
Abstract
Background
Chinese calligraphic handwriting (CCH) has demonstrated a new role in health and therapy. Meanwhile, meditation is an traditional and effective method for coping with stress and staying healthy. This study compared the effectiveness of CCH and meditation as distinctive and parallel stress reduction interventions.
Methods
Thirty graduate students and academic staff members in Taiwan who suffered from stress were selected by the General Health Questionnaire and randomly assigned to one of three treatment groups, ie, a CCH group, a meditation group, or a control group, for 8 consecutive weeks. Changes in physiological parameters were measured before, during, and after treatment.
Results
CCH and meditation showed their strength in the respective indices of stress. There was a significant difference in respiratory rate, heart rate, and electromyographic scores between the groups. Comparing pre- and post-effects, a decrease in heart rate and an increase in skin temperature was seen in subjects who practiced CCH. Increased skin temperature and decreased respiratory rate were also seen in subjects who practiced meditation, along with reduced muscle tension and heart rate.
Conclusion
CCH and meditation have good effects in stress reduction. CCH is a particularly promising new approach to reducing stress.
Introduction
Chinese calligraphic handwriting (CCH) involves use of a soft-tipped brush to write special Chinese characters and is widely regarded as a unique art form. In the past, research on CCH has focused mainly on how to execute and appreciate it artistically by following the experiences of the great masters. During the last three decades, Kao et al have conducted systematic research on the bodily and mental processes involved in brush handwriting from a psychological perspective according to the psychogeometric theory of Chinese character writing.Citation1,Citation2 Recently, some of this research has established CCH as having positive effects on cognitive enhancement in children with attention deficit hyperactivity disorderCitation3 and cognitive recovery in patients with Alzheimer’s disease.Citation4–Citation8 There is also some clinical evidence that CCH can help with behavioral change and emotional stability in patients with depressionCitation1 or cancer.Citation8,Citation9 In light of these findings, we suggest that practicing CCH has a further role in improving the practitioner’s psychological and physical health through training, therapy, and rehabilitative delivery.
Meditation forms part of Asian religion and philosophy, and is a traditional and effective intervention for both mental and psychological conditions, such as depression, anxiety, and various stress-related physical symptoms.Citation10 Meditation essentially consists of a person sitting upright in a comfortable position and concentrating on a single point continuously with mindfulness and attention. Meditation has its origins in the religious practices of India, including Zen and yoga. It is considered to be an emotion-focused method of coping that does not aim to alter the sources of stress. Empirical studies of meditation have confirmed significant improvements in physiological and psychological functioning, such as body flexibility,Citation11 perceptibility,Citation12 cerebral activation, immune system function,Citation13,Citation14 emotional calming,Citation15–Citation17 and cognitive arousal and activation.Citation18–Citation20
Stress and strain are universal experiences in people’s lives, and are of serious concern to psychologists and medical and health professionals. In a rapidly developing and globalizing world, the competitiveness and pursuit of material life contribute to the causation and extent of stress felt in daily life. The consequences of stress may be reflected in terms of behavioral, psychological, and physical symptoms.Citation21–Citation24 Preventative measures, strategic interventions, and effective reduction of stress and strain are important issues in contemporary life. Common interventions for stress reduction include relaxation, meditation, biofeedback training, and emotional outlets. CCH is emerging as a further form of therapy for stress intervention. The main purpose of the present study was to compare the effectiveness of CCH and meditation as methods of stress reduction.
Materials and methods
Participants
Thirty graduate students and staff members were recruited from the National Central University in Taiwan and screened by the 28-item General Health Questionnaire (GHQ-28).Citation25,Citation26 A cutoff of 4/5 was used to define the level of stress in this study according to the GHQ-28 manual.Citation25 Participants were randomly assigned to one of three groups, ie, a CCH group (n=10), a meditation (n=10) group, or a control group (n=10). Each participant reported normal or corrected-to-normal vision, and being right-handed with no prior experience of calligraphy or meditation. All participants gave their informed consent to participate in this study.
Procedures
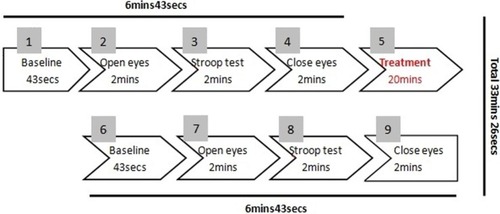
Participants in the three groups received standard treatment in separate rooms that were quiet, well lit, and free from interference. Each group engaged in its respective training activities. Each treatment session lasted 33 minutes and 26 seconds (see ), with one session per week for 8 consecutive weeks. Before the treatement, there was a 6 minute, 43 second preparatory process. All participants underwent baseline measurements of all physiological parameters in 43 seconds. They sat silently with their eyes open for 2 minutes. They then performed a color test for stress arousal (2 minutes), which was followed by closing their eyes for 2 minutes in preparation for treatment with calligraphy or meditation. After 20 minutes of treatment, the recovery process (6 minutes 43 seconds) was the same as that before treatment. We used the baseline measures (the first 43 seconds) before the treatment as the pre-test physiological parameters and the baseline measures (the second 43 seconds) after the treatment as the post-test physiological parameters. Each participant in the CCH group participated in a standard calligraphy training protocol led by a trained researcher. The content of the Chinese calligraphy characters was chosen at random from a handbook of classic calligraphy writing. All participants used the same sized brushes and normal rice paper. The meditation group was instructed on the details of the standard technique of meditation, which required the participants to mindfully control and focus on deep abdominal breathing with eyes closed. The procedure was the same as in the CCH group. Participants in the control group received no particular training during sessions.
Figure 1 Standard treatment procedure for calligraphy and meditation.
Abbreviations: mins, minutes; secs, seconds.
Physiological parameters
Changes in heart rate, electromyographic scores, skin temperature, and respiratory rate were measured before, during, and after each treatment session over 8 consecutive weeks. The BioGraph-Pro-Com+ system (Thought Technology Ltd, Montreal, Canada) was used to monitor indicators of stress. To avoid the influence of diurnal fluctuation on physiological parameters, the treatments and measurements were performed at fixed time periods across days.
Stress-related symptoms
The Chinese version of the GHQ-28Citation25,Citation26 was used to measure the participants’ stress symptoms, and consists of four subscales, ie, somatic symptoms, anxiety and insomnia, social dysfunction, and severe depression. The test was administered to each participant before the experiment to select participants. The validity and reliability of this test is established to be acceptable.Citation27–Citation30 In our study, the GHQ-28 had satisfactory internal consistency (Cronbach’s alpha 0.96).
Statistical analysis
Effectiveness was tested using the Statistical Package for Social Sciences version 19.0 (IBM Corporation, Armonk, N Y, USA). One-way Analysis of Variance (ANOVA) for quantitative variables or chi-square for qualitative variables was used to compare the demographic characteristics and the baselines or the pre-treatment among three groups. Two-way repeated-measures analysis of variance was used to evaluate physiological parameters, with a pre-post contrast effect being the within-group factor and the method of intervention methods as the between groups measure. Post hoc multiple comparisons were performed by using the Last significant Difference (LSD) adjustment. The paired samples t-test was used only when the pre-post main effects were significant within groups.
Results
Sample characteristics
A total of 30 participants (13 males and 17 females, aged 19–35 years) meeting our inclusion criteria were recruited. The demographic and clinical characteristics of the three groups at baseline are shown in . Results of the ANOVA and the chi-square tests showed that none of the demographics, GHQ total and subscale scores, and physiological parameters had any significant differences among the three groups (all P>0.05), except for heart rate (HR) (P=0.049).
Table 1 Demographics and baseline measures by treatment group
Effects of intervention on physiological arousal
There was a significant difference in the pre-post comparison for heart rate (F(1,27)=10.960, P=0.003, effect size 0.289). The interaction effect between pre-post and the groups was also significant (F(2,27)=5.436, P=0.010, effect size 0.287). Paired-samples t-tests showed that both CCH (P=0.003) and meditation (P=0.002) significantly decreased the post-treatment heart rate, but no pre-post difference was found in the control group. There was a significant difference in pre-post scores between the CCH group and the meditation group (P=0.033), with the CCH group showing a greater decline on treatment than the meditation group (see and ).
Figure 2 Heart rate pre- and post-treatment for the three groups.
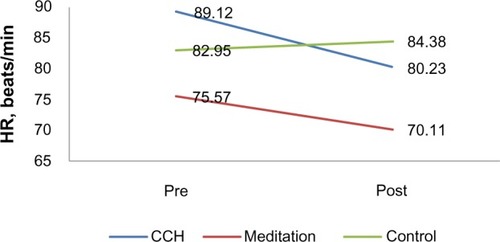
Table 2 Repeated-measures analysis of variance on significant physiological arousal parameters
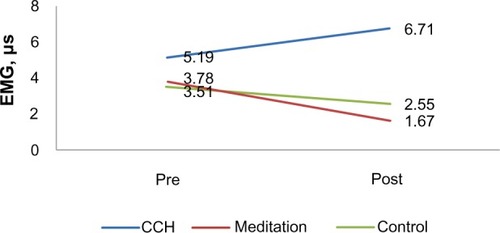
For the electromyographic data, the interaction effect between pre-post and the groups was significant (F(2,27)=3.620, P=0.040, effect size 0.211). However, there was no significant main pre-post effect (F(1,27)=0.838, P=0.368, effect size 0.030). The two active interventions had a different impact on post-treatment measures. Electromyographic scores in the CCH group increased, but not significantly so. However, the meditation group (P=0.000) and the control (P=0.036) group showed a significant decrease in electromyographic scores after treatment. There was also a significant difference in pre-post changes in scores between the CCH group and the meditation group (P=0.036, see and ).
Figure 3 Electromyograghic (EMG) pre- and post-treatment for three groups.
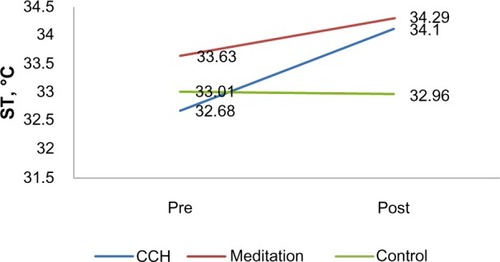
For skin temperature, both the main pre-post effect (F(1,27)=10.540, P=0.003, effect size 0.281) and the interaction effect (F(2,27)=3.981, P=0.031, effect size 0.228) were statistically significant. The CCH (P=0.019) and meditation interventions (P=0.005) significantly increased the participants’ post-treatment skin temperature. Furthermore, the CCH group’s ST (1.42) showed greater pre-post rise than ST increased of the meditation group (0.66) after the treatment, while no pre-post difference was found in the control group (see and ).
Figure 4 Skin temperature (ST) pre- and post-treatment for three groups.
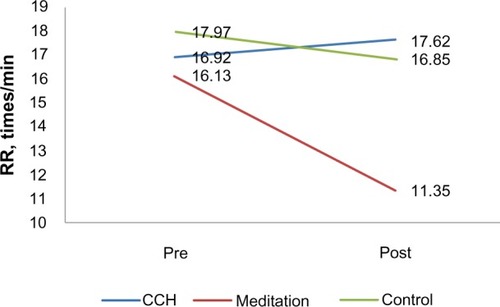
For respiratory rate, the study groups showed different patterns of treatment effect as the intervention proceeded, which was indicated by a significant two-way interaction (F(2,27)=16.383, P=0.000, effect size 0.548). CCH training increased the post-treatment respiratory rate, but the change was not significant. The pre-post changes were significant (see and ) in the meditation (P=0.000) and control (P=0.024) groups. The pre-post changes in the meditation group were significantly different to the changes in the other two groups (P=0.016 versus the CCH group and P=0.013 versus the control group).
Figure 5 Respiration rate (RR) pre- and post-treatment for the three groups.
Discussion
The present study investigated the effects of CCH training and meditation (an established interventional approach), and compared these with a control group. The results of the present study show that 8 weeks of CCH training had a significant attenuating effect on physiological parameters of arousal (heart rate, electromyographic scores, skin temperature, and respiratory rate) in participants suffering from stress on a daily basis. The effectiveness of CCH compared favorably with that of meditation, which is a well established method for stress reduction. These findings are encouraging, in that CCH represents an equally useful technique for reducing stress.
Specifically, CCH training slowed the heart rate, increased the skin temperature, and decreased the respiratory rate. These results are consistent with the findings of previous studies, ie, that participants experience relaxation and emotional calmness when performing CCH.Citation9,Citation31 In 2006, Kao argued that the act of brushing required heightened attention and concentration on the part of the practitioner, and thus resulted in emotional stabilization and physical relaxation.Citation32 It seemed that their bodily activities were inconsistent with their calming mental state, which reflected convincingly that practicing the CCH integrates the mind and the body in this graphonomic process. Further, years of empirical research have found that the act of calligraphic handwriting is capable of improving the writer’s cognitive activity.Citation3–Citation8 A review of the literature on various art therapies, including dance, music, drama, and painting, shows that some of these practices have positive effects on relaxation and emotional expressiveness, but bring about little improvement in the practitioner’s cognitive abilities.Citation33 However, the main difference between art therapies and CCH is that CCH considerably benefits the practitioner’s cognitive and verbal scores, while at the same time promoting relaxation and expressiveness. Therefore, this treatment effect may be more significant in people who are particularly vulnerable to behavioral or cognitive impairment, such as adults with Alzheimer’s disease and children with attention deficit hyperactivity disorder, as well as those suffering from stress or strain, eg, cancer patients. Further research should investigate whether practicing the writing of different typographical styles of Chinese characters will also bring about changes in physical state, mood, and cognitive ability. If empirically confirmed, we could identify different styles of characters targeting different groups of patients.
Meditation is rapidly becoming a contemporary brand of Oriental medicine. Consistent with other studies of meditation, the present study confirmed that practicing meditation can ameliorate several symptoms of psychological stress, ie, reduce heart rate, increase skin temperature, promote muscle relaxation, and slow the respiratory rate. However, this therapy is generally regarded as emotion-focused, and is not able to address the sources of stress. Recent meditative treatments are more oriented toward mindfulness-based interventions, eg, mindfulness-based cognitive therapyCitation34 and mindfulness-based stress reduction,Citation35–Citation37 which are popular in contemporary psychotherapy.
In this regard, researchers have found that the cognitive aspects of mindfulness meditation, such as mindful breathing, may cause changes in the cognitive processes associated with stress management. Trait mindfulness may be predictive of a decreased frequency of negative automatic thoughts during the brief practice of mindfulness training.Citation38–Citation40 This cognitive improvement enriches the therapeutic function of meditation, and thus establishes it as an effective form of complementary and alternative medicine.
Although this study produced some encouraging results, it has some limitations. First, the sample size was small, and there was a significant difference in mean heart rate between the three groups at baseline. However, subjects in the CCH and meditation groups both showed a significant decrease in heart rate during the study. Secondly, the main pre-post effect was significant, and the mean change for the pre-post measure in the CCH group was pronounced. Thirdly, we undertook no training for participants in the control group. The 20-minute no-treatment regimen required subjects in the control group to sit quietly in a silent room, as for the meditation intervention. Therefore, electromyography scores and respiratory rates decreased significantly, which is also observed with the practice of meditation. Future research needs to consider designing more comprehensive and more efficacious components of CCH.
As traditional methods, both CCH and meditation have positive effects in terms of stress reduction. The main difference between CCH and meditation is that CCH integrates the mind and body during writing in the form of enhanced cognitive facilitation and verbal ability, while still maintaining a relaxed state and physiological slow-down.Citation8 The results of this study demonstrate that CCH training and meditation are both practical and effective methods for stress reduction.
Disclosure
The authors report no conflicts of interest in this work.
References
- KaoHSRChinese Calligraphy TherapyHong KongHong Kong University Press2000
- XuMKaoHSZhangMLamSPWangWCognitive-neural effects of brush writing of Chinese characters: cortical excitation of theta rhythmEvid Based Complement Alternat Med2013201397519023533532
- KaoHSRChenCCChangTMThe effect of calligraphy practice on character recognition reaction time among children with ADHD disorderRothRPsychologists Facing the Challenge of a Global Culture with Human Rights and Mental HealthPresented at the 55th Annual Convention of the Council of PsychologistsGraz, AustriaJuly 14–18, 1997
- KaoHSRChinese calligraphy handwriting for health and rehabilitation of the elderlyPresented at the Second World Congress of the International Society of Physical and Rehabilitation MedicinePrague, Czech RepublicMay 18–22, 2003
- KaoHSRGaoDWangMBrush handwriting treatment of cognitive deficiencies in Alzheimer’s disease patientsNeurobiol Aging200021Suppl 114
- KaoHSRGaoDWangMCheungHYChiuJChinese calligraphic handwriting: treatment of cognitive deficiencies of Alzheimer’s disease patientsAlzheimer’s Reports20003281287
- KwokTCBaXKaoHSLiJCHoFKCognitive effects of calligraphy therapy for older people: a randomized controlled trial in Hong KongClin Interv Aging2011626927322087066
- KaoHSRCalligraphy therapy: a complementary approach to psychotherapyAsia Pacific Journal of Counselling and Psychotherapy201015566
- YangXLLiHHHongMHKaoHSThe effectiveness of calligraphy practice and relaxation training in Chinese nasopharyngeal carcinoma patients: a randomized controlled trialInt J Nurs Stud20104755055919945106
- BohlmeijerEPrengerRTaalECuijpersPThe effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: a meta-analysisJ Psychosom Res20106853954420488270
- SchureMBChristopherJChristopherSMind-body medicine and the art of self-care: teaching mindfulness to counseling students through yoga, meditation, and qigongJ Couns Dev2008864756
- GrantJARainvillePPain sensitivity and analgesic effects of mindful states in Zen meditators: a cross-sectional studyPsychosomatic Medicine200971106114 Available from: http://www. psychosomaticmedicine.org/content/71/1/106.shortAccessed December 3, 201319073756
- DavidsonRJKabat-ZinnJAlterations in brain and immune function produced by mindfulness meditation: three caveats. (Response)Psychosom Med200466149152
- AustinJHZen and the Brain: Toward an Understanding of Meditation and ConsciousnessLondon, UKMassachusetts Institute of Technology Press1998
- Orme-JohnsonDWZimmermanEHawkinsMMaharashi’s vedic psychology: the science of the Cosmic psycheKaoHSRSinhaDAsian Perspectives on PsychologyNew Delhi, IndiaSage Publications Inc1997
- OttMJMindfulness meditation: a path of transformation and healingJ Psychosoc Nurs Ment Health Serv200442222915295915
- TannerMATravisFGaylord-KingCHaagaDAGrosswaldSSchneiderRHThe effects of the transcendental meditation program on mindfulnessJ Clin Psychol20096557458919241401
- BrennerMJHomonoffEZen and clinical social work: a spiritual approach to practiceFam Soc200485261269
- Wenk-SormazHMeditation can reduce habitual respondingAltern Ther Health Med200511425815819448
- MooreAMalinowskiPMeditation, mindfulness and cognitive flexibilityConscious Cogn20091817618619181542
- CompasBEConnor-SmithJKSaltzmanHThomsenAHWadsworthMECoping with stress during childhood and adolescence: problems, progress, and potential in theory and researchPsychol Bull20011278712711271757
- DeLongisAFolkmanSLazarusRSThe impact of daily stress on health and mood: psychological and social resources as mediatorsJ Pers Soc Psychol1988544864953361420
- ReicheEMNunesSOMorimotoHKStress, depression, the immune system, and cancerLancet Oncol2004561762515465465
- SegerstromSCMillerGEPsychological stress and the human immune system: a meta-analytic study of 30 years of inquiryPsychol Bull200413060163015250815
- GoldbergDPHillierVFA scaled version of the General Health QuestionnairePsychol Med19799139145424481
- ChanDWThe Chinese version of the General Health Questionnaire: does language make a differencePsychol Med1985151471553991829
- ChanDWChanTSReliability, validity and the structure of the General Health Questionnaire in a Chinese contextPsychol Med1983133633716878523
- ShekDTReliability and factorial structure of the Chinese version of the General Health QuestionnaireJ Clin Psychol1987436836913693557
- ShekDTValidity of the Chinese version of the General Health QuestionnaireJ Clin Psychol1989458908972613898
- ShekDTTsangSKReliability and factor structure of the Chinese GHQ-30 for parents with preschool mentally handicapped childrenJ Clin Psychol1995512272347797646
- GuoNFKaoHSRLiuXCalligraphy, hypertension and the type-A personalityAnn Behav Med200223S159
- KaoHSRShufa: Chinese calligraphic handwriting (CCH) for health and behavioural therapyInt J Psychol200641282286 Available from: http://www.tandfonline.com/doi/abs/10.1080/00207590544000059#. Upc3LEmS3IUAccessed December 3, 2013
- DuncanACArt therapy with patients who have early-stage Alzheimer’s disease and mild cognitive impairmentArt Therapy and Health Care2012266
- TeasdaleJDSegalZVWilliamsJMRidgewayVASoulsbyJMLauMAPrevention of relapse/recurrence in major depression by mindfulness-based cognitive therapyJ Consult Clin Psychol20006861562310965637
- Kabat-ZinnJWherever you go, there you are: Mindfulness Meditation in Everyday LifeNew York, NYHyperion1994
- Kabat-ZinnJMindfulness-based interventions in context: past, present, and futureClinical Psychology: Science and Practice200310144156
- Kabat-ZinnJLipworthLBurneyRThe clinical use of mindfulness meditation for the self-regulation of chronic painJ Behav Med198581631903897551
- FeldmanGGreesonJSenvilleJDifferential effects of mindful breathing, progressive muscle relaxation, and loving-kindness meditation on decentering and negative reactions to repetitive thoughtsBehav Res Ther2010481002101120633873
- FrewenPEvansEMarajNDozoisDPartridgeKLetting go: mindfulness and negative automatic thinkingCognit Ther Res200832758774
- EdenfieldTMSaeedSAAn update on mindfulness meditation as a self-help treatment for anxiety and depressionPsychol Res Behav Manag2012513114123175619