Abstract
Patient-centered care may be pivotal in improving health outcomes for patients with asthma. In addition to increased attention in both research and clinical forums, recent legislation also highlights the importance of patient-centered outcomes research in the Patient Protection and Affordable Care Act. However, whether patient-centered care has been shown to improve outcomes for this population is unclear. To answer this question, we performed a systematic review of the literature that aimed to define current patient-focused management issues, characterize important patient-defined outcomes in asthma control, and identify current and emerging treatments related to patient outcomes and perspectives. We used a parallel search strategy via Medline®, Cochrane Central Register of Controlled Trials, CINAHL® (Cumulative Index to Nursing and Allied Health Literature), and PsycINFO®, complemented with a reference review of key articles that resulted in a total of 133 articles; 58 were interventions that evaluated the effect on patient-centered outcomes, and 75 were descriptive studies. The majority of intervention studies demonstrated improved patient outcomes (44; “positive” results); none showed true harm (0; “negative”); and the remainder were equivocal (14; “neutral”). Key themes emerged relating to patients’ desires for asthma knowledge, preferences for tailored management plans, and simplification of treatment regimens. We also found discordance between physicians and patients regarding patients’ needs, beliefs, and expectations about asthma. Although some studies show promise regarding the benefits of patient-focused care, these methods require additional study on feasibility and strategies for implementation in real world settings. Further, it is imperative that future studies must be, themselves, patient-centered (eg, pragmatic comparative effectiveness studies) and applicable to a variety of patient populations and settings. Despite the need for further research, enough evidence exists that supports incorporating a patient-centered approach to asthma management, in order to achieve improved outcomes and patient health.
Introduction
Asthma is a complex disease entity. Treatment and research efforts often focus on understanding its immunologic and pathophysiologic processes. However, managing asthma presents clinicians with therapeutic challenges beyond this microbiologic level, and involves collaboration among clinicians and patients. In 2006, Irwin and Richardson, reviewed the benefits and barriers to the implementation of patient-centered care and defined patient-focused care as merging patient education, self-care and evidence-based models of medical practice. They further stated the need to introduce more equality into the physician/patient relationship and to focus as vigorously on patients’ knowledge, understanding and participation as we do on understanding the disease itself.Citation1,Citation2 They identified four intervention areas: communication, partnerships, health promotion, and physical care, achieved using the “three Cs: communication, continuity of care, and concordance”Citation1 all of which incorporate a complex interplay of psychological and behavioral characteristics.Citation1–Citation9
Patient-centered care has been demonstrated to improve care for patients with chronic disease such as diabetes and even chronic obstructive pulmonary disease (COPD). Bodenheimer et al discusses the chronic care model’s effect on chronic disease management using diabetes as an example in his 2002 meta-analysis of 39 interventional studies. He found that 32 of the 39 studies found at least one outcome or process measure improved and two-thirds of the articles additionally showed a reduction in overall costs.Citation10 The chronic care model embraces patient-centered care through the use of a comprehensive patient-centered medical home that considers the many barriers to access and successful execution of a care plan. In 2007, the American Academy of Family Physicians (AAFP), American College of Physicians (ACP), American Academy of Pediatrics (AAP), and Alpha Omega Alpha (AOA) all prioritized this concept of a patient-centered medical home.Citation11 In addition, many studies have reviewed specific approaches for intervention in diabetes self-management via educational programs.Citation12 For COPD, Adams et al performed a systematic review of the chronic care model and found that utilizing two components of this approach helped reduce hospitalizations and emergency department (ED) visits.Citation13
Although asthma was represented to a smaller extent in some of these studies,Citation10 the question remains whether the patient-centered care concept, which provides a major component of the chronic care model, actually translates to improvement in asthma outcomes. Research to this point does not appear to sufficiently address patient-centered management therapies and techniques, nor are the research designs themselves adequately patient-focused. The increased attention to patient-centered care comes not only from clinicians, but also researchers and even in legislative efforts, as patient-centered outcomes are recognized as a priority in the Patient Protection and Affordable Care Act 2010.Citation14 To obtain increased resources for clinical, research, and policy efforts to improve patient-centered care for patients with asthma, it is imperative to critically review the existing literature for this patient population to determine what, if any, patient-focused outcomes are improved utilizing this approach. Thus, the objective of our systematic review is to assess the patient-centered approach to the treatment of asthma and to determine whether patient-focused care improves asthma outcomes.
Material and methods
We focused our review using the Medline® search strategy as our primary search engine and then complemented these findings with parallel searches as detailed below. In addition, we limited our review to adults and adolescents, as the care of children largely incorporates the beliefs and actions of the adult caregiver. The Medline search (1950–2010) included MeSH (Medical Subject Headings) terms in conjunction with “asthma”: “patient perspectives”, “patient satisfaction”, “patient perception/patient goals”, “patient centered care”, “quality of life”, “outcomes”, “management” and “self-management”, limited to “human studies” and “English language”, and resulted in 2051 articles. Three independent readers (NQ, AP, VP) performed title and abstract reviews based on exclusion criteria (caregivers, children, asthma camps, asthma action plans, validations of questionnaires, editorials, studies involving small groups lacking easy generalizability, diseases other than asthma) and inclusion criteria (asthma, patient-centered care, adults, adolescents, English language). We also searched CINHAL® (Cumulative Index to Nursing and Allied Health Literature), PsycINFO®, and The Cochrane Central Register of Controlled Trials (2007–2011) databases, utilizing a parallel search strategy and a reference review of key included articles. We first performed a title and abstract review meeting key criteria, resulting in 945 total studies to be retrieved and assessed for final inclusion.
Studies included under these criteria were further subdivided to determine whether the study was primarily descriptive or intervention based. For those that were interventional studies, we extracted them to assess whether patient-focused results improved (“positive”), were equivocal (“neutral”), or did not improve (“negative”). For articles that included a combination of positive, neutral, and negative results, we characterized the article based on their stated primary outcome. If the primary outcome was unclear (as was the case in three articles), we brought them to a committee review and made a group decision on how the article in question should be classified. In the following sections we present the results of this literature review.
Results
Ultimately, 133 studies met all inclusion and no exclusion criteria. Over half were descriptive (75), and the remaining studies were interventional (58:44 positive, 14 neutral, 0 negative) (). The findings from our review are described below and are structured around the themes that arose. We provide a summary of these findings in relationship to these themes in .
Figure 1 Themes of results regarding efforts to improve outcomes through patient-focused care in the management of asthma.
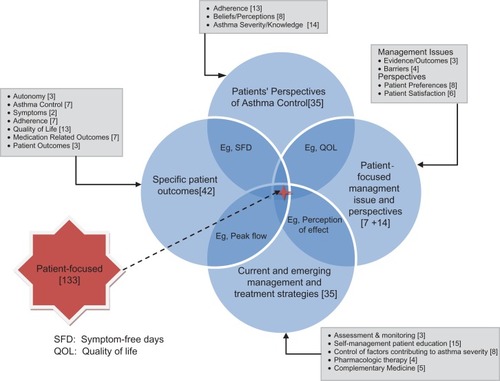
Table 1 Interventional studies
Patient-focused management issues in the treatment of asthma
The first major theme involves issues with implementation of patient-focused care. Most of the studies that focused on this theme were descriptive (6), though the one intervention study favored patient-centered care.
Evidence and outcomes for patient-focused care of asthma
There is some evidence to support that providers employing the patient-centered approach in the management of asthma improve patients’ perspectives of asthma control. Patient preferences for clinical encounters in disease states other than asthma were ascertained from patients through a questionnaire distributed in a pre-operative waiting room, which yielded an impressive 95% return rate, in a study designed by Little et al.Citation15 They discovered key aspects to care, including communication, partnership, and health promotion. Similarly, FlockeCitation16 identified four approaches to physician consultation interactions in his study in a primary-care practice in Northeastern Ohio: person-focused, bio-psychosocial, biomedical, and high physician control, and compared them with patient-evaluated quality attributes. With respect to patients with asthma, the patient-centered approach has been found to not only be something of interest to patients, but something patients are willing to pay for. Barner et alCitation8 looked into how much time and money patients are willing to put into an educational program to have their asthma control improved. They found that when patients were presented with a scenario of an 8-week asthma educational program, they were willing to spend a mean of 5.8 hours a week and $29.50 or more if they perceived a self-management program to be beneficial. Further, the patient-centered approach has been found to improve patient satisfaction, symptom burden, and outcomes even for difficult-to-treat patients and adolescents.Citation1,Citation17 Villanueva et alCitation17 highlighted an intervention using a comprehensive asthma center and found that although initial costs increased, the long-term health benefits and cost savings made it worth it.
Barriers to patient-centered approaches
When studied, patients can provide insight into barriers interfering with the completion of their treatment plan. These barriers include discordance between patients and physicians on patients’ needs versus physicians’ underestimation of the patient’s desire for disease-specific knowledge.Citation3,Citation18 For instance, among patients with pulmonary diseases, information needs are not adequately met by physicians in the form of verbal and written information regarding diagnostics, cause of illness, prognosis, and use of long-term medication.Citation19 White and SanderCitation20 confirm this concept when looking at asthma severity, treatment, and medication side-effects. The authors found that although a majority (73%) of respondents mentioned side-effects of beta-agonists to their physicians, most were told this was to be expected. Because of this, a third (33%) of adults reduced their bronchodilator dose or frequency to avoid side-effects, and a quarter (24%) skipped doses without physician instruction.
Poor patient–clinician communication is independently associated with poor adherence.Citation21 Barry et al studied “patient agendas”, an approach that allows for patients to express their feelings and opinionsCitation22 and discovered unvoiced concerns regarding psychosocial stressors and omission of key biomedical information that resulted in unwanted prescriptions and nonadherence. Newcomb et alCitation23 identified patient barriers to successful asthma management, including a lack of communication from physicians in regards to daily asthma management (31%) and home management of asthma (24%). However, one-third of clinicians report they assist patients in decision-making (30%) and tailor medication schedules around patient routines (33%). Physicians do not recognize this breakdown in communication, compounding the problem further.Citation24 Despite this, patients with asthma seek continuity-of-care and guidance from their physicians, more so than other groups of patients.Citation25
Adolescents’ views of specific barriers differ compared to adults. Adolescence represents a transition to adulthood,Citation26 and asthma complicates this transition.Citation27,Citation28 Psychosocial factors such as anxiety, depression, risk-taking behaviors, and family dysfunction, can complicate asthma control.Citation29 In a cross-sectional study by Rhee, adolescents with asthma cited barriers such as negativity toward providers and medication regimens, cognitive difficulties, peer/family influences, and denial.Citation6 Those with increased knowledge and self-efficacy experience less barriers, suggesting that psychosocial factors may be even stronger predictors of self-management obstacles in adolescents versus adults.
Characterizing specific and important outcomes in patients’ perspectives of asthma control
As seen previously, patients seek an active role and identify barriers to their care. The second theme that arose was quantifying how patients’ perceptions impact asthma control, by looking at patterns of adherence and belief systems. Again, this theme was mostly addressed by descriptive studies (28); though intervention studies found important outcomes with the use of tailored self-management educational programs in patients’ perspectives of asthma control, adherence, and beliefs (5:3 positive, 0 neutral, 2 negative).
Adherence and age, personality, and socioeconomic status
Investigating adherence patterns offers insight into patients’ perspectives.Citation30 Beginning with adolescence, decisions influencing adherenceCitation31,Citation32 are often directly related to perceived vulnerability.Citation33–Citation36 Slack and Brooks,Citation37 found that despite positive attitudes toward taking medication for asthma (P < 0.01) and considering themselves compliant (P < 0.05), adolescents rarely discuss medications with pharmacists, and many wanted more control and additional information.Citation38 Similarly, Buston and WoodCitation39 showed only 8% of the adolescents interviewed reported compliance, with the remaining stating that at least one aspect of their treatment plan was forgotten or ignored most of the time.Citation39
Adherence to asthma management plans for older adults adds complexity.Citation40 Studies have largely excluded this population; additionally Goeman et al acknowledged diagnosing asthma in older adults poses a problem when symptoms are attributed to comorbidities.Citation41 Unclear side-effect profiles (eg, long-acting beta2-agonists), psychosocial factors, costs of medication, and physical limitations all contribute to nonadherence in older adults. Simplification of medication regimens, clearly communicated instructions, with motivational incentives and actively involving patients, may improve adherence to asthma management plans. However, more studies are needed to see whether these interventions would affect adherence and health outcomes.
Additionally, personality traits may relate to adherence. Axelsson et al described the unintentional aspects of personality on adherence and found a significant relationship with negative affectivity and impulsivity on personality testCitation42 and poor asthma control in both men and women.Citation7 While the day-to-day applicability of this is unclear, personality traits further influence the need for individually tailored therapy plans.Citation43 Furthermore, several studies have shown patients who are anxious and depressed have worse asthma controlCitation5 and quality of life,Citation9 in addition to the psychological stressors that impact patients with asthma.Citation4
Beyond factors such as age and personality, Apter et alCitation21 aimed to identify specific factors that influence asthma severity by studying adherence to twice-daily inhaled corticosteroids (ICSs) and administered surveys to assess patients’ understanding and monitoring of their disease. Their study, in fact, demonstrated harm to the patient as adherence to ICSs decreased. Certain factors were associated with decreased adherence such as: less than 12 years of formal education (P < 0.001), poor patient–clinician communication (P < 0.001), household income less than $20,000 (P = 0.002), Spanish as primary language (P = 0.005), and minority status (P = 0.007).
Beliefs and perceptions
Patients’ attitudes toward their disease may influence when and where they seek care. There is ample evidence that many individuals solely seek acute care rather than primary care.Citation44,Citation45 Haire-Joshu et al investigated attitudes and knowledge of low-income, African-American adults in an acute-care setting versus an outpatient private specialty clinic. They found the low-income group encountered daily stressors (such as transportation, finances, crime, and occupation) more frequently, and acute-care patients disagreed with the need for routine physician care (21 versus 2% of private-care patients, P = 0.001). They tended to try to “fight asthma attacks” themselves “rather than getting medical help”, (75% versus 49%, P = 0.01) and subsequently delayed seeking care (58% versus 43%).Citation46 Haire-Joshu et al states that “patient perceptions are important barometers of likely patient action”. Likewise, SibbaldCitation47 found that asthmatics with greatest morbidity delayed appropriate response to symptoms and that 25% expressed strong feelings of stigma and pessimism.
Loignon et alCitation48 recognized that patients adapted three different self-care strategies (controlling symptoms, preventing symptoms, or tolerating symptoms), and social factors contribute to which strategy is employed. Putting this idea into action, van der Palen et alCitation49 found that self-management programs influence positive behavioral changes in patients with asthma by randomizing them to an active control group versus a self-treatment group. All patients received self-management training, but the intervention group learned techniques for self-treatment. They found that only the self-treatment group showed improvements in self-efficacy, social support, self-treatment and self-management behavior. Identifying how patients’ cope with asthma may help clinicians understand how to focus visits.
Adolescent attitudes also lend insight into medication usage patterns. A survey of inner-city high school students evaluated the influence of psychosocial factors on management capabilities: 70% felt in control of their asthma symptoms, and 63% had feelings of anxiety.Citation50 Those who felt in control of their asthma were more likely to carry their asthma inhaler with them (r = 72, P = 0.004). Conversely, those who were embarrassed about their asthma were significantly less likely to do this (r = 0.98, P < 0.001), and only 39% admitted having asthma to friends. Psychosocial factors can either promote or limit self-management strategies, as adolescents that reported feelings of control over asthma symptoms had more positive attitudes toward self-treatment.Citation50 A video intervention assessment (VIA) used in adolescents can reveal physical and psychosocial environments and educate clinicians about day-to-day realities of patients.Citation51,Citation52
Asthma severity and knowledge
Patients differ in expectations of asthma management and views of asthma severity when compared with clinicians.Citation27,Citation53,Citation54 In a survey of adults with persistent asthma, perceptions of asthma severity and its impact on daily activities found suboptimal control in two-thirds (67%) and daily symptoms in a quarter (25%) of patients. However, daily symptoms did not correlate with reported asthma severity; 37% of patients with daily symptoms reported their severity as “mild”. This disparity was also seen in descriptions of asthma exacerbations; physicians described exacerbations in terms of signs and symptoms, while patients focus on inability to perform activities. Finally, almost half (45%) of patients did not agree with their doctors’ instructions to start controller treatment, indicating that patients’ minimize their disease severity.Citation55 In another study, patients’ perceptions of their ability to influence their asthma symptoms (eg, internal locus of control) related to their level of asthma control.Citation56 Choi et al showed that beliefs about disease severity influence asthma medication adherenceCitation57 and found that beliefs did not differ based on asthma severity or current therapy. Recognizing what patients dislike about their medications gives the physician the opportunity for education as well as intervention to adopt a more inclusive approach when discussing asthma treatment plans. By addressing goals and expectations of asthma management, doctors and patients are more likely to accomplish improved control of asthma.
Further, descriptive studies find the belief that asthma is a periodic instead of a chronic disease infiltrates asthma self-care, but specific interventions focusing on reversing this myth are lacking. One simple question asked by Halm et alCitation58 “Do you think you have asthma all of the time, or only when you are having symptoms?”, discovered that half (53%) believed they only had asthma when they were having symptoms. This belief was associated with a one-third decrease in adherence to ICSs when asymptomatic (P < 0.02). This dilemma was echoed by Jones et al study in correlating this belief with poor access to primary care services.Citation59 The psychological burden of near-fatal asthma,Citation60 along with this dichotomy between symptomatic and preventative treatment of asthma,Citation61,Citation62 leads to poor understanding of disease and lack of ability to perceive severity.Citation63 Kendrick et alCitation63 investigated 255 patients with asthma from a general practice disease registry in Bristol to see if their perceived view of asthma severity matched peak expiratory flow measurements. Sixty percent of patients were unable to assess their level of asthma control accurately (P > 0.05), but the authors also state that although similar findings were previously noted, most were in controlled environments which likely differ from real-life situations. Adherence, whether the provider realizes this or not, is often negatively affected by the patients’ perceptions of their symptoms and disease severity.Citation64,Citation65 Whether concentrating educational efforts combating this view specifically affect patient outcomes needs to be further investigated.
While most patients value their health care providers’ role in decision-making about asthma treatment plans, including patients in treatment decisions is crucial.Citation66 Patients desire a larger role, especially when respondents had better insight than clinicians into their own cost barriers and psychosocial factors. Ratcliffe’s descriptive study found that all patients wanted their opinions regarding costs related to the visit and how they perceived their symptoms to be heard by their clinicians.Citation67 Also, direct patient feedback on corticosteroid use with a physician helps adherence and improves understanding of reasoning why patients stop medications,Citation68 providing a framework to tailor specific asthma educational interventions and action plans.Citation58 De Vries et alCitation69 used a multi-center study to investigate the different variants of an asthma educational program in adults with asthma to see whether patient satisfaction differed with various approaches. They discovered that as the intensity of the educational intervention increased, so did the satisfaction. It becomes clear that patient satisfaction and perspective should be addressed when formulating an asthma treatment plan, and that this needs to occur in conjunction with, instead of “for” the patient. More studies will be needed in order to see whether this approach translates into improved patient health outcomes, more than just satisfaction, but collaboration appears to be key in creating coordinated, reliable, and feasible self-management strategies that not only coincide with asthma guidelines but function in the context of patients’ lives.
Overview on the current and emerging treatment options for management of asthma
In this section, we highlight the third theme and provide an overview of current asthma treatment options as described in national and international clinical guidelines and systematic reviews. We also present emerging treatment options with an emphasis on patient-centered care. Of the 35 studies, most were intervention studies (31), of which most had favorable findings (21 positive and 10 equivocal). Studies ranged from 2007–2011 (since guidelines are current through March 2006).
Expert guidelines
The National Asthma Education and Prevention Program (NAEPP) of the National Heart Lung Blood Institute (NHLBI) aims to “help health care professionals bridge the gap between current knowledge and practice” by convening expert panels to prepare national guidelines (expert panel report, [EPR]) for the diagnosis and management of asthma.Citation70 They published three reports, the first in 1991 (EPR 1991)Citation71 and most recently in 2007 (EPR-3).Citation72 This report identified four components of asthma management: assessment and monitoring; patient education; control of factors that may contribute to asthma; and pharmacologic therapy.Citation72 Similarly, the Global Initiative for Asthma (GINA) formed in 1993 to disseminate up-to-date information about asthma care, published their first report in 1995.Citation73 The most recent 2006 guidelines emphasize the importance of a partnership between patient and caregiver in self-management.Citation74
Reviews of asthma management
Several systematic reviews have evaluated asthma self-management. In our search, we found four reviews in the last decade. Two reviewed management strategies,Citation75,Citation76 one evaluated patient-centered approaches,Citation77 and the fourth summarized pharmacological strategies for self-management of asthma exacerbations.Citation78 When searching for evidence of the four components of asthma management (EPR-3), all four addressed pharmacologic therapies, all but one addressed patient education, but none presented data on assessment and monitoring. Current and emerging therapies highlighted in these reviews are summarized in .
Table 2 Summary of current and emerging treatments by systematic reviews (2001–2006)
Current and emerging patient-focused treatment options for asthma
In this section, we review clinical guidelines and more recent studies updated since their publication, that address patient-focused management of asthma.
Assessment and monitoring
Guidelines recommend regular (≥twice yearly) review of asthma management. The EPR-3 guidelines emphasize elements of assessment and monitoring such as “severity, control and responsiveness to treatment”. Standard assessment tools include focused histories and measurements of lung function, such as the examples provided here (Text Box 1).
Because there are multiple barriers to patients receiving regular review of their asthma, patient-centered approaches that decrease these barriers are needed. One novel approach looked at the effectiveness of routine asthma telephone check-ins and showed 26% more asthma patients’ care was reviewed in a practical and cost-effective manner.Citation79 Another implemented a computer-generated reminder system to convey education that would encourage self-care.Citation80 An additional example used an internet program for weekly input by patients, with monitoring and treatment-adjustments by an asthma nurse-specialist. This tailored approach improved asthma control and adherence for the intervention group (P < 0.001 and P = 0.001 respectively).Citation81
Self-management patient education
High-level evidence exists to support the need to provide asthma self-management education to ensure patients have skills necessary to control their asthma.Citation72 This education requires repetition and reinforcement, and the most recent guidelines increased emphasis on written asthma action plans and awareness of cultural and health literacy factors in the delivery of asthma self-management education,Citation72,Citation73 such as the items listed here (Text Box 2). Smith et alCitation82 noted that until recently, research on asthma education primarily focused on behavior change. They emphasize individual-centered rather than educator-centered education and suggest first identifying and acknowledging patients’ individual concerns.Citation71
Focused history
○ Symptoms
○ Quality of life
Medication review
○ Adherence
○ Side effects
○ Inhaler technique
Lung function (spirometry)
○ Peak flow
○ FEV1
○ Airway responsiveness
○ FeNO
Management programs for asthma may improve patient outcomes while reducing care costs; however, not all are equally effective. Reviews found that the highest level of evidence for success were found with self-monitoring tools (eg, symptom or peak-flow based) coupled with written action plans.Citation72,Citation73,Citation83 Newer studies continue to evaluate novel features of various self-management programs. For instance, patient-centered care is now recognized as important in providing high-quality care. Smith et alCitation84 performed a randomized trial evaluating a patient-centered versus standard patient education (SPE) and found subgroups in the intervention group benefited significantly more than the control group. Although this requires further study, patient-centered education may help subpopulations with asthma. Huang et alCitation85 evaluated an individualized program for older adults with asthma, and found that indicators of asthma control improved. Tousman et alCitation86 developed a “learner-centered” program that utilized homework assignments with “individual status reports” in weekly small group meetings; participants improved in knowledge, quality of life (QOL), and behavior change. Finally, Nokela et alCitation87 investigated the use of structured information along with monitoring (asthma diary). Asthma control improved significantly in the intervention group, indicating that a simple patient-driven tool may improve patient outcomes.
Patient education can also occur outside the physician’s office. Community settings, including home-based education as studied by Peeble and Hartert et alCitation77 who evaluated the use of respiratory therapists in a home management program, is one example. Also, school-based education programs are frequently used for children; however, Bruzzese et alCitation89 noted a paucity of interventions for adolescents with asthma, especially those aged 11–14. They found in their randomized school-based trial that the intervention group had decreased night-time symptoms and improved self-care behaviors. Pharmacists are another way to reach patients outside health care encounters. Mehuys et alCitation90 evaluated community pharmacist-led educational interventions and found that they improved adherence and technique with controller medications. One studyCitation91 strove to improve self-efficacy for African-American adults with asthma through a community-based intervention with social workers, involving home visits (versus receiving education via mail), and found the intervention group improved self-efficacy, QOL, and coping.
Another important patient-centered issue related to patient education is the concept of health literacy (ability to understand and participate in one’s health management). Patients with poor health literacy are at greater risk of worse health outcomes and increased hospitalizations,Citation92 and for patients with asthma, this can lead to lack of medication knowledge and inhaler technique.Citation93 Written educational materials and self-management tools may themselves be barriers; therefore, use of communication technology, such as web-based technologyCitation94–Citation96 and multi-media toolsCitation93 may be useful in improving knowledge and self-management skills. Cruz-Correia et alCitation94 found that web-based intervention was feasible, safe, and preferred over paper-based formats. Van der Meer et alCitation95,Citation96 found patients randomized to an internet-based self-management plus educational intervention versus usual care improved lung function and asthma control, even though exacerbations were unchanged. In African-American patients with low literacy, Sobel et alCitation97 found that a multimedia tool significantly improved participants’ understanding of asthma, although at higher rates for patients with marginal and adequate literacy versus those with low literacy.
When tailoring self-management education, adolescents may be particularly amenable to technology. One study employed a web-based program targeting urban African-American high-school students and found that their tailored approach was not only economical and feasible, but also improved asthma outcomes.Citation98 Another used MP3 players to increase knowledge for inner-city African-American adolescents, and found that asthma knowledge improved in those randomized to the intervention group versus control.Citation99 Finally, van der Meer et al’s internet-based self-management strategy found that adolescents with poor asthma control were more able to incorporate asthma self-management through an internet-based program for a long period of time, while those with good control were not.Citation95 This strategy may be particularly useful for this high-risk group of adolescents.
Control of factors contributing to asthma severity
Despite insufficient evidence that environmental strategies prevent the development of asthma, the guidelines recommend testing for exposure and sensitivity to allergens as well as reduction of allergen and respiratory irritant exposure for management of existing asthma, a brief summary is provided (Text Box 3). Studies continue to evaluate ways to minimize environmental and other triggers. Van den Bemt et alCitation100 evaluated the use of dust mite impermeable covers, but did not find improved health-related quality of life (HRQOL) for adults with asthma. In another study, Brodtkorb et alCitation101 evaluated the use of laminar airflow during sleep in adolescents with allergic asthma and found that it may add quality-adjusted life-years at a reasonable cost, but further work needs to be done to understand the full potential of this therapy.
Although asthma treatment is the subject of the next section, it is important to highlight that there are some pharmacologic therapies that are being studied to aid in decreasing effect of factors affecting severity of asthma, therefore they will be included here. In one study by Keith et alCitation102 montelukast was found to be effective as an add-on therapy for patients with dual diagnoses of asthma and allergic rhinitis, uncontrolled on ICSs or ICSs + long-acting beta-agonist (LABA) regimen(s), while another study found improvements in lung function and QOL without modification of effects by decreasing airway inflammation.Citation103 Voltolini et alCitation104 studied sublingual immunotherapy for dual-diagnosed patients, and found promising results in the ability to step down asthma therapy (77% versus 0%, P = 0.05). Van Rensen et alCitation105 found the benefits of omalizumab (anti-IgE) in asthma may be due to a decrease in eosinophilic inflammation. Miller et alCitation106 then compared the ability to sleep, work, and participate in activities among patients with IgE-mediated (allergic) asthma. They received salmeterol/fluticasone combination with or without omalizumab, and found the omalizumab group was more than twice as likely to have controlled asthma (odds ratio 2.62; P = 0.005). These findings support the use of omalizumab as adjunctive therapy for patients with IgE-mediated (allergic) asthma and who have severe persistent asthma. Riscili et al,Citation107 however, did not find empiric treatment of “silent” reflux helpful.
Evaluate for allergen exposures
Test for sensitivity to allergens
Reduce exposure to allergens
Avoid exposure to respiratory irritants (eg tobacco smoke)
Consider allergen immunotherapy for certain individuals
Evaluate for co-morbid conditions that may interfere with asthma control
○ Gastroesophageal reflux disease (GERD)
○ Obesity
○ Rhinitis
Pharmacologic therapy
The guidelines provide up-to-date pharmacologic therapy recommendations, such as those listed here (Text Box 4). This section, therefore, will focus on patient-centered approaches to therapeutic advances, including use of respiratory inhalers and complementary and alternative medicine (CAM).
Respiratory inhalers
Because most asthma medications are delivered by respiratory inhaler devices, adherence to therapeutic regimens is complex, beyond the usual adherence challenges of motivation. Even with good intentions, if patients misuse inhalers, they may not receive an adequate dose, unknowingly decreasing adherence. Numerous studies evaluate ability of patients to use inhalers and their preferences and several novel educational strategies aimed to improve skills related to use of medications. Ulrik et alCitation108 evaluated the use of asthma compliance enhancement training with the use of combination salmeterol/fluticasone propionate. This technique did not increase the likelihood of “total control”. Another study utilized reminder labels applied directly to inhaler devices to remind patients of inhaler technique after education by pharmacists; this improved technique and asthma outcomes.Citation109 One study evaluated an interactive voice response intervention to improve adherence, and found the intervention group adhered 32% more frequently (P = 0.003).Citation110 Paasche-Orlow et alCitation93 looked at whether health literacy affected patients’ abilities to learn and retain discharge instructions. Although baseline medication knowledge and metered-dose inhaler (MDI) technique were worse for patients with inadequate health literacy, patients were able to learn and retain tailored hospital-based education. Building on this work, Press et alCitation111 specifically evaluated a “teach-to-goal” strategy that utilized cycles of assessment and education of patients until they mastered the inhaler technique. By using these cycles of “teach-back” and education, 100% of patients, regardless of their level of health literacy, mastered the inhaler technique for both MDIs and Diskus devices, after at most two rounds of teaching.
Long-term control medications
○ Inhaled corticosteroids (i)
○ Systemic corticosteroids
○ Cromolyn Sodium/Nedocromil (ii)
○ Imunomodulators
○ Leukotriene Receptor Antagonists
○ 5-Lipoxygenase Inhibitor
○ Long-Acting Beta2-Agonists (LABA)
○ Methylxanthines
Quick-relief medications
○ Short Acting Beta-Agonists (SABA) (iii)
○ Ipratropium (iv)
○ Systemic Corticosteroids
Devices
○ Inhalers
▪ (A) Metered dose inhaler (i–iv)
▪ (B) Breathe actuated MDI (iii)
▪ (C) Dry powder inhaler (i, iii, iv)
○ Spacer/holding chamber (A)
○ Nebulizer(i–iv)
Complementary and alternative health
CAM is defined as “a group of diverse medical and health-care systems, practices, and products that are not generally considered to be part of conventional medicine” by the National Center for CAM.Citation112 A prior review by Slader et alCitation113 found a wide range of prevalence estimates (4%–79%) for CAM use among asthmatics; the most common use being breathing techniques, herbal products, homeopathy, and acupuncture. Use does not differ by race or ethnicity.Citation114 Slader’s review found that few studies have shown efficacy in asthma, and therefore conclusions are of limited use due to inadequate quality and small sample sizes.Citation113,Citation115–Citation121 At least one study reported adverse effects of use of herbal products for asthma management.Citation122 Thomas et al evaluated breathing exercises for asthma. While there was some signal that patient-centered outcomes such as QOL, nonpathophysiologic measures were improved, this technique is unlikely to reduce the need for pharmacologic therapies,Citation119 though one study found promising results.Citation120 The guidelines state that there is insufficient evidence to recommend/not recommend CAM, with two exceptions: acupuncture is contraindicated in the treatment of asthma (a recent study in 2010 also found no improvement in pulmonary function, though there was a “favorable effect” on QOL),Citation121 and certain herbal preparations are cautioned against for risk of potential harm secondary to either interactions with recommended asthma medications and/or they may be irritants. Most importantly, since up to half of patients do not report CAM use to their clinicians,Citation122 the guidelines recommend that clinicians specifically inquire about their patients’ use of CAM and advise against substituting CAM for their clinicians’ recommended treatment plan.
Identification and impact on specific patient outcomes
The following section expounds on studies specifying patient priorities in asthma care including autonomy, and how they affect asthma control, QOL, and patient outcomes. The fourth theme focused on patient-centered features of asthma management and resulted in 42 studies, half were descriptive (22), and half were interventions (20), with largely favorable results (16 positive, 3 equivocal, 1 negative).
Autonomy
Autonomy preferences vary among patients with asthma. Gibson et al examined decision-making and information seeking in relation to QOL.Citation123 Subjects recruited from pharmacies were compared with patients who were recently hospitalized for acute severe asthma. Both groups had QOL impairment, but this was greatest in the post-hospitalization group (P < 0.05), and as severity of the asthma exacerbation increased, the desire to make decisions decreased (P < 0.05). Although patients with asthma have strong preferences for joint decision-making, they do not want to be the sole decision-makers during an exacerbation. These findings are similar to those found in developing countries.Citation124 Further, Adams et alCitation125 also found that physicians’ participatory style relates to patients’ use of acute health visits and HRQL. Therefore, while autonomy is important when aiming for high self-efficacy, a balance between autonomy and the ability to use joint decision-making needs to be further explored.
Asthma control outcomes
Asthma control is considered the ultimate outcome for patients with asthma; patients’ perspectives and adherence are directly related to this outcome. Holt et alCitation126 describes that although the majority (93%) of patients studied had suboptimally controlled asthma, most (76%) felt their asthma was well controlled and were satisfied (80%) with their control.
It has already been established by previous studies that educational programs for asthma patients result in improved control of asthma.Citation127,Citation128 To study whether individualized asthma self-management improved markers of asthma control, Janson et alCitation129 performed a randomized control trial of individualized education with self-monitoring of symptoms and peak flow versus usual care. Patients in the self-management group maintained consistently higher ICS adherence levels, and had threefold greater odds of higher than 60% adherence. Thoonen et alCitation130 investigated whether self-management can provide a safe treatment strategy in general practice by randomizing patients to usual care (UC) or self-management (SM), and the SM group showed a mean of 78% successfully treated weeks per patient compared with 72% in the UC group (P = 0.003). Urek et alCitation131 studied the effect of different educational modalities in asthma control, QOL, and knowledge. Adults with moderate persistent asthma on ICSs received either individual verbal instructions (IVI), written information as an “asthma booklet” (B) or integrated asthma classes “asthma school” (AS). AS and IVI groups showed significantly greater improvement in QOL (P < 0.001) and asthma-related knowledge (P < 0.001) than the B group. The IVI, the most interactive group, produced the best response overall in both parameters of asthma control and QOL.Citation131 Similarly, Wilson et alCitation132 examined a shared decision-making model (SDM) and showed that mutual information sharing improved such factors as QOL.
Symptoms
One important measure of control is symptom burden. Clinical measures of outcome such as FEV1 (forced expiratory volume in 1 second) and peak flow rates tend to be associated with acute episodes of asthma. This concept led to the development of the “symptom free day” (SFD).Citation133 However, since SFD assigns equal weights to symptoms which may not be accurate, McKenzie et al used discrete choice methods to study symptom-based outcome measures by assessing preferences of those with moderate to severe asthma. They showed that patients weigh daytime cough and breathlessness higher than other symptoms. Future studies need to explore preference-based weights for asthma symptoms for improved accuracy of the SFD.Citation133 Perceptual accuracy and its relation to treatment adherence has not shown a positive correlation thus far, but respiratory function variability (peak flow variability) within individuals has been correlated with increased symptom perception accuracy.Citation134 A specific tool, like peak flow, that provides a consistent framework for both patients and physicians to measure symptom severity is necessary.
Adherence
Patient characteristics that influence adherence were addressed above. However, adherence is an important measure of asthma control and therefore this element will be addressed in this section. The effects of asthma education on promoting medication adherence were examined by Schaffer and TianCitation135 by randomly assigning patients to receive an experimental audiotape, a standard asthma-management booklet, both, or no intervention. Mean treatment adherence improved from 15% to 19% in the intervention groups and declined 22% in the control group over the course of 6 months, showing that education is a factor in adherence.
Many factors such as beliefs, attitudes, and experiences of patients influence adherence. Self-management necessitates some degree of active participation and motivation on behalf of the patient.Citation123 Ponieman et alCitation136 evaluated inner-city asthma patients’ beliefs about their ICSs and showed these beliefs influenced adherence, further postulating that addressing modifiable beliefs improves adherence. Asthma patients with a high preference for involvement and information had nonadherence to medication and had a higher interest in self-management.Citation137 A follow-up study found that the patients’ perceived burden of illness plays a more important role for education, self-management, and guideline adherence than the actual severity of the disease.Citation138
Other factors that affect adherence outcomes with medical regimens include knowledge, attitudes, and self-efficacy.Citation139 Menckeberg et al’s studyCitation140 reiterated what was discussed in the adherence section but are more specific to the medication-related outcomes. Patients’ perception of necessity and concerns about side-effects along with environmental factors further influence their attitudes and adherence. OsmanCitation141 discusses how attitudes are affected by friends, family, and media as well as patients’ personal experiences with medication characteristics. He proposes that “for most patients attitudes to medication will follow control of symptoms”. By focusing on improving patients’ control of symptoms and QOL, we will improve their attitude towards using medication.
Quality of life related outcomes
Psychosocial factors can also influence patient outcomes. Depressive symptoms and lower degrees of self-efficacy have been correlated with lower asthma-related QOL scores.Citation142–Citation146 Calfee et alCitation147 found that greater perceived control was associated with improved physical health status, better asthma-related QOL, fewer days of restricted activity, and lower asthma severity scores. And although these differences were not mediated by changes in asthma practices, there was a significantly decreased prospective risk of ED visits and hospitalizations for asthma which is in contrast to previous studiesCitation148,Citation149 showing changes as a result of self-management programs. This discrepancy could be linked to inaccurate perceptions of asthma control. Clark et alCitation7 also found that QOL improves in women with asthma when a tailored educational intervention for women was employed. Also, Lloyd et alCitation150 found that people with the worst HRQL were willing to pay the least to avoid symptoms and asthma attacks. Clearly, there is significant influence of psychosocial factors on patient outcomes.
The Asthma Quality of Life Questionnaire (AQLQ) is one method to identify the causes of distress when patients present with acute severe asthma. Adults presenting to the ED with acute severe bronchoconstriction had severe impairment in asthma-specific QOL at baseline, but improved after treatment (P < 0.00001). By utilizing tools such as AQLQ, physicians can gain insight into how distressing the experience is for patients, both from a symptomatic and emotional perspective, while identifying the degree and cause of the distress.Citation151
Medication-related outcomes
Current and emerging treatments were discussed above; however, patient outcomes related to use of these therapies will be summarized in this section. Objective measures of improved outcomes such as lung function are commonly used to assess the efficacy of medications. However, these changes may not reflect what patients value, therefore making patient-reported outcomes (PROs) vital to evaluating asthma therapies. Four articles compared PROs between dry powder and pressurized MDIs,Citation153–Citation157 and one discussed features of inhaler devices that patients prefer.Citation157 Positive correlation to compliance has also been shown with low daily frequency of medication administration.Citation154 Patient-reported outcomes addressed were: HRQLCitation155 or QOL,Citation139,Citation156 ability to sleep, work, and participate in leisurely activities,Citation117,Citation139 asthma control,Citation117,Citation139,Citation155,Citation156 patient satisfaction,Citation153–Citation157 patient preferences,Citation156 and onset of effect.Citation156 Chervinsky et al,Citation152 in a double-blind controlled study of adults with moderate-to-severe asthma, studied PROs on differing doses/combinations of budesonide and/or formoterol pMDI. They found that the group receiving combined budesonide/formoterol reported significantly greater improvements on the AQLQ(S) and asthma control variables (P < 0.001), improved Patient Satisfaction with Asthma Medication Questionnaire scores, and Physician-Patient Global Assessment. O’Connor et alCitation153 looked at the outcome of onset of effect in adjustable versus fixed doses of budesonide/formoterol compared with fluticasone/propionate/salmeterol and found a higher reported onset of effect in the budesonide/formoterol group. Finally, Price et alCitation157 evaluated salmeterol/fluticasone (stable-dose) versus formoterol/budesonide (adjustable maintenance dosing) and found that the former resulted in significant improvements, including increased symptom-free days, decreased rates of exacerbation, and better HRQL.
The question of quick onset of effect of maintenance therapy was addressed by Leidy et al.Citation158 They found 87% who perceived their inhaler working right away identified sensations of easier breathing, and propose if patients feel maintenance therapy works right away, this may provide positive reinforcement and improve adherence. Further studies on this topic are necessary, as perception may be one key to improving adherence. Tying all this together, a study by Schatz et alCitation159 looked at the ratio of controller medication to total asthma medication use and its relation to patient-centered outcomes in adult HMO members with persistent asthma. Patients with a ratio of ≥0.05 had mean asthma QOL, asthma control, and symptom severity scale scores that were significantly more favorable (P < 0.0001). The authors concluded that the study provided support for the use of the medication ratio as an asthma quality of care measure.Citation160
Patient outcomes
D’Souza et alCitation161 evaluated the long-term effectiveness of self-management plans with the adult “credit card”. There was a significant improvement in all but one asthma morbidity measure (>7 days out of action). The proportion of “waking most nights” in the previous 12 months decreased from 29% to 9% (P = 0.02), emergency visits to GPs decreased from 43% to16% (P = 0.001), ED visits decreased from 19% to 5% (P = 0.02), and hospital admissions decreased from 17% to 5% (P = 0.04). Similarly, Lemaigre et alCitation162 showed that even a shortened asthma self-management group program could produce effects on knowledge and asthma symptoms; however, these effects did not persist significantly after 3 months. Lastly, a guideline-based asthma management program within a managed care organization showed statistically significant improvements in patients’ HRQL, satisfaction, education, disease knowledge, and confidence in ability to manage their disease.Citation163
Patient-focused perspectives
In this section we review the final theme highlighting patient perspectives on asthma management plans and resulting patient satisfaction. Fourteen studies explored this theme, most (11) were descriptive; of the 3 intervention studies, the findings were mostly in favor of patient-centered care (2 positive, 1 equivocal, 0 negative).
Patient preferences
Ultimately, patient preferences are an important aspect of asthma management. Ulrik et alCitation164 asked patients to rank three treatment models according to preferences: 1) fixed daily-dosing of controller therapy; 2) fixed dosing of controller medication, with written plan outlining adjustment during worsening; 3) or daily-dosing of low-dose combination reliever/controller medication with this inhaler used as needed until control of symptoms occurred. The first model was preferred, and the distribution of preferences mirrored how patients already reported taking their medication. More than half of patients took less medication than prescribed when having fewer symptoms. There was no significant association between self-perceived severity of asthma and the response to therapy in case of exacerbation. These findings illustrate that patients’ strategies of management when encountering disease variability are not necessarily driven by their knowledge of disease but more by preferences towards specific strategies.Citation164
Another aspect of self-management involves increasing awareness of worsening of disease. Tools to identify patient responses to worsening of their asthma and the reasons for their particular responses need to be improved. While patients prefer monitoring symptoms to peak flow measurements (PFM), likely because of easeCitation161 (only 10%–16% of patients report use),Citation63,Citation165 neither method is perfect. Symptom monitoring lacks objectivity, while peak flow monitoring can be impractical at times. However, preferences for symptom monitoring, despite increased objectivity with PFMCitation166 demonstrates that ease of self-management and simplification of care regimens are patient preferencesCitation167 of which clinicians need to be aware. Preferences for both education content and modality have also been studied and reveal the Internet and telephone as a preferred means for communication with an information provider.Citation168
Incorporating patients’ preferences when it comes to treatment decisions has been shown to improve disease management.Citation169 McTaggart-Cowan et alCitation170 evaluated treatment preferences in terms of risk/benefit tradeoffs using discrete choice experiments and found the relative importance of six attributes of asthma therapy. Patients preferred a treatment regimen that resulted in more SFDs but were willing to forgo some of this benefit in exchange for a more convenient regimen. Furthermore, gender, age, asthma control, and high socioeconomic status were statistically significant predictors of maintaining current asthma therapy.Citation170 This provides useful information for physicians when designing management plans, as every patient has a unique risk–benefit ratio secondary to these factors.
Patient satisfaction
A tailored approach to management appears to be a key element to patient satisfaction. Studies have examined patient satisfaction from education provided in different settings.Citation67,Citation171 In another study performed by Thoonen et al,Citation172 patients in a tailored education group had patient satisfaction increase, whereas there was no change in usual care group. Providing patients with tools to evaluate and highlight their own needs and demands was associated with an increase in patient satisfaction. Little et alCitation169 found communication aimed at understanding the patients’ needs and fears is crucial to patient centeredness. To provide patients with asthma education that they perceive as being relevant to themselves, we have to make our educational interventions both accessible and in accordance to their needs. Preferences for different styles to asthma education according to extent of teaching and intensity showed a significant positive linear association between intensity of the education program and effect on asthma knowledge and HRQL.Citation69
This same idea can be applied to specific medication devices; this resulted in one study that examined patient preference for a dose-counter.Citation173 Although patients must keep track of doses to determine when to replace their MDIs,Citation173 63% do not realize that they are supposed to keep track of the number of actuations,Citation174 and 54% of patients do not know the number of actuations for their inhalers.Citation175 Patients use various inaccurate methods to determine MDI depletion,Citation176,Citation177 and may then provide “doses” that contain less therapeutic medication.Citation178 Patients using their MDIs past the recommended number of actuations compromise their disease control.Citation179 Sheth et alCitation173 found that 95% of patients were satisfied with the counter, 92% agreed that it would prevent them from running out of medication, 73% felt the MDI dose-counter would help improve control of their disease, and 92% felt added reassurance about medication supply. By focusing efforts on innovations that make the use of medications easier, the authors propose we can potentially improve efficacy of and adherence to those treatments and consequently asthma control.
Conclusion
Our review aimed to answer whether patient-centered care improves patient-focused outcomes for patients with asthma. We hypothesized that in order to achieve improved patient outcomes, it is vital to incorporate a patient-centered approach to asthma management, and that clinicians’ should expand from managing the disease according to guidelines, to collaborating with patients to self-manage their disease. Our review cited 133 total articles addressing this issue with the majority (43/60) of the intervention studies favoring a patient-centered approach. Many of these studies were in specific patient populations, making these data difficult to generalize, and the interventions themselves may be difficult to implement globally. Therefore, to better answer this question, improved research strategies that incorporate patient-centered techniques will need to be conducted, along with increasing clinician awareness and policy changes.
Current barriers to self-management of asthma can be addressed by patient-centered care, and through novel approaches, we can provide education and expand multi-media tools that better tailor treatment to include psychosocial factors. In addition to patient education, approaches to monitoring, such as checking in via telephone, help to provide patient-focused care in a practical and cost-effective manner.
Providers may perceive their own barriers clashing with the ideals of patient-focused care, such as time limitations and adaptations; however, Clark et alCitation180 proved that patient-centered care is a learned skill and can be provided without requiring greater time spent with the patient. While these studies are promising, they alone will not change the type of care patients receive without greater efforts to implement those changes. Further, benefit to the provider as far as improved satisfaction and decreased malpractice has been found.Citation1,Citation2
Future patient-centered research studies should investigate feasibility and strategies to implement patient-centered care for a host of patient needs, and should themselves be patient-focused. Without incorporating our patients’ view-points and insight into treatment plans, suboptimal adherence and patient outcomes are likely.
Acknowledgements
We would like to thank Meryl Prochaska, Krista Hoff, and Nicole Babuskow for their essential help with this project.
Disclosure
The authors report no conflicts of interest with this work. Dr Press reports receiving funding from the National Cancer Institute (KM1CA156717). Drs Qamar, Pappalardo, and Arora do not have funding to report.
References
- IrwinRSRichardsonNDPatient-focused care: using the right toolsChest20061301 Suppl73S82S16840370
- BaumanAEFardyJHHarrisPGGetting it right: why bother with patient-centered care?Med J Aust2003179525325612924973
- SextonDLStephanieRNCalcasolaSLBottomleySRFunkMAdults’ experience with asthma and their reported uncertainty and coping strategiesClin Nurse Spec199913181410335144
- VamosMKolbeJPsychological factors in severe chronic asthmaAust N Z J Psychiatry199933453854410483849
- Di MarcoFVergaMSantusPClose correlation between anxiety, depression, and asthma controlRespir Med20101041222819733042
- RheeHBelyeaMJCiurzynskiSBraschJBarriers to asthma self-management in adolescents: Relationships to psychosocial factorsPediatr Pulmonol200944218319119142893
- ClarkNMGongZMWangSJValerioMABriaWFJohnsonTRFrom the female perspective: Long-term effects on quality of life of a program for women with asthmaGend Med20107212513620435275
- BarnerJCMasonHLMurrayMDAssessment of asthma patients’ willingness to pay for and give time to an asthma self-management programClin Ther199921587889410397382
- KullowatzAKanniessFDahmeBMagnussenHRitzTAssociation of depression and anxiety with health care use and quality of life in asthma patientsRespir Med2007101363864416891108
- BodenheimerTEdwardWCrumbachKImproving primary care for patients with chronic illness. The Chronic Care Model, Part 2JAMA20022881909191412377092
- KinsmanDBlaserJJoint principles of a patient-centered medical home released by organizations representing more than 300,000 physicians: principles call for changes at the physician practice level to improve outcomesACP Newsroom Published March 5, 2007. Available from: http://www.acponline.org/pressroom/pcmh.htm. Accessed March 21, 2011.
- MulcahyKMaryniukMPeeplesMDiabetes self-management education core outcomes measuresDiabetes Educ200329576877014603868
- AdamsSGSmithPKAllanPFSystematic review of the chronic care model in chronic obstructive pulmonary disease prevention and managementArch Intern Med2007167655156117389286
- Patient Protection and Affordable Care Act 2010. (United States Congress).
- LittlePEverittHWilliamsonIPreferences of patients for patient centered approach to consultation in primary care: observational studyBMJ200132246847211222423
- FlockeSAMillerWLCrabtreeBFRelationships between physician practice style, patient satisfaction, and attributes of primary careJ Fam Pract20025183584012401151
- VillanuevaAGMitchellLPonticelliDEffectiveness of an asthma center in improving care and reducing costs in patients with difficult-to-control asthmaChest2000118Suppl815S
- LaineCDavidoffFLewisCEImportant elements of outpatient care: a comparison of patients’ and physicians’ opinionsAnn Intern Med19961256406458849148
- KoningCJMailleARStevensIPatients’ opinions on respiratory care: do doctors fulfill their needs?J Asthma1995323553637559276
- WhiteMVSanderNAsthma from the perspective of the patientJ Allergy Clin Immunol19991042 Pt 2S47S5210452788
- ApterAJReisineSTAffleckGBarrowsEZuWallackRLAdherence with twice-daily dosing of inhaled steroids. Socioeconomic and health-belief differencesAm J Respir Crit Care Med19981576 Pt 1181018179620910
- BarryCABradleyCPBrittenNPatients’ unvoiced agendas in general practice consultations: qualitative studyBMJ20003201246125010797036
- NewcombPAMcGrathKWCovingtonJKLazarusSCJansonSLBarriers to patient-clinician collaboration in asthma management: the patient experienceJ Asthma201047219219720170328
- AdamsSGSmithPKAllanPFAnzuetoAPughJACornellJESystematic review of the chronic care model in chronic obstructive pulmonary disease prevention and managementArch Intern Med2007167655156117389286
- LoveMMMainousAGTalbertJCContinuity of care and the physician-patient relationship: the importance of continuity for adult patients with asthmaJ Fam Pract200049998100411093565
- CourielJAsthma in adolescencePaediatr Respir Rev200341475412615032
- PriceJThe transition of management from childhood to adolescenceEur Respir Rev199771923
- LenneyWWellsNEJO’NeillBABurden of childhood asthmaEur Respir Rev199444962
- TownsSJvan AsperenPPDiagnosis and management of asthma in adolescentsClin Respir J200932697620298380
- JonesKGBellJFehrenbachCPearceLGrimleyDMcCarthyTPUnderstanding patient perceptions of asthma: results of the Asthma Control and Expectations (ACE) surveyInt J Clin Pract2002562899311926712
- RheeHWyattTHWenzelJAAdolescents with asthma: learning needs and internet use assessmentRespir Care200651121441144917134525
- JonesBLKellyKJThe adolescent with asthma: fostering adherence to optimize therapyClin Pharmacol Ther200884674975318946465
- MarquisPTrudeauEQuality of life and patient satisfaction: two important aspects in asthma therapyCurr Opin Pulm Med20017Suppl 1S18S2011385812
- WeinsteinAGDirection, motivation, and successful self-management of asthma: focus on drug complianceJ Asthma19842142812836146596
- ClarkNJonesPKellerSPatient factors and compliance with asthma therapyRespir Med1999931285686210653046
- RatcliffeJVan HaselenRBuxtonMAssessing patients’ preferences for characteristics associated with homeopathic and conventional treatment of asthma: a conjoint analysis studyThorax200257650350812037224
- SlackMKBrooksAJMedication management issues for adolescents with asthmaAm J Health-Syst Pharm19955213141714217671039
- ReidDAbramsonMRavenJManagement and treatment perceptions among young adults with asthma in Melbourne: the Australian experience from the European Community Respiratory Health SurveyRespirology20005328128711022992
- BustonKMWoodSFNon-compliance amongst adolescents with asthma: listening to what they tell us about self-managementFam Pract200017213413810758075
- GoemanDPDouglassJAOptimal management of asthma in elderly patients: strategies to improve adherence to recommended interventionsDrugs Aging200724538139417503895
- GoemanDPO’HeirREJenkinsC“You have to learn to live with it”: a qualitative and quantitative study of older people with asthmaClin Resp J20071299105
- AxelssonMEmilssonMBrinkEPersonality, adherence, asthma control and health-related quality of life in young adult asthmaticsRespir Med200910371033104019217764
- HylandMELeyAFisherDWWoodwardVMeasurement of psychological distress in asthma and asthma management programmesBr J Clin Psychol199534Pt 46016118563667
- WanTUse of health services by the elderly in low-income communitiesHealth Soc198260182107
- DavisKRowlandDUninsured and underserved: Inequities in health care in the United StatesMilbank Q198361140176
- Haire-JoshuDFisherEBJrMunroJWednerHJA comparison of patient attitudes toward asthma self-management among acute and preventive care settingsJ Asthma19933053593718407736
- SibbaldBPatient self care in acute asthmaThorax1989442971012929006
- LoignonCBedosCSevignyRUnderstanding the self-care strategies of patients with asthmaPatient Educ Couns200975225626219041209
- Van der PalenJKleinJJZielhuisGAvan HerwaardenCLSeydelERBehavioural effect of self-treatment guidelines in a self-management program for adults with asthmaPatient Educ Couns200143216116911369149
- CohenRFrancoKMotlowFReznikMOzuahPOPerceptions and attitudes of adolescents with asthmaJ Asthma200340220721112765323
- RichMLamolaSAmoryCSchneiderLAsthma in life context: Video Intervention/Prevention Assessment (VIA)Pediatrics20001053 Pt 146947710699095
- RichMTaylorSAChalfenRIllness as a social construct: understanding what asthma means to the patient to better treat the diseaseJt Comm J Qual Improv200026524425318350769
- SawyerSMFardyHJBridging the gap between doctors’ and patients’ expectations of asthma managementJ Asthma200340213113812765314
- NguyenBPWilsonSRGermanDFPatients’ perceptions compared with objective ratings of asthma severityAnn Allergy Asthma Immunol19967732092158814046
- JonesAPillRAdamsSQualitative study of views of health professionals and patients on guided self management plans for asthmaBMJ200032172751507151011118179
- LaforestLHasnaouiAEPribilCRiglentCSchwalmM-SGanseEVAsthma patients’ perception of their ability to influence disease control and managementAnn Allergy Asthma Immunol200910237838419492658
- ChoiTNWestermannHSaylesWMancusoCACharlsonMEBeliefs about asthma medications: patients perceive both benefits and drawbacksJ Asthma200845540941418569235
- HalmEAMoraPLeventhalHNo symptoms, no asthma: the acute episodic disease belief is associated with poor self-management among inner-city adults with persistent asthmaChest2006129357358016537854
- JonesIRAhmedNKellyMWith an attack I associate it more with going into hospital: understandings of asthma and psychosocial stressors; are they related to use of services?Soc Sci Med200866376577518006131
- VazquezIRomero-FraisEBlanco-AparicioMPsychological and self-management factors in near-fatal asthmaJ Psychosom Res201068217518120105700
- HandCHBradleyCHealth beliefs of adults with asthma: toward an understanding of the difference between symptomatic and preventive use of inhaler treatmentJ Asthma19963353313388827940
- KapteinAAHughesBMScharlooMIllness perceptions about asthma are determinants of outcomeJ Asthma200845645946418612897
- KendrickAHHiggsCMWhitfieldMJAccuracy of perception of severity of asthma: patients treated in general practiceBMJ199330769014224248374455
- RubinfeldARPainMCFRelationship between bronchial reactivity, airway caliber, and the severity of asthmaAm Rev Respir Dis1977115381387842951
- PeifferCMarsacJLockhartAChronobiological study of the relationship between dyspnoea and airway obstruction in symptomatic asthmatic subjectsClin Sci1989772372442805590
- AdamsRJSmithBJRuffinREPatient preferences for autonomy in decision making in asthma managementThorax200156212613211209101
- MarksonLEVollmerWMFittermanLInsight into patient dissatisfaction with asthma treatmentArch Intern Med2001161337938411176763
- OnyirimbaFApterAReisineSDirect clinician-to-patient feedback discussion of inhaled steroid use: its effect on adherenceAnn Allergy Asthma Immunol200390441141512722963
- De VriesUMuhligSWaldmannHCPatient satisfaction with different asthma-training variantsPatient Educ Couns200870226627518320609
- National Heart Lung and Blood InstituteNational Asthma Education and Prevention Program Available from: http://www.nhlbi.nih.gov/about/naepp/. Accessed February 11, 2011.
- Expert panel report: guidelines for the diagnosis and management of asthma (EPR 1991) NIH Publication No. 91-3642Bethesda, MDUS Department of Health and Human Services; National Institutes of Health; National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program1991
- National Heart Lung and Blood InstituteGuidelines for the diagnosis and management of asthma (EPR-3) Available from: http://www.nhlbi.nih.gov/guidelines/asthma. Accessed February 11, 2011.
- Global Initiative for Asthma [homepage on the Internet] Available at: http://www.ginasthma.org/ReportItem.asp?intId=96. Accessed April 29, 2011.
- Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA)2008 Available from: http://www.ginasthma.org/Guidelineitem.asp?|1=2&|2=1&intId=1388. Accessed April 29, 2011.
- GreenRHBrightlingCEPavordIDWardlawAJManagement of asthma in adults: current therapy and future directionsPostgrad Med J20037925926712782771
- CurrieGPDevereuxGSLeeDKCAyeresJGRecent developments in asthma managementBMJ200533058558915761000
- PeebleRSHartertTVHighlights from the Annual Scientific Assembly: patient-centered approaches to asthma management: strategies for treatment and management of asthmaSouth Med J200295777577912144090
- ReddelHKBarnesDJfor the Exacerbation Advisory PanelPharmacological strategies for self-management of asthma exacerbationsEur Respir J20062818219916816348
- PinnockHAdlemLGaskinSHarrisJSnellgroveCSheikhAAccessibility, clinical effectiveness, and practice costs of providing a telephone option for routine asthma reviews: phase IV controlled implementation studyBr J Gen Pract20075771472217761059
- CurtinKHayesBDHollandCLKatzLAComputer-generated intervention for asthma population care managementEff Clin Pract199811434610345260
- Van der MeerVvan StelHFBakkerMJWeekly self-monitoring and treatment adjustment benefit patients with partly controlled and uncontrolled asthma: an analysis of the SMASHING studyResp Res20101174
- SmithSMitchellCBowlerSPatient-centered education: applying learner-centered concepts to asthma educationJ Asthma20074479980418097853
- GibsonPGPowellHWilsonASelf-management education and regular practitioner review for adults with asthmaCochrane Database Syst Rev20031CD00111712535399
- SmithSMitchellCBowlerSStandard versus patient-centred asthma education in the emergency department: a randomized studyEur Respir J20083199099718216062
- HuangTTLiYTWangCHIndividualized programme to promote self-care among older adults with asthma: randomized controlled trialJ Adv Nursing20085220348358
- TousmanSZeitzHTaylorLDBristolCDevelopment, implementation and evaluation of a new adult asthma self-management programJ Community Health Nurs200724423725118092916
- NokelaMArnlindMHEhrsPOThe influence of structured information and monitoring on the outcome of asthma treatment in primary care: a cluster randomized studyRespiration201079538839419672055
- ShelledyDCLegrandTSGardnersDDPetersJIA randomized, controlled study to evaluate the role of an in-home asthma disease management program provided by respiratory therapists in improving outcomes and reducing the cost of careJ Asthma20094619420119253130
- BruzzeseJMUnikelLGallagherREvansDCollandVFeasiblity and impact of a school-based intervention for families of urban adolescents with asthma: results from a randomized pilot trialFam Proc20084795113
- MehuysEVan BortelLDe BolleLEffectiveness of pharmacist intervention for asthma control improvementEur Respi J2008314790799
- MartinMACatramboneCDKeeRAImproving asthma self-efficacy: developing and testing a pilot community-based asthma intervention for African American adultsJ Allergy Clin Immunol2009123115315919130936
- US Department of Health and Human ServicesHealthy People 2010: Understanding and Improving Health2nd edWashington, DCGovernment Printing Office2000
- Paasche-OrlowMKRiekertKABilderbackATailored education may reduce health literacy disparities in asthma self-managementAm J Respir Crit Care Med200517298098616081544
- Cruz-CorreiaRFonsecaJLimaLWeb-based or paper-based self-management tools for Asthma – patients’ opinions and quality of data in a randomized crossover studyStud Health Technol Inform200712717818917901611
- Van der MeerVvan StelHFDetmarSBOttenWSterkPJSontJKInternet-based self-management offers an opportunity to achieve better asthma control in adolescentsChest200713211211917400674
- Van der MeerVBakkerMJvan den HoutWBInternet-based self-management plus education compared with usual care in asthmaAnn Intern Med200915111012019620163
- SobelRMPaasche-OrlowMKWaiteKRRittnerSSWilsonEAHWolfMSAsthma 1-2-3: a low literacy multimedia tool to educate African American adults about asthmaJ Community Health20093432132719353250
- JosephCLMPetersonEHavstadSA Web-based, tailored asthma management program for urban African-American high school studentsAm J Respir Crit Care Med200717588889517290041
- MosnaimGSCohenMSRhoadsCHRittnerSSPowellLHUse of MP3 players to increase asthma knowledge in inner-city African-American adolescentsInt J Behav Med20081534134619005935
- Van den BemtLde VriesMPCloostermanSInfluence of house dust mite impermeable covers on health-related quality of life of adult patients with asthma: results of a randomized clinical trialJ Asthma2007441084384818097861
- BrodtkorbTHZetterströmOTinghögGCost-effectiveness of clean air administered to the breathing zone in allergic asthmaClin Resp J201042104110
- KeithPKKochCDjandjiMMontelukast as add-on therapy with inhaled corticosteroids or inhaled corticosteroids and long-acting beta-2-agonists in the management of patients diagnosed with asthma and concurrent allergic rhinitis (the RADAR trial)Can Respir J200916Suppl A17A24A
- BarnesNLavioletteMAllenDEffects of montelukast compared to double dose budesonide on airway inflammation and asthma controlRespir Med2008816521658
- VoltoliniSTroiseCIncorvaiaCEffectiveness of high dose sublingual immunotherapy to induce a stepdown of seasonal asthma: a pilot studyCurr Med Res Opin2010261374019895362
- Van RensenELEvertseCEvan SchadewijkWAEosinophils in bronchial mucosa of asthmatics after allergen challenge: effect of anti-IgE treatmentAllergy2009641728019076931
- MillerDPTomGRasouliyanLChippsBPatient-reported outcomes among omalizumab and salmeterol/fluticasone combination therapy patientsJ Asthma200946217918519253127
- RisciliBPParsonsJPMastronardeJGTreating silent reflux disease does not improve poorly controlled asthmaClev Clin J Med2010773155160
- UlrikCSClaudiusBKTammMEffect of asthma compliance enhancement training on asthma control in patients on combination therapy with salmeterol/fluticasone propionate: a randomised controlled trialClin Resp J200933161168
- BashetiIAArmourCLBosnic-AnticevichSZReddelHKEvaluation of a novel educational strategy, including inhaler-based reminder labels, to improve asthma inhaler techniquePatient Educ Couns2008721263318314294
- BenderBGApterABogenDKTest of an interactive voice response intervention to improve adherence to controller medications in adults with asthmaJ Am Board of Family Med2010232159165
- PressVGAroraVMShahLMMisuse of respiratory inhalers in hospitalized patients with asthma or COPDJ Gen Intern Med Epub Jan 20 2011.
- National Center for Complementary and Alternative Medicine [homep-age on the Internet] Available from: http://nccam.nih.gov. Accessed February 11, 2011.
- SladerCAReddelHJenkinsCRArmourCLBosnic-AnticevichSZComplementary and alternative medicine use in asthma: who is using what?Respiratory200611373387
- MarinoLAShenJCharacteristics of complementary and alternative medicine use among adults with current asthma; 2006J Asthma20104752152520536278
- HollowayEALassersonTJBreathing exercise for asthmaCochrane Database Syst Rev20041CD1277
- ArnoldEClarkCELassersonTJWuTHerbal intervention for chronic asthma in adults and childrenCochrane Database Syst Rev20081CD05989
- McCarneyRWLindeKLassersonTJHomeopathy for chronic asthmaCochrane Database Sys Rev20041CD0353
- BieloryLRussinJZuckermanGBClinical efficacy, mechanism of action, and adverse effects of complementary and alternative therapies for asthmaAllergy Asthma Proc20042528329115603200
- ThomasMMcKinleyRKMellorSBreathing exercises for asthma: a randomised controlled trialThorax200964556119052047
- CowieRLConleyDPUnderwoodMFReaderPGA randomised controlled trial of the Buteyko technique as an adjunct to conventional management of asthmaRespir Med2008102572673218249107
- ChoiJYJungHJKimJIA randomized pilot study of acupuncture as an adjunct therapy in adult asthmatic patientsJ Asthma201047777478020701479
- ShawANobleASalisburyCSharpDThompsonEPetersTJPredictors of complementary therapy use among asthma patients: results of a primary care surveyHealth Soc Care Community200816215516418290981
- GibsonPGTalbotPIToneguzziRCSelf-management, autonomy, and quality of life in asthmaChest19951074100310087705105
- SidanaASinghDMohanAGuleriaRQuality of life and autonomy preferences in stable asthmatics: a developing country scenarioRespirology2009141838919144053
- AdamsRJSmithBJRuffiREImpact of the physician’s participatory style in asthma outcomes and patient satisfactionAnn Allergy Asthma Immunol20018626327111289322
- HoltSKljakovicMReidJfor POMS Steering CommitteeAsthma morbidity, control and treatment in New Zealand: results of the Patient Outcomes Management Survey (POMS); 2001NZ Med J20031161174U436
- WilliamsMVBakerDWHonigEGLeeTMNowlanAInadequate literacy is a barrier to asthma knowledge and self careChest1998114100810159792569
- GibsonPGHenryRLVimpaniGVHallidayJAsthma knowledge, attitudes and quality of life in adolescentsArch Dis Child1995733213267492196
- JansonSLMcGrathKWCovingtonJKChengSCBousheyHAIndividualized asthma self-management improves medication adherence and markers of asthma controlJ Allergy Clin Immunol2009123484084619348923
- ThoonenBPSchermerTRVan Den BoomGSelf-management of asthma in general practice, asthma control and quality of life: a randomized controlled trialThorax2003581303612511716
- UrekMCTudoricNPlavecDUrekRKoprivc-MilenovicTStojicMEffect of educational programs on asthma control and quality of life in adult asthma patientsPatient Educ Couns2005581475415950836
- WilsonSRStrubPBuistASShared treatment decision making improves adherence and outcomes in poorly controlled asthmaAm J Respir Crit Care Med2010181656657720019345
- McKenzieLCairnsJOsmanLSymptom-based outcome measures for asthma: the use of discrete choice methods to assess patient preferencesHealth Policy200157319320411459626
- OhmRAaronsonLSSymptom perception and adherence to asthma controller medicationsJ Nurs Scholarsh200638329229717044348
- SchafferSDTianLPromoting adherence: effects of theory-based asthma educationClin Nurs Res2004131698914768768
- PoniemanDWisniveskyJPLeventhalHMusumeci-SzaboTJHalmEAImpact of positive and negative beliefs about inhaled corticosteroids on adherence in inner-city asthmatic patientsAnn Allergy Asthma Immunol2009103384219663125
- SchneiderAWensingMQuinzlerRBieberCSzecsenyiJHigher preference for participation in treatment decisions is associated with lower medication adherence in asthma patientsPatient Educ Couns2007671–2576217346917
- SchneiderABiesseckerKQuinzlerRAsthma patients with low perceived burden of illness: a challenge for guideline adherenceJ Eval Clin Pract200713684685218070254
- SchererYKBruceSKnowledge, attitudes, and self-efficacy and compliance with medical regimen, number of emergency department visits, and hospitalizations in adults with asthmaHeart Lung200130425025711449211
- MenckebergTTBouvyMLBrackeMBeliefs about medicines predict refill adherence to inhaled corticosteroidsJ Psychosom Res2008641475418157999
- OsmanLMHow do patients’ views about medication affect their self-management in asthma?Patient Educ Couns1997321 SupplS43S499516759
- MancusoCARinconMMcCullochCESelf-efficacy, depressive symptoms, and patients’ expectations predict outcomes in asthmaMed Care2001391326133811717574
- LavoieKLCartierALabrecqueMAre psychiatric disorders associated with worse asthma control and quality of life in asthma patients?Respir Med2005991249125716140225
- GoldneyRDRuffinRFisherLJAsthma symptoms associated with depression and lower quality of life: a population surveyMed J Aust200317843744112720509
- SándezEVázquezMIRomero-FraisEBlanco-AparicioMOteroIVereaHDepression, panic-fear, and quality of life in near-fatal asthma patientsJ Clin Psychol Med S2005122175184
- SchneiderALoweBMeyerFJBiesseckerKJoosSSzecsenyiJDepression and panic disorder as predictors of health outcomes for patients with asthma in primary careRespir Med2008102335936618061424
- CalfeeCSKatzPPYelinEHIribarrenCEisnerMDThe influence of perceived control of asthma on health outcomesChest200613051312131817099005
- JansonSLFahyJVCovingtonJKEffects of individual self-management education on clinical, biological and adherence outcomes in asthmaAm J Med200311562062614656614
- SainiBKrassIArmourCDevelopment, implementation, and evaluation of a community pharmacy-based asthma care modelAnn Pharmacother200481954196015479780
- LloydAMcintoshEWilliamsAEKapteinARabeKFHow does patients’ quality of life guide their preferences regarding aspects of asthma therapy? A patient-preference study using discrete-choice experiment methodologyThe Patient: Patient-Centered Outcomes Research200814309316
- JuniperEFSvenssonKMorkACStahlEMeasuring health-related quality of life in adults during an acute asthma exacerbationChest20041251939714718426
- ChervinskyPBakerJBenschGPatient-reported outcomes in adults with moderate to severe asthma after use of budesonide and formoterol administered via 1 pressurized metered-dose inhalerAnn Allergy Asthma Immunol2008101546347319055199
- O’ConnorRDPatrickDLParasuramanBMartinPGoldmanMComparison of patient-reported outcomes during treatment with adjustable- and fixed-dose budesonide/formoterol pressurized metered-dose inhaler versus fixed-dose fluticasone propionate/salmeterol dry powder inhaler in patients with asthmaJ Asthma201047221722320170333
- HodderRReesePRSlatonTAsthma patients prefer Respimat Soft Mist Inhaler to TurbuhalerInt J Chron Obstruct Pulmon Dis2009422523219554196
- MurphyKNelsonHParasuramanBBoggsRMillerCO’DowdLThe effect of budesonide and formoterol in one pressurized metered-dose inhaler on patient-reported outcomes in adults with mild-to-moderate persistent asthmaCurr Med Res Opin200824387989418267051
- Van SchayckCPBijl-HoflandIDFolgeringHInfluence of two different inhalation devices on therapy compliance in asthmatic patientsScand J Prim Health Care200220212612812184713
- PriceDBWilliamsAEYoxallSSalmeterol/fluticasone stable-dose treatment compared with formoterol/budesonide adjustable maintenance dosing: impact on health-related quality of lifeRespir Res200784617610727
- LeidyNKGutierrezBLamplKUryniakTO’BrienCDCan patients with asthma feel inhaler therapy working right away? Two clinical trials testing the effect of timing of assessment on patient perceptionJ Asthma200946101006101219995138
- SchatzMZeigerRSVollmerWMThe controller-to-total asthma medication ratio is associated with patient-centered as well as utilization outcomesChest20061301435016840381
- KnoellDLPiersonJFMarshCBAllenJNPathakDSMeasurement of outcomes in adults receiving pharmaceutical care in a comprehensive asthma outpatient clinicPharmacotherapy1998186136513749855341
- D’SouzaWJTe KaruHFoxCLong-term reduction in asthma morbidity following an asthma self-management programmeEur Respir J19981136116169596111
- LemaigreVVan den BerghOVictoirADe PeuterSVerledenGMEffects of a shortened asthma self-management group programActa Clin Belg2010651293620373595
- BuchnerDAButtLTDe StefanoAEdgrenBSuarezAEvansRMEffects of an asthma management program on the asthmatic member: patient-centered results of a 2-year study in a managed care organizationAm J Manag Care1998491288129710185979
- UlrikCSSoes-PetersenUBackerVLangePHarvingHPlaschkePDisease variability in asthma: how do the patients respond? – and why?J Asthma200845650751118612905
- GarrettJFenwickJMTaylorGMitchellEReaHPeak expiratory flow meters (PEFMs) – who uses them and how does education affect the pattern of utilization?Aust NZ J Med199424521529
- HarverAHumphriesCTKotsesHDo asthma patients prefer to monitor symptoms or peak flow?J Asthma200946994094319905923
- HaughneyJFletcherMWolfeSRatcliffeJBriceRPartridgeMRFeatures of asthma management: quantifying the patient perspectiveBMC Pulm Med200771618062804
- BushAKaragiannisGEStamatopoulosVGKotisTPublic perception of realtime information services for environmental monitoring and management of asthmaJ Telemed Telecare200612Suppl 1111316884564
- LittlePEverittHWilliamsonIObservational study of effect of patient centeredness and positive approach on outcomes of general practice consultationsBMJ200132390891111668137
- McTaggart-CowanHMShiPFitzgeraldJMAn evaluation of patients’ willingness to trade symptom-free days for asthma-related treatment risks: a discrete choice experimentJ Asthma200845863063818951253
- LiuMYJenningsJPSamuelsonWMSullivanCAVeltriJCAsthma patients’ satisfaction with the frequency and content of pharmacist counselingJ Am Pharm Assoc (Wash)199939449349810467812
- ThoonenBPSchermerTRJansenMAsthma education tailored to individual patient needs can optimise partnerships in asthma self-managementPatient Educ Couns200247435536012135827
- ShethKWassermanRLLincourtWRLocantoreNWCarranza-RosenzweigJCrimCFluticasone propionate/salmeterol hydro-fluoroalkane via metered-dose inhaler with integrated dose counter: Performance and patient satisfactionInt J Clin Pract200660101218122416981966
- SanderNFusco-WalkerSJHarderJMChippsBEDose counting and the use of pressurized metered-dose inhalers: running on emptyAnn Allergy Asthma Immunol200697343816892778
- OgrenRABaldwinJLSimonRAHow patients determine when to replace their metered-dose inhalersChest200212187187611888975
- RubinBKDurotoyeLHow do patients determine that their metered-dose inhaler is empty?Chest20041261134113715486374
- CainWTOppenheimerJJThe misconception of using floating patterns as an accurate means of measuring the contents of metered-dose inhaler devicesAnn Allergy Asthma Immunol20018741741911730185
- Guidance for Industry Integration of Dose-counting Mechanisms into MDI Drug ProductsUS Department of Health and Human Services, Food and Drug Administration Center for Drug Evaluation and Research, Division of Pulmonary and Allergy Drug ProductsRockville, MarylandGuidance for Industry2003
- BergnerAGriesnerWA2ndBergnerRKMetered-dose inhalers: the specified number of spraysJAMA199326915068445810
- ClarkNMGongMSchorkMALong-term effects of asthma education for physicians on patient satisfaction and use of health servicesEur Respir J200016152110933079