
Abstract
Introduction
The aim of this study was to evaluate the effect of perioperative vitamin D levels in terms of functional results, patient-related outcome measures (PROMs) and infection risk after hip or knee replacement.
Materials and Methods
A systematic search in PubMed, Cochrane library, ScienceDirect and ClinicalTrials.gov was conducted according to the PRISMA guidelines from inception to January 2020.
Results
Eighteen studies with more than 8000 knee and 1500 hip joint arthroplasties were included. The mean follow-up ranged from 6 weeks to 1 year and mean patients’ age from 59.4 to 76 years. Hypovitaminosis was diagnosed in 26.7% of cases. Most studies did not find significant differences in pre- and postoperative functional results, PROMs and length of hospital stay between hypovitaminosis and euvitaminosis groups. Deficient patients may be at higher risk of postoperative joint stiffness. Patients suffering from hip and knee periprosthetic joint infection seem to have lower vitamin D levels compared to those with aseptic loosening of implants.
Conclusion
The necessity of pre-operative correction of vitamin D levels to achieve better functional results and minimize the risk of infection following hip and knee arthroplasty remains inconclusive. Extend of exposure to low vitamin D levels and comparison between outliers needs further evaluation.
Introduction
Vitamin D deficiency is the most common nutritional deficiency worldwide.Citation1 The incidence of hypovitaminosis D is rising globally, affecting approximately one billion people.Citation2 Staying indoors for prolonged periods, wearing clothes that cover the skin, and using sunscreen are some of the primary causes of this increasing epidemic, the repercussions of which remain obscure.Citation2
The metabolism of vitamin D is well described.Citation3 Vitamin’s D main role is the regulation of calcium metabolism by controlling its absorption by the small intestine. It promotes bone resorption by stimulating the activity of osteoclasts.Citation3 Vitamin D plays a determining role in muscle function through regulating the deposition of phosphorus in myocytes, in the metabolism of creatine phosphate as well as in muscle cells’ response to insulin and muscle action.Citation4 As a result, the role of vitamin D in bone resistance is crucial, promoting the stimulation of bone turnover and muscle function.Citation3
The proven interactions between Vitamin D and at least, 200 genes of the human genome reflect its complicated character and at the same time, open the way for new pathways of research.Citation2 In the recent years, the relevant literature has expanded to include discussions around the effects of the vitamin D on the health of the articular cartilage, on muscle function and the risk of falls in the elderly.Citation5,Citation6 Abnormal vitamin D levels have been associated with osteomalacic myopathy, impaired muscle strength, changes in gait, and muscle pain.Citation3,Citation7 Vitamin D is also known to regulate the production of the extracellular substance of chondrocytes and could thus, be potentially correlated with the pathogeny of osteoarthritis.Citation8 Moreover, supplementation of vitamin D seems to improve functional ability in osteoarthritic patients.Citation9,Citation10
The crucial role of vitamin D in optimizing the mechanical loading through its effect on muscle function and bone turnover has also been evaluated in the outcomes of total joint arthroplasty (TJA).Citation11–Citation28 A high prevalence of vitamin D deficiency is recorded among patients undergoing TJA due to osteoarthritis, giving rise to the hypothesis that perioperative levels of vitamin D might play a role in patients undergoing lower limb arthroplasty.Citation29,Citation30 Several studies have reported a correlation between vitamin D levels and functional status as well as the risk of complications following TJA with conflicting outcomes.Citation11–Citation14,Citation16 However, the literature is still inconsistent in this respect.
The purpose of this systematic review is to thoroughly evaluate the role of perioperative vitamin D levels in a) postoperative functional outcomes; b) patient related outcome measures (PROMs); and c) the risk of infection in patients undergoing knee or hip arthroplasty.
Materials and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.Citation31
Data Sources and Search Strategy
We systematically searched PubMed, Cochrane library and ScienceDirect from inception to January 2020. For registered, ongoing trials, a search was conducted on ClinicalTrials.gov. The reference lists of the relevant studies retrieved were also hand-screened for additional missing records.
The search terms used were “knee arthroplasty”, “hip arthroplasty” and “vitamin D”. Free text searching was combined with Medical Subject Headings terms, and the detailed search strategy utilized can be found in the Supplementary Table 1.
Inclusion and Exclusion Criteria
The search was limited to articles that were published in the English language. The inclusion criteria included randomised controlled trials, retrospective and prospective cohort studies as well as case-control studies that a) reported mean pre- and postoperative vitamin D values in patients undergoing knee or hip arthroplasty b) reported pre- and postoperative functional scores and PROMs for these patients and c) compared functional outcomes and PROMs between vitamin D deficient and sufficient patient groups. Case reports, reviews or conference presentations were excluded from the study.
Outcome Measures
The primary outcomes were the effect of vitamin D levels in the functional outcomes and PROMs following knee or hip arthroplasty. Secondary outcomes were comparison of a) survivorship b) length of stay (LOS) and c) complications, namely infection, between vitamin D sufficient and deficient patients undergoing knee or hip arthroplasty.
Study Selection and Data Extraction
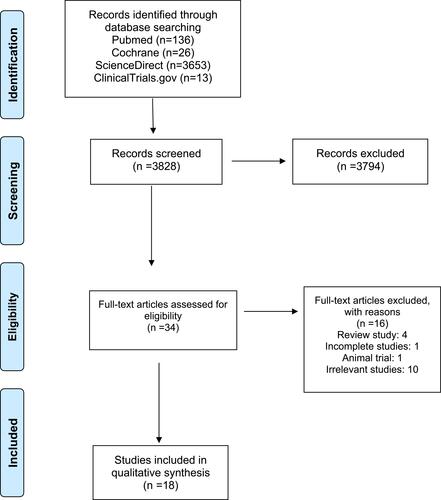
Two authors (PK and DK) independently searched the electronic databases for potentially relevant studies. After removing duplicates, the titles and abstracts of the retrieved records were screened for eligibility. In case of disagreement, a third investigator (ET) independently evaluated the study. Consequently, any discrepancies about the study selection process were solved by discussion and eligibility was defined by agreement with all authors. The various reasons for ineligible studies are presented in the flowchart of .
Figure 1 PRISMA flowchart illustrating the search strategy.
Data extraction was independently performed by two investigators (PK and EK) in duplicate for each eligible study. Data collected included the year of publication, study design, patients’ demographics, methodological features of the trial, PROMs, functional results, LOS and infection rate. Any potential disagreement was resolved by discussion between the reviewers. Where necessary, a third investigator (ET) was contacted, and independently extracted data before consensus was reached.
Data Analysis and Methodological Quality Assessment
We performed a narrative synthesis of the literature to evaluate the included data. The quality of the studies was assessed using the Newcastle – Ottawa Scale (NOS).Citation32 The NOS assesses the selection and comparability of study groups and ascertainment of the exposure-outcome using a “star system” where studies can be granted up to nine stars.
Results
Search Results
The initial search of the literature retrieved 3828 available articles. After removing duplicates and irrelevant studies by screening the title and abstract, 34 studies remained for review. Sixteen records were excluded because they were either incomplete studies, review studies or considered irrelevant after reading the full text. In total, 18 studies were included in the systematic review.Citation11–Citation28 Details of the study screening and selection are displayed in the flowchart of .
Methodological Quality Assessment
Five studies were of high methodological quality,Citation11,Citation14,Citation15,Citation18,Citation21 12 were of moderate qualityCitation12,Citation13,Citation16,Citation17,Citation19,Citation20,Citation22-Citation25,Citation27,Citation28 and 1 of low quality.Citation26
The results of the quality assessment are demonstrated in Supplementary Table 2.
Study Characteristics
The included studies were published between 2008 and 2018. There were ten retrospective case series, six prospective cohort studies, one retrospective and one prospective case-control study. The sample size ranged from 42 to 6593, with a mean follow-up from six weeks to one year. We extracted data from more than 8000 knee and 1500 hip replacements. The mean reported age of the patients ranged from 59.4 to 76 years. Seventeen studies reported on the prevalence of hypovitaminosis D;Citation11–Citation23,Citation25–Citation28 2598 out of 9720 (26.7%) patients were diagnosed with low vitamin D levels. The detailed descriptive characteristics of the included studies are presented in .
Table 1 Descriptive Characteristics of the Included Studies
Functional Outcomes in Knee Replacement
Seven studies reported functional outcomes and PROMs according to vitamin D status on 7360 knee arthroplasties ().Citation11–Citation15,Citation17,Citation25 The most commonly used PROMs were Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Knee Society Score (KSS). The majority of studies showed no significant differences in preoperative WOMAC score between deficient and sufficient patients.Citation13–Citation15 Only one study demonstrated a higher preoperative WOMAC score in vitamin D deficient patients.Citation12 Mean preoperative WOMAC score, as evaluated in four studies, ranging from 41.2 to 79.6 in hypovitaminosis group and 42.3 to 75.8 in euvitaminosis group.Citation12–Citation15
Table 2 Effect of Vitamin D in Functional Outcomes in Patients Undergoing Knee Arthroplasty
Postoperatively, three studies reported insignificant differences in overall WOMAC score between vitamin D deficient and sufficient patients.Citation12–Citation14 However, one study found that WOMAC stiffness subset had significantly less postoperative improvement in deficient patients.Citation14 The series with the longest follow up, revealed significantly worse functional results in deficient patients.Citation15 Mean postoperative WOMAC score ranged from 17.6 to 62.2 in the hypovitaminosis group and 15.8 to 52.5 in the euvitaminosis group.Citation12–Citation15
KSS was evaluated in three studies.Citation11,Citation12,Citation25 Mean preoperative KSS score ranged from 31.5 to 56.2 in vitamin D deficient and 37.1 to 58.9 in vitamin D sufficient patients. Two studies reported comparable preoperative outcomes in both deficient and sufficient groups.Citation11,Citation12 One study showed significantly lower KSS score in vitamin D deficient patients.Citation25
Postoperatively, there was no significant difference in KSS between groups in two studies.Citation12,Citation25 One study found that functional KSS was significantly lesser in the vitamin D deficient group than in the vitamin D non-deficient group postoperatively; clinical KSS score remained comparable in both groups.Citation11 Mean postoperative KSS score ranged from 74.6 to 91.9 in the hypovitaminosis group and 80.4 to 91.2 in the euvitaminosis group.Citation11,Citation12,Citation25
Among other functional scores, 12-Item Short Form Survey mental component summary (SFMCS), 12-Item Short Form Survey physical component summary (SFPCS), alternative step test (AST), timed up and go test (TUGT), six-meter walk test (SMT), sit to stand test (STS) and Activities-specific Balance Confidence Scale (ABC) did not differ significantly preoperatively between patients with low and normal vitamin D levels. Postoperatively, SFPCS, SFMCS, ABC, STS, TUGT remained comparable between the two groups. However, the mean time taken for postoperative AST and SMT (8.8 vs 7.7 s, p = 0.012) was significantly longer in the vitamin D-deficient group than in the vitamin D non-deficient group.Citation11,Citation12,Citation14 Mean pre- and postoperative scores are demonstrated in detail in Supplementary Table 3.
Functional Outcomes in Hip Replacement
Six studies reported functional outcomes and PROMs according to vitamin D status on 721 hip replacements ().Citation18–Citation22,Citation28 Preoperative WOMAC score showed no significant difference between sufficient and deficient patients.Citation18,Citation19,Citation21 Mean preoperative WOMAC score ranged from 40.4 to 59 in the deficient and from 43.5 to 54 in the sufficient group. Postoperatively, the mean WOMAC score remained comparable between the two groups.Citation19,Citation21 One study found that an increase in 25-hydroxyvitamin D3 (25(OH)D3) concentration six weeks postoperatively was correlated with improved hip function.Citation18
Table 3 Effect of Vitamin D in Functional Outcomes in Patients Undergoing Hip Arthroplasty
Harris Hip Score (HHS) was evaluated in two studies.Citation19,Citation20 One study found significantly higher preoperative HHS in vitamin D sufficient group.Citation20 The result of the second study was dependent on the vitamin D cut off point. When the threshold of hypovitaminosis was set in 20 ng/mL, the authors found comparable pre- and postoperative HHS independent of vitamin D levels. However, using the 30 ng/mL as a cut-off point, deficient patients found to have significantly lower pre- and postoperative HHS than sufficient patients.Citation19
Among the other functional outcomes evaluated, there was no association between serum vitamin D levels and Chair Stand Test (CST), 10 Meter Walking Test (10MWT), in-hospital functional milestones and 36-Item Short Form Survey (SF-36).Citation18,Citation21,Citation22 TUGT was recorded in two studies.Citation18,Citation21 One study showed a significant improvement in TUGT over time but independent of vitamin D status.Citation18 Contrary to these findings, a significant improvement in TUGT only in the low vitamin D group was revealed in another study.Citation21 Mean pre- and postoperative scores are demonstrated in detail in Supplementary Table 4.
LOS
Five studies reported on the duration of hospitalization according to preoperative vitamin D status.Citation13,Citation15,Citation22,Citation26,Citation27 Mean LOS was longer in the hypovitaminosis D group (3.8 to 15.6 days) compared to the euvitaminosis D group (3.6 to 11.3 days). The difference in LOS found to be statistically significant in two studies, with a mean difference between 1 to 4.3 days.Citation15,Citation25 ()
Table 4 Length of Hospital Stay Based on the Vitamin D Level of Groups of Patients
Survival Rate of the Prosthesis
Survivorship was recorded in one study with the largest sample.Citation17 Out of 6593 total knee arthroplasties (TKA), 868 suffered from hypovitaminosis D in this retrospective cohort study. At first-year follow-up, the incidence of revision arthroplasty for prosthesis explantation was found to be higher among the vitamin D deficient patients (OR, 2.97; 95% CI, 2.04–4.31; p<0.001). However, this was mainly attributed to periprosthetic joint infection (PJI) as the rates of non-infectious component revision were comparable between the two groups.
Complications - Risk of Infection
Six studies evaluated complication rate between vitamin D deficient and sufficient patients.Citation16,Citation17,Citation22,Citation24,Citation26,Citation27 They comprised of 7385 joint replacements; 6635 primary knee arthroplasties, 238 primary total hip arthroplasties (THA), 186 revision TKA, 186 revision THA, 109 unclarified primary, and 31 unclarified revision joint arthroplasties. Among the complications reported, PJI was the best described. Two studies reported that patients with low vitamin D levels are more likely to suffer from PJI.Citation17,Citation27 One study found no significant differences in complication rates between sufficient and deficient groups.Citation22
Other failures reported were postoperative deep venous thrombosis, myocardial infarction, cerebrovascular accident and postoperative stiffness requiring manipulation under anesthesia, all of which were found to be higher in vitamin D deficient patients as documented by one study only.Citation17
Vitamin D Levels in Patients with PJI vs Aseptic Loosening
Four studies compared vitamin D levels of patients following revision joint replacement due to infection or aseptic loosening with conflicting outcomes.Citation16,Citation24,Citation26,Citation27 Two of them concluded that patients undergoing revision for PJI were more likely to have low preoperative vitamin D levels as compared to those for aseptic loosening.Citation26,Citation27 One study revealed lower vitamin D levels in patients with aseptic loosening compared to those undergoing revision for PJI.Citation24 Another study found no significant differences as to vitamin D status in the 25(OH)D3 levels between these two groups.Citation16
Vitamin D Levels in Patients with PJI vs Primary Arthroplasty
Two studies compared vitamin D status in patients scheduled for primary or revision joint arthroplasty due to PJI.Citation16,Citation26 One of them reported non-significant differences (p=0.846), while the other one found a significantly lower vitamin D status in the PJI group (p<0.001).Citation16,Citation26
Vitamin D Levels in Patients with Aseptic Loosening vs Primary Arthroplasty
Two studies reported no significant differences in vitamin D status between patients undergoing primary or revision joint replacement due to aseptic loosening.Citation16,Citation26 ()
Table 5 Comparison of Vitamin D Levels Between Groups of Patients Undergoing Revision for Periprosthetic Join Infection or Aseptic Loosening or Primary Arthroplasty
Discussion
In this systematic review, we aimed to configure the potential role of vitamin D levels in lower limb arthroplasty in terms of PROMs, implant survivorship, LOS, and complications. The majority of studies did not report any differences in postoperative functional scores based on vitamin D status.Citation13,Citation14,Citation21,Citation22,Citation25,Citation28 It seems that patients with lower Vitamin D levels may be at higher risk of joint stiffness postoperatively.Citation17 Vitamin D may also be a protective factor against PJI.Citation26
The existing literature shows a high prevalence of vitamin D deficiency in patients with osteoarthritis undergoing arthroplasty.Citation25 The incidence of hypovitaminosis D in patients undergoing TKA ranges from 36.4% up to 76.2%.Citation12–Citation14,Citation23,Citation25,Citation33,Citation34 Similar rates were reported in patients scheduled for THA; ranging from 22% up to 82.8%.Citation19–Citation22,Citation28,Citation35 In our systematic review, we found 26.7% of patients undergoing joint replacements suffering from low vitamin D levels. This, however, might be an incidental finding attributed to factors, such as advanced age, osteoporosis and sun restriction.
The role of vitamin D in the pathogenesis of osteoarthritis could be explored further through analysis of preoperative data of patients undergoing TJA. Most studies reported no connection between hypovitaminosis D and preoperative physical function of the knee or hip joint.Citation11,Citation13-Citation15,Citation18,Citation19 These findings contrast with other studies reporting that deficient patients scheduled for TKA had worse preoperative WOMAC score.Citation12 The similar finding was reported in patients who had undergone THA as preoperative HHS was higher in sufficient patients scheduled for THA.Citation20 However, these are only point measurements and potentially, underestimate the disease course and the effect of hypovitaminosis D on the disease progress.
On the other hand, the postoperative progress of patients undergoing THA and TKA is dependent on a number of factors, including the patients’ age, the types of prostheses, and the disease duration.Citation36 The potential for a positive correlation between vitamin D levels and improved postoperative results is open to research and might, in fact, actually be given the possible positive effect of vitamin D on the function of muscular system and integration of prostheses.
Postoperatively, the outcomes regarding the knee function after ΤΚΑ remain inconclusive. More specifically, several studies showed comparable postoperative clinical results between vitamin D sufficient and deficient groups.Citation12,Citation14 Contrary to this finding, many studies showed an association between low vitamin D levels and worse postoperative clinical outcomes after TKA, such as KSS & AST as well as stiffness subcategory of WOMAC score.Citation11,Citation17 The short follow-up period and the inability to measure any potential vitamin D intake are the main drawbacks of these series. Moreover, the absence of comparability as regards the preoperative levels of vitamin D, the disease duration, the type of prosthesis, and the surgical methods all reduce the reliability of the results.
As for the postoperative function of the hip joint, the results are equivocal. There seems to be a positive association between vitamin D levels and improved postoperative PROMs.Citation18,Citation20 A weak association has also been found between vitamin D deficiency and a negative change in peak extension and peak power generation when analyzing the gait patterns after THA.Citation28 Once again, the exclusion of the most severe cases, the short follow-up period and the absence of comparability in regard to prostheses type and surgical methods all affect the reliability of the studies. So further research is needed to determine the long-term effects of vitamin D deficiency in patients undergoing hip arthroplasty.
Unfortunately, there is limited literature evidence on the effect of vitamin D on implant survival and the ways in which the vitamin can prolong prostheses survivorship.Citation17 It might be the case that it is associated with higher osseointegration yet, this primarily concerns uncemented prostheses. A sole study demonstrated that vitamin D deficiency was an independent risk factor for prosthesis explantation following knee arthroplasty.Citation17 However, this was mainly attributed to infectious reasons as the non-infectious component revision rate was found to be comparable between deficient and sufficient groups.Citation17
The role of vitamin D in the prevention of septic conditions is well-documented.Citation37–Citation40 It prevents the overexpression of inflammatory cytokines, such as interleukin-6 and C-reactive protein and is a crucial mediator in the aggregation of leukocytes, local inflammation, and anti-bacterial responses in innate immunity.Citation41 The levels of vitamin D have also been inversely associated with the risk of infectious complications after surgery.Citation42,Citation43 In orthopaedic procedures, the evidence is relatively scarce.Citation16,Citation24,Citation26,Citation27 Several studies found lower vitamin D levels in patients with PJI compared to those with aseptic loosening.Citation26,Citation27 Interestingly, there was one study that reported higher vitamin D levels in patients with PJI.Citation24 However, the absence of measurements of serum vitamin D in the postoperative follow-up negatively impacts upon the quality of these findings.
The main limitation of this systematic review is the different vitamin D reference range reported in the studies. The classification of vitamin D status based on serum 25-hydroxyvitamin has not been unanimously accepted, which complicates the interpretation of the data.Citation44 What is thus, needed is the standardization of the definition of vitamin D insufficiency. Another concern that could be raised is the retrospective design in the majority of the studies. High-quality randomized control trials are necessary to prove the effectiveness of vitamin D on PROMs following lower limb arthroplasty. A third objection is the comparability of the groups. Functional results following TJA are multifactorial. There was no clear indication in the studies that vitamin is connected to some extent to the outcomes.
Conclusions
In conclusion, our study identified a high prevalence of hypovitaminosis in osteoarthritis patients undergoing joint arthroplasty. Although a positive correlation of vitamin D status and postoperative functional outcomes is reported in some studies, the necessity of preoperative correction of vitamin D remains an open question. Moreover, despite the acknowledged role of vitamin D in infectious diseases, it is yet to be clarified whether supplementation of vitamin D has a protective effect in PJI.
Abbreviations
TJA, total joint arthroplasty; PROMs, patient-related outcome measures; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; LOS, length of stay; NOS: Newcastle – Ottawa Scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; KSS, Knee Society Score; SFPCS, 12-Item Short Form Survey mental component summary; SFMCS, 12-Item Short Form Survey physical component summary; AST, alternative step test; TUGT, timed up and go test; SMT, six-meter walk test; STS, sit to stand test; ABC, Activities-specific Balance Confidence Scale; 25(OH)D3, 25-hydroxyvitamin D3; HHS, Harris Hip Score; CST, Chair Stand Test; 10MWT,10 Meter Walking Test; SF36, 36-Item Short Form Survey; TKA, total knee arthroplasty; THA, total hip arthroplasty; PJI, periprosthetic joint infection.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
Τhe authors would like to thank Theodora Panagiotidou for proofreading the article.
Disclosure
The authors declare that they have no conflict of interest.
Additional information
Funding
References
- Mithal A, Wahl DA, Bonjour J-P, et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int. 2009;20(11):1807–1820. doi:10.1007/s00198-009-0954-6
- Neal S, Sykes J, Rigby M, Hess B. A review and clinical summary of vitamin D in regard to bone health and athletic performance. Phys Sportsmed. 2015;43(2):161–168. doi:10.1080/00913847.2015.1020248
- Bikle D. Vitamin D and bone. Curr Osteoporos Rep. 2012;10(2):151–159. doi:10.1007/s11914-012-0098-z
- Dawson-Hughes B. Vitamin D and muscle function. J Steroid Biochem Mol Biol. 2017;173:313–316. doi:10.1016/j.jsbmb.2017.03.018
- Tomlinson PB, Joseph C, Angioi M. Effects of vitamin D supplementation on upper and lower body muscle strength levels in healthy individuals. A systematic review with meta-analysis. J Sci Med Sport. 2015;18(5):575‐580. doi:10.1016/j.jsams.2014.07.022
- Dhaliwal R, Aloia JF. Effect of vitamin D on falls and physical performance. Endocrinol Metab Clin North Am. 2017;46(4):919‐933. doi:10.1016/j.ecl.2017.07.004
- Wicherts IS, van Schoor NM, Boeke AJP, et al. Vitamin D status predicts physical performance and its decline in older persons. J Clin Endocrinol Metab. 2007;92(6):2058–2065. doi:10.1210/jc.2006-1525
- Cao Y, Winzenberg T, Nguo K, Lin J, Jones G, Ding C. Association between serum levels of 25-hydroxyvitamin D and osteoarthritis: a systematic review. Rheumatology (Oxford). 2013;52(7):1323–1334. doi:10.1093/rheumatology/ket132
- Sanghi D, Mishra A, Sharma AC, et al. Does vitamin D improve osteoarthritis of the knee: a randomized controlled pilot trial. Clin Orthop Relat Res. 2013;471(11):3556–3562. doi:10.1007/s11999-013-3201-6
- Manoy P, Yuktanandana P, Tanavalee A, et al. Vitamin D supplementation improves quality of life and physical performance in osteoarthritis patients. Nutrients. 2017;9(8):799. doi:10.3390/nu9080799
- Shin K-Y, Park KK, Moon S-H, Yang IH, Choi H-J, Lee W-S. Vitamin D deficiency adversely affects early post-operative functional outcomes after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2017;25(11):3424–3430. doi:10.1007/s00167-016-4209-8
- Maniar RN, Patil AM, Maniar AR, Gangaraju B, Singh J. Effect of preoperative vitamin D levels on functional performance after total knee arthroplasty. Clin Orthop Surg. 2016;8(2):153–156. doi:10.4055/cios.2016.8.2.153
- Lee A, Chan SKC, Samy W, Chiu CH, Gin T. Effect of hypovitaminosis D on postoperative pain outcomes and short-term health-related quality of life after knee arthroplasty: a cohort study. Medicine. 2015;94(42):e1812. doi:10.1097/MD.0000000000001812
- Allain TJ, Beresford PA, Newman JH, Swinkels A. Vitamin D levels in patients undergoing knee arthroplasty: does vitamin D status effect postoperative outcomes? E Spen Eur E J Clin Nutr Metab. 2008;3(1):e17–e21. doi:10.1016/j.eclnm.2007.10.002
- Jansen J, Tahmassebi J, Haddad FS. Vitamin D deficiency is associated with longer hospital stay and lower functional outcome after total knee arthroplasty. Acta Orthop Belg. 2017;83(4):664–670.
- Zajonz D, Prager FL, Edel M, et al. The significance of the vitamin D metabolism in the development of periprosthetic infections after THA and TKA: a prospective matched-pair analysis of 240 patients. Clin Interv Aging. 2018;13:1429–1435. doi:10.2147/CIA.S171307
- Hegde V, Arshi A, Wang C, et al. Preoperative vitamin D deficiency is associated with higher postoperative complication rates in total knee arthroplasty. Orthopedics. 2018;41(4):e489–e495. doi:10.3928/01477447-20180424-04
- Visser E, de Roos NM, Oosting E, Endenburg SC, Dronkers JJ. Association between preoperative vitamin D status and short-term physical performance after total hip arthroplasty: a prospective study. Ann Nutr Metab. 2018;73(3):252–260. doi:10.1159/000492938
- Lavernia CJ, Villa JM, Iacobelli DA, Rossi MD. Vitamin D insufficiency in patients with THA: prevalence and effects on outcome. Clin Orthop Relat Res. 2014;472(2):681–686. doi:10.1007/s11999-013-3172-7
- Nawabi DH, Chin KF, Keen RW, Haddad FS. Vitamin D deficiency in patients with osteoarthritis undergoing total hip replacement: a cause for concern? J Bone Joint Surg Br. 2010;92(4):496–499. doi:10.1302/0301-620X.92B3.23535
- Unnanuntana A, Saleh A, Nguyen JT, et al. Low vitamin D status does not adversely affect short-term functional outcome after total hip arthroplasty. J Arthroplasty. 2013;28(2):315–322.e2. doi:10.1016/j.arth.2012.04.027
- Unnanuntana A, Rebolledo BJ, Gladnick BP, et al. Does vitamin D status affect the attainment of in-hospital functional milestones after total hip arthroplasty? J Arthroplasty. 2012;27(3):482–489. doi:10.1016/j.arth.2011.05.023
- Maier GS, Maus U, Lazovic D, Horas K, Roth KE, Kurth AA. Is there an association between low serum 25-OH-D levels and the length of hospital stay in orthopaedic patients after arthroplasty? J Orthop Traumatol. 2016;17(4):297–302. doi:10.1007/s10195-016-0414-y
- Signori V, Romanò CL, De Vecchi E, Mattina R, Drago L. May osteoarticular infections be influenced by vitamin D status? An observational study on selected patients. BMC Musculoskelet Disord. 2015;16:183. doi:10.1186/s12891-015-0648-5
- Jansen JA, Haddad FS. High prevalence of vitamin D deficiency in elderly patients with advanced osteoarthritis scheduled for total knee replacement associated with poorer preoperative functional state. Ann R Coll Surg Engl. 2013;95(8):569–572. doi:10.1308/rcsann.2013.95.8.569
- Maier GS, Horas K, Seeger JB, Roth KE, Kurth AA, Maus U. Is there an association between periprosthetic joint infection and low vitamin D levels? Int Orthop. 2014;38(7):1499–1504. doi:10.1007/s00264-014-2338-6
- Traven SA, Chiaramonti AM, Barfield WR, et al. Fewer complications following revision hip and knee arthroplasty in patients with normal vitamin D levels. J Arthroplasty. 2017;32(9S):S193–S196. doi:10.1016/j.arth.2017.02.038
- Cunha BM, da Cunha BM, Gava AD, de Oliveira SB, de David AC, Dos Santos-Neto LL. Vitamin d is related to gait recovery after total hip arthroplasty: a prospective analysis. Gait Posture. 2016;50:96–101. doi:10.1016/j.gaitpost.2016.08.014
- Garfinkel RJ, Dilisio MF, Agrawal DK. Vitamin D and its effects on articular cartilage and osteoarthritis. Orthop J Sports Med. 2017;5(6):2325967117711376.
- Piuzzi NS, George J, Khlopas A, et al. High prevalence and seasonal variation of hypovitaminosis D in patients scheduled for lower extremity total joint arthroplasty. Ann Transl Med. 2018;6(16):321. doi:10.21037/atm.2018.08.21
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700
- Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses; 2016. Available from http://www.ohri. ca/programs/clinical epidemiology/oxford.asp2008. Accessed December 2016.
- Reid D, Toole BJ, Knox S, et al. The relation between acute changes in the systemic inflammatory response and plasma 25-hydroxyvitamin D concentrations after elective knee arthroplasty. Am J Clin Nutr. 2011;93(5):1006–1011. doi:10.3945/ajcn.110.008490
- Kelly MA, Campbell J, Sheahan J, Murphy P. Vitamin D insufficiency in patients undergoing total knee arthroplasty in ireland. Ir Med J. 2017;110(10):649.
- Glowacki J, Hurwitz S, Thornhill TS, Kelly M, LeBoff MS. Osteoporosis and vitamin-D defi-ciency among postmenopausal women with osteoarthritis undergoing total hip arthro-plasty. J Bone Joint Surg Am. 2003;85-A:2371–2377. doi:10.2106/00004623-200312000-00015
- Dennis DA, Komistek RD, Stiehl JB, Walker SA, Dennis KN. Range of motion after total knee arthroplasty: the effect of implant design and weight-bearing conditions. J Arthroplasty. 1998;13(7):748‐752. doi:10.1016/s0883-5403(98)90025-0
- Torres C, Sánchez de la Torre M, García-Moruja C, et al. Immuno-phenotype of vitamin D receptor polymorphism associated to risk of HIV-1 infection and rate of disease progression. Curr HIV Res. 2010;8(6):487–492.3. doi:10.2174/157016210793499330
- Abhimanyu A, Coussens AK. The role of UV radiation and vitamin D in the seasonality and outcomes of infectious disease. Photochem Photobiol Sci. 2017;16(3):314–338. doi:10.1039/C6PP00355A
- Trongtrakul K, Feemuchang C. Prevalence and association of vitamin D deficiency and mortality in patients with severe sepsis. Int J Gen Med. 2017;10:415–421. doi:10.2147/IJGM.S147561
- Tiwari S, Pratyush DD, Gupta SK, Singh SK. Vitamin D deficiency is associated with inflammatory cytokine concentrations in patients with diabetic foot infection. Br J Nutr. 2014;112(12):1938–1943. doi:10.1017/S0007114514003018
- Shojaei M, Sabzeghabaei A, Helia Valaei Barhagh H,Soheil Soltani S. The correlation between serum level of vitamin D and outcome of sepsis patients; a cross-sectional study. Arch Acad Emerg Med. 2019;7(1):e1.
- Braun A, Chang D, Mahadevappa K, et al. Association of low serum 25-hydroxyvitamin D levels and mortality in the critically ill. Crit Care Med. 2011;39(4):671–677. doi:10.1097/CCM.0b013e318206ccdf
- Matthews LR, Ahmed Y, Wilson KL, Griggs DD, Danner OK. Worsening severity of vitamin D deficiency is associated with increased length of stay, surgical intensive care unit cost, and mortality rate in surgical intensive care unit patients. Am J Surg. 2012;204(1):37–43. doi:10.1016/j.amjsurg.2011.07.021
- Thacher TD, Clarke BL. Vitamin D insufficiency. Mayo Clin Proc. 2011;86(1):50‐60. doi:10.4065/mcp.2010.0567