participants. There were no significant differences observed between the two groups (all p > 0.05) for the majority of the variables (eg, age, education level, ethnicity, residence location, marital status, single-child status, and caregiver’s education). Conversely, significant differences were found regarding the duration of HIV infection (t = 2.55, p = 0.013). Participants in the depressed group remained HIV-positive for longer. Family income was also significantly different between the two groups (χ2 = 9.47, p = 0.024), with lower monthly family incomes reported among the depressed group.
Associations Among Main Study Variables
As shown in , family functioning was negatively associated with stigma (r = −0.17, p = 0.019) and depressive symptoms (r = −0.25, p = 0.001) and was positively associated with resilience (r = 0.18, p = 0.012). Stigma had a negative relationship with resilience (r = −0.53, p < 0.001) and a positive relationship with depressive symptoms (r = 0.53, p < 0.001). Resilience was negatively associated with depressive symptoms (r = −0.59, p < 0.001). Depressive symptoms had a positive association with duration of HIV infection (r = 0.18, p = 0.019). Lastly, family monthly income was negatively associated with depressive symptoms (r = −0.22, p = 0.003). In addition, the VIF of family functioning, stigma, and resilience were 1.04, 1.40, and 1.41, respectively, suggesting a low possibility of multicollinearity.
Table 2 Descriptive Statistics and Correlation Matrix of Main Measures (N= 191)
Path Analysis
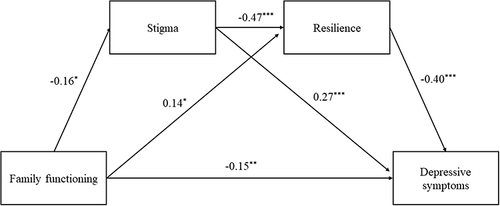
An EFA found 12 factors with eigenvalues > 1 and the first factor accounted for 19.60% of the total variance (< 40%), indicating that common method variance was not of great concern in the current study. Potentially confounding factors that were significantly associated with depressive symptoms were controlled in the model as covariates, including duration of HIV infection and family monthly income. depicts the standardized regression results of serial mediation to test the significance of the effects of family functioning on depressive symptoms through mediators of stigma and resilience. As shown in , family functioning had a significant negative association with stigma (b = −0.16, p = 0.032, 95% CI [−0.31, −0.01]), but a positive relationship with resilience (b = 0.14, p = 0.031, 95% CI [0.01, 0.27]). There was a positive association between stigma and depressive symptoms (b = 0.27, p < 0.001, 95% CI [0.14, 0.39]), and the negative relationships between resilience and depressive symptoms (b = −0.40, p < 0.001, 95% CI [−0.53, −0.27]) were both significant. A significant negative association between stigma and resilience was also observed (b = −0.47, p < 0.001, 95% CI [−0.60, −0.34]). Moreover, the direct effect of family functioning on depressive symptoms remained significant (b = −0.15, p = 0.008, 95% CI [−0.27, −0.04]). Therefore, stigma and resilience significantly mediated the relation between family functioning and depressive symptoms (Indirect effect = −0.03, 95% CI, −0.08 ~ −0.01). The model explained 7.48% variances in stigma, 29.88% variances in resilience, and 45.71% variances in depressive symptoms.
Table 3 Decomposition of the Effect of Family Functioning on Depression (N= 191)
Figure 1 Standardized path coefficients for the mediating model.
Sensitivity Analysis
We randomly selected 80% of the subjects from the full sample (N=150) to test the mediation effects, and obtain very similar results (see ). Both stigma (Indirect effect = −0.06, 95% CI, −0.13 ~ −0.01) and resilience (Indirect effect = −0.06, 95% CI, −0.14 ~ −0.001) were significant partial mediators in the relationship between family functioning and depressive symptoms. A parallel and chain mediating role of stigma and resilience in the relationship between family functioning and depressive symptoms was also supported (Indirect effect = −0.04, 95% CI, −0.11 ~ −0.01). The model explained 10.89% variances in stigma, 26.49% variances in resilience, and 45.78% variances in depressive symptoms.
Table 4 Sensitivity Analysis (N= 150)
Discussion
This study aimed to advance our understanding of how family functioning impacts depressive symptoms by testing the mediating roles of stigma and resilience in a sample of HIV-positive MSM. The findings demonstrated that stigma and resilience acted as a mediator between family functioning and depressive symptoms among HIV-positive MSM, respectively. Moreover, a chain mediation of stigma and resilience in the relationship between family functioning and depressive symptoms were also confirmed. By exploring the underlying mechanisms of how family functioning attenuated HIV-positive MSM’ depressive symptoms, our results provide clinical practitioners with important information for intervention efforts for HIV-positive MSM.
Consistent with the Circumplex model of marital and family systemsCitation14 and previous findings, the results demonstrated that family functioning was negatively associated with depressive symptoms.Citation52,Citation53 Compared with other social relationships, the Chinese emphasize the importance of family relationships. We therefore speculated that prejudice from family members may have a significant negative impact on the mental health of HIV-positive MSM. Chinese families have low acceptance of sexual minorities,Citation16 so low levels of family support are associated with increased depression, anxiety, and loneliness.Citation54 Conversely, family acceptance protected against depression in lesbian, gay, bisexual, and transgender (LGBT) sexual minorities.Citation55,Citation56 Meanwhile, stigma was positively associated with depressive symptoms and negatively associated with resilience. These findings were consistent with those from previous studies. HIV-positive MSM with higher resilience experienced less severe depressive symptoms.Citation37 Other studies of sexual minoritiesCitation57 and HIV patientsCitation58 also supported our findings on the intensified effects of stigma on depressive symptoms.
The current study extended previous literature to further clarify how family functioning lowers the subsequent depressive symptoms of HIV-positive MSM via stigma. As hypothesized, stigma constituted the mediating processes through which family functioning led to depressive symptoms. Some empirical studies have also supported this mediating role. The study by Lee et al showed that family functioning was negatively associated with stigma.Citation26 Individuals are less prone to perceive stigma within a well-functioning and cohesive family system. A cohesive family environment may give more opportunities for patients to openly share and discuss their fears and uncertainties, thus resulting in lower levels of felt stigma.Citation59 A study of patients with tuberculosis also supports the findings of the current study, documenting that stigma partially mediated the effect of family functioning on depressive symptoms.Citation60
Our study has identified the positive association between family functioning and resilience. Previous theories hold that resilience is driven by both internal and external protective factors. Among external protective factors, family environment and social support can provide material or spiritual support for the individual and are considered important factors influencing resilience.Citation61 In the current study, resilience mediates the relationship between family functioning and depressive symptoms among HIV-positive MSM. Specifically, good family functioning promoted resilience and consequently relieved depressive symptoms. Our observation is in line with the findings reported in previous literature documenting how higher resilience reduced the risk of depressive symptoms in various samples. For instance, a previous work among the elderly found that depressive symptoms were significantly negatively correlated with family functioning and resilience, while resilience is significantly positively correlated with family functioning.Citation62 A survey of refugees by Nam et al (2016) showed that family cohesion, a core component of family functioning, was significantly associated with depression, and the relationship was partially mediated by resilience.Citation35
It is worth noting that the chain effect of stigma and resilience mediates family functioning and depressive symptoms among HIV-positive MSM. Persistent and extremely distressing stigma can trigger strong negative emotions that impair an individual’s adaptive coping strategies. These maladaptive coping strategies may weaken their resilience. Another study of sexual minorities has similarly shown that stigma eroded resilience and consequently intensified depressive symptoms.Citation63 In addition, in line with previous studies,Citation64,Citation65 we discovered multiple psychosocial factors, such as duration of HIV infection and low family income, were associated with depressive symptoms in univariate analysis (p < 0.05). These factors should also be taken into great consideration for effective psychosocial intervention for HIV-positive MSM.
Several limitations of the present study should be acknowledged. First, although this study used highly reliable measurement variables, the self-report method may be affected by memory biases. Second, using a convenience sample from only one province may not constitute a sample representative of all Chinese HIV-positive MSM. Third, the cross-sectional design of this study restricts our ability to establish temporal relationships and make causal inferences among the variables. Thus, follow-up formative work and clinical interviews could deepen the analysis. Lastly, some important confounding factors, such as negative life events and sleep quality, were not taken into account in this study, which may also affect the study findings.
Conclusions
This study revealed that stigma and resilience have mediating effects on the association between family functioning and depressive symptoms among Chinese HIV-positive MSM. These findings have important implications for the early detection, prevention, and treatment of depression among HIV-positive MSM. Based on our research findings, HIV-positive MSM with family dysfunction can be identified as a high-risk group for depression. Undoubtedly, early intervention is crucial for this population. When implementing interventions, the effects of stigma and resilience on depressive symptoms should be comprehensively considered.
Data Sharing Statement
The data presented in this study are available on request from the corresponding authors (Dr. QD).
Ethics Statement
The survey was carried out in accordance with the latest version of the Declaration of Helsinki and approved by the Ethics Committees of Xiangya Nursing School of Central South University. The survey was under the principle of voluntary participation. The participants (or their guardians, if age < 18) carefully read, signed and returned the informed consent form to the researcher. The participants were assured that the information obtained would remain confidential.
Disclosure
The authors declare that they have no conflicts of interest in this work.
Additional information
Funding
References
- UNAIDS. 2020 Global AIDS report; 2020. Available from: https://www.unaids.org/sites/default/files/media_asset/2020_global-aids-report_en.pdf.
- Centers for Disease Control and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas, 2017. Centers for Disease Control and Prevention; 2018.
- Hess KL, Hu X, Lansky A, Mermin J, Hall HI. Lifetime risk of a diagnosis of HIV infection in the United States. Ann Epidemiol. 2017;27(4):238–243. doi:10.1016/j.annepidem.2017.02.003
- Coelho L, Torres T, Veloso V, et al. The prevalence of HIV Among Men Who Have Sex With Men (MSM) and Young MSM in Latin America and the Caribbean: a systematic review. AIDS Behav. 2021;25(10):3223–3237. doi:10.1007/s10461-021-03180-5
- Liu B, Yu M, Chen J, Li W. The HIV prevalence in older men who have sex with men in Western & Central Europe and North America-a meta-analysis. Int J STD AIDS. 2021;32(4):352–360. doi:10.1177/0956462420967576
- Dong MJ, Peng B, Liu ZF, et al. The prevalence of HIV among MSM in China: a large-scale systematic analysis. BMC Infect Dis. 2019;19(1):1000. doi:10.1186/s12879-019-4559-1
- Ahaneku H, Ross MW, Nyoni JE, et al. Depression and HIV risk among men who have sex with men in Tanzania. AIDS Care. 2016;28(Suppl 1):140–147. doi:10.1080/09540121.2016.1146207
- Armstrong NM, Surkan PJ, Treisman GJ, et al. Optimal metrics for identifying long term patterns of depression in older HIV-infected and HIV-uninfected men who have sex with men. Aging Mental Health. 2019;23(4):507–514. doi:10.1080/13607863.2017.1423037
- Tao J, Vermund SH, Lu H, et al. Impact of depression and anxiety on initiation of antiretroviral therapy among men who have sex with men with newly diagnosed HIV infections in China. AIDS Patient Care STDS. 2017;31(2):96–104. doi:10.1089/apc.2016.0214
- Araujo K, Silva S, Freire DA, et al. Correlation between quality of life, depression, satisfaction and functionality of older people with HIV. Rev Bras Enferm. 2021;74(Suppl 2):e20201334. doi:10.1590/0034-7167-2020-1334
- Gonzalez JS, Batchelder AW, Psaros C, Safren SA. Depression and HIV/AIDS treatment nonadherence: a review and meta-analysis. J Acquir Immune Defic Syndr. 2011;58(2):181–187. doi:10.1097/QAI.0b013e31822d490a
- Panganiban-Corales AT, Medina MJ. Family resources study: part 1: family resources, family function and caregiver strain in childhood cancer. Asia Pac Fam Med. 2011;10(1):14. doi:10.1186/1447-056X-10-14
- Keitner GI, Miller IW. Family functioning and major depression: an overview. Am J Psychiatry. 1990;147(9):1128–1137. doi:10.1176/ajp.147.9.1128
- Olson DH. Circumplex model of marital and family systems: assessing family functioning. In: Walsh F, editor. Normal Family Process. Guilford, New York: The Guilford Press; 1993.
- Wouters E, Masquillier C, le Roux BF. The importance of the family: a longitudinal study of the predictors of depression in HIV patients in South Africa. AIDS Behav. 2016;20(8):1591–1602. doi:10.1007/s10461-016-1294-0
- Wang Y, Hu Z, Peng K, et al. Discrimination against LGBT populations in China. Lancet Public Health. 2019;4(9):e440–e441. doi:10.1016/S2468-2667(19)30153-7
- Goffman E. Stigma and social identity. In: Deviance and Liberty. London: Routledge; 1963.
- Murphy PJ, Garrido-Hernansaiz H, Mulcahy F, Hevey D. HIV-related stigma and optimism as predictors of anxiety and depression among HIV-positive men who have sex with men in the United Kingdom and Ireland. AIDS Care. 2018;30(9):1173–1179. doi:10.1080/09540121.2018.1445827
- Tao J, Wang L, Kipp AM, et al. Relationship of stigma and depression among newly HIV-diagnosed Chinese men who have sex with men. AIDS Behav. 2017;21(1):292–299. doi:10.1007/s10461-016-1477-8
- Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. 2003;129(5):674–697. doi:10.1037/0033-2909.129.5.674
- Liu Y, Jiang C, Li S, et al. Association of recent gay-related stressful events with depressive symptoms in Chinese men who have sex with men. BMC Psychiatry. 2018;18(1):217. doi:10.1186/s12888-018-1787-7
- Choi KH, Steward WT, Miege P, Hudes E, Gregorich SE. Sexual stigma, coping styles, and psychological distress: a longitudinal study of men who have sex with men in Beijing, China. Arch Sex Behav. 2016;45(6):1483–1491. doi:10.1007/s10508-015-0640-z
- Crockett KB, Kalichman SC, Kalichman MO, Cruess DG, Katner HP. Experiences of HIV-related discrimination and consequences for internalised stigma, depression and alcohol use. Psychol Health. 2019;34(7):796–810. doi:10.1080/08870446.2019.1572143
- Lipira L, Williams EC, Nevin PE, et al. Religiosity, social support, and ethnic identity: exploring “Resilience Resources” for African-American Women Experiencing HIV-Related Stigma. J Acquir Immune Defic Syndr. 2019;81(2):175–183. doi:10.1097/QAI.0000000000002006
- Arshi M, Yavari M, Fekr AH, Safi MH, Moghanibashi-Mansourieh A, Moshayyedi M. Investigation of relationship between family social support and the level of stigma perceived by PLWHA in Iran. Soc Work Public Health. 2020;35(3):90–99. doi:10.1080/19371918.2020.1742840
- Lee SA, Kim SJ, Kim HJ, et al. Family cohesion is differently associated with felt stigma depending on enacted stigma in adults with epilepsy. Epilepsy Behav. 2020;112:107446. doi:10.1016/j.yebeh.2020.107446
- Masten AS, Best KM, Norman G. Resilience and development: contributions from the study of children who overcome adversity. Dev Psychopathol. 1990;2:425–444. doi:10.1017/S0954579400005812
- Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–562. doi:10.1111/1467-8624.00164
- Chan YC. Factors affecting family resiliency: implications for social service responses to families in Hong Kong. Indian Journal of Social Work. 2006;67(3):201–214.
- Lenette C, Brough M, Cox L. Everyday resilience: narratives of single refugee women with children. Qual Soc Work. 2013;12(5):637–653. doi:10.1177/1473325012449684
- Schweitzer R, Greenslade J, Kagee A. Coping and resilience in refugees from the Sudan: a narrative account. Aust N Z J Psychiatry. 2007;41(3):282–288. doi:10.1080/00048670601172780
- Loh J, Schutte NS, Thorsteinsson EB. Be happy: the role of resilience between characteristic affect and symptoms of depression. J Happiness Stud. 2014;15(5):1125–1138. doi:10.1007/s10902-013-9467-2
- Chung J, Lam K, Ho KY, et al. Relationships among resilience, self-esteem, and depressive symptoms in Chinese adolescents. J Health Psychol. 2020;25(13–14):2396–2405. doi:10.1177/1359105318800159
- Hu T, Zhang D, Wang J. A meta-analysis of the trait resilience and mental health. Pers Individ Dif. 2015;76:18–27. doi:10.1016/j.paid.2014.11.039
- Nam B, Kim JY, DeVylder JE, Song A. Family functioning, resilience, and depression among North Korean refugees. Psychiatry Res. 2016;245:451–457. doi:10.1016/j.psychres.2016.08.063
- Meyer IH. Resilience in the study of minority stress and health of sexual and gender minorities. Psychol Sexual Orient Gender Divers. 2015;2(3):209–213. doi:10.1037/sgd0000132
- Yan H, Li X, Li J, et al. Association between perceived HIV stigma, social support, resilience, self-esteem, and depressive symptoms among HIV-positive men who have sex with men (MSM) in Nanjing, China. AIDS Care. 2019;31(9):1069–1076. doi:10.1080/09540121.2019.1601677
- Smilkstein G, Ashworth C, Montano D. Validity and reliability of the family APGAR as a test of family function. J Fam Pract. 1982;15(2):303–311.
- Lv F, Zeng G, Liu SN, Zhong TL, Zhan ZQ. A study on validity and reliability of the family APGAR. Chin Public Health. 1999;15:987–988.
- Fife BL, Wright ER. The dimensionality of stigma: a comparison of its impact on the self of persons with HIV/AIDS and cancer. J Health Soc Behav. 2000;41(1):50–67. doi:10.2307/2676360
- Pan AW, Chung L, Fife BL, Hsiung PC. Evaluation of the psychometrics of the Social Impact Scale: a measure of stigmatization. Int J Rehabil Res. 2007;30(3):235–238. doi:10.1097/MRR.0b013e32829fb3db
- Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
- Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
- Cheng C, Dong D, He J, Zhong X, Yao S. Psychometric properties of the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) in Chinese undergraduates and depressive patients. J Affect Disord. 2020;261:211–220. doi:10.1016/j.jad.2019.10.018
- Wang L, Shi Z, Zhang Y, Zhang Z. Psychometric properties of the 10-item Connor-Davidson Resilience Scale in Chinese earthquake victims. Psychiatry Clin Neurosci. 2010;64(5):499–504. doi:10.1111/j.1440-1819.2010.02130.x
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient health questionnaire. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
- Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
- Brien RO. A caution regarding rules of thumb for variance inflation factors. Qual Quant. 2007;41(5):673–690. doi:10.1007/s11135-006-9018-6
- Hayes A. Introduction to mediation, moderation, and conditional process analysis. J Educ Meas. 2013;51:335–337. doi:10.1111/jedm.12050
- Johnson RE, Rosen CC, Djurdjevic E. Assessing the impact of common method variance on higher order multidimensional constructs. J Appl Psychol. 2011;96(4):744–761. doi:10.1037/a0021504
- Wang D, Zhao J, Ross B, et al. Longitudinal trajectories of depression and anxiety among adolescents during COVID-19 lockdown in China. J Affect Disord. 2022;299:628–635. doi:10.1016/j.jad.2021.12.086
- Wang J, He M, Zhao X. Depressive symptoms, family functioning and quality of life in Chinese patients with type 2 diabetes. Can J Diabetes. 2015;39(6):507–512. doi:10.1016/j.jcjd.2015.06.001
- Shao J, Chang ES, Chen C. The relative importance of parent-child dynamics and minority stress on the psychological adjustment of LGBs in China. J Couns Psychol. 2018;65(5):598–604. doi:10.1037/cou0000281
- Snapp SD, Watson RJ, Russell ST, Diaz RM, Ryan C. Social support networks for LGBT young adults: low cost strategies for positive adjustment. Fam Relat. 2015;64(3):420–430. doi:10.1111/fare.12124
- Ryan C, Russell ST, Huebner D, Diaz R, Sanchez J. Family Acceptance in Adolescence and the Health of LGBT Young Adults. J Child Adolesc Psychiatr Nurs. 2010;23(4):205–213. doi:10.1111/j.1744-6171.2010.00246.x
- Miedema SS, Haardorfer R, Keyes C, Yount KM. Does socio-structural context matter? A multilevel test of sexual minority stigma and depressive symptoms in four Asia-pacific countries. J Health Soc Behav. 2019;60(4):416–433. doi:10.1177/0022146519877003
- Damtie Y, Kefale B, Yalew M, et al. Depressive symptoms and associated factors among HIV positive patients attending public health facilities of Dessie town: a cross-sectional study. PLoS One. 2021;16(8):e0255824. doi:10.1371/journal.pone.0255824
- Mendes TP, Crespo CA, Austin JK. Family cohesion, stigma, and quality of life in dyads of children with epilepsy and their parents. J Pediatr Psychol. 2017;42(6):689–699. doi:10.1093/jpepsy/jsw105
- Qiu L, Yang Q, Tong Y, Lu Z, Gong Y, Yin X. The mediating effects of stigma on depressive symptoms in patients with tuberculosis: a structural equation modeling approach. Front Psychiatry. 2018;9:618. doi:10.3389/fpsyt.2018.00618
- Shao L, Zhong JD, Wu HP, Yan MH, Zhang JE. The mediating role of coping in the relationship between family function and resilience in adolescents and young adults who have a parent with lung cancer. Support Care Cancer. 2022;30(6):5259–5267. doi:10.1007/s00520-022-06930-w
- Lu C, Yuan L, Lin W, Zhou Y, Pan S. Depression and resilience mediates the effect of family function on quality of life of the elderly. Arch Gerontol Geriatr. 2017;71:34–42. doi:10.1016/j.archger.2017.02.011
- Wang Y, Lao CK, Wang Q, Zhou G. The impact of sexual minority stigma on depression: the roles of resilience and family support. Sex Res Soc Policy. 2022;19(6):442–452. doi:10.1007/s13178-021-00558-x
- Gianella S, Saloner R, Curtin G, et al. A cross-sectional study to evaluate the effects of age and duration of HIV infection on anxiety and depression in Cisgender Men. AIDS Behav. 2022;26(1):196–203. doi:10.1007/s10461-021-03373-y
- Zhou Q, Fan L, Yin Z. Association between family socioeconomic status and depressive symptoms among Chinese adolescents: evidence from a national household survey. Psychiatry Res. 2018;259:81–88. doi:10.1016/j.psychres.2017.09.072