
Abstract
Background
Patient delay in presenting to hospital with stroke symptoms remains one of the major barriers to thrombolysis treatment, leading to its suboptimal use internationally. Educational interventions such as mass media campaigns and community initiatives aim to reduce patient delays by promoting the signs and symptoms of a stroke, but no consistent evidence exists to show that such interventions result in appropriate behavioral responses to stroke symptoms.
Methods
A systematic literature search and narrative synthesis were conducted to examine whether public educational interventions were successful in the reduction of patient delay to hospital presentation with stroke symptoms. Three databases, MEDLINE, CINAHL, and PsycINFO, were searched to identify quantitative studies with measurable behavioral end points, including time to hospital presentation, thrombolysis rates, ambulance use, and emergency department (ED) presentations with stroke.
Results
Fifteen studies met the inclusion criteria: one randomized controlled trial, two time series analyses, three controlled before and after studies, five uncontrolled before and after studies, two retrospective observational studies, and two prospective observational studies. Studies were heterogeneous in quality; thus, meta-analysis was not feasible. Thirteen studies examined prehospital delay, with ten studies reporting a significant reduction in delay times, with a varied magnitude of effect. Eight studies examined thrombolysis rates, with only three studies reporting a statistically significant increase in thrombolysis administration. Five studies examined ambulance usage, and four reported a statistically significant increase in ambulance transports following the intervention. Three studies examining ED presentations reported significantly increased ED presentations following intervention. Public educational interventions varied widely on type, duration, and content, with description of intervention development largely absent from studies, limiting the potential replication of successful interventions.
Conclusions
Positive intervention effects were reported in the majority of studies; however, methodological weaknesses evident in a number of studies limited the generalizability of the observed effects. Reporting of specific intervention design was suboptimal and impeded the identification of key intervention components for reducing patient delay. The parallel delivery of public and professional interventions further limited the identification of successful intervention components. A lack of studies of sound methodological quality using, at a minimum, a controlled before and after design was identified in this review, and thus studies incorporating a rigorous study design are required to strengthen the evidence for public interventions to reduce patient delay in stroke. The potential clinical benefits of public interventions are far-reaching, and the challenge remains in translating knowledge improvements and correct behavioral intentions to appropriate behavior when stroke occurs.
Introduction
Thrombolysis with tissue plasminogen activator within a 3- to 4.5-hour window following onset of ischemic stroke is associated with improved patient outcome and reduction in disability,Citation1 with the chances of a favorable outcome falling twofold for every 90-minute delay in treatment.Citation2 Despite its proven efficacy, provision rates remain suboptimal internationally.Citation3 Interventions targeted at the public aim to reduce patient delay in presentation with stroke symptoms, and thus play an important role in improving treatment rates for thrombolysis in ischemic stroke. Patient delay in accessing medical care has been cited as the biggest barrier to thrombolysis treatment for ischemic stroke,Citation4–Citation6 with prehospital delays estimated to account for up to 68% of total delay from onset to treatment.Citation7 The aim of public-focused educational interventions is to reduce patient delay by educating the public of the common signs and symptoms of stroke and the correct course of action should symptoms occur.
Much of the published literature to date that examines the effectiveness of public educational interventions is concerned with nonbehavioral intervention end points where no definitive behavior occurs, such as stroke knowledge and intentions to call emergency medical services (EMS).Citation8–Citation11 However, the association between stroke knowledge and improved time to presentation is poor,Citation12–Citation14 and recent guidelines highlight that the only acceptable outcome of a health intervention is a behavioral outcome or a measurable consequence of the target behavior:Citation15 ie, where the target behavior occurs following the intervention. Outcomes of a public stroke education intervention need to provide a measure of the clinical impact of the intervention. Measurable behavioral outcomes of an intervention, such as stroke onset to door (OTD) times, or measurable consequences such as thrombolysis rates, emergency department (ED) presentations with stroke symptoms, or ambulance dispatches help provide an estimate of the real effectiveness of an intervention of this type. The aim of this review was to examine the effectiveness of interventions that aim to reduce prehospital delay by systematically reviewing studies containing such behavioral end points.
Methods
Search strategy
Three electronic databases, MEDLINE, CINAHL, and PsycINFO, were searched from database start date to October 24, 2014 for educational interventions targeted at the public that aim to reduce prehospital delay and that had a measurable behavioral outcome. The key search term “stroke” was accompanied with all combinations of the terms “thrombolysis”, “tPA”, “actilyse”, “alteplase”, “delay”, “intervention”, “education”, “paramedic”, “ambulance”, “emergency”, “awareness”, “campaign”, and “time”. The Google Scholar search engine and reference lists for included papers were additionally searched in order to identify studies that may not have been identified through the database searches. Reference lists for identified review papers were scanned and cross-referenced with studies identified from the primary search. Two authors independently screened and reviewed abstracts and titles for relevant papers. Disagreements were discussed with a third reviewer.
Inclusion and exclusion criteria
Studies were included if a measurable behavioral outcome of a public educational intervention to reduce prehospital delay was assessed. Randomized controlled trials (RCTs), non-RCTs, and prospective, retrospective, and cross-sectional studies were included. Studies were excluded if the intervention outcome was stroke knowledge, attitudes, behavioral intentions, or any other nonbehavioral outcome. Studies were also excluded if the article was a review or discussion paper, if an English or German translation of the paper was not available, or if the article was not published in full in a peer-reviewed journal.
Data extraction and synthesis
The following data were extracted: author, publication year, location and setting, sample characteristics, intervention duration and content, behavioral outcomes assessed, and intervention results. Given the heterogeneity of study types, meta-analysis was not indicated, and a qualitative narrative synthesis was conducted.
Outcomes
The main outcomes of interest were reduction in OTD time, thrombolysis rates, activation of ambulance transports, ED presentations with stroke symptoms, and patient mortality.
Quality assessment
Critical appraisal of primary studies is an essential feature of systematic reviews; however, no consensus exists on the “gold standard” appraisal method for assessing methodological quality.Citation16 The Crowe Critical Appraisal Tool (CCAT)Citation17 was selected for the purposes of this review. It is a generic critical appraisal tool that has been reported to be simple to implement and applicable to all research designs in health, with obtained scores being directly comparable. Studies are scored from 0 to 5 on eight dimensions: preamble, introduction, design, sampling, data collection, ethical matters, results, and discussion. Each dimension includes up to three subcategories with a number of descriptors marked as present, absent, or not applicable. The total score, ranging from 0 to 40, may be displayed as a percentage. The CCAT demonstrates good reliability andCitation18,Citation19 construct validity,Citation20 comprehensively assesses the key aspects of research, and can be utilized across different research designs.
Results
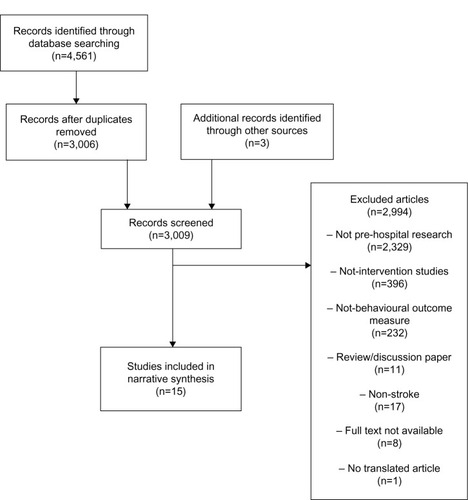
Database searches identified 4,561 citations, with 3,006 remaining after duplicate removal. Three studies were additionally identified through Google Scholar searches. Fifteen studies met the inclusion criteria. outlines the screening process and the reasons for study exclusion.
Figure 1 Flow chart of studies screened, excluded (with reasons), and included in the review.
displays the main characteristics of the final studies. A single cluster RCTCitation21 was identified, and two time series design studiesCitation22,Citation23 were identified. Three studiesCitation24–Citation26 were controlled before and after studies, and five studiesCitation27–Citation31 were uncontrolled before and after studies. There were two retrospective observational studiesCitation32,Citation33 and two prospective observational studies.Citation34,Citation35 The main outcome of interest, reduction in prehospital delay, was assessed in 13 of the studies.Citation21,Citation23–Citation31,Citation34,Citation35 Rates of thrombolysis were assessed in eight studies.Citation21,Citation22,Citation24,Citation26,Citation29,Citation31,Citation33,Citation34 Five studiesCitation23,Citation25,Citation29,Citation30,Citation32 examined ambulance dispatches for stroke, three studiesCitation22,Citation23,Citation28 examined ED presentations, and two studiesCitation21,Citation26 examined patient mortality as behavioral indicants of intervention effectiveness.
Table 1 Summary of data extracted from studies included in review
Study quality was assessed independently by two reviewers using the CCAT, with disagreements discussed with a third reviewer. All papers were rated on the eight dimensions of the CCAT, and a total score for each study was derived from the average score of the independent ratings and expressed as a percentage. Overall, the methodological quality was mixed. As only one study was identified as an RCT design, the majority of studies lacked quality in research design, management of bias, and sampling. Data collection methods and comprehensive reporting of results were also identified as poor quality for some studies.
Study population
Data collection settings were the hospital ED in the majority of cases, with information obtained mainly from patient medical records or hospital stroke registries. One studyCitation35 obtained additional data from the patient and/or family, with another studyCitation32 retrospectively examining patients with an ambulance dispatch for stroke in an urban ambulance service over a 10-year period. In three studies,Citation27,Citation31,Citation35 patients were recruited as part of a thrombolysis trial.
Intervention characteristics
Intervention content
summarizes the content of the interventions described in the included studies. Intervention descriptions varied considerably between studies. Five studies described mass media campaigns aimed at the general public, all using a specific slogan to promote stroke awareness. The Australian,Citation32 UK,Citation22,Citation33,Citation36 and IrishCitation23 studies described the FAST (Face, Arm, Speech, Time) campaign, which highlights three main symptoms of stroke and the need to contact EMS immediately. The Canadian studyCitation28 utilized the SUDDENS campaign, highlighting ‘sudden’ onset of weakness, trouble speaking, vision, headache, and/or dizziness. The remaining studies described both public and professional education campaigns that were broadcast at a local and regional level. The professional campaigns focused on reducing prehospital and in-hospital delays, from initiation of EMS contact to treatment in the acute hospital setting. These were aimed at professionals involved in acute stroke care, including paramedics, ED staff, and general practitioners. Three studiesCitation24,Citation26,Citation27 used educational messages that described thrombolysis treatment, emphasizing the time-dependent nature of the treatment in addition to its efficacy. The RCTCitation21 posted educational packs to inhabitants aged over 50 years in 48 randomized zip codes, each containing a personalized letter outlining signs and symptoms of stroke, a bookmark, and a sticker outlining the main symptoms and EMS contact details.
Table 2 Intervention content of included studies
Intervention development
Only the intervention by Morgenstern et alCitation24 comprehensively described the stages of development of the intervention. The community intervention component involved role-modeling of the appropriate response to stroke symptoms by publicly advertising stroke survivors in the community and their successful experience of thrombolysis. The purpose of community role-modeling was to demonstrate that immediate stroke response was associated with better outcome. Morgenstern et alCitation24 also developed a local advisory board and conducted a telephone survey (n=656) for the purposes of identifying factors related to intention to react rapidly to signs of stroke. The authors additionally conducted focus groups with stroke survivors to assess factors that contributed to delay in time to hospital presentation with stroke. The professional education component involved systems change in hospitals, change of perceived norms in the medical community, and reinforcement of behavior change.
Patient delay times
Thirteen studies examined change in patient prehospital delay times as an outcome following a public educational intervention. The majority of studies reported statistically significant effects in terms of reducing patient delay, with ten studies reporting a statistically significant reduction in prehospital delay following the intervention, with the magnitude of change varying per study.
RCT study
The RCTCitation21 reported a statistically significant reduction of 27% in prehospital delay in women in the intervention group, with no change observed in men.
Controlled before and after studies
The controlled study by Morgenstern et alCitation24 involving community and professional intervention in the US reported an overall decrease in prehospital delay; however, the decrease was general and not specific to the intervention group. Hence, the public intervention was not associated with this overall decrease. Two Chinese controlled before and after studies reported significant reductions in patient delay. The study by Chen et alCitation25 evidenced a significant yearly decline in median OTD time from 280 minutes in 2008 to 79 minutes in 2010 in the intervention community, with no changes reported in the controlled community. Sun et alCitation26 reported a reduction of 2.2 hours in the intervention group for OTD time, with a significantly greater proportion (26%) in the intervention group arriving to hospital in less than 3 hours.
Time series study
An Irish time series analysis by Mellon et alCitation23 reported no effect of the FAST campaign on OTD time over a 12-month period.
Uncontrolled before and after studies
A US study by Alberts et alCitation27 conducted in 1994 reported a statistically significant linear reduction in time to arrival over the course of the study, from 3.2 hours to 1.5 hours. However, the authors caution that although the percentage of patients arriving early increased, the time from stroke onset to first medical contact did not, suggesting that the delay reduction might be attributed to faster paramedic response. A German study conducted in 1995 by Müffelmann et alCitation31 reported an overall statistically significant reduction in time to presentation from 8 hours to 5 hours. A study by Luiz et al,Citation30 also conducted in Germany, reported a 62% reduction in median delay time following intervention, from 368 minutes to 140 minutes. Another US study by Wojner-Alexandrov et alCitation29 reported no significant decrease in delay in the active intervention phase; however, there was a significant difference in patients presenting <120 minutes in the active intervention phase as compared with the preintervention data. A final US study by Hodgson et alCitation28 examined time to presentation in categories of less than 5 hours and less than 2.5 hours. A statistically significant increase in both categories was reported following the intervention; however, the magnitude of effect was small in both instances.
Prospective observational studies
One US study by Barsan et alCitation35 was conducted in 1992 before routine thrombolysis administration; thus, despite the reported effect of increased presentations under 24 hours from 40% to 85%, the intervention encouraged treatment within 8 hours and examined presentation within 24 hours of symptom onset as a behavioral outcome. Therefore, early presentation within the current thrombolytic treatment window was not examined. A study in Germany by Schmidt et alCitation34 reported a decrease in median delay from 12 to 3.2 hours. This decrease was statistically nonsignificant in the small sample studied; however, it had clinical significance as the largest reported reduction in OTD time of approximately 9 hours.
Retrospective observational study
The retrospective UK study by Addo et alCitation33 analyzing stroke events over 10 years examined the change in the proportion of patients who delayed pre and post a year-long intervention with the FAST campaign and reported no change in the proportion of patients arriving within 3 hours or a decrease in prehospital delay as a result of a public stroke awareness campaign.
Increase in thrombolysis rates
Eight studies examined thrombolysis rates as a behavioral outcome measure, with only three studies reporting a statistically significant increase in thrombolysis rates following a public educational intervention.
Interestingly, the RCTCitation21 reported no significant difference in thrombolysis rates between the intervention and control groups. The time series analysis by Flynn et alCitation22 analyzed data from the Safe Implementation of Thrombolysis in Stroke UK database, which included data from 27 hospital sites across England. Findings showed an overall increase in thrombolysis rates over the study period, with specific increases observed following waves 1 and 3 of the FAST campaign. The controlled before and after study by Moregenstern et alCitation24 reported a statistically significant increase in thrombolysis rates from 2.21% to 8.65% for ischemic stroke in the intervention community following an educational intervention, with no change observed in the control community. A follow-up studyCitation36 within this population reported a sustained increase in thrombolysis rates (11.2%) in the intervention community at 6 months postintervention. The controlled before and after study by Sun et alCitation26 reported a 4.8% increase in thrombolysis rates in the intervention community following a community-based intervention. An uncontrolled before and after study by Wojner-Alexandrov et alCitation29 examined the change in thrombolysis rates in nine treatment centers from the preintervention to the active intervention phase. No consistent trend was observed over the intervention phase, although four hospitals reported a rise in thrombolysis (only one of these being a statistically significant rise), while two hospitals in this cohort reported decreased thrombolysis rates. Another uncontrolled before and after study by Müffelmann et alCitation31 reported an increase in thrombolysis cases, from one case to nine cases, following a public education campaign. The prospective study by Schmidt et alCitation34 reported an overall increase in thrombolysis rates but did not provide statistical analysis of the reported change. The retrospective study by Addo et alCitation33 reported no significant difference in thrombolysis rates before or after a public stroke awareness campaign.
Activation of ambulance transport
Ambulance transports for stroke were outcome measures in five studies, with four reporting statistically significant increases in ambulance transportations for stroke following an educational intervention. The controlled study by Chen et alCitation25 reported that the percentage of patients calling EMS increased per year from 2008, with a 10.8% overall increase noted and an increased proportion evident in the intervention community in 2010. The study by Bray et alCitation32 examined the impact of a multimedia educational intervention on the proportional increase in ambulance dispatches over a 10-year period. The authors reported a yearly significant increase in ambulance dispatches in the month after the annual stroke awareness week from 2007 once the message to call an ambulance in response to stroke was added to the existing media message. The study by Wojner-Alexandrov et alCitation29 reported a significant increase in paramedic transports for stroke during the intervention phase as compared with the preintervention phase. The retrospective study by Luiz et alCitation30 reported a 4.5% increase in EMS transports for stroke postintervention. The same study also examined the time taken from symptom onset to EMS activation (ie, calling the EMS telephone number) and found a significant reduction of 79% in median activation time to 54 minutes.
ED presentations
Three studies examined ED presentations with stroke as an outcome measure, with all studies reporting some statistically significant effects, with increases in ED presentations for stroke observed. One before and after study by Hodgson et alCitation28 examined ED presentations with stroke symptoms and reported a mean increase in ED presentations over the study period. The authors reported that exposure to the mass media campaign accounted for 9% of the total variance in ED admissions for stroke, 15% of the variance for presentations under 5 hours, and 5% of the variance for presentations within 2.5 hours. The UK time series analysis by Flynn et alCitation22 of all ED activity for England from May 2007 to February 2011Citation22 revealed that there was a general increase in ED presentations over the study period. However, when ED trends immediately following the FAST campaign were examined, only the time period following wave 1 of the FAST campaign evidenced a significant increase. The second time series analysis by Mellon et alCitation23 reported similar findings to the UK analyses. The Irish data examined ED presentations with stroke symptoms over a 12-month period, with significant increases in ED presentations only observed following wave 1 of the FAST campaign.
Mortality
The RCTCitation21 examined the percentage of deaths during hospital stay between the intervention and control groups, reporting no statistical difference in mortality between the groups. A controlled before and after study by Sun et alCitation26 reported no difference in the 90-day fatality rate between the intervention and control groups; however, interestingly, the intervention group had significantly higher functional outcome scores, measured on the Barthel Index, than the control group at 90 days poststroke.
Discussion
This review examined the effectiveness of public interventions aimed at reducing patient prehospital delay in acute ischemic stroke. Outcomes of interest were focused on patient behavior (patient delay, EMS use, and ED presentation) or measurable consequences of behavior (thrombolysis rates and mortality). The findings suggest that educational interventions aimed at the public have some positive effects on reducing patient delay to hospital presentation and other behavioral indicants such as ambulance use, ED presentation with suspected stroke, and thrombolysis rates. However, results must be interpreted with caution, as large heterogeneity was evident between study designs and methodology.
Interventions such as multimedia campaigns have demonstrated efficacy in increasing stroke knowledge and awareness and the intention to respond to stroke as an emergency.Citation37–Citation39 However, bridging the gap between behavioral intention and behavior itself remains a challenge in acute stroke care and has similarly been identified as a key challenge in other health contexts, such as acute myocardial infarction.Citation40 The intervention in this review that evidenced the largest and, more crucially, more sustained behavioral change in thrombolysis rates involved a scientifically based, multifaceted behavioral intervention that was developed from focus groups with stroke survivors in order to identify themes and issues that contribute to delay.Citation24 The theory-based strategy involved role-modeling of response to stroke by promoting community figures who were stroke survivors and demonstrated that immediate response to stroke symptoms results in a better outcome. Furthermore, this type of intervention did more than just demonstrate signs and symptoms to the public; it outlined the time-dependent nature of successful treatments for ischemic stroke, which highlights this strategy as a possible key component in interventions to reduce delay in presentation with stroke symptoms.
The intervention in the RCT studyCitation21 did not have an observable impact on delay behavior. This finding has been similarly reported in RCT studies examining the effect of interventions to reduce delay in presentation with symptoms of an acute myocardial infarction. Stroke researchers can potentially learn from the more established acute myocardial infarction literature in order to improve treatment outcomes for acute ischemic stroke. Both conditions are life-threatening events with acute onset and similar mechanism of infarction. Successful treatment involves revascularization, and hence both have similar need for time-dependent intervention. A large randomized clinical trialCitation41 to reduce prehospital delay in acute coronary syndrome (n=5,322) found that a one-to-one educational and counseling intervention with patients with documented heart disease at 2-year follow-up resulted in no change to prehospital delay times, although the experimental group was more likely to call emergency services and self-medicate with aspirin following symptom onset. Secondary analysis of this cohortCitation42 aimed to characterize the patients who best responded to the intervention, in order to understand the mechanisms by which interventions work. It was found that decreasing anxiety was associated with prehospital delay reduction, and authors suggest that tailoring interventions to target psychosocial and emotional responses to acute onset of symptoms may be more effective than addressing knowledge, attitudes, or intention. Methods such as community role-modeling of stroke survivors may be useful in reducing potential anxiety and removing potential psychosocial barriers to timely acute stroke care.
Seven studies in this review that reported significant effects described interventions that targeted both professional and public behavior. Professional education may have contributed to improved thrombolysis rates through improved prehospital paramedic response and in-hospital systemic delay reductions. This interaction effect was not examined in any study presented here, and it is therefore difficult to draw conclusions on which element (public or professional) was most effective. Patient recognition and action in the wake of stroke symptom onset is the first step in the symptom delay trajectory, and the studies included in this review focused on public interventions that targeted this step in the onset to treatment delay trajectory. The next two stages, from initiation of medical contact to hospital arrival, and from arrival to treatment, are out of the patient’s control and rely on prompt professional action to reduce delays to treatment. Significant advances in prehospital management of stroke by paramedic protocols and EMS systems, coupled with in-hospital improvements in the management of stoke, have translated into shorter overall onset to treatment times. For example, a recent single-center studyCitation43 reported a door-to-needle time of 20 minutes, which was attributed to concurrent in-hospital systemic changes and the employment of a prehospital notification system, which resulted in a smoother transition from prehospital to in-hospital emergency care. A multicenter interventionCitation44 also reported a clinically significant increase in thrombolysis use in the target population following a multicomponent intervention, although this increase was not statistically significant. A shorter door-to-needle time affords the stroke patient slightly more time to recognize and respond accordingly to stroke symptoms without risk of missing the thrombolysis treatment window. The findings from the time series analyses included in this review provide further evidence for this gradual improvement in pre and in-hospital acute management of stroke. Flynn et alCitation22 highlight that in the study period from 2007 to 2011, there were significant increases in ED presentations for stroke, coupled with a decline in time-consuming general practitioner-referred stroke cases, and an increase in thrombolysis rates over time. These service improvements occurred in parallel with improvements in patient response attributable to the FAST campaign. Changing the public perception of acute stroke is a challenging and lengthy process involving large, heterogeneous populations. Perhaps a sustainable reduction in onset-to-needle time may be best achieved over a shorter time frame by improving in-hospital acute stroke care, as in-hospital interventions have the advantage of focusing on a single network or organization in a controlled environment, such as the ED or EMS network.
This review had some limitations. The heterogeneity of the included studies limited the comparability of the interventions, and critical appraisal of the included studies revealed that potential bias or confounders were not successfully addressed in the majority of studies. Only one RCT was identified, and therefore methodological deficiencies of included studies limit the weight that can be given to the demonstrated effects. Some of the included studies also retrospectively examined intervention effects as a secondary analysis to a larger study, which again decreases the methodological rigor. Studies in this area should utilize, at a minimum, a controlled before and after design or interrupted time series design if an RCT design is not feasible,Citation42 in order to associate any observed changes with the specified intervention.
Conclusions
In conclusion, this review found that interventions to educate the public on the correct response to stroke symptoms evidenced varying degrees of success, with most interventions successful in initiating correct public responses when stroke occurred. Studies that were particularly successful in achieving reductions in prehospital delay adopted a combined multilevel approach to education, incorporating mass media, targeted community education, and professional education. Sustained reduction in patient delay and increased thrombolysis administration were achieved by an intervention that specifically promoted the use of thrombolysis for stroke and its associated benefits. There is a need for well-designed research trials with clearly described intervention components to provide evidence for the effectiveness of interventions to reduce delayed presentation with stroke symptoms.
Acknowledgments
This project was funded by the Health Research Board in Ireland through the HRB PhD Scholars Programme in Health Services Research, Grant No PhD/2007/16.
Disclosure
The authors report no conflicts of interest in this work.
References
- HackeWKasteMBluhmkiEThrombolysis with alteplase 3 to 4.5 hours after acute ischaemic strokeNEMJ200835913171329
- LeesKRBluhmkiEvon KummerRTime to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trialsLancet20103751695170320472172
- SchumacherHCBatemanBTBoden-AlbalaBUse of thrombolysis in acute ischaemic stroke: analysis of the Nationwide Inpatient Sample 1999–2004Ann Emerg Med2007509910717478010
- EvensonKRRosamondWDMorrisDLPrehospital and in-hospital delays in acute stroke careNeuroepidemiology200120657611359072
- EvensonKRForakerRERosamondWDA comprehensive review of prehospital and in-hospital delay times in acute stroke careInt J Stroke2009418719919659821
- KwanJ HPSandercockPA systematic review of barriers to delivery of thrombolysis for acute strokeAge Ageing20043311612114960425
- WesterPRadbergJLundgrenBPeltonenMFactors associated with delayed admission to hospital and in-hospital delays in acute stroke and TIA: a prospective, multicenter studyStroke199930140489880386
- SilverFRubiniFBlackDHodgsonCAdvertising strategies to increase public awareness of the warning signs of strokeStroke2003341965196912855823
- ReevesMJHoganJGRaffertyAPKnowledge of stroke risk factors and warning signs among Michigan adultsNeurology2002591547155212451195
- ReevesMJRaffertyAPAranhaAATheisenVChanges in knowledge of stroke risk factors and warning signs among Michigan adultsCerebrovasc Dis20082538539118349531
- FogleCOserCTroutmanPPublic education strategies to increase awareness of stroke warning signs and the need to call 911J Public Health Manag Pract200814E17E2218408540
- FussmanCRaffertyAPLyon-CalloSMorgensternLBReevesMJLack of association between stroke symptoms knowledge and intent to call 911Stroke2010411501150720466995
- CarrollCHobartJFoxCTeareLGibsonJStroke in Devon: knowledge was good, but action was poorJ Neurol Neurosurg Psychiatry20047556757115026498
- ReevesMJReducing the delay between stroke onset and hospital arrival: is it an achievable goal?J Am Heart Assoc201213e00247723130150
- MichieSJohnstonMTheories and techniques of behaviour change. Developing a cumulative science of behaviour changeHealth Psychol Rev2012616
- MojaLPTelaroED’AmicoRMoschettiICoeLLiberatiAAssessment of methodological quality of primary studies by systematic reviews: results of the metaquality cross sectional studyBMJ2005330105315817526
- CroweMSheppardLA review of critical appraisal tools show they lack rigor: alternative tool structure is proposedJ Clin Epidemiol201164798921130354
- CroweMSheppardLCampbellAReliability analysis for a proposed critical appraisal tool demonstrated value for diverse research designsJ Clin Epidemiol20126537538322078576
- CroweMSheppardLCampbellAComparison of the effects of using the Crowe Critical Appraisal Tool versus informal appraisal in assessing health research: a randomised trialInt J Evid Based Healthc2011944444922093394
- CroweMSheppardLA general critical appraisal tool: an evaluation of construct validityInt J Nurs Stud2011481505151621802686
- Müller-NordhornJWegscheiderKNolteCPopulation-based intervention to reduce prehospital delays in patiens with cerebrovascular eventsArch Intern Med20091691484149019752406
- FlynnDFordGRodgersHPriceCSteenNThomsonRGA time series evaluation of the FAST national stroke awareness campaign in EnglandPLoS One20149e10428925119714
- MellonLHickeyADoyleFDolanEWilliamsDCan a media campaign change health service use in a population with stroke symptoms? Examination of the first Irish stroke awareness campaignEmerg Med J Epub7262013
- MorgensternLBStaubLChanWImproving delivery of acute stroke therapy: the TLL Temple Foundation Stroke ProjectStroke20023316016611779906
- ChenSSunHZhaoXEffects of comprehensive education protocol in decreasing pre-hospital stroke delay among Chinese urban community populationNeurol Res201335552252823594430
- SunXZhangNWangTPublic and professional education on urgent therapy for acute ischaemic stroke: a community-based intervention in ChangshaNeurol Sci2013342131213523504220
- AlbertsMJPerryADawsonDVBertelsCEffects of public and professional education on reducing the delay in presentation and referral of stroke patientsStroke1992233523561542895
- HodgsonCLindsayPRubiniFCan mass media influence emergency department visits for stroke?Stroke2007382115212217540967
- Wojner-AlexandrovAWAlexandrovAVRodriguezDPersseDGrottaJCHouston Paramedic and Emergency Stroke Treatment and Outcomes Study (HoPSTO)Stroke2005361512151815961712
- LuizTMoosmannAKochCBehrensSDaffertshoferMEllingerKOptimized logistics in the prehospital management of acute strokeAnasthesiol Intensivmed Notfallmed Schmerzther200136735741 German11743669
- MüffelmannBGlahnJKunzSBusseOStrategies for early admission of stroke patientsNervenarzt199566111115 German7715749
- BrayJEMosleyIBaileyMBargerBBladinCStroke public awareness campaigns have increased ambulance dispatches for stroke in Melbourne, AustraliaStroke2011422154215721757668
- AddoJAyisSLeonJRuddAGMcKevittCWolfeCDelay in presentation after an acute stroke in a multiethnic population in South London: the South London Stroke RegisterJ Am Heart Assoc201213e00168523130144
- SchmidtNKHuwelJWeisnerBCauses of a prolonged prehospital phase in patients admitted to a stroke unit. Can it be influenced by campaigns to educate the public?Nervenarzt20057618118515300319
- BarsanWBrottTBroderickJHaleyELevyDEMarlerJUrgent therapy for acute stroke. Effects of a stroke trial on untreated patientsStroke199425213221377974533
- MorgensternLBBartholomewKGrottaJStaubLKingMChanWSustained benefit of a community and professional intervention to increase acute stroke therapyArch Intern Med20031632198220214557217
- WallHKBeaganBMO’NeillJFoellKMBoddie-WillisCLAddressing stroke signs and symptoms through public education: the Stroke Heros Act FAST campaignPrev Chronic Dis20085A4918341784
- SchneiderATPancioliAMKhouryJCTrends in community knowledge of the warning signs and risk factors for strokeJAMA200328934334612525235
- MiyamatsuNKimuraKOkamuraTIguchiYNakayamaHToyotaAEffects of public education by television on knowledge of early stroke symptoms among a Japanese population aged 40 to 74: years a controlled studyStroke20124354554922052523
- MoserDKKimbleLPAlbertsMJReducing delay in seeking treatment by patients with acute coronary syndrome and stroke: a scientific statement from the American Heart Association Council on Cardiovascular Nursing and Stroke CouncilJ Cardiovasc Nurs20072232634317589286
- DracupKMcKinleySRiegelBMoserDKMeischkeHDoeringLVA randomised clinical trial to reduce patient prehospital delay to treatment in acute coronary syndromeCirc Cardiovasc Qual Outcomes2009252453220031889
- RiegelBElmiAMoserDKWho listens to our advice? A secondary analysis of data from a clinical trial testing an intervention designed to decrease delay in seeking treatment for acute coronary syndromePatient Educ Couns201185e33e3821300515
- MeretojaAStrbianDMustanojaSTatlisumakTLindsbergPJKasteMReducing in-hospital delay to 20 minutes in stroke thrombolysisNeurology201279430631322622858
- DirksMNiessenLWvan WijngaardenJDPromoting thrombolysis in acute ischemic strokeStroke20114251325133021393587