Abstract
Hypertension in the elderly is one of the main risk factors of cardiovascular and cerebrovascular diseases. Knowledge regarding the mechanisms of hypertension and specific considerations in managing hypertensive elderly through pharmacological intervention(s) is fundamental to improving clinical outcomes. Recent clinical studies in the elderly have provided evidence that angiotensin II type 1 (AT1) receptor antagonists can improve clinical outcomes to a similar or, in certain populations, an even greater extent than other classical arterial blood pressure-lowering agents. This newer class of antihypertensive agents presents several benefits, including potential for improved adherence, excellent tolerability profile with minimal first-dose hypotension, and a low incidence of adverse effects. Thus, AT1 receptor antagonists represent an appropriate option for many elderly patients with hypertension, type 2 diabetes, heart failure, and/or left ventricular dysfunction.
Introduction
Hypertension is a crucial, modifiable risk factor for cardiovascular and cerebrovascular diseases and remains a leading cause of preventable morbidity and mortality in most developed countries.Citation1 In 2000, it was estimated that 26% of adults worldwide (972 million) had hypertension, and this number is expected to increase to 29.2% (1.56 billion) by 2025.Citation2 The incidence of hypertension increases worldwide with the progression of an aging population, making it the most dominant and common morbid condition in the elderly. In the Framingham Heart Study, it was estimated that normotensive adults aged 55–65 years had more than a 90% lifetime risk of developing hypertension during the rest of their life.Citation3 Hence, age is considered to be the most crucial causative factor for hypertension and cardiovascular death.Citation4
Clinical trials have demonstrated that treatment of hypertension in the elderly prevents heart failure, reduces the risk of stroke, and prolongs life.Citation5–Citation9 Notably, (patho) physiological modifications linked to both aging and high arterial blood pressure must be taken into consideration when choosing an appropriate blood pressure-lowering treatment for the elderly.Citation10 For example, characteristic changes that occur in the elderly with high blood pressure are decreased cardiac output, increased peripheral resistance due to age-related decline of vascular compliance, impaired baroreceptor sensitivity, and reduced intravascular volume.Citation11,Citation12
Major benefits of antihypertensive therapy are related to lowering and controlling of blood pressure through lifestyle modification(s) and drug therapy.Citation13,Citation14 Therapeutic management of hypertension in the elderly includes five main classes of drugs that have been clinically studied and successfully used over several decades. These classes include angiotensin II type 1 (AT1) receptor antagonists (angiotensin receptor blockers or ARBs), angiotensin-converting enzyme inhibitors (ACEIs), β-adrenergic receptor antagonists (β-blockers), calcium channel blockers, and thiazide diuretics.Citation15 The diversity of these medications has fuelled debates regarding which class of antihypertensive is most suitable as a first-line therapeutic agent.Citation16 In addition, although the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends two-drug combinations in patients who have significantly elevated blood pressure (ie, 20 mm Hg above their systolic blood pressure goal and/or 10 mm Hg above diastolic blood pressure goal), this recommendation may not be prudent in older patients due to the risk of orthostatic hypotension.Citation17 In addition, multiple drug therapies may increase the risk of other undesirable adverse effects and problems with drug adherence, which are important issues of consideration in pharmacotherapy of the elderly. Medications used in the elderly should ideally meet the following criteria: i) once- or twice-daily administration, ii) low incidence of side effects, and iii) low cost with available equivalent drugs of similar effectiveness.Citation18
The purpose of this review is to discuss the pharmacology of angiotensin receptor antagonists, particularly as it relates to the elderly, and describe data that support the use of these agents in older hypertensive patients. Information on the use of other antihypertensive drugs in the elderly is reviewed elsewhere.Citation19–Citation22
Overview of the use of AT1 receptor antagonist in the elderly
Angiotensin receptor antagonists act on the final step of the renin–angiotensin–aldosterone system (RAAS) by selectively blocking the AT1 receptor and preventing the effects of angiotensin II mediated by this receptor (). Blockade of the AT1 receptor by angiotensin receptor blockers (ARBs) results in a dose-dependent fall of peripheral resistance without a significant change in the heart rate or cardiac output.Citation23 ARBs offer a variety of advantages for elderly hypertensive patients; they have excellent tolerability, have minimal drug interactions, and may be dosed once daily.Citation24 Because of these factors, medication adherence may also be optimized, which is particularly important considering that polypharmacy is common among hypertensive elderly.Citation25
Figure 1 Schematic illustration of the RAAS and the main pathways by which RAAS regulates cardiovascular function.Citation148,Citation149
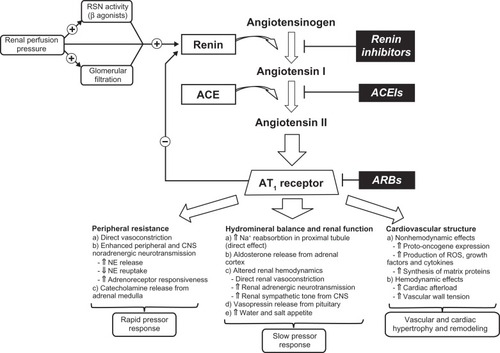
The integral role of circulatory RAAS in maintaining normal hemodynamic status is well documented.Citation26–Citation28 It is also known that activity of this system declines with age, which is mainly due to reduction of renin activity and plasma aldosterone concentrations.Citation29,Citation30 Notably, increased activity of RAAS has not proven to be the major cause of primary (essential) hypertension, unlike in progression of atherosclerosis and vascular disease, where angiotensin II, the main effector molecule of the system, is highly implicated.Citation31 Most physiological actions of angiotensin II, including smooth muscle contraction, release of aldosterone, and cell growth and proliferation, are due to activation of the AT1 receptor.Citation32 In addition, excessive binding of angiotensin II to this receptor is one of the main pathological mechanisms leading to sustained vasoconstriction, cardiac hypertrophy, fibrosis, endothelial dysfunction, heart failure, arrhythmias, and atherogenesis.Citation33–Citation38
The first therapeutic agents that targeted the RAAS in treatment of hypertension were ACEIs, which were developed more than 30 years ago.Citation39 ACEIs have been demonstrated to be very effective in the treatment of hypertension, as well as other cardiovascular and renal diseases.Citation40,Citation41 However, some of the side effects of ACEIs and their inability to block alternative pathways of angiotensin II generation (eg, chymase in the heart) were reasons for the development of AT1 receptor antagonists, which specifically block the effects of angiotensin II mediated through the AT1 receptor.Citation42
A common side effect of ACE inhibitors is cough. Although the mechanism(s) behind ACEI-induced cough is not fully understood, it may involve elevated levels of bradykinin and stimulation of vagal C fibers.Citation43 The frequency of cough varies among different patient populations. The rate appears to be around 10% in white patients but may be as high as 44% in Asian patients.Citation44 Cough is more common among women than men, tends to be dry, is mildly annoying, and often requires cessation of therapy.Citation45
Angioedema is a rare but potentially life-threatening side effect of ACEIs.Citation43,Citation46 It is characterized by localized swelling of the lips, mouth, tongue, throat, nose, or other parts of the face.Citation43 The mechanism of this side effect appears to involve bradykinin and/or one of its metabolites. The rate of angioedema has been reported to be 1 per 1000 (0.1%) in primarily white patients but appears to be higher in black patients.Citation47,Citation48
ARBs were introduced in the mid-1990s as more selective drugs for RAAS inhibition with an improved safety and tolerability profile.Citation49,Citation50 The first orally active selective AT1 receptor antagonist approved by the US Food and Drug Administration in 1995 was losartan. Over the past two decades, it has undergone extensive pharmacological and clinical investigations.Citation51,Citation52 This was followed by development of several other ABRs, including valsartan, irbesartan, candesartan, telmisartan, eprosartan, and olmesartan, which differ by modifications in their chemical structure and have somewhat different pharmacological properties.Citation53
Clinical studies of angiotensin AT1 receptor antagonists in hypertension and related cardiovascular disorders
ARBs are widely used for the treatment of hypertension because of well-documented safety and efficacy. A meta-analysis by the Blood Pressure Lowering Treatment Trialists’ Collaboration group indicates that similar to other commonly used blood pressure-lowering regimens, various AT1 receptor blockers result in a similar reduction of total major cardiovascular events through management of elevated arterial blood pressure.Citation54 A recent meta-analysis of 108 studies in 464,000 patients by Law et al also confirmed that all the major classes of blood pressure-lowering drugs have a similar effect on reducing coronary heart disease events and stroke for a given reduction in blood pressure.Citation55
Heart failure and left ventricular dysfunction are two of the main outcomes of uncontrolled hypertension in elderly patients.Citation56 Overactivation of the RAAS and the sympathetic nervous system are crucial in the pathogenesis and progression of chronic heart failure.Citation57 For this reason, treatments targeting the RAAS, typically with an ACE inhibitor or ARB, in patients with heart failure have been shown to substantially improve mortality and morbidity.Citation58–Citation60
The Evaluation of Losartan in the Elderly (ELITE) trial was the first moderately long (48 weeks) randomized study comparing losartan with captopril in 722 elderly patients aged ≥65 years with New York Heart Association (NYHA) class II–IV heart failure and an ejection fraction of ≤40%.Citation61 After 48 weeks, patients in both groups had similar improvement in NYHA functional class compared with baseline (80% of losartan-treated patients vs 81% of captopril-treated patients), and hospitalizations were less frequent with losartan than with captopril treatment (22.2% vs 29.7%). However, significantly more patients withdrew from captopril than from losartan (21% vs 12%; P = 0.002), primarily due to captopril-related side effects such as cough, angioedema, and rash. Moreover, patients in the losartan group had a 46% reduction in all-cause mortality in comparison with those in the captopril group (P = 0.035), which was primarily due to a reduced incidence of sudden cardiac death. Notably, the reduction in mortality with ACEI or ARB treatment was not the primary endpoint of this study. As a result, a large-scale randomized trial, the Losartan Heart Failure Survival Study (ELITE II), was initiated.
ELITE II was a double-blind randomized controlled trial in 3152 patients (mean age 71 years) with NYHA class II–IV heart failure and an ejection fraction of ≤40% and was designed to test the superiority of losartan to captopril in improving survival and tolerability.Citation62 After a median follow-up of 555 days, there was no significant difference in all-cause mortality (17.7% losartan vs 15.9% captopril), sudden death (8.2% losartan vs 6.4% captopril), or resuscitated arrests (9.0% losartan vs 7.3% captopril). However, significantly fewer patients discontinued treatment in the losartan group because of adverse effects (9.7% vs 14.7%; P = 0.001) or cough (0.3% vs 2.7%).
The Valsartan Heart Failure Trial was the first large trial to study the effects of additional ARB treatment on standard heart failure therapy.Citation63 In this study, 5010 patients (mean age 62.7 years) with NYHA class II–IV and an ejection fraction of ≤40% were randomized to receive valsartan or placebo in addition to standard therapy. After an average follow-up of 23 months, there was no difference in overall mortality between the two groups (19.7% valsartan vs 19.4% placebo). However, valsartan treatment was associated with a reduced risk for a combined endpoint of mortality plus morbidity, cardiac arrest with resuscitation, hospitalization for heart failure, or intravenous inotropic or vasodilator therapy (28.8% valsartan vs 32.1% placebo; P = 0.009). This reduction was mainly driven by a 24% reduction in risk of hospitalization for heart failure in the valsartan group.Citation63 Notably, a subgroup of 366 patients (7%) in this study were not treated with an ACEI, which allowed comparison of valsartan as monotherapy with placebo.Citation64 The results from this subgroup indicated a significant reduction in both all-cause mortality (30%; P = 0.01) and all-cause hospitalizations (45%; P = 0.0002). Exclusion of this subgroup of patients made the observed overall reduction in the combined endpoint of mortality and morbidity no longer significant for the whole study.
The Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity (CHARM) trials compared candesartan with placebo (in parallel, double-blind, randomized controlled studies) in three distinct populations with NYHA class II–IV heart failure. Patients were randomized to one of three trials: those who were not receiving ACEIs because of intolerance (CHARM-Alternative), patients with similar symptoms who were already receiving an ACEI (CHARM-Added), and patients with left ventricular ejection fractions ≥40% (CHARM-Preserved).Citation65 The CHARM-Alternative trial included 2028 patients (average age 66.5 years).Citation66 During a median follow-up of 33.7 months, the addition of candesartan to patients who were not on an ACEI was associated with a 30% decrease in risk of cardiovascular death or hospital admissions for heart failure compared with placebo (covariate adjusted hazards ratio, 0.70; P < 0.0001). In addition, study drug withdrawal rates were similar in both groups (30% vs 29%). In the CHARM-Added trial, the addition of candesartan to ongoing ACEI therapy was assessed in 2548 patients (mean age 64 years) with heart failure. After a median follow-up of 41 months, there was a significant reduction in cardiovascular death or hospital admissions for heart failure in the candesartan group compared with placebo (38% vs 42%; unadjusted hazard ratio [HR] 0.85; P = 0.011).Citation68 However, study-drug withdrawal rates due to adverse events or laboratory abnormalities were significantly higher in the candesartan group compared with placebo (24.2% vs 18.3%; P = 0.0003). The CHARM-Preserved trial assessed the effect of candesartan in 3023 patients (mean age 67.1 years) with a preserved ejection fraction (ie, ≥40%). At the end of 36.6 months, there was no difference in cardiovascular death (170 vs 170), but there were fewer hospital admissions for heart failure with candesartan (230 vs 279; P = 0.017).Citation67 Composite outcomes that included nonfatal myocardial infarction and nonfatal stroke also showed similar results to the primary outcomes in both groups (25.6% candesartan vs 28.4% placebo; P = 0.078; covariate adjusted HR 0.86; P = 0.037). Overall results of the CHARM trials indicate that in patients with heart failure and left ventricular dysfunction, candesartan is an effective alternative to ACEIs in patients not able to tolerate an ACEI. In addition, routine use of an ARB in addition to standard therapy, which includes ACEIs, or in elderly patients with heart failure and preserved left ventricular function does not appear justified due to a lack of efficacy and/or additional side effects.
The Optimal Trial in Myocardial Infarction with Angiotensin II Antagonist Losartan (OPTIMAAL) was another large randomized trial that studied the superiority of losartan to captopril in decreasing all-cause mortality in high-risk patients.Citation69 In the study, 5477 patients (mean age 67.4 years) who had confirmed acute myocardial infarction and heart failure during the acute phase or a new Q wave anterior infarction or reinfarction were randomly assigned and titrated to a target dose of losartan (50 mg once daily) or captopril (50 mg three times daily) as tolerated. After an average follow-up of 2.7 years, there were no significant differences in all-cause mortality (18.2% vs 16.4%), sudden death or resuscitated arrests (8.7% vs 7.4%), or nonfatal reinfarctions (14.0% vs 13.9%) between the two treatment groups. Similar to previous findings, losartan was better tolerated than captopril with fewer patient withdrawals (17% vs 23%; P < 0.0001).
The Valsartan in Acute Myocardial Infarction trial (VALIANT) was a double-blind, randomized study that compared the effects of valsartan in patients who had suffered a recent myocardial infarction.Citation70 In this study, 17,703 patients (mean age 64 years) were randomized to receive valsartan, valsartan plus captopril, or captopril in addition to standard therapy within 0.5–10 days after an acute myocardial infarction. After a median follow-up of 24.7 months, there were no differences in mortality or fatal and nonfatal cardiovascular events between the three groups (valsartan group 19.9%; valsartan plus captopril group 19.3%; captopril group 19.5%). The HR for death in the valsartan group as compared with the captopril group was 1.00 (97.5% confidence internal [CI] 0.90–1.11; P = 0.98), and the HR for death in the valsartan plus captopril group as compared with the captopril group was 0.98 (97.5% CI 0.89–1.09; P = 0.73). Notably, the valsartan plus captopril group had the most drug-related adverse effects compared with the other two groups (34.8% valsartan plus captopril group vs 29.4% valsartan group vs 28.4% captopril group; P < 0.05 for differences between the captopril group).
The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET) involved 25,620 patients (mean age 66.4 years) with established coronary artery, peripheral vascular or cerebrovascular disease, or diabetes with end-organ damage, who after a 3-week single-blind run-in period underwent double-blind randomization with the ACEI ramipril (n = 8576), ARB telmisartan (n = 8542), or both drugs combined (n = 8502).Citation71 The primary purpose of this study was to determine whether telmisartan was superior or inferior to ramipril and whether the combination was superior to ramipril monotherapy in reducing morbidity and mortality in patients at high risk of having a vascular event or diabetes but without heart failure. After a median follow-up of 56 months, there was no statistically significant difference in death from cardiovascular causes, myocardial infarction, and stroke or in hospitalization for heart failure between the treatment groups (16.5% ramipril vs 16.7% telmisartan vs 16.3% combination). Compared with ramipril, telmisartan was associated with lower rates of cough (1.1% vs 4.2%; P < 0.001) and angioedema (0.1% vs 0.3%; P = 0.01) and higher rates of hypotensive symptoms (1.7% vs 2.6%; P < 0.001). In addition, compared with ramipril alone, the combination was associated with more hypotensive symptoms (1.7% vs 4.8%; P < 0.001), syncope (0.2% vs 0.3%; P = 0.03), diarrhea (0.1% vs 0.5%; P < 0.001), and renal dysfunction (0.7% vs 1.1%; P < 0.001). Thus, although telmisartan was demonstrated to be noninferior to ramipril in reducing cardiovascular events in patients at high risk of an event, the combination of an ACEI and an ARB did not result in additive benefits and was associated with increased side effects.
The Telmisartan Randomized Assessment Study in ACE Intolerant Subjects With Cardiovascular Disease (TRANSCEND) was one of the components of ONTARGET, which involved 5926 high-risk patients who exhibited clinical intolerance to ACEIs.Citation72 After a 3-week run-in period, patients were randomized to receive telmisartan (n = 2954) or placebo (n = 2972), and the same primary outcome as in ONTARGET was assessed. After a median follow-up of 56 months, there was no difference in the primary outcome of cardiovascular death, myocardial infarction, stroke, or hospitalization for heart failure between telmisartan and placebo (HR 0.92; 95% CI 0.81–1.05; P = 0.216). The composite of cardiovascular death, myocardial infarction, or stroke was lower in telmisartan group compared with placebo after adjustment for multiplicity of comparisons and overlap with the primary outcome (relative risk 0.87; 95% CI 0.76–1.00; unadjusted P = 0.048 vs adjusted P = 0.068). Telmisartan was associated with a decreased risk of hospitalization for cardiovascular reasons compared with placebo (30.3% vs 33.0%; P = 0.025).
The findings of these major clinical outcome studies on ARBs are summarized in . Overall, the major clinical outcomes of these trials, which primarily involved elderly patients, demonstrate that ARBs reduce cardiovascular events in patients, including those who are at high risk, equivalent to ACEIs and that this class of drugs can be considered as a first-line therapy in those intolerant to ACEI therapy.
Table 1 Major clinical trials of angiotensin II type 1 receptor antagonists in the elderly
Use of angiotensin II AT1 receptor antagonists in type 2 diabetes
Diabetes is rapidly increasing worldwide in all patient groups, including the elderly.Citation73 It is estimated that 50% of patients with diabetes suffer from hypertension, and this number is even higher in the elderly.Citation74 Additionally, chronic kidney disease (CKD) is a major cause of morbidity and mortality in patients with diabetes, and the role of the RAAS in the development of CKD in patients with diabetes has been well documented.Citation75,Citation76 A number of clinical studies, including Irbesartan in Type 2 Diabetes (IRMA 2),Citation77 the Irbesartan Type 2 Diabetic Nephropathy Trial (IDNT),Citation78 Reduction in End Points in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL),Citation79 and Microalbuminuria Reduction with Valsartan (MARVAL),Citation80 have established the superior efficacy of AT1 receptor antagonists over conventional, non-ACEI, blood pressure-lowering agents in patients with type 2 diabetes and renal insufficiency. Importantly, these studies have highlighted that the renoprotective effects of AT1 receptor antagonists are not solely due to a reduction of blood pressure. Instead, multiple actions of ARBs appear to be responsible for beneficial effects of these agents in diabetes.Citation81 In fact, blockade of angiotensin II binding to the AT1 receptor results in improvement of insulin and glucose metabolism at different levels, including an improvement in insulin secretion and peripheral insulin responses.Citation82,Citation83 Moreover, angiotensin II signaling is implicated in vascular injury associated with diabetes, and inhibition of AT1 receptors attenuates these responses markedly, including the diabetic proinflammatory state.Citation84
These molecular mechanisms can be translated into clinical settings. A recent meta-analysis that combined 22 clinical trials with 143,153 patients treated with different antihypertensive agents confirmed that ARBs potently decrease the relative risk for new onset of diabetes by 38% compared with diuretics.Citation85 In these studies, treatment of patients with diabetes with ARBs resulted in a substantial reduction of cardiovascular endpoints, underlining that blockade of AT1 receptors may potentially provide not only antidiabetic action but also cardiovascular protection in diabetes. As a result, AT1 receptor antagonists are recommended as a first-line therapy in patients with hypertension and concomitant type 2 diabetes and/or CKD.Citation13,Citation86
Efficacy and tolerability studies of ARBs in elderly patients
The Losartan Intervention for Endpoint Reduction in Hypertension Study (LIFE) was one of the first clinical trials to demonstrate that AT1 receptor antagonists may have greater benefits than other antihypertensives in high-risk patients, including the elderly.Citation87 In this double-blind trial, 9193 patients aged between 55 and 80 years (mean age 66.7 years) with hypertension and left ventricular hypertrophy on ECG were randomized to either once-daily losartan or atenolol. After a mean follow-up of 4 years, the primary composite endpoint of cardiovascular morbidity and mortality, which included stroke, myocardial infarction, and cardiovascular death, was reduced 13% more in losartan-treated patients compared with the atenolol-treated group (P = 0.021). In addition, the incidence of fatal or nonfatal stroke was 25% lower in the losartan group compared with the atenolol group (P = 0.001). There were no statistically significant differences in coronary events between both groups (17% vs 15% for losartan and atenolol, respectively). Importantly, the extent of a reduction of mean arterial blood pressure was essentially identical in the treatment groups (102.2 vs 102.4 mm Hg for losartan and atenolol, respectively). In a subgroup of 1195 patients with diabetes, losartan decreased the primary composite endpoint by 24% (18% vs 23% for losartan and atenolol, respectively; P = 0.031). In addition, there was a statistically significant reduction in cardiovascular and total mortality in the losartan group (P = 0.028 and P = 0.002, respectively).Citation88 Notably, when stratified by race (black and nonblack groups), there was a lower risk for the primary endpoint with atenolol versus losartan (HR 1.67 for losartan vs atenolol; P = 0.033).Citation89,Citation90
The Study of Cognition and Prognosis in the Elderly (SCOPE) was a prospective, double-blind, randomized, parallel-group study that compared candesartan with placebo in 4964 elderly hypertensive patients aged between 70 and 89 years. The primary goal of this study was to assess whether treatment with candesartan in elderly subjects with mildly to moderately elevated blood pressure results in a reduction of cardiovascular events, cognitive decline, and dementia.Citation91 During a mean follow-up of 44.6 months, there was no difference in the reduction of mean arterial blood pressure with candesartan versus placebo (145.2 vs 148.5 mm Hg, respectively). However, despite no significant difference in arterial blood pressure, candesartan was associated with a 27.8% reduction in nonfatal stroke (P = 0.04) and a 23.6% reduction in all strokes (P = 0.056) compared with placebo. There was no statistically significant difference in myocardial infarction (1.9% candesartan vs 2.0% placebo) or cardiovascular mortality (15.6% candesartan vs 16.6% placebo). An analysis including only patients with isolated systolic hypertension, a type of hypertension very common in the elderly, showed a 40% reduction in stroke in patients treated with candesartan (P = 0.05).Citation92,Citation93
The Valsartan Antihypertensive Long-term Use Evaluation (VALUE) trial was a double-blind, randomized, parallel-group study in 15,245 patients aged above 50 years (mean age 67.2 years) suffering from hypertension and additional diseases conferring high risk of cardiac events, where the effects of an ARB therapy (valsartan 80–160 mg/day) were compared with calcium channel blocker therapy (amlodipine 5–10 mg/day).Citation94 During the first year, amlodipine reduced the mean arterial blood pressure by an extra 1.5/1.3 mm Hg compared with valsartan (P < 0.001). However, over a mean follow-up of 4.2 years, there was no statistically significant difference between the groups with regard to cardiac mortality (4.0% vs 4.0%), morbidity (7.7% vs 7.6%), or overall mortality (11.0% vs 10.8%). There was a trend toward a higher incidence of stroke (4.2% valsartan and 3.7% amlodipine; P = 0.08) and myocardial infarction (4.8% valsartan vs 4.1% amlodipine; P = 0.02) and a decreased incidence of heart failure (4.6% valsartan vs 5.3% amlodipine; P = 0.12) in the valsartan group. Additionally, it was shown that valsartan therapy reduced the onset of diabetes in patients by 23% (P = 0.0001).Citation94 Similar findings were reported in other clinical trials with AT1 receptor antagonists,Citation65,Citation95 which may represent a long-term benefit of ARBs that is probably not easily observable in short-term clinical studies monitoring cardiovascular outcomes.Citation65,Citation95
Clinical trials investigating the efficacy of AT1 receptor antagonists have reported adverse event rates similar to those seen with placebo and considerably lower than those in groups treated with ACEIs.Citation62,Citation96–Citation98 Comparable tolerability profiles were identified in the elderly population, with relatively few undesirable effects reported in patients receiving ARBs compared with ACEIs.Citation61
Undesirable effects of AT1 receptor antagonists that have been reported include fatigue, dizziness, headache, hyperkalemia, hypotension, and acute renal insufficiency in predisposed patients or those at risk.Citation99,Citation100 Hyperkalemia is increased primarily in patients already receiving therapy that targets the RAAS (eg, concomitant ACEI use or aldosterone receptor antagonists), as well as in patients with accompanying renal impairment, heart failure, and/or renal tubular acidosis associated with diabetes.Citation101,Citation102 Additionally, a dramatic increase (∼seven-fold) in the risk of hyperkalemia-associated hospitalizations was reported in patients on concomitant therapy of ARBs or ACEIs and trimethoprim–sulfamethoxazole in elderly patients, suggesting the use of alternative antibiotic therapy in this population.Citation103
As with many other drugs that posses a vasodilating effect, ARBs should be used with caution in patients with aortic or mitral stenosis and obstructive hypertrophic cardiomyopathy. In long-term studies, ARBs did not appear to affect concentrations of fasting serum glucose, fasting triglycerides, serum uric acid, urinary uric acid secretion, or total cholesterol.Citation104,Citation105 ARBs have been extensively employed in patients with unilateral renal stenosis without any secondary effects on renovascular hypertension.Citation101,Citation102
In a recent meta-analysis of randomized controlled trials of ARBs, Sipahi et al reported that ARBs are associated with a modestly increased risk of new cancer diagnosis (7.2% vs 6.0%; risk ratio 1.08; 95% CI 1.01–1.15; P = 0.016).Citation106 Undoubtedly, this study received considerable attention, as the possibility that ARBs might increase the risk for cancer is of great concern.Citation107 Importantly, the authors of the study as well as many critics acknowledge the limitations of the analysis, which was based on a post hoc analysis of an incomplete database and included trials that were not designed to explore cancer outcomes.Citation108 Despite the limitations, the study of Sipahi et al raises several concerns that have important clinical relevance, and their findings warrant further investigations to draw conclusions about the exact risk of cancer associated with the overall class of ARBs and/or particular members of this class.Citation109
Very few drug–drug interactions of clinical importance have been noted with ARBs.Citation52,Citation100,Citation110 These observations were confirmed by in vitro screening studies with human hepatic cytochrome P450 (CYP) enzymes, indicating negligible inhibitory potential of these drugs.Citation111 In addition, neither induction nor inhibition of CYP isoenzymes was observed with valsartan.Citation100 Likewise, nonsignificant interactions were observed between irbesartan and CYP2C9 substrates such as tolbutamide, warfarin, and nifedipine.Citation112
Pharmacokinetic and pharmacodynamic properties of various AT1 receptor antagonists
It is well known that pharmacokinetic profiles of drugs can be modified by age.Citation113 For example, changes in the body composition (eg, lean body mass, body water, and fat) can influence drug distribution and half-life without substantial changes in drug absorption.Citation114,Citation115 In patients with chronic diseases that are often common in the elderly, plasma albumin concentrations may be decreased, resulting in elevated concentrations of free acidic drugs.Citation116 In addition, the level of plasma α-1-acid glycoprotein, a key plasma protein responsible for binding and transport of many drugs, is also increased in several conditions, including cardiovascular, kidney, liver, inflammatory, and central nervous system disorders.Citation117 Increased bioavailability and prolonged half-life of drugs in aging patients can also be reasoned by decreased intestinal and hepatic metabolism of drugs, as well as decreased renal elimination of metabolites and parent compounds.
The main pharmacokinetic properties of currently available ARBs are summarized in . Telmisartan is a highly lipophilic drug with a long plasma half-life (20–38 h) and large volume of distribution (7 L/kg). In contrast, candesartan has a very small volume of distribution (0.13 L/kg), indicating restrictive protein binding of the drug and limited tissue distribution. Among all of the ARBs, only losartan, candesartan, and irbesartan are metabolized by CYP isoenzymes.Citation118 Approximately 14% of a given dose of losartan is converted into the free carboxylic acid form EXP3174, an active metabolite of the parent drug with noncompetitive/insurmountable antagonistic activity.Citation102 Irbesartan is mainly metabolized by CYP2C9 and CYP3A4, and it undergoes glucuronidation.Citation99 Valsartan undergoes an oxidative biotransformation to an active metabolite valerly-4-hydroxy-valsartan.Citation119
Table 2 Pharmacology and pharmacokinetics of ARBs
A number of ARBs (eg, eprosartan, irbesartan, and telmisartan) undergo phase II metabolic transformation through acyl glucuronidation in the liver and gastrointestinal system.Citation120,Citation121 Glucuronides are excreted by urine and bile, and in the latter case the conjugates are cleaved by bacterial enzymes, leading to liberation of parent compounds or metabolites in the gastrointestinal system. Notably, this metabolic pathway may be impaired by deficiency of uridine diphosphate glucuronosyltransferase 1A1, which is considered a potential target for polymorphic variations.Citation122 AT1 receptor antagonists are largely eliminated by biliary excretion, although losartan and olmesartan show more substantial renal excretion. Average elimination time of the AT1 receptor blockers is between 5 and 9 h, except losartan, which has the shortest plasma elimination half-life of 1–3 h, and telmisartan, which has the longest plasma elimination half-life of ∼24 h.Citation52,Citation100,Citation107,Citation123,Citation124 In general, duration of action of receptor antagonists depends on the rate of their dissociation from the target receptor, which is the case for ARBs as well. All of the ARBs are very effective with once-daily administration, although losartan and eprosartan may provide better 24-h effects when given twice daily.
The area under the plasma concentration–time curve for a number of ARBs (ie, candesartan, eprosartan, irbesartan, olmesartan, and valsartan but not telmisartan) has been shown to increase in the elderly compared with a younger population.Citation121,Citation125–Citation129 Nevertheless, the recommended starting dose for most AT1 receptor antagonists (candesartan, eprosartan, irbesartan, losartan, olmesartan) has not been changed in the elderly, which is explained by possible decreased activity of circulating RAAS. It has been demonstrated that patients with moderate hepatic impairment have increased plasma concentrations of most AT1 receptor antagonists, which may require dose adjustments in individual patients, depending on tolerability and response to the drug.Citation105 The recommended maximal daily dose of ARBs for patients with moderate hepatic impairment should not exceed 12 mg for candesartan, 20 mg for olmesartan, 40 mg for telmisartan, or 80 mg for valsartan.Citation130–Citation133 In addition, patients with portal hypertension and liver cirrhosis should only be treated with irbesartan.Citation134 As renal elimination is not a major route of excretion for most AT1 receptor antagonists, dose adjustments are usually not required for patients with renal impairment, although lower starting doses are typically used for most patients. Importantly, careful monitoring of renal function is vital after starting ARBs in patients with pre-existing renal impairment.Citation101,Citation135,Citation136
Summary and conclusion
ARBs represent a contemporary class of drugs often used for the treatment of elevated arterial blood pressure in the elderly population, both as monotherapy or in combination with other antihypertensive agents. Although current hypertension guidelines recommend thiazide diuretics as first-line therapy for most patients with hypertension in the absence of a compelling indication, data are now available supporting the use of ARBs as a first-line agent, and it is likely that they will be included as an option for initial management when the new JNC 8 guidelines are released.Citation13,Citation17,Citation137,Citation138 In addition to hypertension, ARBs are also recommended as a first-line agent in patients with type 2 diabetes with microalbuminuria or nephropathy.Citation17,Citation139 In patients with high arterial blood pressure and heart failure, ARBs are recommended only when ACEIs are not tolerated.Citation140 They are also recommended for elderly patients with hypertension and left ventricular hypertrophy, as they have been found to be superior to β-blocker-based regimens in such high-risk subjects and have a better profile for stroke prevention.Citation87 Due to the fact that ARBs are very well tolerated, may be dosed once daily, and have few drug–drug interactions, these agents are an important alternative to other blood pressure-lowering medications. The main disadvantage of ARBs is their cost, as they are typically the most expensive group of blood pressure-lowering agents. However, with the approval of generic losartan and other generic agents in future, it is likely that the use of ARBs as first-line therapy, particularly in the elderly, will continue to grow.
Disclosure
The authors report no conflicts of interest in this work.
References
- ElliottWJManagement of hypertension in the very elderly patientHypertension200444680080415505119
- KearneyPMWheltonMReynoldsKMuntnerPWheltonPKHeJGlobal burden of hypertension: analysis of worldwide dataLancet2005365945521722315652604
- VasanRSBeiserASeshadriSResidual lifetime risk for developing hypertension in middle-aged women and men: The Framingham Heart StudyJAMA200228781003101011866648
- LakattaEGArterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part III: cellular and molecular clues to heart and arterial agingCirculation2003107349049712551876
- BeckettNSPetersRFletcherAETreatment of hypertension in patients 80 years of age or olderN Engl J Med2008358181887189818378519
- StaessenJAFagardRThijsLRandomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial InvestigatorsLancet199735090807577649297994
- DahlofBLindholmLHHanssonLScherstenBEkbomTWesterPOMorbidity and mortality in the Swedish trial in old patients with hypertension (STOP-hypertension)Lancet19913388778128112851682683
- Medical Research Council European trial of chorion villus samplingMRC working party on the evaluation pf chorion villus samplingLancet19913378756149114991675367
- SHEP Cooperative Research GroupPrevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP)JAMA199126524325532642046107
- IsrailiZHHallWDACE inhibitors. Differential use in elderly patients with hypertensionDrugs Aging1995753553718573991
- SvanborgAAge-related changes in cardiac physiology. Can they be postponed or treated by drugs?Drugs Aging19971064634729205851
- CleophasTJvan MarumRAge-related decline in autonomic control of blood pressure: implications for the pharmacological management of hypertension in the elderlyDrugs Aging200320531331912696992
- ChobanianAVBakrisGLBlackHRSeventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureHypertension20034261206125214656957
- ManciaGde BackerGDominiczakA2007 Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)Eur Heart J200728121462153617562668
- KalraSKalraBAgrawalNCombination therapy in hypertension: an updateDiabetol Metab Syndr2010214420576135
- WrightJMLeeCHChambersGKSystematic review of antihypertensive therapies: does the evidence assist in choosing a first-line drug?CMAJ19991611253210420860
- ChobanianAVBakrisGLBlackHRThe seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 reportJAMA2003289192560257212748199
- OgiharaTRakugiHHypertension in the elderly: a Japanese perspectiveDrugs Aging200522429731415839719
- HallerHEffective management of hypertension with dihydropyridine calcium channel blocker-based combination therapy in patients at high cardiovascular riskInt J Clin Pract200862578179018355239
- HillemanDELucasBDJrAngiotensin-converting enzyme inhibitors and stroke risk: benefit beyond blood pressure reduction?Pharmacotherapy20042481064107615338854
- BangaloreSMesserliFHKostisJBPepineCJCardiovascular protection using beta-blockers: a critical review of the evidenceJ Am Coll Cardiol200750756357217692739
- FlegJLAronowWSFrishmanWHCardiovascular drug therapy in the elderly: benefits and challengesNat Rev Cardiol201011620213930
- WernerCBaumhakelMTeoKKRAS blockade with ARB and ACE inhibitors: current perspective on rationale and patient selectionClin Res Cardiol200897741843118454336
- WeberMAchieving blood pressure goals: should angiotensin II receptor blockers become first-line treatment in hypertension?J Hypertens Suppl2009275S9S1419587555
- CooneyDPascuzziKPolypharmacy in the elderly: focus on drug interactions and adherence in hypertensionClin Geriatr Med200925222123319555869
- CovicAGusbeth-TatomirPThe role of the renin-angiotensin-aldosterone system in renal artery stenosis, renovascular hypertension, and ischemic nephropathy: diagnostic implicationsProg Cardiovasc Dis200952320420819917331
- TurgutFBalogunRAAbdel-RahmanEMRenin-angiotensin-aldosterone system blockade effects on the kidney in the elderly: benefits and limitationsClin J Am Soc Nephrol2010571330133920498247
- SiragyHMCareyRMRole of the intrarenal renin-angiotensin-aldosterone system in chronic kidney diseaseAm J Nephrol201031654155020484892
- BelminJLevyBIMichelJBChanges in the renin-angiotensin-aldosterone axis in later lifeDrugs Aging1994553914007833591
- TsunodaKAbeKGotoTEffect of age on the renin-angiotensin-aldosterone system in normal subjects: simultaneous measurement of active and inactive renin, renin substrate, and aldosterone in plasmaJ Clin Endocrinol Metab19866223843893510226
- SchiffrinELTouyzRMMultiple actions of angiotensin II in hypertension: benefits of AT1 receptor blockadeJ Am Coll Cardiol200342591191312957442
- KaschinaEUngerTAngiotensin AT1/AT2 receptors: regulation, signalling and functionBlood Press2003122708812797627
- BenigniACassisPRemuzziGAngiotensin II revisited: new roles in inflammation, immunology and agingEMBO Mol Med20102724725720597104
- YamamotoRAkazawaHItoKAngiotensin II type 1a receptor signals are involved in the progression of heart failure in MLP-deficient miceCirc J200771121958196418037754
- SasakiTKuzuyaMNakamuraKAT1 blockade attenuates atherosclerotic plaque destabilization accompanied by the suppression of cathepsin S activity in apoE-deficient miceAtherosclerosis2010210243043720079903
- EhrlichJRNattelSNovel approaches for pharmacological management of atrial fibrillationDrugs200969775777419441867
- TadevosyanAMaguyAVilleneuveLRNuclear-delimited angiotensin receptor-mediated signaling regulates cardiomyocyte gene expressionJ Biol Chem201028529223382234920463030
- BilletSAguilarFBaudryCClauserERole of angiotensin II AT1 receptor activation in cardiovascular diseasesKidney Int200874111379138418650793
- SkeggsLTJrKahnJRLentzKShumwayNPThe preparation, purification, and amino acid sequence of a polypeptide renin substrateJ Exp Med1957106343945313463253
- KatragaddaSAroraRRRole of angiotensin-converting enzyme inhibitors in vascular modulation: beyond the hypertensive effectsAm J Ther2010171e11e2320090429
- MorathCSchmiedBMehrabiAAngiotensin-converting enzyme inhibitors and angiotensin II type 1 receptor blockers after renal transplantationClin Transplant200923Suppl 21333619930314
- BrownNJVaughanDEAngiotensin-converting enzyme inhibitorsCirculation19989714141114209577953
- IsrailiZHHallWDCough and angioneurotic edema associated with angiotensin-converting enzyme inhibitor therapy. A review of the literature and pathophysiologyAnn Intern Med199211732342421616218
- WooKSNichollsMGHigh prevalence of persistent cough with angiotensin converting enzyme inhibitors in ChineseBr J Clin Pharmacol19954021411448562296
- OsIBratlandBDahlofBGisholtKSyvertsenJOTretliSFemale sex as an important determinant of lisinopril-induced coughLancet199233987893721346451
- HooverTLippmannMGrouzmannEMarceauFHerscuPAngiotensin converting enzyme inhibitor induced angiooedema: a review of the pathophysiology and risk factorsClin Exp Allergy2010401506119659669
- BrownNJRayWASnowdenMGriffinMRBlack Americans have an increased rate of angiotensin converting enzyme inhibitor-associated angioedemaClin Pharmacol Ther19966018138689816
- SlaterEEMerrillDDGuessHAClinical profile of angioedema associated with angiotensin converting-enzyme inhibitionJAMA198826079679702840522
- TomlinsonBYoungRPChanJCChanTYCritchleyJAPharmacoepidemiology of ACE inhibitor–induced coughDrug Saf19971621501519067125
- McInnesGTO’KaneKPIstadHKeinanen-KiukaanniemiSvan MierloHFComparison of the AT1-receptor blocker, candesartan cilexetil, and the ACE inhibitor, lisinopril, in fixed combination with low dose hydrochlorothiazide in hypertensive patientsJ Hum Hypertens200014426326910805052
- GoaKLWagstaffAJLosartan potassium: a review of its pharmacology, clinical efficacy and tolerability in the management of hypertensionDrugs19965158208458861549
- SimpsonKLMcClellanKJLosartan: a review of its use, with special focus on elderly patientsDrugs Aging200016322725010803861
- UngerTPharmacology of AT1-receptor blockersBlood Press Suppl2001351011683476
- TurnbullFBlood Pressure Lowering Treatment Trialists’ CollaborationEffects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trialsLancet200336293951527153514615107
- LawMRMorrisJKWaldNJUse of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studiesBMJ2009338b166510.1136/bmj.b166519454737
- GradmanAHPapademetriouVCombined renin-angiotensin-aldosterone system inhibition in patients with chronic heart failure secondary to left ventricular systolic dysfunctionAm Heart J2009157Suppl 6S17S2319450720
- FrancisGSCohnJNJohnsonGRectorTSGoldmanSSimonAPlasma norepinephrine, plasma renin activity, and congestive heart failure. Relations to survival and the effects of therapy in V-HeFT II. The V-HeFT VA Cooperative Studies GroupCirculation199387Suppl 6VI40VI488500238
- RieggerGABouzoHPetrPImprovement in exercise tolerance and symptoms of congestive heart failure during treatment with candesartan cilexetil. Symptom, Tolerability, Response to Exercise Trial of Candesartan Cilexetil in Heart Failure (STRETCH) InvestigatorsCirculation1999100222224223010577995
- CohnJNRationale for angiotensin II receptor blocker therapy in chronic heart failureJ Renin Angiotensin Aldosterone Syst20001Suppl 2S38S4017199220
- MaggioniAPAnandIGottliebSOLatiniRTognoniGCohnJNEffects of valsartan on morbidity and mortality in patients with heart failure not receiving angiotensin-converting enzyme inhibitorsJ Am Coll Cardiol20024081414142112392830
- PittBSegalRMartinezFARandomised trial of losartan versus captopril in patients over 65 with heart failure (Evaluation of Losartan in the Elderly Study, ELITE)Lancet199734990547477529074572
- PittBPoole-WilsonPASegalREffect of losartan compared with captopril on mortality in patients with symptomatic heart failure: randomised trial–the Losartan Heart Failure Survival Study ELITE IILancet200035592151582158710821361
- CohnJNTognoniGValsartan Heart Failure Trial InvestigatorsA randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failureN Engl J Med2001345231667167511759645
- DicksteinKELITE II and Val-HeFT are different trials: together what do they tell us?Curr Control Trials Cardiovasc Med20012524024311806803
- PfefferMASwedbergKGrangerCBEffects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programmeLancet2003362938675976613678868
- GrangerCBMcMurrayJJYusufSEffects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-alternative trialLancet2003362938677277613678870
- McMurrayJJOstergrenJSwedbergKEffects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trialLancet2003362938676777113678869
- YusufSPfefferMASwedbergKEffects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved TrialLancet2003362938677778113678871
- DicksteinKKjekshusJOPTIMAAL Steering Committee of the OPTIMAAL Study GroupEffects of losartan and captopril on mortality and morbidity in high-risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Optimal trial in myocardial infarction with angiotensin II antagonist losartanLancet2002360933575276012241832
- PfefferMAMcMurrayJJVelazquezEJValsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or bothN Engl J Med2003349201893190614610160
- YusufSTeoKKPogueJTelmisartan, ramipril, or both in patients at high risk for vascular eventsN Engl J Med2008358151547155918378520
- YusufSTeoKAndersonCEffects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: a randomised controlled trialLancet200837296441174118318757085
- UngerJParkinCGType 2 diabetes: an expanded view of pathophysiology and therapyPostgrad Med2010122314515720463424
- UK Prospective Diabetes Study GroupTight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38BMJ199831771607037139732337
- RuilopeLMAngiotensin receptor blockers: RAAS blockade and renoprotectionCurr Med Res Opin20082451285129318366863
- SiamopoulosKCKalaitzidisRGInhibition of the renin-angiotensin system and chronic kidney diseaseInt Urol Nephrol20084041015102518704745
- ParvingHHLehnertHBrochner-MortensenJGomisRAndersenSArnerPThe effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetesN Engl J Med20013451287087811565519
- LewisEJHunsickerLGClarkeWRRenoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetesN Engl J Med20013451285186011565517
- BrennerBMCooperMEde ZeeuwDEffects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathyN Engl J Med20013451286186911565518
- VibertiGWheeldonNMMicroAlbuminuria Reduction With VALsartan (MARVAL) Study InvestigatorsMicroalbuminuria reduction with valsartan in patients with type 2 diabetes mellitus: a blood pressure-independent effectCirculation2002106667267812163426
- ScheenAJPrevention of type 2 diabetes mellitus through inhibition of the Renin-Angiotensin systemDrugs200464222537256515516153
- DerosaGCiceroAFD’AngeloATelmisartan and irbesartan therapy in type 2 diabetic patients treated with rosiglitazone: effects on insulin-resistance, leptin and tumor necrosis factor-alphaHypertens Res2006291184985617345784
- NagelJMTietzABGokeBParhoferKGThe effect of telmisartan on glucose and lipid metabolism in nondiabetic, insulin-resistant subjectsMetabolism20065591149115416919531
- WiernspergerNVascular defects in the aetiology of peripheral insulin resistance in diabetes. A critical review of hypotheses and factsDiabetes Metab Rev19941032873077835173
- ElliottWJMeyerPMIncident diabetes in clinical trials of antihypertensive drugs: a network meta-analysisLancet2007369955720120717240286
- American Diabetes AssociationStandards of medical care in diabetes–2010Diabetes Care201033Suppl 1S11S6120042772
- DahlofBDevereuxRBKjeldsenSECardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenololLancet20023599311995100311937178
- LindholmLHIbsenHDahlofBCardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenololLancet200235993111004101011937179
- DevereuxRBLylePALosartan for the treatment of hypertension and left ventricular hypertrophy: the Losartan Intervention For Endpoint reduction in hypertension (LIFE) studyExpert Opin Pharmacother20045112311232015500378
- JuliusSAldermanMHBeeversGCardiovascular risk reduction in hypertensive black patients with left ventricular hypertrophy: the LIFE studyJ Am Coll Cardiol20044361047105515028365
- LithellHHanssonLSkoogIThe Study on Cognition and Prognosis in the Elderly (SCOPE): principal results of a randomized double-blind intervention trialJ Hypertens200321587588612714861
- PapademetriouVFarsangCElmfeldtDStroke prevention with the angiotensin II type 1-receptor blocker candesartan in elderly patients with isolated systolic hypertension: the Study on Cognition and Prognosis in the Elderly (SCOPE)J Am Coll Cardiol20044461175118015364316
- ChobanianAVClinical practice. Isolated systolic hypertension in the elderlyN Engl J Med2007357878979617715411
- JuliusSKjeldsenSEWeberMOutcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trialLancet200436394262022203115207952
- LindholmLHPerssonMAlaupovicPCarlbergBSvenssonASamuelssonOMetabolic outcome during 1 year in newly detected hypertensives: results of the Antihypertensive Treatment and Lipid Profile in a North of Sweden Efficacy Evaluation (ALPINE study)J Hypertens20032181563157412872052
- McKelvieRSYusufSPericakDComparison of candesartan, enalapril, and their combination in congestive heart failure: randomized evaluation of strategies for left ventricular dysfunction (RESOLVD) pilot study. The RESOLVD Pilot Study InvestigatorsCirculation1999100101056106410477530
- HallWDMontoroRLittlejohnTJainAFelicianoNZhengHEfficacy and tolerability of valsartan in combination with hydrochlorothiazide in essential hypertensionClin Drug Investig1998163203210
- CritchleyLAHypotension, subarachnoid block and the elderly patientAnaesthesia19965112113911439038450
- GillisJCMarkhamAIrbesartan. A review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in the management of hypertensionDrugs19975468859029421695
- MarkhamAGoaKLValsartan. A review of its pharmacology and therapeutic use in essential hypertensionDrugs19975422993119257084
- WeirMRAre drugs that block the renin-angiotensin system effective and safe in patients with renal insufficiency?Am J Hypertens19991212 Pt 3195S203S10619572
- BurnierMBrunnerHRAngiotensin II receptor antagonistsLancet2000355920463764510696996
- AntoniouTGomesTJuurlinkDNLoutfyMRGlazierRHMamdaniMMTrimethoprim-sulfamethoxazole-induced hyperkalemia in patients receiving inhibitors of the renin-angiotensin system: a population-based studyArch Intern Med2010170121045104920585070
- PuigJGMateosFBunoAOrtegaRRodriguezFDal-ReREffect of eprosartan and losartan on uric acid metabolism in patients with essential hypertensionJ Hypertens19991771033103910419078
- CsajkaCBuclinTBrunnerHRBiollazJPharmacokinetic-pharmacodynamic profile of angiotensin II receptor antagonistsClin Pharmacokinet19973211299012554
- SipahiIDebanneSMRowlandDYSimonDIFangJCAngiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trialsLancet Oncol201011762763620542468
- GoldsteinMRMascitelliLPezzettaFAngiotensin-receptor blockade, cancer, and concernsLancet Oncol201011819
- BöhmMLaufsUPfreundschuhMComment on: Angiotensinreceptor blockade and risk of cancer: meta-analysis of randomised controlled trialsLancet Oncol20101181820816376
- MeredithPAMcInnesGTComment on: Angiotensinreceptor blockade and risk of cancer: meta-analysis of randomised controlled trialsLancet Oncol20101181920816377
- SharpeMJarvisBGoaKLTelmisartan: a review of its use in hypertensionDrugs200161101501152911558835
- TaavitsainenPKiukaanniemiKPelkonenOIn vitro inhibition screening of human hepatic P450 enzymes by five angiotensin-II receptor antagonistsEur J Clin Pharmacol200056213514010877007
- MarinoMRVachharajaniNNDrug interactions with irbesartanClin Pharmacokinet200140860561411523726
- CodyRJPhysiological changes due to age. Implications for drug therapy of congestive heart failureDrugs Aging1993343203348369592
- MorganDJBrayKMLean body mass as a predictor of drug dosage. Implications for drug therapyClin Pharmacokinet19942642923078013162
- TurnheimKDrug dosage in the elderly. Is it rational?Drugs Aging19981353573799829164
- FuANairKSAge effect on fibrinogen and albumin synthesis in humansAm J Physiol19982756 Pt 1E1023E10309843745
- IsrailiZHDaytonPGHuman alpha-1-glycoprotein and its interactions with drugsDrug Metab Rev200133216123511495502
- UngerTKaschinaEDrug interactions with angiotensin receptor blockers: a comparison with other antihypertensivesDrug Saf2003261070772012862505
- WaldmeierFFleschGMullerPPharmacokinetics, disposition and biotransformation of [14C]-radiolabelled valsartan in healthy male volunteers after a single oral doseXenobiotica199727159719041679
- RuilopeLJagerBEprosartan for the treatment of hypertensionExpert Opin Pharmacother20034110711412517247
- TeneroDMMartinDEMillerAKEffect of age and gender on the pharmacokinetics of eprosartanBr J Clin Pharmacol19984632672709764969
- UchidaSWatanabeHNishioSAltered pharmacokinetics and excessive hypotensive effect of candesartan in a patient with the CYP2C91/3 genotypeClin Pharmacol Ther200374550550814586391
- MallionJSicheJLacourciereYABPM comparison of the antihypertensive profiles of the selective angiotensin II receptor antagonists telmisartan and losartan in patients with mild-to-moderate hypertensionJ Hum Hypertens1999131065766410516734
- WhiteWBAnwarYAMansoorGASicaDAEvaluation of the 24-hour blood pressure effects of eprosartan in patients with systemic hypertensionAm J Hypertens200114121248125511775134
- HubnerRHogemannAMSunzelMRiddellJGPharmacokinetics of candesartan after single and repeated doses of candesartan cilexetil in young and elderly healthy volunteersJ Hum Hypertens199711Suppl 2S19S259331000
- SioufiAMarfilFJaouenAThe effect of age on the pharmacokinetics of valsartanBiopharm Drug Dispos19981942372449604123
- VachharajaniNNShyuWCSmithRAGreeneDSThe effects of age and gender on the pharmacokinetics of irbesartanBr J Clin Pharmacol19984666116139862252
- von BergmannKLaeisPPuchlerKSudhopTSchwochoLRGonzalezLOlmesartan medoxomil: influence of age, renal and hepatic function on the pharmacokinetics of olmesartan medoxomilJ Hypertens Suppl2001191S33S4011451213
- McClellanKJMarkhamATelmisartanDrugs199856610391044 discussion104510469878991
- StangierJSuCASchondorferGRothWPharmacokinetics and safety of intravenous and oral telmisartan 20 mg and 120 mg in subjects with hepatic impairment compared with healthy volunteersJ Clin Pharmacol20004012 Pt 11355136411185634
- ThurmannPAValsartan: a novel angiotensin type 1 receptor antagonistExpert Opin Pharmacother20001233735011249553
- GleiterCHMorikeKEClinical pharmacokinetics of candesartanClin Pharmacokinet200241171711825094
- BrousilJABurkeJMOlmesartan medoxomil: an angiotensin II-receptor blockerClin Ther20032541041105512809956
- SchepkeMWernerEBieckerEHemodynamic effects of the angiotensin II receptor antagonist irbesartan in patients with cirrhosis and portal hypertensionGastroenterology2001121238939511487548
- BurnierMAngiotensin II type 1 receptor blockersCirculation2001103690491211171802
- WeirMRDiabetes and hypertension: how low should you go and with which drugs?Am J Hypertens2001145 Pt 217S26S11370956
- CuspidiCNegriFZanchettiAAngiotensin II receptor blockers and cardiovascular protection: focus on left ventricular hypertrophy regression and atrial fibrillation preventionVasc Health Risk Manag200841677318629360
- HanesDSWeirMRUsefulness of ARBs and ACE inhibitors in the prevention of vascular dementia in the elderlyAm J Geriatr Cardiol200716317518217483670
- European Society of Hypertension-European Society of Cardiology Guidelines Committee2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertensionJ Hypertens20032161011105312777938
- SimkoFSimkoJFabryovaMACE-inhibition and angiotensin II receptor blockers in chronic heart failure: pathophysiological consideration of the unresolved battleCardiovasc Drugs Ther200317328729014669746
- PloskerGLFosterRHEprosartan: a review of its use in the management of hypertensionDrugs200060117720110929934
- BottorffMBTeneroDMPharmacokinetics of eprosartan in healthy subjects, patients with hypertension, and special populationsPharmacotherapy1999194 Pt 273S78S10213525
- McClellanKJBalfourJAEprosartanDrugs1998555713718 discussion7197209585867
- TeneroDMartinDChapelskyMEffect of hepatic disease on the pharmacokinetics and plasma protein binding of eprosartanPharmacotherapy199818142509469680
- MarkhamASpencerCMJarvisBIrbesartan: an updated review of its use in cardiovascular disordersDrugs20005951187120610852648
- MarinoMRLangenbacherKMRaymondRHFordNFLasseterKCPharmacokinetics and pharmacodynamics of irbesartan in patients with hepatic cirrhosisJ Clin Pharmacol19983843473569590462
- WarnerGTJarvisBOlmesartan medoxomilDrugs200262913451353 discussion1354135612076183
- KaramyanVTSpethRCEnzymatic pathways of the brain renin-angiotensin system: unsolved problems and continuing challengesRegul Pept20071431–3152717493693
- SaseenJJMacLaughlinEJHypertensionDiPiroJTTalbertRLYeeGRMatzkeGRWellsBGPoseyLMPharmacotherapy: a Pathophysiologic Approach7th edMcGraw-Hill Companies, Inc.2008139171