
Abstract
Purpose
The purpose of this study was to identify risk factors for poor health-related quality of life (HRQL) in multi-morbid adult cancer survivors and explore whether perceived treatment and self-management burden mediate any of these relationships.
Methods
Ninety-one multi-morbid cancer survivors (median age: 65 years) completed surveys at baseline and 6 months. Demographic, psychosocial, and health care-related factors were assessed as were perceived treatment burden and general HRQL (physical and mental health). Data on medical diagnoses and cancer treatment were extracted from the medical record. Bivariate correlations screened for associations between predictors and outcomes, with significant predictors entered into multivariable linear regressions to identify unique risk factors for greater treatment burden and poorer HRQL. Follow-up regressions examined whether treatment burden mediated any of the risk factor–outcome relationships.
Results
Factors that correlated with higher baseline treatment burden included: having more diagnoses, less formal education, having seen more physicians in the past 6 months, having a mental health diagnosis, not having a set routine for one’s self-management, low health literacy, low self-efficacy for self-management, and low social support (Ps <0.05). Among these, factors that also correlated with worse 6-month HRQL outcome included: having more diagnoses, having seen more physicians in the past 6 months, having a mental health diagnosis, not having a set routine for one’s self-management, low health literacy, low self-efficacy, and low social support (Ps <0.05). Multivariable regressions showed that some of these factors independently predicted higher treatment burden and/or worse HRQL. Low self-efficacy was the most robust independent risk factor for poor HRQL (bs: 0.34–0.49, Ps <0.005), with evidence supporting that the relationships were partially mediated by treatment burden.
Conclusion
Monitoring of psychosocial and health care-related risk factors for high treatment burden and poor HRQL can identify multi-morbid cancer survivors in need of extra support and could inform a more personalized treatment approach.
Introduction
A “cancer survivor” is any person with a history of cancer, from the time of diagnosis onward.Citation1 There are over 15 million cancer survivors alive today (excluding those with superficial basal or squamous cell skin cancers). In the US, a 37% increase in the number of cancer survivors 5 or more years from diagnosis is projected over the next decade.Citation2 Reasons for this include improvements in early detection and screening, earlier diagnosis, and advances in treatment, all coupled with increases in cancer incidence produced by the aging of the population.Citation2,Citation3 Because ~60% of all cancer survivors are 65 years of age or older,Citation4 many are also coping with other age-related medical conditions, both comorbid complications stemming from cancer therapies (eg, congestive heart failure) and conditions unrelated to the cancer.Citation4,Citation5 In a recent National Cancer Institute-funded project (the Follow-up Care Use of Cancer Survivors study), the mean number of comorbid conditions in survivors was five, 1.9 of which were diagnosed after the cancer diagnosis, on average.Citation4 Research has shown that multi-morbidity in cancer survivors is associated with worse health outcomes, including poorer health-related quality of life (HRQL)Citation6 and worse overall survival.Citation4,Citation5
In general, the literature on multi-morbidity and HRQL, whether directed toward people treated for cancer or for other major illnesses, has not given much theoretical consideration to plausible underlying mechanisms of effect beyond an implied additive model of physical and mental health impacts of single disease states.Citation7 One mechanism that may warrant more consideration is the role played by the complex and often burdensome nature of treatment and self-management for multiple comorbid conditions, including when one of the conditions is cancer. Treatment burden has been defined as the personal workload of health care, including treatment and self-management of chronic health conditions, as well as its impact on patient functioning and well-being.Citation8 Treatment burden is relevant to people with multiple comorbidities as such individuals are often required to engage in a complex array of self-care activities to maintain their health.Citation9 The weight of such burden has been found to be associated with nonadherence to medical regimens,Citation8,Citation10,Citation11 more hospitalizations,Citation12 poorer HRQL,Citation8,Citation13–Citation15 and lower survival rates.Citation16 New patient self-report measures are allowing greater scrutiny of the relationship between burden and health outcomes.Citation8,Citation17 The multi-domain Patient Experience with Treatment and Self-management (PETS) is one such measure.Citation8 In addition to assessing generic challenges in the work of self-care (eg, medication taking, monitoring health, medical appointments, financial concerns), the PETS also includes two scales that assess the impact of treatment and self-management burden on overall well-being – the role-social activity limitations scale and the physical/mental exhaustion from self-management scale.
The primary aim of the present study was to investigate the extent that certain demographic, psychosocial, medical, and health care-related variables act as independent risk factors for greater treatment burden and poorer general HRQL in multi-morbid cancer survivors. Consistent with other studies of cancer patients and survivors, we hypothesized that less formal education, lower self-efficacy for self-management (ie, less confidence in self-management ability), lower social support, having more comorbid medical conditions, and having a diagnosis of a comorbid mental health condition (ie, depression, anxiety, or both) would be associated with greater perceived treatment burden and poorer HRQL in multi-morbid cancer survivors.Citation2,Citation6,Citation18–Citation21 Furthermore, since low health literacy (ie, the capacity to process and understand basic health information)Citation22 has been consistently associated with worse health outcomes in people with chronic illness, we further hypothesized that lower levels of subjective health literacy would be associated with greater perceived treatment burden and poorer HRQL in multi-morbid survivors. Based on findings from qualitative studies and reviews of people coping with multiple comorbid conditions, especially those conditions that are chronic or require sustained self-care,Citation9,Citation23–Citation26 we also hypothesized that multi-morbid cancer survivors who lack a set routine for their self-management and those who must see several different physicians for their health conditions will report greater treatment burden and poorer HRQL. Finally, consistent with recent analyses of the role of treatment burden in the process of coping with chronic illness,Citation27 we explored whether any of the relationships between risk factors and HRQL are mediated by treatment burden.
Methods
Subjects
As part of a larger prospective validation study of the PETS measure, a cohort of adults living with multiple chronic conditions (MCCs) was identified from the Rochester Epidemiology Project (REP), a medical records-linked system for residents of Olmsted County, Minnesota. The REP captures and stores medical record data on diagnoses, treatments and other procedures, drug prescriptions, hospitalizations, as well as emergency room and office visits for virtually the entire local population.Citation28 It has been used as a population-based sampling frame for survey studies.Citation29,Citation30 For the parent study, 1,496 people were identified with two or more of 20 chronic conditions defined as prevalent by the US Department of Health and Human Services.Citation31 Cancer was one of the eligible conditions. Persons with severe cognitive impairments or other conditions that would make it difficult to complete a survey (eg, dementia) were excluded. Of the 1,496 people invited to participate, 443 agreed by returning a completed baseline survey (30%). Of this sample of responders, 115 had a documented cancer diagnosis more than a year prior to survey completion. Twenty-four responders who had only a diagnosis of non-melanoma skin cancer were excluded, leaving 91 people (21% of responders) for the present study.
Procedure
A survey booklet consisting of all study measures was mailed to the sample of eligible persons along with a cover letter and privacy authorization form (Health Insurance Portability and Accountability Act [HIPAA]). The study was approved as having minimal risk with use of oral consent by the Mayo Clinic Institutional Review Board (IRB #14-008629). A signed HIPAA form was required prior to use of any protected health information extracted from the medical record. Informed consent was met via the cover letter with consent implied by return of a completed survey. Survey packets (including a stamped return envelope) were mailed at study outset (baseline) and at 6-month follow-up. At each time point, two repeat mailings were sent to those who failed to respond within 3 weeks of the initial mailing. Participants were compensated $10 for each completed survey.
Measurement of study variables
The survey assessed demographics (ie, age, race/ethnicity, education status, marital status, and occupation status), psychosocial factors (ie, self-efficacy, social support, health literacy), health care-related factors (ie, care fragmentation, having a set self-management routine), treatment burden, and HRQL. The eight-item Perceived Medical Condition Self-Management (PMCSM) scale was used to assess self-efficacy for managing chronic conditions, and the six-item ENRICHD Social Support Instrument (ESSI) was used to assess available emotional, informational, and instrumental support from others. The PMCSM scale and ESSI have been found to be reliable and valid in people with chronic illnesses.Citation32,Citation33 A validated single-item screener assessed subjective health literacy: “How often do you have problems learning about your medical condition because of difficulty understanding written information (all of the time, most of the time, some of the time, little of the time, none of the time)?”Citation34 The following items were developed to assess care fragmentation and the presence of a self-management routine, respectively: “How many different physicians have you seen for your health conditions in the past 6 months (1, 2, 3, 4, 5+)?” and “I have a set routine for all of my self-management (agree/disagree).” Impact of treatment burden on well-being was assessed using the role-social activity limitations and physical/mental exhaustion scales of the PETS.Citation8 The scales have been found to be reliable and valid in diverse samples of people with MCCs, including cancer.Citation8,Citation27 Baseline assessments of all of the above factors were used to test the hypothesized longitudinal relationships with the HRQL outcomes.
HRQL was assessed using responses to the 6-month follow-up survey. The 6-month HRQL assessment was used in this analysis because we wanted to determine how well survivors’ prior status on the risk factors and perceived treatment burden would predict HRQL at a later time. General physical and mental health status were assessed using the global physical health (GPH) and global mental health (GMH) summary scores of the Patient-Reported Outcomes Measurement Information System-10 (PROMIS-10), respectively. The PROMIS-10 has been found to be reliable and valid in diverse samples of people with chronic illnesses.Citation35
Indicators extracted from the electronic medical record at baseline included gender, medical condition diagnoses, primary cancer diagnosis, date of cancer diagnosis, and cancer treatment. Diagnoses were summed to create a variable indicating the total number of conditions extracted, including the cancer. Diagnosis of a mental health condition was indicated by a medical record-confirmed diagnosis of depression, anxiety, or both.
Statistical analyses
Descriptive statistics were used to characterize the subjects. Predictive, risk-factor models were then built in stages beginning with unadjusted Pearson product-moment correlations (r) to screen for bivariate relationships between baseline variables, treatment burden, and the 6-month HRQL outcomes. This included point-biserial correlations for any binary predictors, which can be approximated using Pearson’s r.Citation36 Significant correlation with one or more outcomes (P<0.05, two-tailed) indicated which baseline factors to include in each multivariable linear regression model (ie, candidate risk factors). Per Cohen criteria, rs ≥0.30 were considered to be at least moderate in size.Citation37 Next, four multivariable linear regressions were conducted, one for each of the two PETS treatment burden scales (role-social activity limitations and physical/mental exhaustion) and one for each of the two PROMIS-10 summary scores (6-month GPH and 6-month GMH). Strength of the association of each predictor with each criterion, relative to other variables in the model, was indicated by the standardized regression weight (standardized β). The alpha for significance of β was set at 0.05. Overall fit of each regression was indicated by the model R2, that is, the total percent of variance in the specified criterion explained by the entered predictors. All analyses were conducted in IBM SPSS® Statistics version 22.
Exploring mediation
The regression methodology outlined by Baron and KennyCitation38 and KennyCitation39 was used to explore possible mediation of the relationship of the baseline predictors to the 6-month HRQL outcomes through baseline treatment burden. A series of three regressions is used with mediation supported if: 1) there is evidence of a relationship between a predictor and an outcome (regression 1); 2) there is evidence of a relationship between a predictor and a proposed mediating factor (regression 2); and 3) the magnitude of the relationship between the predictor and outcome is reduced when the mediating factor is simultaneously entered into the regression equation (regression 3). The extent of mediation (complete vs partial) is determined by the magnitude of the reduction in the relationship between the predictor and the outcome after the mediating factor is entered into the regression by comparing the regression coefficients of the same predictor in regressions 1 and 3. Sobel’s method,Citation40 a method endorsed by Kenny,Citation39 can be used to determine the statistical significance of any observed mediating effect by testing whether the indirect effect is significantly different from zero.
The multivariable regressions testing predictors of baseline treatment burden and the 6-month HRQL outcomes (as described above) were used to identify which relationships required exploration of potential mediation. To minimize the number of regressions needed, we explored whether a single “overall treatment burden” score could be used. A recent study derived and used a single factor score of the role-social activity limitations and physical/mental exhaustion scales of the PETS after showing that these two scales were highly correlated (r=0.69).Citation27 Alpha for the significance of regression coefficients and Sobel’s test (Z) was set at 0.05, two-tailed.
Results
Characteristics of study subjects
Descriptive and medical characteristics of the study subjects are shown in . Briefly, median age of the subjects was 65 years and there were slightly more women (59%) than men. Most identified their race as white (81%) and had at least some formal college or university education (74%). Data from the electronic medical record indicated that the most frequent cancer diagnoses were breast (21%) and genitourinary (19%) cancer, and most had been treated with surgery (63%). The median length of time between diagnosis of the primary cancer and completion of the baseline survey was 6.5 years (range: 1.1–40.5 years). Median number of diagnosed conditions including the cancer was five.
Table 1 Descriptive and medical characteristics of study subjects (N=91)
Bivariate correlations of baseline risk factors, treatment burden, and HRQL outcomes
presents the unadjusted Pearson correlations (r) of the potential risk factors, the two treatment burden impact scales (ie, role-social activity limitations and physical/mental exhaustion due to self-management), and the 6-month HRQL outcomes (PROMIS GPH, PROMIS GMH). Four factors were associated with both of the PETS treatment burden scales. Having seen more physicians in the past 6 months, having a diagnosis of a mental health condition (depression, anxiety, or both), not having a set routine for one’s self-management, and lower self-efficacy for self-management were associated with greater treatment burden impact (Ps <0.05). Magnitudes of most of these correlations (88%) were medium in size or greater (r≥0.30).Citation37 Having no more than a high school education, lower health literacy, and lower perceived social support were associated with more physical/mental exhaustion (Ps <0.01), but were not significantly associated with role-social activity limitations. More diagnosed conditions were associated with more role-social activity limitations (P<0.01), but were not associated with physical/mental exhaustion.
Table 2 Pearson product-moment correlations of baseline predictors (ie, risk factors), treatment burden, and 6-month health-related quality of life
These risk factors were also associated with the 6-month HRQL outcomes (). Having seen more physicians in the past 6 months, having a diagnosis of a mental health condition, lower self-efficacy, and lower perceived social support were associated with worse 6-month GPH and worse 6-month GMH (Ps <0.05). Most of these correlations (75%) were medium in size or greater in magnitude (>0.30). Furthermore, more diagnosed conditions and lower subjective health literacy were associated with lower 6-month GPH, while not having a set self-management routine was associated with lower 6-month GMH. Education status was not significantly associated with either HRQL outcome. Finally, baseline scores from both the treatment burden scales were moderately to strongly associatedCitation37 with the 6-month HRQL outcomes (rs ranging from −0.47 to −0.56).
Multivariable regression models of treatment burden and HRQL outcomes
The unadjusted correlations screened risk factors for entry into a series of linear regression analyses. These regression models examined predictors of treatment burden and HRQL and determined: 1) if certain risk factors, assessed at baseline, were independently associated with both treatment burden and HRQL, and 2) whether some risk factors may influence HRQL outcomes indirectly through treatment burden (ie, mediation). displays the results of linear regression models (Models 1 and 2) that regress baseline scores of the two PETS treatment burden impact scales onto the baseline risk factors found to be correlated with treatment burden impact in . In Model 1, having seen more physicians in the past 6 months (standardized β=0.35) and lower self-efficacy (β=−0.31) were associated with more role-social activity limitations due to self-management (overall model R2=0.36). In Model 2, not having a set self-management routine (β=−0.21), lower health literacy (β=−0.25), and lower self-efficacy (β=−0.22) were associated with more physical/mental exhaustion due to self-management (overall model R2=0.45).
Table 3 Multiple linear regressions of treatment burden scales onto risk factors
displays the results of linear regressions of the 6-month HRQL outcomes onto the baseline risk factors found to be correlated with these outcomes in . In Model 3, lower self-efficacy at baseline (β=0.49) predicted worse GPH at 6 months (overall model R2=0.43). In Model 4, lower self-efficacy at baseline (β=0.34) predicted worse GMH at 6 months (overall model R2=0.41).
Table 4 Multiple linear regressions of 6-month health-related quality-of-life outcomes onto baseline risk factors
Regression analyses to explore mediation by treatment burden
Because the regression models identified that perceived self-efficacy was associated with both treatment burden and the HRQL outcomes, we tested whether the effects of perceived self-efficacy on 6-month HRQL are mediated through its effect on treatment burden (). In order to reduce the number of regressions needed to test for mediation, we created an aggregated factor score of “overall treatment burden” using principal components analysis of the items of the two PETS scales. This is justified by the very high correlation observed between the role-social activity limitations and physical/mental exhaustion scales (r=0.73). The first component extracted accounted for 65.5% of the total variance (eigenvalue =7.2). After oblique rotation with Kaiser normalization, all items were found to load highly on this one factor (≥0.55). The treatment burden factor score was saved and used in the subsequent tests of mediation. All regression models used to test for mediation were adjusted for the number of diagnosed conditions.
Figure 1 Hypothesized mediational pathway.
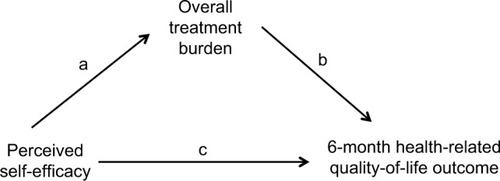
A simple regression confirmed that lower self-efficacy predicted higher overall treatment burden (β=−0.42, P<0.001; overall model R2=0.24). This supports path a in . summarizes the findings of the set of models testing for mediation effects of self-efficacy on 6-month HRQL through overall treatment burden. Higher overall treatment burden at baseline was independently predictive of lower GPH (β=−0.40) and lower GMH (β=−0.30) at 6 months (path b in ). Furthermore, when overall treatment burden was included in a model with baseline self-efficacy (Model 2 in each series), the regression coefficient for self-efficacy decreased for both HRQL outcomes compared to the regression coefficients for self-efficacy displayed in Model 1 of each series, that is, the direct effects of self-efficacy on HRQL. However, the regression coefficients for self-efficacy remained significant even after overall treatment burden was entered (Model 2). Hence, for GPH and GMH, there was evidence for a partial mediation effect of treatment burden impact (paths a and b in ). Based on Sobel’s method for determining the significance of an indirect effect of a predictor on an outcome through a mediator,Citation40 we found that mediation by overall treatment burden was statistically significant for both GPH at P=0.008 and GMH at P=0.03 (two-tailed).
Table 5 Mediation of the relationship between self-efficacy and 6-month health-related quality-of-life outcomes by overall treatment burden
Discussion
Our study attempts to understand risk factors that predict quality-of-life deficits in cancer survivors with multi-morbidity, excluding those with cognitive impairment. To our knowledge, it is one of the first to focus on the role of perceived treatment and self-management burden in cancer survivors. Treatment burden, that is, the personal work and challenges of treatment and self-management as well as their effect on well-being, adversely impacts the quality of life of people coping with multi-morbidity.Citation8,Citation13
Psychosocial factors were found to be predictive of treatment burden and HRQL. Self-efficacy for self-managing chronic conditions was associated with all of the outcomes assessed. Survivors who reported less confidence in their ability to manage their chronic conditions reported more role-social activity limitations and greater physical/mental exhaustion due to self-management. They also reported worse GPH and GMH at 6 months after baseline. The relationship between self-efficacy and health outcomes has been consistently observed across a range of chronic health conditions including people with MCCs.Citation8,Citation18,Citation41 A recent cross-sectional study of 182 cancer survivors has shown that self-efficacy for managing chronic disease is strongly associated with HRQL and overall life satisfaction.Citation19 Given that self-efficacy was related to both treatment burden and the HRQL outcomes and treatment burden was associated with both of the HRQL outcomes, we further analyzed whether treatment burden acts as a mediator (ie, self-efficacy → treatment burden → HRQL).Citation38 We found that overall treatment burden (as defined by a factor score combining items from the role-social activity limitations and physical/mental exhaustion scales of the PETS) partly mediated the relationship of self-efficacy at baseline and general physical and general mental health at 6-month follow-up. Hence, it is possible that confidence in one’s ability to self-manage may partly influence physical and mental health by affecting perceived treatment burden.
Regarding other psychosocial factors, subjective health literacy was independently associated with treatment burden. Survivors who reported more problems with understanding written medical information about their health condition(s) reported feeling more physically and mentally exhausted with their self-management. Brief indicators of health literacy have been found to be predictive of general health status and perceptions of treatment burden,Citation8,Citation42 and some have speculated that the ability to self-manage one’s health situation is a critical link between health literacy and health outcomes.Citation43 While perceived available social support was correlated with treatment burden and HRQL, it was not found to be independently predictive of either in the multivariable regression analyses. However, social support was found to be moderately correlated with self-efficacy (r=0.42). Hence, it is plausible that support from others may influence treatment burden and HRQL by enhancing a person’s confidence in his/her ability to self-manage.
Certain health care-related factors were found to increase the risk for poorer outcomes. Greater care fragmentation in the form of having to see more physicians for one’s health was associated with more role-social activity limitations due to self-management. Cancer survivors often end up serving as the primary coordinators of their care, care that is frequently spread across a number of different medical specialties and physicians.Citation44 Having less time for other role and social activities in life may be an unavoidable consequence. Furthermore, our findings support that having a routine for all of one’s self-management may relieve feelings of physical/mental exhaustion. Prior qualitative studies with multi-morbid patients indicate that integration of self-care into one’s daily routine may be an effective way to manage competing demands and mitigate treatment burden.Citation23,Citation24 Medical factors such as diagnosis of a mental health condition and the number of diagnosed conditions, as well as formal education status, were not uniquely predictive of treatment burden or HRQL. Such factors may not be as predictive of survivor well-being when more specific psychosocial and health care-related factors are taken into account.
Practical implications of study findings
The reality for many cancer survivors, especially longer-term survivors 5+ years removed from a cancer diagnosis, is that they will be faced with other chronic medical conditions, either preexisting at the time of cancer diagnosis or newly emerging.Citation4 Hence, cancer survivorship care will need to be balanced with management of other chronic conditions, taking into account total treatment burden. Our study highlights the importance of confidence in one’s ability to self-manage (self-management self-efficacy) as well as the impact of required treatment and self-management on survivor well-being (treatment burden). Low health literacy, greater care fragmentation, and the absence of routines for self-management may also add to the burden of the survivor. Periodic monitoring of these factors that could begin during treatment and continue throughout survivorship might be helpful as a first step in helping identify survivors in need of intervention or extra attention.
More research is warranted to determine whether systematically assessing cancer survivors’ overall treatment burden and engaging supportive services or strategies to integrate these needs with their other ongoing self-care activities can be beneficial. If found to be effective, a focus on overall treatment burden might be considered as an additional element to address in the cancer survivor’s survivorship care plan (SCP) as it evolves over months or years. Currently, the SCP is usually developed by the oncology team and focuses exclusively on adjustment to and follow-up of the cancer.Citation1 A more holistically integrated SCP could involve inputs from both the oncology and primary care teams, be tailored to address the nuances of a complex health situation, and become a tool for promoting consistent and effective messaging to the cancer survivor. Another approach may be to develop a focus on overall treatment burden within a shared-care model of cancer follow-up.Citation3
Limitations
There are limitations to this study. First, generalizability of study findings may be limited by the small size and lack of diversity. We were able to identify a subset of 91 people with a prior cancer diagnosis from a larger prospective study of 443 people with MCCs. While small, the sample size was sufficient for the regression analyses used.Citation45 Furthermore, it is noteworthy that the regressions accounted for substantial amounts of variance in the treatment burden and HRQL outcomes assessed (from 36% to 45%). Study subjects were however largely white and educated, and persons with cognitive impairments were not represented as this was an exclusion criterion of the parent study given the length of the administered survey battery. Other selection biases may be present due to the relatively low rate of response to the survey in the parent study (30%). Second, our count of the number of diagnoses did not make use of a standard comorbidity index. We did not have access to every single medical diagnosis of each person, only those forming the inclusion criteria for the parent study. Hence, our count of diagnoses may have lacked precision. Third, due to the small sample size, we did not have adequate statistical power to test the exploratory path models using structural equation modeling (SEM). SEM tests the overall fit of a hypothesized path model and also allows examination of bidirectional relationships between variables (ie, reciprocal causality).Citation46 It is possible that self-efficacy and treatment burden are reciprocally related; however, a larger sample will be needed to test this. Finally, we conducted analyses on multi-morbid cancer survivors with a wide range of times since cancer diagnosis (from 1 to 40 years). Experiences may be somewhat different across various phases of survivorship (ie, reentry, early term, and long term).Citation2
Conclusion
Today, many cancer survivors are living with other chronic health conditions and must learn to balance cancer recovery with the demands of managing other health problems. We identified risk factors for poor adjustment in multi-morbid cancer survivors, including perceived treatment burden. These risk factors speak to the challenges inherent in self-managing a complex health situation. Standardized assessment of these factors could assist health care teams by alerting them of survivors in need of additional supports and/or intervention. In the long run, this could inform greater tailoring of care plans for the multi-morbid survivor that would include input from primary care, oncology, and any other relevant medical specialties. While advances in screening, diagnosis, and treatment are adding years to the life of the cancer survivor, it is equally important to prioritize adding life to the years.
Acknowledgments
The research reported in this manuscript was supported by the National Institute of Nursing Research of the National Institutes of Health (USA) under award number R01NR015441. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors thank Ms Ann Harris and the Mayo Clinic Survey Research Center for formatting, distribution, and receipt of the survey. They also thank Ms Kandace Lackore, Ms Sarah Jenkins, and Mr Richard Pendegraft for database support.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Cancer SocietyCancer Treatment & Survivorship Facts & Figures 2016-2017Atlanta, GAAmerican Cancer Society2016
- StantonALRowlandJHGanzPALife after diagnosis and treatment of cancer in adulthood: contributions from psychosocial oncology researchAm Psychol201570215917425730722
- RubinGBerendsenACrawfordSMThe expanding role of primary care in cancer controlLancet Oncol201516121231127226431866
- LeachCRWeaverKEAzizNMThe complex health profile of long-term cancer survivors: prevalence and predictors of comorbid conditionsJ Cancer Surviv20159223925125319681
- GrossCPGuoZMcAvayGJAlloreHGYoungMTinettiMEMultimorbidity and survival in older persons with colorectal cancerJ Am Geriatr Soc200654121898190417198496
- WeaverKEForsytheLPReeveBBMental and physical health-related quality of life among U.S. cancer survivors: population estimates from the 2010 National Health Interview surveyCancer Epidemiol Biomarkers Prev201221112108211723112268
- SevickMATrauthJMLingBSPatients with complex chronic diseases: perspectives on supporting self-managementJ Gen Intern Med200722Suppl 343844418026814
- EtonDTYostKJLaiJSDevelopment and validation of the patient experience with treatment and self-management (PETS): a patient-reported measure of treatment burdenQual Life Res201726248950327566732
- MayCMontoriVMMairFSWe need minimally disruptive medicineBMJ2009339b280319671932
- HaynesRBMcDonaldHPGargAXHelping patients follow prescribed treatment: clinical applicationsJAMA2002288222880288312472330
- VijanSHaywardRARonisDLHoferTPBrief report: the burden of diabetes therapy: implications for the design of effective patient-centered treatment regimensJ Gen Intern Med200520547948215963177
- HoPMRumsfeldJSMasoudiFAEffect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitusArch Intern Med2006166171836184117000939
- BoydCMWolffJLGiovannettiEHealthcare task difficulty among older adults with multimorbidityMed Care201452Suppl 3S118S12524561750
- BrodMHammerMChristensenTLessardSBushnellDMUnderstanding and assessing the impact of treatment in diabetes: the treatment-related impact measures for diabetes and devices (TRIM-Diabetes and TRIM-Diabetes device)Health Qual Life Outcomes2009718319740444
- PifferiMBushADi CiccoMHealth-related quality of life and unmet needs in patients with primary ciliary dyskinesiaEur Respir J201035478779419797134
- RasmussenJNChongAAlterDARelationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarctionJAMA2007297217718617213401
- TranVTMontoriVMEtonDTBaruchDFalissardBRavaudPDevelopment and description of measurement properties of an instrument to assess treatment burden among patients with multiple chronic conditionsBMC Med2012106822762722
- AroraNKJohnsonPGustafsonDHMcTavishFHawkinsRPPingreeSBarriers to information access, perceived health competence, and psychosocial health outcomes: test of a mediation model in a breast cancer samplePatient Educ Couns2002471374612023099
- FosterCBreckonsMCotterellPCancer survivors’ self-efficacy to self-manage in the year following primary treatmentJ Cancer Surviv201591111925028218
- HelgesonVSCohenSSocial support and adjustment to cancer: reconciling descriptive, correlational, and intervention researchHealth Psychol19961521351488681922
- HewittMRowlandJHMental health service use among adult cancer survivors: analyses of the National Health Interview surveyJ Clin Oncol200220234581459012454116
- Institute of MedicineHealth Literacy: A Prescription to End ConfusionWashington, DCNational Academies Press2004
- RidgewayJLEggintonJSTiedjeKFactors that lessen the burden of treatment in complex patients with chronic conditions: a qualitative studyPatient Prefer Adherence2014833935124672228
- RosbachMAndersenJSPatient-experienced burden of treatment in patients with multimorbidity – a systematic review of qualitative dataPLoS One2017126e017991628644877
- VogeliCShieldsAELeeTAMultiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costsJ Gen Intern Med200722Suppl 339139518026807
- ShippeeNDShahNDMayCRMairFSMontoriVMCumulative complexity: a functional, patient-centered model of patient complexity can improve research and practiceJ Clin Epidemiol201265101041105122910536
- SchwartzCEZhangJMichaelWEtonDTRapkinBDReserve-building activities attenuate treatment burden in chronic illness: the mediating role of appraisal and social supportHealth Psychol Open201851205510291877344029785278
- St SauverJLGrossardtBRYawnBPData resource profile: the Rochester epidemiology project (REP) medical records-linkage systemInt J Epidemiol20124161614162423159830
- BrownAWMoessnerAMMandrekarJDiehlNNLeibsonCLMalecJFA survey of very-long-term outcomes after traumatic brain injury among members of a population-based incident cohortJ Neurotrauma201128216717621121813
- ChamberlainAMMcNallanSMDunlaySMPhysical health status measures predict all-cause mortality in patients with heart failureCirc Heart Fail20136466967523625946
- GoodmanRAPosnerSFHuangESParekhAKKohHKDefining and measuring chronic conditions: imperatives for research, policy, program, and practicePrev Chronic Dis201310E6623618546
- WallstonKAOsbornCYWagnerLJHilkerKAThe perceived medical condition self-management scale applied to persons with HIV/AIDSJ Health Psychol201116110911520656769
- MitchellPHPowellLBlumenthalJA short social support measure for patients recovering from myocardial infarction: the ENRICHD social support inventoryJ Cardiopulm Rehabil200323639840314646785
- ChewLDGriffinJMPartinMRValidation of screening questions for limited health literacy in a large VA outpatient populationJ Gen Intern Med200823556156618335281
- HaysRDBjornerJBRevickiDASpritzerKLCellaDDevelopment of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global itemsQual Life Res200918787388019543809
- NormanGRStreinerDLBiostatistics: The Bare Essentials3rd edShelton, CTPeople’s Medical Publishing House2008
- CohenJStatistical Power Analysis for the Behavioral Sciences2nd edHillsdale, NJLawrence Erlbaum Associates1988
- BaronRMKennyDAThe moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerationsJ Pers Soc Psychol1986516117311823806354
- KennyDAMediation [webpage on the Internet]2018 Available from: http://davidakenny.net/cm/mediate.htmAccessed July 18, 2018
- SobelMEAsymptotic confidence intervals for indirect effects in structural equation modelsLeinhardtSSociological MethodologySan Francisco, CAJossey-Bass1982290312
- BanduraASelf-efficacy: The Exercise of ControlNew York, NYW.H. Freeman1997
- BaylissEAEllisJLSteinerJFBarriers to self-management and quality-of-life outcomes in seniors with multimorbiditiesAnn Fam Med20075539540217893380
- Paasche-OrlowMKWolfMSThe causal pathways linking health literacy to health outcomesAm J Health Behav200731Suppl 11926
- Institute of MedicineCommittee on Improving the Quality of Cancer Care. Addressing the challenges of an aging populationLevitLABaloghEPNassSJGanzPADelivering High Quality Cancer Care: Charting a New Course for a System in CrisisWashington, DCAcademies Press2013
- KleinbaumDGKupperLLMullerKEApplied Regression Analysis and Other Multivariable Models2nd edBoston, MAPWS-Kent1988
- PaxtonPMHippJRMarquart-PyattSNonrecursive Models: Endogeneity, Reciprocal Relationships, and Feedback LoopsWashington, DCSage Publications, Inc2011