
Abstract
Objective
This study aimed to investigate the association of physical activity and sleep metrics, measured via wrist-worn accelerometers, with depression in people with type 1 diabetes.
Patients and Methods
People with type 1 diabetes were recruited from the Dasman Diabetes Institute in Kuwait and were invited to wear a wrist-worn accelerometer device for 7 days. Mean physical activity (overall acceleration), inactivity, light activity, moderate activity, vigorous activity, the distribution of physical activity intensity (intensity gradient), sleep duration and sleep efficiency were quantified from the accelerometer data. The associations of these metrics with depression were investigated using multiple linear regression.
Results
A total of 551 people with type 1 diabetes (age 33.1 (9.5) years) were included. Overall physical activity (B = −0.09, CI = −0.14 to –0.04), moderate intensity activity (B = −0.02, CI = −0.02 to −0.01), vigorous intensity activity (B = −0.16, CI = −0.27 to −0.05), and the intensity gradient (B = −2.11, CI = −3.51 to −0.72) were negatively associated with depression score (p < 0.01) and these associations remain significant even after adjustment for age, sex, diabetes duration, and BMI. However, sleep duration and efficiency were not associated with depression. After mutual adjustment overall physical activity (B = −0.07, CI = −0.12 to −0.01), but not the intensity gradient (B = −0.90, CI = −2.47 to 0.68), remained associated with depression.
Conclusion
Overall, moderate and vigorous physical activity, and the intensity gradient were associated with lower symptoms of depression. Overall physical activity, rather than the distribution of activity intensity, appears more important in depression. This information can help guide physical activity interventions to improve depression in people with type 1 diabetes.
Introduction
Diabetes is one of the largest public health concerns, imposing a substantial burden on public health systems across the world. The prevalence of diabetes has been steadily increasing worldwide over the past few decades. Around 73 million adults in the Middle East and North Africa (MENA) region are living with diabetes, with approximately 25% of adults living with diabetes in Kuwait.Citation1 About 5–10% of people with diabetes have type 1 diabetes. People with diabetes are more likely to develop depression than people without diabetes.Citation2 The prevalence of depression is notably high and is associated with poorer glycemic control.Citation3,Citation4 The chronic nature of diabetes, the stress of managing the condition, and the impact on daily life can contribute to the development of depressive symptoms. At the same time, depression can interfere with diabetes management, leading to poor glycemic control, medication non-adherence, unhealthy lifestyle choices, and increased risk of complications.Citation2,Citation5 Poor diabetes management can lead to poor blood sugar control and a higher risk of severe hypoglycemia, diabetes ketoacidosis, nerve damage, kidney damage, eye problems, or heart problems, and reduced potency of immunity.Citation6,Citation7 In addition, depressive people experience negative thoughts about their future, and a high level of depression often leads to sleep deprivation, tiredness, anxiety, death, or suicide.Citation8
Substantial amount of research demonstrates a positive link between regular physical activity and mental health in the general population.Citation9,Citation10 As a result, physical activity positively impacts mental health and can help alleviate symptoms of depression and anxiety, which may indirectly contribute to better overall health outcomes.Citation8,Citation11 For example, many studies show that physical activity modifies the severity of disease in different patient states, leading to better health outcomes.Citation12,Citation13 Additionally, improved glucose variability has been observed in people with type 1 diabetes who spend a higher proportion of their day engaged in moderate to high-intensity physical activities.Citation14 Conversely, depression and anxiety have been shown to be associated with poorer glycemic control and long-term glycemic variability in people with type 1 diabetes.Citation15,Citation16 Long-term sedentary behavior is as a potential risk factor for depressive symptoms, as reported in healthy adults in the US.Citation17 Furthermore, both sedentary behavior and the severity of depression increase the risk of type 2 diabetes.Citation18,Citation19 On top of this, there are high levels of inactivity in people with type 1 diabetes, particularly those who have depressive symptoms.Citation20 Poor sleep may also contribute to poor blood glucose control, mental health, and diabetes morbidities.Citation21 There have, however, to our knowledge been no studies, which have directly assessed the link between physical activity/sleep and depression in people with type 1 diabetes.
While physical activity levels are generally low across the globe, this is a particular problem in Kuwait with only ~35% of the Kuwaiti population estimated as being sufficiently physically active, with men more physically active than women, with high levels of sedentary behaviors.Citation22 Similarly, only ~29% of people with type 2 diabetes were defined as being physically active.Citation3,Citation5 These reports are based on limited and self-reported data, and it is known that self-reported physical activity levels suffer from reporting bias and associations with health are inaccurate.Citation23 There is little accelerometer-measured physical activity or sleep data in people with type 1 diabetes, nor, as mentioned earlier, is there any data investigating the associations of these metrics with depression.
The aim of the current study was to investigate the association of objectively measured physical activity, sedentary behaviors, and sleep levels with depression in people with type 1 diabetes.
Materials and Methods
Setting and Participants
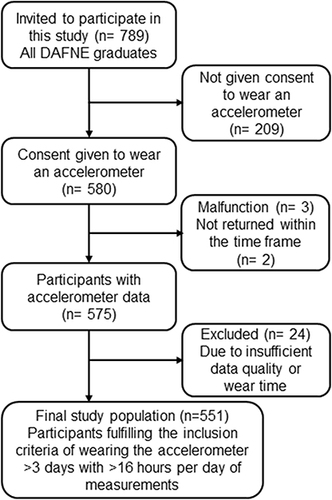
A cross-sectional study was conducted at the Dasman Diabetes Institute in Kuwait, from August 2021 to March 2023. People with type 1 diabetes who attended the DAFNE clinics were invited to participate in the study. All patients had a documented diagnosis of type 1 diabetes (per the American Diabetes Association (ADA) 2022 definition/criteria). All participants were enrolled in the Dose Adjustment for Normal Eating (DAFNE) program, a structured education program for type 1 diabetes. This study received approval from the Ethical Committee of the Ministry of Health, Kuwait (435/2016), and followed the guidelines outline in the Declaration of Helsinki. The study was fully explained to the participants, both orally and in writing, prior to them providing written informed consent. The exclusion criteria were diagnosed with severe mental disorders, schizophrenia, depressive psychosis, dementia, severe personality disorder or having any of the study data missing. The CONSORT flow diagram presents the number of participants included in this study ().
Figure 1 The CONSORT flow diagram shows the participant numbers.
Data Collection
For this study, demographic and clinical data were collected. Age was calculated from participants’ date of birth, clinical history recorded, and measurements of body mass, height, BMI and waist circumference made. The clinical data, such as HbA1c, total cholesterol, HDL cholesterol, LDL cholesterol and triglycerides were collected from the electronic health records during the same visit.
Assessment of Depression Symptoms
The Patient Health Questionnaire-9 (PHQ-9), is a 9-items depression scale, used to screen the presence and severity of depressive symptoms according to the Diagnostic and Statistical Manual of Mental Disorders-IV criteria (DSM-IV).Citation24 Each of the nine symptoms was scored as “0” (not at all), “1” (several days), “2” (more than half the days), or “3” (nearly every day) giving a range of scores between 0 and 27; the higher the score, the greater the severity. A PHQ-9 score 5–9 was defined as a mild level of depression, ≥10 was defined as a moderate-to-severe level of depression.Citation3
Accelerometry and Data Processing
Participants were issued with a GENEActiv original accelerometer and instructed to wear this 24 h per day for a 7-day period. The accelerometer was set to record at 100 Hz. To generate overall summary data for physical activity, sedentary behavior and sleep analysis was performed using GGIR.Citation25 Acceleration data collected was calibrated to local gravity using the methods established by van Hees et al.Citation26 Physical activity levels were quantified using methods previously describedCitation27,Citation28 with the intensity distribution calculated according to previously published methods as Rowlands et al.Citation29 Briefly, the natural log of both intensity and time accumulated at that intensity was plotted for each participant and the gradient of the line was used as the intensity gradient. Sleep was detected, without a sleep log using previously established methods with sleep efficiency defined as the time asleep within the sleep period window time.Citation30 A valid day was defined as having >16 hours of data in it, and we excluded participants with less than 3 valid days of data or if wear data were not present for every 15 minutes of the 24-hour cycle. From this analysis, we quantified the overall physical activity using the mean acceleration across the day the Euclidean Norm Minus One (ENMO variable) measured in mg. We also quantified the time spent sedentary (0–40 mg), time spent doing light (40–100 mg), moderate (100–400 mg), and vigorous physical activity (>400 mg), the intensity gradient and intercept, and sleep duration and efficiency. To investigate the time course of physical activity accelerometer data were processed to generate 24 h data for overall ENMO and in acceleration categories of: 0–40 mg, 40–100 mg, 100–200 mg, 300–400 mg and >400 mg. Such a broad range of physical activity parameters were selected to quantify different aspects of physical activity – overall amount, distribution of intensity and time spent at different intensities to give an accurate overall picture of physical activity.
Statistical Analysis
Normality was checked using the Shapiro–Wilk test. Physical activity and sleep variables were compared between the sexes using Mann–Whitney U-tests. To investigate the association of average (across the seasons) physical activity and sleep variables with depression we used multiple linear regression analysis with the following models: unadjusted (model 1); adjusted for age, duration of diabetes, BMI and sex (model 2) and adjusted for model 2 + intensity gradient (when acceleration was exposure) or acceleration (when intensity gradient was exposure) (model 3). This analysis was performed in all participants, rather than stratified by sex, to maintain statistical power in the analysis. Significance was accepted as P <0.05 and R and SPSS used for statistical analysis.
Results
The demographic and clinical characteristics of the participants are presented in . A total of 551 people with type 1 diabetes participated in this study, of them 289 (52.5%) were women. Participants’ ages ranged from 18 to 75 years, with an average of 31.1 ± 9.5 years. The average duration of diabetes was 17.3 ± 8.5 years, with the majority (75.4%) having diabetes duration of 10 years or more. The mean value for HbA1c was 8.2 ± 1.6%, and BMI was 27.2 ± 5.1 Kg/m2. The depression symptoms among the participants were 58.8% of them, mild-level depression was present in 37.0% and moderate-to-severe levels was 21.8%.
Table 1 Baseline Demographics Total and by Sex
The accelerometer metrics are presented in . The overall mean acceleration was 25.1 ± 8.1 mg, which included the time spent in light activity (236.2± 88.7 mint/day), moderate activity (66.7 ± 45.1 mint/day), and vigorous activity (1.6 ± 3.5 mint/day). Inactivity was 707.1 ± 154.5 mint/day and sleep duration was 349.6 ± 96.0 min/day. The Mann–Whitney U-tests used compared the acceleration between men and women. The result shows significantly higher acceleration in men (p = 0.01), but higher intensity gradients in women (p = 0.006). Women have a longer sleeping duration (p = 0.002) but no difference in sleep efficiency (p = 0.41). Time spent in inactivity was higher in men (p = 0.037), and time spent in moderate to vigorous physical activity (MVPA) was also greater in men (p < 0.001).
Table 2 Basic Physical Activity Characteristics Total and by Sex
The associations of the accelerometer metrics with depression are presented in .
Table 3 Association of Accelerometer Measured Physical Activity and Depression in People with Type 1 Diabetes
Overall physical activity (B = −0.09, CI = −0.14 to – 0.04), moderate intensity activity (B = −0.02, CI = −0.02 to −0.01), vigorous intensity activity (B = −0.16, CI = −0.27 to −0.05), MVPA (B = −0.02, p = 0.001), and the intensity gradient (B = −2.11, CI = −3.51 to −0.72) were negatively associated with depression score (p < 0.01) and these associations remain significant even after adjustment for age, sex, diabetes duration, and BMI. However, sleep duration and efficiency were not associated with depression. After mutual adjustment, overall physical activity (B = −0.07, CI = −0.12 to −0.01), but not the intensity gradient (B = −0.90, CI = −2.47 to 0.68), remained associated with depression.
Discussion
This is the first study that correlated the objectively measured physical activity intensity, and sleep by accelerometer with depression in people with type 1 diabetes. We quantified standard physical activity/sleep metrics such as average duration of inactivity, light activity, moderate activity, vigorous activity, sleep duration and efficiency, and also the novel metric of the intensity gradient, which provides information about the distribution of time at physical activity intensities. This provides us with a comprehensive evaluation of the volume and distribution of physical activity. The overall physical activity (average daily acceleration) was relatively low, and slightly higher in men compared to women. This higher overall activity in men was primarily driven by higher levels of moderate and vigorous physical activity. Sleep duration and efficiency were generally lower than current recommendations, with women reporting higher values than men. This study also examined the association between physical activity and depression, with higher physical activity associated with lower depressive symptoms.
As mentioned, the current study has demonstrated that physical activity and sleep are low in people with type 1 diabetes. There are very few studies that have quantified physical activity and sleep in adults with type 1 diabetes. One small study from the UK demonstrated that physical activity levels in people with type 1 diabetes are lower than in healthy adults of a similar age.Citation31,Citation32 However, making direct comparisons with this study is not feasible because they used differences in data processing methods. We can make some comparisons with data processed in a similar way where the overall daily acceleration in the current cohort was similar to the levels seen in people with type 2 diabetes (age 60 years) in the UK.Citation33 In the current study, we also compared physical activity and sleep in men and women. We found that light physical activity and sleep efficiency were similar between men and women. However, other metrics differed between men and women. There were apparent differences, with men spending more time inactive than women when we compared. Women were more on sleeping duration, whereas men were more on moderate to vigorous activity levels than women. Social and cultural norms in Arab countries are a possible reason for different physical activity patterns in men and women,Citation34 including, but not limited to the fact that women might have more constraints and obligations due to the roles and responsibilities in the family and society.Citation35 The roles shaped by societal and cultural expectations may limit the time and opportunities women have to engage in physical activity. For instance, women may prioritize family duties due to traditional gender roles,Citation35 or they might face societal and cultural barriers that discourage women from participating in activities outside the home.Citation34 Additionally, there may be a lack of awareness about the importance of physical activity in the management of diabetes, particularly among women.Citation36 Overall physical activity level was more in men than women.
The difference in physical activity and inactivity patterns in women and men may be related to higher depression symptoms in women than in men. This sex discrepancy in physical activityCitation36 and depression symptoms has been reported previously in studies in various populations.Citation37,Citation38 Depression and inactivity have a bidirectional relationship, where low physical activity can increase depression and/or depression can reduce activity levels.Citation39
Most of the studies have evaluated physical activity using validated questionnaires, comparing depression between active and non-active groups. However, none has investigated the association of objective assessments of physical activity/sleep with depression in individuals with type 1 diabetes. This study employs objective measures of physical activity and sleep metrics to investigate a pragmatic association of all metrics physical activity and sleep with depression. In our analysis, we found that overall physical activity and the distribution of physical activity intensity, the intensity gradient, were negatively associated with depression symptoms, independently of participants’ age, sex, BMI and diabetes duration. This is consistent with previous work where average daily acceleration was negatively associated with depression symptoms in U.S adults with diabetesCitation40 and in older European adults.Citation41 The result also agrees with a systematic review and meta-analysis of people without diabetes, which found a significant protective effect of physical activity on depression.Citation42 A study using the UK Biobank data recently showed that swapping sedentary behavior for physical activity is associated with lower depressive symptoms.Citation43 The association of depression symptoms with lower leisure-time physical activity has also been reported in both healthy elderly people and adult individuals with type 1 diabetes.Citation20,Citation44 Interestingly, after mutual adjustment only the overall physical activity, and not the intensity, gradient remained associated with depression, which indicates that the former may be both more affected by depression and be more effective in combatting depression. The current study is unable to determine the direction of causality, but as we mentioned earlier this relationship is generally bidirectional.
The role of physical activity in the improvement of depression in diabetes patients involves various physiological mechanisms. Physical activity influences the secretion and regulation of various hormones in the body, such as cortisol, adrenaline, and growth factors.Citation45 These hormonal changes can have a positive impact on mood, stress response, and overall well-being.Citation46 A study of patients with type 1 diabetes found that low physical activity was associated with higher midnight salivary cortisol and was independently linked to self-reported depression.Citation47 Exercise has been shown to increase the release of these neurotransmitters, leading to enhanced mood and reduced depressive symptoms. Over time, exercise can help regulate and reduce the excessive activation of the hypothalamic-pituitary-adrenal (HPA) axis, leading to decreased stress levels and improved mood.Citation2 A recent study reported that exercise enhances kynurenine metabolism in muscles and consequently prevents stress-induced depression.Citation48 To improve the long-term health of individuals with type 1 diabetes, efforts to increase both mental well-being and physical activity should continue to be recommended.
Beyond the direct findings of this study, it is essential to consider the broader implications these results have for public health and clinical practice, particularly in the management of Type 1 Diabetes. The findings of this study have significant implications for public health, especially concerning the management of Type 1 diabetes. Understanding the relationship between physical activity, sleep patterns, and depression can inform more holistic treatment approaches.
Overall, this information provides us with a comprehensive overview of physical activity and sleep in people with type 1 diabetes. Our analysis of the association of physical activity and sleep metrics highlights the importance of overall, more so than the distribution, physical activity in depression. No previous work has investigated the associations of the novel intensity gradient metric with depression, so the current study provides novel information on this metric in relation to depression. This data can help direct and target interventions to improve physical activity and sleep in people with type 1 diabetes. These insights could lead to the development of targeted physical activity, potentially reducing the burden of depression in individuals with Type 1 diabetes. Additionally, the study’s outcomes may encourage healthcare providers to routinely assess physical activity and sleep patterns as part of the diabetes management plan. On a broader scale, this research can contribute to policy-making, emphasizing the importance of integrating mental health care with chronic disease management. However, this analysis cannot confirm causality or its direction, in our observations and further clinical trials are needed in this area.
This single-center study is not without limitations, and it is prudent to consider these. The study is a cross-sectional analysis, where physical activity, sleep and depression levels were measured at the same time; however, we cannot confirm causality in this relationship. On top of this, we did not conduct an a priori sample size calculation and so the study may be underpowered. The analysis was conducted under free-living conditions, reflecting the pragmatic association between physical activity and depression levels, and so there may be other potential confounding variables not considered. All participants were enrolled in the DAFNE program and adhered to its educational guidelines, potentially influencing their lifestyle, and limiting the generalizability of the findings to populations not exposed to similar programs. A key strength of our study is that we objectively measured physical activity and sleep in a large sample of people with type 1 diabetes.
Author Contributions
All authors contributed significantly to the conception, study design, execution, data acquisition, analysis and interpretation, and drafting or critical review of the article. All authors approved the final version for publication, selected the journal for submission, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We would like to acknowledge the nursing staff at Dasman Diabetes Institute and the study participants.
Data Sharing Statement
Data will be available from a reasonable request from the corresponding author.
Additional information
Funding
References
- IDF diabetes atlas. International Diabetes Federation (IDF) 2021. Available from: https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf. Accessed July 10, 2024.
- Moulton CD, Pickup JC, Ismail K. The link between depression and diabetes: the search for shared mechanisms. Lancet Diabetes Endocrinol. 2015;3(6):461–471. doi:10.1016/S2213-8587(15)00134-5
- Al-Ozairi E, Al Ozairi A, Blythe C, Taghadom E, Ismail K. The epidemiology of depression and diabetes distress in type 2 diabetes in Kuwait. J Diabete Res. 2020;2020:7414050. doi:10.1155/2020/7414050
- AlOzairi A, Irshad M, AlKandari J, AlSaraf H, Al-Ozairi E. Prevalence and predictors of diabetes distress and depression in people with type 1 diabetes. Front Psychiatr. 2024;15:1367876. doi:10.3389/fpsyt.2024.1367876
- Al-Ozairi A, Taghadom E, Irshad M, Al-Ozairi E. Association between depression, diabetes self-care activity and glycemic control in an Arab population with type 2 diabetes. Diabetes Metabol Synd Obes. 2023;16:321–329. doi:10.2147/dmso.s377166
- DiMeglio LA, Evans-Molina C, Oram RA. Type 1 diabetes. Lancet. 2018;391(10138):2449–2462. doi:10.1016/s0140-6736(18)31320-5
- Al-Ozairi E, Irshad M, Taghadom E, Varghese A, Sojan L, Alkandari J. Effect of COVID-19 vaccine on blood glucose metrics in Arabic people with type 1 diabetes. Front Endocrinol. 2023;14:1120384. doi:10.3389/fendo.2023.1120384
- Kim D-J. Effects of physical activity on depression in adults with diabetes. Osong Pub Health Res Perspect. 2018;9(4):143–149. doi:10.24171/j.phrp.2018.9.4.02
- Liu F, Duan H, Hou Y, Zhang B, Wu J, Guo L. The relationship between physical exercise and aggressive behavior among college students: the mediating roles of life satisfaction, meaning in life, and depression. Psychol Res Behav Manage. 2024;17:305–315. doi:10.2147/prbm.s450326
- Li S, Wang Y. The relationship between risk perception, physical activity, and adolescent mental health: a cross-lagged analysis. Psychol Res Behav Manage. 2023;16:3347–3357. doi:10.2147/prbm.s422982
- Sutin AR, Luchetti M, Stephan Y, Terracciano A. Meaning in life and accelerometer-measured physical activity: association based on 67,038 UK Biobank participants. Mental Health Phys Act. 2021;21:100412. doi:10.1016/j.mhpa.2021.100412
- Sutkowska E, Stanek A, Madziarska K, et al. Physical activity modifies the severity of COVID-19 in hospitalized patients—Observational study. J Clin Med. 2023;12(12):4046. doi:10.3390/jcm12124046
- Braun JM, Papandonatos GD, Li N, et al. Physical activity modifies the relation between gestational perfluorooctanoic acid exposure and adolescent cardiometabolic risk. Environ. Res. 2022;214(Pt 3):114021. doi:10.1016/j.envres.2022.114021
- Al Kandari J, Al Ozairi E, Irshad M, Varghese A, Gray SR. Association of physical activity metrics with glucose variability in people with type 1 diabetes: a cross-sectional study. Euro J Sport Sci. 2024;24(2):210–216. doi:10.1002/ejsc.12062
- Egbuonu I, Trief PM, Roe C, Weinstock RS. Glycemic outcomes related to depression in adults with type 1 diabetes. J Health Psychol. 2021;26(8):1282–1290. doi:10.1177/1359105319877298
- Déniz-García A, Díaz-Artiles A, Saavedra P, Alvarado-Martel D, Wägner AM, Boronat M. Impact of anxiety, depression and disease-related distress on long-term glycaemic variability among subjects with Type 1 diabetes mellitus. BMC Endocr Disord. 2022;22(1):122. doi:10.1186/s12902-022-01013-7
- Guo Y, Li K, Zhao Y, Wang C, Mo H, Li Y. Association between long-term sedentary behavior and depressive symptoms in U.S. adults. Sci Rep. 2024;14(1):5247. doi:10.1038/s41598-024-55898-6
- Åsvold BO, Midthjell K, Krokstad S, Rangul V, Bauman A. Prolonged sitting may increase diabetes risk in physically inactive individuals: an 11 year follow-up of the HUNT Study, Norway. Diabetologia. 2017;60(5):830–835. doi:10.1007/s00125-016-4193-z
- Rubin RR, Ma Y, Marrero DG, et al. Elevated depression symptoms, antidepressant medicine use, and risk of developing diabetes during the diabetes prevention program. Diabetes Care. 2008;31(3):420–426. doi:10.2337/dc07-1827
- Ahola AJ, Tikkanen-Dolenc H, Forsblom C, Harjutsalo V, Groop P-H; on behalf of the FinnDiane Study G. Symptoms of depression are associated with reduced leisure-time physical activity in adult individuals with type 1 diabetes. Acta Diabetologica. 2021;58(10):1373–1380. doi:10.1007/s00592-021-01718-6
- Perfect MM. Sleep-related disorders in patients with type 1 diabetes mellitus: current insights. Nat Sci Sleep. 2020;12:101–123. doi:10.2147/nss.s152555
- Chaabane S, Chaabna K, Abraham A, Mamtani R, Cheema S. Physical activity and sedentary behaviour in the Middle East and North Africa: an overview of systematic reviews and meta-analysis. Sci Rep. 2020;10(1):9363. doi:10.1038/s41598-020-66163-x
- Celis-Morales CA, Perez-Bravo F, Ibañez L, Salas C, Bailey ME, Gill JM. Objective vs. self-reported physical activity and sedentary time: effects of measurement method on relationships with risk biomarkers. PLoS One. 2012;7(5):e36345. doi:10.1371/journal.pone.0036345
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient health questionnaire. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
- Migueles JH, Rowlands AV, Huber F, Sabia S, van Hees VT. GGIR: a research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J Measure Phys Behav. 2019;2(3):188–196. doi:10.1123/jmpb.2018-0063
- van Hees VT, Fang Z, Langford J, et al. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: an evaluation on four continents. J Appl Physiol. 2014;117(7):738–744. doi:10.1152/japplphysiol.00421.2014
- Sabia S, van Hees VT, Shipley MJ, et al. Association between questionnaire- and accelerometer-assessed physical activity: the role of sociodemographic factors. American Journal of Epidemiology. 2014;179(6):781–790. doi:10.1093/aje/kwt330
- van Hees VT, Gorzelniak L, Dean León EC, et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS One. 2013;8(4):e61691. doi:10.1371/journal.pone.0061691
- Rowlands AV, Edwardson CL, Davies MJ, Khunti K, Harrington DM, Yates T. Beyond cut points: accelerometer metrics that capture the physical activity profile. Med Sci Sports Exercise. 2018;50(6):1323–1332. doi:10.1249/mss.0000000000001561
- van Hees VT, Sabia S, Jones SE, et al. Estimating sleep parameters using an accelerometer without sleep diary. Sci Rep. 2018;8(1):12975. doi:10.1038/s41598-018-31266-z
- Matson RIB, Leary SD, Cooper AR, Thompson C, Narendran P, Andrews RC. Objective measurement of physical activity in adults with newly diagnosed type 1 diabetes and healthy individuals. Front Public Health. 2018;6:360. doi:10.3389/fpubh.2018.00360
- Narendran P, Jackson N, Daley A, et al. Exercise to preserve β-cell function in recent-onset Type 1 diabetes mellitus (EXTOD) – a randomized controlled pilot trial. Diabetic Med. 2017;34(11):1521–1531. doi:10.1111/dme.13439
- Cassidy S, Fuller H, Chau J, Catt M, Bauman A, Trenell MI. Accelerometer-derived physical activity in those with cardio-metabolic disease compared to healthy adults: a UK Biobank study of 52,556 participants. Acta Diabetol. 2018;55(9):975–979. doi:10.1007/s00592-018-1161-8
- Sharara E, Akik C, Ghattas H, Makhlouf Obermeyer C. Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC Public Health. 2018;18(1):639. doi:10.1186/s12889-018-5472-z
- Azevedo MR, Araújo CL, Reichert FF, Siqueira FV, da Silva MC, Hallal PC. Gender differences in leisure-time physical activity. Int J Pub Health. 2007;52(1):8–15. doi:10.1007/s00038-006-5062-1
- Ferrand C, Perrin C, Nasarre S. Motives for regular physical activity in women and men: a qualitative study in French adults with type 2 diabetes, belonging to a patients’ association. Health Soc Care Commun. 2008;16(5):511–520. doi:10.1111/j.1365-2524.2008.00773.x
- Bąk E, Marcisz-Dyla E, Młynarska A, Sternal D, Kadłubowska M, Marcisz C. Prevalence of depressive symptoms in patients with type 1 and 2 diabetes mellitus. Patient Preference Adherence. 2020;14:443–454. doi:10.2147/ppa.s237767
- Deischinger C, Dervic E, Leutner M, et al. Diabetes mellitus is associated with a higher risk for major depressive disorder in women than in men. BMJ Open Diabetes Res Care. 2020;8(1). doi:10.1136/bmjdrc-2020-001430
- Pearce M, Garcia L, Abbas A, et al. Association Between physical activity and risk of depression: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(6):550–559. doi:10.1001/jamapsychiatry.2022.0609
- Loprinzi PD, Franz C, Hager KK. Accelerometer-assessed physical activity and depression among U.S. adults with diabetes. Mental Health Phys Act. 2013;6(2):79–82. doi:10.1016/j.mhpa.2013.04.003
- Felez-Nobrega M, Werneck AO, El Fatouhi D, de Luca K, Islam SMS, Franzese F. Device-based physical activity and late-life depressive symptoms: an analysis of influential factors using share data. J Affective Disorders. 2023;322:267–272. doi:10.1016/j.jad.2022.11.006
- Gianfredi V, Blandi L, Cacitti S, et al. Depression and objectively measured physical activity: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(10). doi:10.3390/ijerph17103738
- Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–539. doi:10.1016/j.neubiorev.2019.09.040
- Bhamani MA, Khan MM, Karim MS, Mir MU. Depression and its association with functional status and physical activity in the elderly in Karachi, Pakistan. Asian J Psychiatr. 2015;14:46–51. doi:10.1016/j.ajp.2014.12.004
- Galassetti P, Riddell MC. Exercise and type 1 diabetes (T1DM). Compr Physiol. 2013;3(3):1309–1336. doi:10.1002/cphy.c110040
- Melancon MO, Lorrain D, Dionne IJ. Changes in markers of brain serotonin activity in response to chronic exercise in senior men. Appl Physiol Nutr Metab. 2014;39(11):1250–1256. doi:10.1139/apnm-2014-0092
- Melin EO, Thunander M, Landin-Olsson M, Hillman M, Thulesius HO. Depression, smoking, physical inactivity and season independently associated with midnight salivary cortisol in type 1 diabetes. BMC Endocr Disord. 2014;14:75. doi:10.1186/1472-6823-14-75
- Su C-H, Chuang H-C, Hong C-J. Physical exercise prevents mice from L-Kynurenine-induced depression-like behavior. Asian J Psychiatr. 2020;48:101894. doi:10.1016/j.ajp.2019.101894