
Abstract
Purpose
This study aims to investigate the status of family functioning and dissatisfaction of family function from the perception of adolescents with affective disorders and explore associated factors.
Methods
This was a multicentric cross-sectional study conducted from April 2022 to February 2023. Adolescents with affective disorders were surveyed in representative samples drawn from three hospitals in Sichuan province, China. Data were obtained from 235 participants regarding their demographic characteristics, family characteristics, disease-related characteristics, and family functioning.
Results
The study found family functioning and its’ dissatisfaction both lower than national norms from the perspectives of adolescents. Younger age, single-parent family, and reconstituted family were predictors of not close of cohesion. Younger age, lower educational level of father, and reconstituted family were associated with less change of flexibility. Less times of hospitalizations, higher educational level of father, stem family were more satisfy with cohesion. Higher educational level of father, and stem family were also associated with greater satisfaction with flexibility.
Conclusion
The study demonstrated that the family function of adolescents of affective disorders was poor, more attention should be paid to it. Age, family structure, number of hospitalizations and the educational level of father were influencing factors of family functioning. Therefore, it is important for medical worker to assess demographic and family characteristics of adolescents with affective disorders. Younger children, children of reconstituted family and single-parent family, children with repeated hospitalizations and fathers of lower level of education should be given emphasized in implementation of interventions. Based on the evaluation results, personalized family therapy has been proved to be an affective measure and could be used in clinical work.
Introduction
Affective disorders, including major depressive disorder and bipolar disorder, in which mood disturbance is the predominant clinical feature. These are among the most commonly occurring and seriously impairing diseases worldwide. It estimated that the lifetime prevalence of affective disorders was on a range from 8.5% to 10.7%.Citation1 China Mental Health Survey (CMHS) investigated the prevalence of mental disorders in 2019, results showed the lifetime prevalence of mental disorders was 16.6%. Among these mental disorders, affective disorders ranked second with a lifetime prevalence of 4.06%.Citation2 Adolescent period is a key period of physical and mental development, with rapid physical, emotional, and cognitive changes. Affective disorder is a common disease harming to the physical and mental health of young people. The incidence of affective disorders among adolescents increases year by year.Citation3
Affective disorders are associated with functional impairment and increased risk of premature death due to suicide and medical comorbidities,Citation4,Citation5 leading to a heavy socio-economic burden. Affective disorders have bad influence over the ability of study and daily living of adolescents, even cause self-injury and suicide.Citation6,Citation7
Family Functioning
Family functioning generally refers to the quality of family life at the systemic and dyadic levels and concerns wellness, competence, strengths, and weaknesses of a family.Citation8 According to the Circumplex Model of Marital and Family Systems,Citation9 it is organized by two dimensions – cohesion and flexibility. Cohesion is defined as the emotional bonding that family members have toward one another.Citation10 Flexibility is defined as the ability of the family system to change its power structure, role relationships, and relationship rules in response to situational or developmental demands.Citation11 Poorly functioning families are considered unbalanced on these dimensions, falling either low or high on these characteristics.Citation12
Families are matter to the individuals in enhancing their physiological and psychological development.Citation13 It is also emphasized for adolescents who are experiencing major emotional, cognitive, and social changes.Citation14 Previous research showed that the family relationships of adolescents in early life have great effect on health across their lifespan.Citation15 Healthy family functioning is associated with adolescent positive mental health, including existential well-being, life satisfaction, self-esteem, and a sense of mastery.Citation8 Poor family functioning is a risk factor for the development of mental health problems among adolescents. It may be related to adolescent behavioral and emotional problems,Citation16,Citation17 anxiety, depression,Citation16,Citation18 obsessive-compulsive disorder,Citation19 and severity of suicidal ideation.Citation20
It is widely acknowledged that affective disorders are marked by considerable impairment in family functioning.Citation21 Family functioning was found to be significantly associated with severity of disease,Citation22,Citation23 suicide attempts,Citation24 the episode of disease,Citation25 the mental health of other family members,Citation26,Citation27 and family structure.Citation28 A family member with any psychiatric illness (schizophrenia, bipolar disorder, major depression, anxiety disorders, eating disorders, substance abuse and adjustment disorders) is a general adverse factor leading to poor family functioning. Family structure refers to the combination of family members, that is, the patterns of interaction between individuals within a family. Based on the number of family members and the relationships between them, family structure is generally classified into four types: nuclear family, stem family, reconstituted family, and single-parent family. A nuclear family typically comprises two parents and their unmarried children. A stem family centers around parents, living with a couple of married children or other relatives. A reconstituted family, also called a blended family, forms when at least one adult brings children from a prior marriage or relationship. Meanwhile, a single-parent family consists of a parent raising underage children who lack independence or are still in full-time education.
Adequate family functioning has a positive impact of the treatment of affective disorders.Citation18,Citation20 Family functioning is vital important to both adolescents and individuals diagnosed with affective disorder. Closer attention needs to be paid to adolescents with affective disorder.
Overview of the Present Study
Most studies have focused on investigating the current status of family functioning among participants and its influencing factors, with fewer studies regarding the assessment of ideal family functioning. In this study, not only was the actual family functioning of adolescents with affective disorder measured, but also their ideal family functioning from the youth perspective. The difference between actual and ideal family function represents the level of dissatisfaction with family functioning. More specifically, family dissatisfaction, taken as the degree of dissatisfaction felt by an individual in relation to his family and the relationships therein. The dissatisfaction calculated with family functioning can effectively identify the target population for intervention implementation. The factors influencing dissatisfaction with family functioning can further clarify the key populations and considerations for intervention implementation.
Theory and Hypotheses
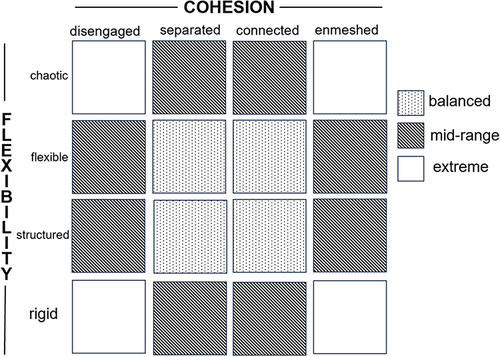
The study based on the Circumplex Model, one of the intervention models which assesses the family dynamics. The Circumplex Model is built on three dimensions; cohesion, flexibility, and communication. The Circumplex Model could be best illustrated by a diagram as following. The model represents the interaction of dimensions of cohesion and flexibility. The matrix outlining 16 distinct family types, further divided into three primary kinds of family functioning: balanced families, mid-range families, and extreme families. The last dimension, communication, is viewed as a dimension that can facilitate movement between flexibility and cohesion.Citation9,Citation10 Shown in .
Figure 1 The Circumplex Model.
Given the above-mentioned considerations, the aim of the study was to measure the state of family function, work out dissatisfaction of family function and explore their related factors of adolescents with affective disorders in China. Thus, we propose the following hypotheses:
Hypothesis 1: Adolescents with affective disorders will perceive lower levels of family functioning compared to adolescents without affective disorders.
Hypothesis 2: Adolescents with affective disorders will perceive higher degree of family dissatisfaction compared to adolescents without affective disorders.
Hypothesis 3: Family structure would be an important factor of family functioning and dissatisfaction of family functioning.
Materials and Methods
Study Design
This was a multicentric cross-sectional study conducted from May 2022 to December 2023 in three hospitals of two cities in Sichuan province, China. Convenience sampling was used to select participants into the study. All three hospitals were Grade-A tertiary hospitals, and national or provincial regional mental health centers. This design allows researchers to assess various aspects of family functioning and gather data from multiple families at a specific moment. Moreover, a cross-sectional design facilitates the efficient collection of data, making it feasible to assess a wide range of variables in different place.
Participants
Participants were recruited from adolescent inpatients diagnosed with affective disorders in three hospitals. The inclusion criteria were as follows: 1) patients clinically diagnosed having affective disorder using International Classification of diseases (ICD-11); 2) patients aged 10–19; 3) patients having primary school education or above; 4) be willing to participant. Patients with other serious mental illnesses, such as schizophrenia, mental retardation et al were excluded.
Data Collection
Data were collected using a paper-and-pencil questionnaire. Patients completed questionnaires during their hospital stay. Trained investigators explained the study purpose, procedure, potential risks and benefits, and guaranteed confidentiality and voluntary participation before data collection. Informed consent was obtained from participants or their legal guardians before data collection and could withdraw from the study at any time. Time needed to complete the survey was 20 to 30 minutes. The disease-related characteristics were filled with the assistance of investigators. All questionnaires were checked for completeness and accuracy on the spot. All the questionnaires from three hospitals were administered by the research team. After excluding participants who failed to provide information on the main variables, the final valid sample consisted of 235 adolescents.
Measures
Demographics Characteristics
Demographic characteristics including gender, age, ethnic groups, educational level, and residence. A total of 235 teenagers diagnosed with affective disorders were recruited from three different hospitals in Sichuan province. The participants’ average age was 14.8 years (SD = 1.62), with an age range of 11–18 years old. Most participants were female (187, 79.6%), and the Han population (222, 94.5%).
Family Characteristics
Family characteristics were recorded as whether one-child family, family structure, educational level of father, and educational level of mother. There was a relatively even educational level (Junior school and below/High school), and whether one-child family (Yes/No) proportion.
Disease-Related Characteristics
The information of diagnosis, disease duration, number of episodes, number of hospitalizations, whether consider NSSI (nonsuicidal self-injury) in the past month and whether commit NSSI in the past month was collected. About 80% (190, 80.9%) participants were diagnosed with depressive disorder. Approximately 90% participants considered NSSI in the past month (224, 95.3%) and committed NSSI in the past month (212, 90.2%).
Family Functioning
Family functioning was measured by using the Chinese version of Family Adaptability and Cohesion Evaluation Scale, version III (FACES-III).Citation29,Citation30 Both realistic state and ideal state of FACES were evaluated in this study. The FACES is a family self-report assessment, consists of 30 items relating to 2 dimensions: family flexibility and cohesion. Each item is scored on a 5-point Likert scale ranging from 1 (never) to 5 (nearly always). Scores of the two dimensions are calculated separately. The absolute value of the difference between two dimensions represents the level of dissatisfaction, higher numerical values indicate higher dissatisfaction. The flexibility is divided into four different levels according to Circumplex Model, described as chaotic (too much change, <44.7), flexible (44.7–50.9), structured (50.9–57.1), and rigid (not enough change, >57.1). The cohesion is divided into four levels: disengaged (not close enough, <55.9), separated (55.9–63.9), connected (63.9–71.9), and enmeshed (overly close, >71.9). The resulting matrix forms a typology of 16 different family types, which collapsed further into three major categories of family functioning: balanced families, mid-range families, and extreme families. This scale was translated into different languages and widely used.Citation11,Citation31,Citation32 The Cronbach’s α of Chinese version of FACES is 0.68–0.85.Citation30,Citation33
Data Preparation and Data Analysis
Before data entry, we checked completeness and accuracy of questionnaires. Some missing values were supplemented according to medical records of participants. Other missing values were substituted by average or median.
All statistics were analyzed using SPSS statistics 26.0, and a P value less than 0.05 was considered statistically significant. Descriptive statistics was performed by mean (standard deviation, SD), median (interquartile range, IQR), frequency and percentage. Independent sample T-test, one-way ANOVA, and rank sum test were used to examine the realistic state and dissatisfaction of adolescent affective disorders with different categorical variables. Spearman rank correlation analysis was used to assess the relationship between continuous data and outcome indicators. A multiple linear regression analysis was conducted to explore the associated factors of the realistic state and dissatisfaction.
Results
Family Function
Four family structures were recorded in this study: nuclear family (80, 34.0%), single-parent family (36, 15.3%), reconstituted family (37, 15.7%), and stem family (82, 34.9%).
shows the results of realistic and ideal FACES scores. The mean score of realistic cohesion and flexibility were 56.31 ± 11.77 and 36.63 ± 10.61 separately, resulting in about 60% extreme families (137,58.3%) and only 28 balanced families (11.9%). Both the ideal scores of cohesion (69.03 ± 11.41) and flexibility (51.71 ± 11.54) were considerably superior to the realistic state. Four levels of cohesion and flexibility are presented in .
Table 1 Dimensions and Family Types of Family Function of Adolescent with Affective Disorders (N = 235)
Table 2 Four Levels of Cohesion and Flexibility of Adolescent Affective Disorders (N = 235)
Factors Associated with Realistic and Dissatisfaction of Family Functioning
The results of inter-group comparison and Spearman correlation analysis showed that age (r = 0.170, P<0.01), gender (T = 2.423, P < 0.05), family structure (F = 7.100, P < 0.01), and educational level of mother (F = 2.735, P < 0.01) were significantly associated with realistic cohesion among adolescent affective disorders. There are statistically significant relationships between age (r = 0.224, P < 0.01), family structure (F = 5.617, P < 0.01), educational level of mother (F = 2.662, P < 0.05), whether consider NSSI in the past month (F = 3.068, P < 0.05) and realistic flexibility. These results are shown in and .
Table 3 General Characteristics of Adolescent Affective Disorders, and the Univariate Analysis of Realistic Family Functioning (N = 235)
Table 4 the Univariate Analysis of Dissatisfaction of Cohesion and Flexibility (N = 235)
The result of multiple linear regression analysis is shown in . Younger age (B = 0.983, P = 0.034), single-parent family (B = −5.129, P = 0.023), and reconstituted family (B = −7.456, P=0.001) were predictors of not close of cohesion. Younger age (B = 1.349, P = 0.001), lower educational level of father (B = 1.204, P = 0.022), and reconstituted family (B = −4.291, P = 0.034) were associated with less change of flexibility.
Table 5 Multiple Linear Regression on Realistic Family Function and Dissatisfaction of Adolescent Affective Disorders (N = 235)
We also found that less times of hospitalizations (B = 2.191, P = 0.010), higher educational level of father (B = −1.188, P = 0.039), stem family (B = −3.762, P = 0.031) got a lower score of cohesion dissatisfaction. Higher educational level of father (B = −1.404, P = 0.016), and Stem family (B = −4.349, P = 0.013) were also represented a lower score of flexibility dissatisfaction.
Discussion
This study aimed to investigate the status of family functioning and dissatisfaction of family function among adolescents with affective disorders and explore associated factors. The average scores of family cohesion and flexibility were 56.31 ± 11.77 and 36.63 ± 10.61, separately. Both scores are lower than the national norms (cohesion, 63.90 ± 8.00; flexibility, 50.90 ± 6.20). The dissatisfaction of two dimensions were calculated in this study. Median scores of cohesion and flexibility were 12.00 (2.38, 20.00) and 13.00 (6.00, 24.00), higher than the national norms.Citation33 The results were in line with previous studies.Citation21,Citation34 Further analysis showed only 28 (11.9%) participants were balanced families, meaning that most families incline to be unhealthy.Citation10
The Factors of Realistic Cohesion and Flexibility
The results of this study demonstrated that older teenagers had higher score of realistic cohesion and flexibility. This finding was in line with previous study,Citation35 elder people tended to describe their families as having high flexibility Levels. One possible reason of the result is older adolescents may have more mature mind and behavior as they grow. They have a better learn of their family members, such as the way expressing love, which could make family relationship closer. Another reason may be older adolescents gradually get used to the way of doing things of their family members. It is easier for these families to reach a consensus and solve problems.
We also observed that participants from reconstituted family have lower family cohesion and flexibility. One possible explanation of the result may be that the time together of children and stepparents has been brief. They are not familiar with each other, leading to difficulty of establishing intimate relationships. Person of reconstituted family unwilling to exposure their mind, making it hard to change of family system.
In the study, multiple linear regression analysis showed that these of single-parent family have lower family cohesion comparing with nuclear family. One reason may be single-parent family have heavier economic burden of raising children. Father/mother spends more time on work, and less family time on children. Besides, the absence of the one-parent role resulting in the quantitative lack of affection and company comparing with nuclear family. In addition, previous researchesCitation28 showed that had significantly higher odds of mental health issues such as depression, suicidal ideation, perceived stress, and poor perceived health status, leading to poorer family functioning.
Therefore, it’s important for medical worker to assess demographic and family characteristics of adolescents with affective disorders. More attention should be paid to younger children, children of reconstituted family and single-parent family. Family therapies were proved to be effective in reducing emotional problems and behavior problems.Citation36,Citation37 Proper family therapy could be used in clinical work based on preliminary evaluation results.
The Factors of Cohesion and Flexibility Dissatisfaction
We found the higher educational level of fathers, the lower level of family functioning dissatisfied the children perceived. Previous research has indicated that father involvement is more strongly correlated with positive outcomes on child emotional, behavior, cognitive, and academic development.Citation37,Citation38 Since fathers would make fewer changes in their behaviors and perceptions of child rearing compared with mothers,Citation39 higher educated fathers may have more knowledge of parenting. This was confirmed in our study. The multiple linear regression analysis of realistic flexibility showed fathers of higher level of education indicated higher family flexibility. Given that fathers’ presence and behaviors toward their children, father involvement should be concerned, and they should be encouraged to participant in parent-training programs.
We also observed that participants from stem families have more satisfaction of family compared with nuclear family. Stem family consists of three generations of immediate relatives, grandparents, parents, and unmarried children. It is the second family type following nuclear family in China.Citation40 In a stem family, both the grandparents and parents share the responsibility of raising the children. Some studies revealed that emotional support within families promoted family functioning.Citation12 For one thing, most grandparents have retired and have more time with the children. For another thing, grandparental closeness love is a prevalent social occurrence, referring to the deep emotional bond between grandparents and grandchildren. This relationship often transcends blood ties, resembling more of an emotional refuge. Therefore, grandparents are more likely to meet their children’s needs and expectations than their parents.
The findings suggest the more hospitalizations, the higher cohesion dissatisfaction. More hospitalizations mean more time in hospital. The lack of family communication and family activity may lead to poor family cohesion.
The results suggested that adolescent patients with repeated hospitalizations and fathers of lower level of education should be emphasized in implementation of interventions. Personalized intervention programs could be made according to individual circumstances. For adolescents with repeated hospitalizations, tracking family situation, assessing effectiveness, and devising stepped intervention measures would be useful. For fathers with lower level of education, using simpler and more understandable methods and repeated interventions to enhance the effectiveness of the intervention.
Limitations and Future Research
Further, there were several limitations in the study. First, the study only focused on youth perspective, family members were not included. Hence, whether the participants’ views represented a full or valid picture of family functioning is unknown. In future studies, involved other people of a family in comprehensive assessment of family functioning is an effective method to enhance research reliability. Secondly, this study did not comprehensively include both internal and external influencing factors, such as, severity of affective disorders, peer relationships socio-occupational functioning and school environments. Future studies could delve into more associated factors during the survey based on existing work. Also, the study is cross-sectional so that causal relationships cannot be identified with confidence. Future studies can use longitudinal methods to find better evidence for cause and effect. The sample size in this study is limited, and all three survey points are in urban areas, leading to relatively poor representation. A large amount of sample and rural areas should be considered in future research.
Conclusion
The study demonstrated that the family function of adolescents of affective disorders was poor, more attention should be paid to it. Age, family structure, number of hospitalizations and the educational level of father were influencing factors of family functioning. Therefore, it’s important for medical worker to assess demographic and family characteristics of adolescents with affective disorders. Younger children, children of reconstituted family and single-parent family, children with repeated hospitalizations and fathers of lower level of education should be given emphasized in implementation of interventions. Based on the evaluation results, personalized family therapy has been proved to be an affective measure and could be used in clinical work.
Ethics Statements
All procedures of this study were in accordance with the ethical standards of the institutional research committee and the Helsinki Declaration. This study was approved by West China Hospital Medical Ethics Committee. Informed consent was obtained from participants or their legal guardians before data collection.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Ventimiglia I, Van der Watt A, Kidd M, et al. Association between trauma exposure and mood trajectories in patients with mood disorders. J Affect Disord. 2020;262:237–246. doi:10.1016/j.jad.2019.10.057
- Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
- Fu XL, Zhang K, Chen XF, et al. 中国国民心理健康发展报告 (2021~2022) [Report on national mental health development in China (2021–2022)]. Beijing: Social Sciences Academic Press (China); 2023. Chinese.
- Hayes JF, Miles J, Walters K, King M, Osborn DP. A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr Scand. 2015;131(6):417–425. doi:10.1111/acps.12408
- Baxter AJ, Page A, Whiteford HA. Factors influencing risk of premature mortality in community cases of depression: a meta-analytic review. Epidemiol Res Int. 2011;2011(7397):1–12. doi:10.1155/2011/832945
- Li YX, Ren GY, Ren K, et al. A qualitative study on the influencing factors of parents′ participation in emotional management of adolescents with affective disorder. Chin J Pran Nurse. 2023;39(12):937–943. doi:10.3760/cma.j.cn211501-20220613-01840
- World Health Organization. Adolescent and young adult health unit. Available from: https://www.who.int/news-room/factsheets/detail/adolescents-health-risks-and-solutions. Accessed January 10, 2024.
- Shek DT. Family functioning and psychological well-being, school adjustment, and problem behavior in Chinese adolescents with and without economic disadvantage. J Genet Psychol. 2002;163(4):497–502. doi:10.1177/0192513x04272618
- Olson DH, Sprenkle DH. Circumplex model of marital and family systems: Vl. Theoretical update. Fam Process. 1983;22(1):69–83. doi:10.1111/j.1545-5300.1979.00029.x
- Olson D. FACES IV and the Circumplex Model: validation study. J Marital Fam Ther. 2011;37(1):64–80. doi:10.1111/j.1752-0606.2009.00175.x
- Cong CW, Tan CS, Noew HS, et al. Psychometric evaluation of the Malay version of the family adaptability and cohesion evaluation scale III for Malaysian adolescents. Int J Environ Res Public Health. 2022;19(1):156. doi:10.3390/ijerph19010156
- Wang YH, Haslam M, Yu M, et al. Family functioning, marital quality and social support in Chinese patients with epilepsy. Health qual Life Out. 2015;13(1):10. doi:10.1186/s12955-015-0208-6
- Botha F, Booysen F. Family functioning and life satisfaction and happiness in south African households. Soc Indic Res. 2013;119(1):163–182. doi:10.1007/s11205-013-0485-6
- Mastro Theodoros S, Canário C, Cristina Gugliandolo M, Merkas M, Keijsers L. Family functioning and adolescent internalizing and externalizing problems: disentangling between-, and within-family associations. J Youth Adolesc. 2020;49(4):804–817. doi:10.1177/0192513X09348488
- Chen E, Brody GH, Miller GE. Childhood close family relationships and health. Am Psychol. 2017;72(6):555–566. doi:10.1037/amp0000067
- Simpson EG, Vannucci A, Ohannessian CM. Family functioning and adolescent internalizing symptoms: a latent profile analysis. Journal of Adolescence. 2018;64(1):136–145. doi:10.1016/j.adolescence.2018.02.004
- Lee HS. Effect of self-differentiation and family function on mental health in adolescents. J Korean Acad Child Health Nurs. 2010;16(4):297–303. doi:10.4094/jkachn.2010.16.4.297
- Huang X, Hu N, Yao Z, et al. Family functioning and adolescent depression: a moderated mediation model of self-esteem and peer relationships. Front Psychol. 2022;13:962147. doi:10.3389/fpsyg.2022.962147
- Murphy YE, Flessner CA. Family functioning in paediatric obsessive compulsive and related disorders. Br J Clin Psychol. 2015;54(4):414–434. doi:10.1111/bjc.12088
- Dardas LA. Family functioning moderates the impact of depression treatment on adolescents’ suicidal ideations. Child Adolesc Ment Health. 2019;24(3):251–258. doi:10.1111/camh.12323
- MacPherson HA, Ruggieri AL, Christensen RE, et al. Developmental evaluation of family functioning deficits in youths and young adults with childhood-onset bipolar disorder. J Affect Disord. 2018;235:574–582. doi:10.1016/j.jad.2018.04.078
- Tamplin A, Goodyer IM. Family functioning in adolescents at high and low risk for major depressive disorder. Eur Child Adolesc Psychiatry. 2001;10(3):170–179.
- Reinares M, Bonnín CM, Hidalgo-Mazzei D, et al. Family functioning in bipolar disorder: characteristics, congruity between patients and relatives, and clinical correlates. Psychiatry Res. 2016;245:66–73. doi:10.1016/j.psychres.2016.08.010
- Berutti M, Dias RS, Pereira VA, Lafer B, Nery FG. Association between history of suicide attempts and family functioning in bipolar disorder. J Affect Disord. 2016;192:28–33. doi:10.1016/j.jad.2015.12.010
- Weinstock LM, Keitner GI, Ryan CE, et al. Family functioning and mood disorders: a comparison between patients with major depressive disorder and bipolar I disorder. J Consult Clin Psychol. 2006;74(6):1192–1202. doi:10.1037/0022-006X.74.6.1192
- Du Rocher Schudlich TD, Youngstrom EA, Calabrese JR, et al. The role of family functioning in bipolar disorder in families. J Abnorm Child Psychol. 2008;36(6):849–863. doi:10.1007/s10802-008-9217-9
- Foster CE, Webster MC, Weissman MM, et al. Course and severity of maternal depression: associations with family functioning and child adjustment. J Youth Adolesc. 2008;37(8):906–916. doi:10.1007/s10964-007-9216-0
- Park H, Lee KS. The association of family structure with health behavior, mental health, and perceived academic achievement among adolescents: a 2018 Korean nationally representative survey. BMC Public Health. 2020;20(1):510. doi:10.1186/s12889-020-08655-z
- Green RG, Harris RN, Forte JA, et al. Evaluating FACES III and the circumplex model: 2440 families. Fam Proc. 1991;30(1):55–73. doi:10.1111/j.1545-5300.1991.00055.x
- Fei LP, Shen QJ, Zhen YP, et al. “家庭亲密度和适应性量表”和“家庭环境量表的”初步评价 [Preliminary evaluation of Chinese version of FACES II and FES: comparison of normal families and families of schizophrenic patients]. Chin Ment Health J. 1991;5(5):198–202. Chinese.
- Williams LR, Anthony EK. A model of positive family and peer relationships on adolescent functioning. J Child Fam Stud. 2015;24:658–667. doi:10.1007/s10826-013-9876-1
- Park YY, Jeong YJ, Lee J, et al. The influence of family adaptability and cohesion on anxiety and depression of terminally ill cancer patients. Support Care Cancer. 2018;26(1):313–321. doi:10.1007/s00520-017-3912-4
- Hu YL, Liang LP, Mei YT, et al. Correlation analysis of psychological resilience and family closeness and adaptability in moderately depressed patients. Chin J Nurs. 2017;33(13):1013–1015. doi:10.3760/CMA.J.ISSN.1672-7088.2017.13.014
- Berryhill MB, Smith J. College student chaotically-disengaged family functioning, depression, and anxiety: the indirect effects of positive family communication and self-compassion. Marriage Fam Rev. 2021;57(1):1–23. doi:10.1080/01494929.2020.1740373
- Rada C. Latent class analysis approach for the family adaptability and cohesion evaluation scale IV among young people from Romania: the first step for validation. J Family Issues. 2018;39(6):1598–1615. doi:10.1177/0192513X17714508
- Carr A. Family therapy and systemic interventions for child‐focused problems: the current evidence base. J Fam Ther. 2019;41(2):153–213. doi:10.1111/1467-6427.12226
- Pérez-García M, Sempere-Pérez J, Rodado-Martínez JV, López DP, Llor-Esteban B, Jiménez-Barbero JA. Effectiveness of multifamily therapy for adolescent disruptive behavior in a public institution: a randomized clinical trial. Child Youth Serv Rev. 2020;117:105289. doi:10.1016/j.childyouth.2020.105289
- Lundahl BW, Tollefson D, Risser H, et al. A meta-analysis of father involvement in parent training. Res Social Work Prac. 2016;18(2):97–106. doi:10.1177/1049731507309828
- Planalp EM, Braungart-Rieker JM. Determinants of father involvement with young children: evidence from the early childhood longitudinal study-birth cohort. J Fam Psychol. 2016;30(1):135–146. doi:10.1037/fam0000156
- Jia T. 结构家庭治疗法介入主干家庭亲子冲突问题的个案研究 [Case study of structural family therapy in parent-child conflict problems of stem family]. Chongqing: Southwest University; 2020. Chinese.