
Abstract
Psoriasis is the skin disease that most frequently affects the nails. Depending on the very nail structure involved, different clinical nail alterations can be observed. Irritation of the apical matrix results in psoriatic pits, mid-matrix involvement may cause leukonychia, whole matrix affection may lead to red lunulae or severe nail dystrophy, nail bed involvement may cause salmon spots, subungual hyperkeratosis, and splinter hemorrhages, and psoriasis of the distal nail bed and hyponychium causes onycholysis whereas that of the proximal nail fold causes psoriatic paronychia. The more extensive the involvement, the more severe is the nail destruction. Pustular psoriasis may be seen as yellow spots under the nail or, in case of acrodermatitis continua suppurativa, as an insidious progressive loss of the nail organ. Nail psoriasis has a severe impact on quality of life and may interfere with professional and other activities. Management includes patient counseling, avoidance of stress and strain to the nail apparatus, and different types of treatment. Topical therapy may be tried but is rarely sufficiently efficient. Perilesional injections with corticosteroids and methotrexate are often beneficial but may be painful and cannot be applied to many nails. All systemic treatments clearing widespread skin lesions usually also clear the nail lesions. Recently, biologicals were introduced into nail psoriasis treatment and found to be very effective. However, their use is restricted to severe cases due to high cost and potential systemic adverse effects.
Introduction
Psoriasis is a chronic inflammatory disease with a strong genetic background but highly influenced by environmental factors. Its prevalence is ~1–2% of the world population with considerable differences among regions and individuals with different skin types. It is the skin disease that most frequently affects the nail. At the time of consultation, roughly one half of the patients suffer from nail changes. Over lifetime, up to 90% of all psoriatics will have had nail alterations. The prevalence of nail psoriasis is even higher in psoriatic arthritis.Citation1 Nail lesions often appear around 10 years later than skin lesions, which may in part be the reason for nail psoriasis being observed less frequently in children. In general, cutaneous psoriasis is more severe in individuals with nail involvement.
Etiology and pathogenesis
Neither gender nor race predilection appears to exist. There is no association of HLA-C0602 with nail and joint involvement, but nail psoriasis is often associated with an inflammation at the insertion points of tendons and ligaments giving rise to enthesitis. Thus, the nail lesions were believed to represent an abnormal response to tissue stressing of the integrated nail-joint apparatus, rather than being due to autoimmunity. The nail and joint disease may be linked to tissue-specific factors, including tissue biomechanical stressing and microtrauma, that lead to activation of aberrant innate immune responses.Citation2 However, a case of skin and nail psoriasis definitely disappearing after allogeneic bone marrow transplantation is more in favor of predominant immunogenetic factors.Citation3
Clinical characteristics of nail psoriasis
Psoriasis causes a variety of both specific as well as ambiguous nail lesions. Fingernails are more frequently affected than toe nails, probably because they grow faster. Particularly, for scientific purposes, nail psoriasis is often divided into matrix and nail bed involvement or both, which is also reflected in many trials differentiating the response into general, more on matrix or nail bed psoriasis. Pits are the most characteristic and most frequent signs and are seen as small, sharply delimited depressions in the nail surface. They are of remarkably even size and depth. Their distribution may be haphazard or they may sometimes be arranged in parallel transverse or short longitudinal lines. They are the result of tiny psoriatic foci in the apical matrix producing parakeratosis, which breaks off when it grows out from under the proximal nail fold then leaving these depressions. Sometimes, the para-keratosis remains and is seen as an ivory-colored spot in the proximal half of the nail plate. Pits may be single, which is not yet psoriasis specific, or multiple. Ten pits in one nail or >50 pits on all nails are regarded as proof of psoriasis. Red spots in the lunula usually represent a very active psoriasis lesion with dilatation of the capillaries and thinning of the suprapapillary plate. Red or mottled lunulae are due to the dilatation of matrix blood vessels.Citation4
Total matrix affection results in complete nail destruction with crumbling of the plate, whereas leukonychia is seen when the mid- to distal matrix is affected and parakeratotic cells are incorporated into the nail plate making it optically opaque. In most cases, psoriatic leukonychia is an ill-defined white transverse band. Splinter hemorrhages are very narrow, some millimeters long reddish-darkbrown to black streaks. They are analogous to Auspitz’s phenomenon of the skin and either due to hemorrhage from the dilated capillaries in the nail bed or due to blood clots in these longitudinally arranged small vessels. Salmon or oil spots are very frequent and represent psoriatic plaques in the most distal matrix and the nail bed. This area looks like paper on which a drop of oil has fallen: a yellowish-brownish spot with a red margin shines through the plate because the psoriatic squames compressed under the nail are imbibed with serum. When a salmon spot reaches the hyponychium, the parakeratosis breaks out and psoriatic onycholysis develops. This typically has a reddish proximal margin differentiating it from most other causes of onycholysis, such as onychomycosis. Subungual hyperparakeratosis may be thick and then no oil drop phenomenon is seen. The hyperkeratosis may be very marked and at times so extreme as to resemble pachyonychia congenita. Psoriasis affecting the dorsal as well as the ventral surface of the proximal nail fold results in swelling and rounding of its free edge. This leads to a spontaneous loss of the cuticle characterizing the pattern of chronic paronychia.
As mentioned earlier, psoriatic arthritis is very frequently associated with severe nail involvement and psoriatic paronychia, complete nail destruction, and swelling of the distal interphalangeal joint. This has a serious negative influence on the quality of life.
In contrast, psoriatic pachydermoperiostosis is closely related to psoriatic arthritis but usually without obvious nail changes. Mainly the big toe is considerably swollen and often painful.
Three different forms of pustular psoriasis are differentiated. Nail changes are seen in all of them. The nail changes in the palmar plantar pustular psoriasis of Barber–Königsbeck are similar to the common type of psoriasis, but the surface defects may be larger and are called elkonyxis. Yellow subungual spots represent large Munro’s abscesses. Subungual abscesses are frequent in the generalized pustular psoriasis of von Zumbusch. Acrodermatitis continua suppurativa of Hallopeau is the most notorious form of pustular psoriasis of the nails. It often begins with one single digit where the skin of the distal phalanx turns red and develops some pustules migrating under the nail and causing nail dystrophy. With time, the entire nail unit may disappear leaving a red smooth digit tip until the disease slowly wanes off. Less frequently, acrodermatitis continua suppurativa may initially involve several fingers and toes and run a rapid and severe course. Recently, a mutation in the interleukin 36 receptor antagonist gene leading to a defect in interleukin 36 antagonist was identified in generalized pustular psoriasis and acrodermatitis continua suppurativa supporting the view that it belongs to the autoinflammatory diseases group.Citation5,Citation6 Pustulosis palmoplantaris is histopathologically and genetically different and rarely affects the periungual skin.Citation7
Reiter’s disease is also known as reactive arthritis. It is a systemic condition with characteristic joint, mucosal, eye, genito-urinary, skin, and nail changes. The latter are very similar to pustular psoriasis. However, they often have a more brownish tint due to a higher content of erythrocytes in the pustules. Histopathology with extensive spongiform pustules is virtually identical to pustular psoriasis.Citation8
Nail psoriasis in children
Psoriasis may occur at any age. Although rare, it was also observed in the newborn. Erythrodermic psoriasis in children usually shows ungual involvement with nail dystrophy and marked subungual hyperkeratosis similar to pityriasis rubra pilaris. Even pustular psoriasis and psoriatic arthritis were observed in children.Citation6
Diagnosis of nail psoriasis
In most cases, nail psoriasis follows cutaneous psoriasis and is therefore easy to diagnose. However, ~5% of nail psoriasis occurs isolated and may pose diagnostic challenges. This is particularly the case when even the nail alterations are atypical such as a single nail in a child or of a toe, isolated nail bed psoriasis without pits and salmon spots. Histopathology is usually diagnostic, provided the biopsy is sufficient, which is, unfortunately, often not the case. It has to be remembered that matrix lesions cause changes of the nail plate and those of the nail bed are seen under the nail plate. The biopsy has to be taken slightly more proximal than anticipated and must include enough subungual soft tissue. In contrast, nail clippings are diagnostic for the most important differential diagnosis, the various onychomycosis forms, and sometimes give a strong hint at nail psoriasis. Furthermore, nail psoriasis exhibits some features not commonly seen in cutaneous lesions.Citation1 Dermatoscopy makes the clinical signs more obvious and helps in the diagnosis. Videodermatoscopy allows higher magnifications than the usual hand-held dermatoscopes. Capillaroscopy shows the dilated tortuous capillaries of the proximal nail fold. This is even better visible in laser confocal microscopy. The features of high-frequency ultrasound are less reliable but may be of help for the very experienced. Optical coherence microscopy uses a similar principle but has a much higher resolution.
Differential diagnosis
In most cases, nail psoriasis is diagnosed on clinical grounds.Citation8 Skin lesions elsewhere with one or several psoriatic nail features suggest the correct diagnosis. With a good biopsy, histopathology is usually pathognomonic and helps to delineate nail psoriasis from other conditions, particularly onychomycosis. The clinical diagnosis of pustular psoriasis is made on the basis of red skin areas with a rim of small pustules. Reiter’s disease requires additional laboratory examinations.Citation1
Onychomycosis is said to be the most frequent nail disease. It has many features in common with nail psoriasis, both clinically and histopathologically ().Citation1
Table 1 Differential diagnosis of nail psoriasis and onychomycosis
Another important differential diagnosis is the asymmetric gait nail unit syndrome seen mainly in the big toenail as an onycholysis without further criteria of nail psoriasis or onychomycosis.Citation9 Furthermore, nonspecific nail dystrophy, particularly of toenails, is very common in the elderly, in subjects with peripheral arterial disease, chronic venous stasis, after trauma to the leg, in peripheral neuropathy, and in some dermatoses such as eczema, nail lichen planus, Darier’s disease, Hailey-Hailey disease, alopecia areata, and many drugs.Citation1,Citation8
Grading and assessment of nail psoriasis
Reliable repeatable specific validated severity and outcome measures are necessary to evaluate a disease and its response to a specific treatment.Citation11 This was missing in nail psoriasis until the nail psoriasis severity index (NAPSI), target NAPSI, and its many variants were established.Citation12 NAPSI is calculated by dividing each nail into four quadrants. Each quadrant is evaluated for the presence of psoriasis manifestations of the nail matrix, such as pitting, leukonychia, red spots in the lunula, and nail plate crumbling, as well as of the nail bed, such as oil-drop phenomenon, onycholysis, subungual hyperkeratosis, and splinter hemorrhages. If any of these signs is present in all four quadrants, a score of 4 is given. A score of 0 represents no signs in any quadrant. Each nail is evaluated for a matrix and a nail bed score of 0–4. They are combined to yield a maximal score of 0–8 for each nail. All nails may be evaluated, with the total NAPSI score being the sum of the scores, up to 80 if only fingers are considered, or up to 160 if fingers plus toes are included.Citation12 If only the most seriously affected nail is evaluated, it is called target NAPSI; this is often done to assess the effects of a therapeutic regimen.Citation11 Many therapeutic studies use (target) NAPSI-50, NAPSI-75, and NAPSI-90 to indicate the percentage of patients that reach a (target) NAPSI improvement of 50, 75, or 90%, respectively. The NAPSI has some disadvantages, such as being too time-consuming to be used in clinical practice, and that the NAPSI scores often do not correspond with the clinical severity of nail psoriasis.Citation13 A new scoring system, the N-NAIL, overcomes many of these limitations, but it has yet to prove its clinical practicability.Citation13 The use of many different scoring systems, major differences in study design, inclusion criteria, and follow-up make it difficult if not impossible to compare the results of most nail psoriasis trials.Citation11 In addition, subjective and objective patient factors such as quality of life, satisfaction with treatment ease and outcome, adverse effects and not the least practicability, and cost of treatment are important factors.Citation11 Such an evaluation and assessment tool for nail psoriasis has recently been published under the term of nail assessment in psoriasis and psoriatic arthritis.Citation14
Associations
Psoriasis is a frequent skin disease. In the last decades, a metabolic syndrome associated with psoriasis has been described; however, this is not of particular importance for ungual psoriasis except in psoriatic arthritis. Associations and co-occurrence with other skin disorders involving the nail are rather common. The most important differential diagnosis is onychomycosis. Both conditions may look very similar. A psoriatic nail may be colonized with pathogenic fungi, and a true infection of the psoriatic nail is not infrequent ().Citation1,Citation15
Impact on quality of life
Nail psoriasis has a profound negative influence on all aspects of quality of life as well as on daily, sports, and professional activities.Citation16–Citation20 Women try to hide their nails and cover them with nail lacquer; although common nail varnishes are not harmful, artificial nails, particularly when long, increase the mechanical stress and strain to the nail plate – nail bed attachment acting as a Köbner phenomenon and worsening nail psoriasis. Similarly, professional activities with particular use of the fingers may have a deteriorating effect on the disease. Matrix involvement scores higher than pure nail bed affection as it results in more obvious nail plate damage.Citation19
Course
Nail psoriasis is chronic but often improves and worsens without known reasons (–). Trauma may play an important role in the exacerbation of nail psoriasis. There may be periods without any nail alterations.Citation1,Citation8,Citation10
Figure 1 The thumbs of the patient mainly show nail bed involvement with subungual hyperkeratosis, salmon spot, and onycholysis.
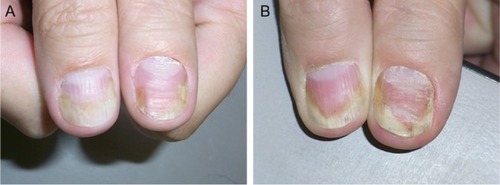
Figure 2 Further development of the nail psoriasis.
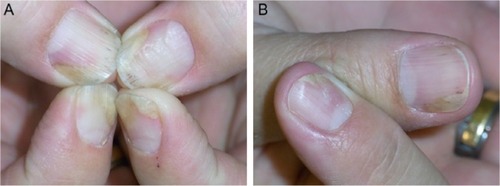
Figure 3 As topical and injection treatments are insufficient and inconvenient, systemic methotrexate is instituted.
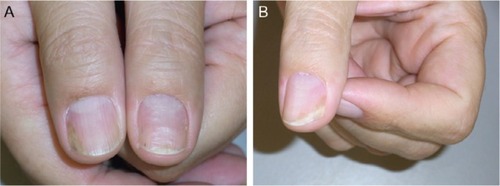
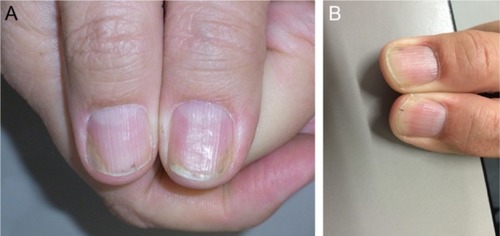
Figure 4 There is residual nail bed psoriasis under methotrexate therapy. Finally, a biological treatment is instituted.
Management of nail psoriasis
Management of the disease includes patient education, avoidance of trauma to the nails, and different therapeutic approaches with physical and pharmaceutical procedures and agents.
Patient counseling includes education on the nature of psoriasis, how life may be influenced by nail involvement, about the specific problems of treatment, that nail psoriasis is not due to an allergy or an “unhealthy” diet and thus is not treatable with particular foods. However, smoking increases the risk of psoriasis and obesity and alcohol use are associated with a higher risk for psoriasis. It is important to avoid trauma to the nail unit that will inevitably exacerbate the condition or induce recurrences. Manicure and nail cleaning have to be performed cautiously without further traumatizing the hyponychium and attachment of the nail to the nail bed. It is helpful to explain that genes are the most important etiological factors and that the skin and nail lesions are amenable to treatment but that the genes cannot be corrected. Many genes contribute to the psoriatic personality, which may explain the enormous variability of the clinical features including the response to treatment. Particularly, chronic repeated trauma is thought to be an aggravating factor. The development of pits may be the result of microtraumata to the enthesis of the extensor tendon and the dorsal aponeurosis of the distal interphalangeal joint.Citation2 They may be masked using nail varnish.
All nail psoriasis treatments require a long time, as the nail is a slow-growing cutaneous appendage. The effect of any treatment can usually not be evaluated before 3–6 months, and it may take a year or longer to reach the maximum improvement achievable with a given therapy. Pretreatment photographs are highly recommended and should be repeated at all follow-up visits to show the therapeutic result to the patients. Concomitant onychomycosis may prevent clinical cure, and it is a must to exclude fungal infection when starting nail psoriasis therapy; a single remaining altered nail during an otherwise efficacious therapy may be a hint at a concomitant mycotic infection.Citation1,Citation21
Many different therapeutic measures are available. Their choice depends on various factors such as severity of nail involvement and its impact on quality of life, associated skin lesions, psoriatic arthritis, comorbidities, profession, age, patient preferences, potential risks, and not the least costs and their reimbursement.
Nail psoriasis is very recalcitrant to almost all topical treatments, whereas systemic therapies clearing the skin are usually effective also in nail psoriasis.Citation22 The problem of all topical drugs is their limited penetration to the diseased tissue: through all layers of the proximal nail fold with the underlying nail in matrix lesions, through the nail plate, and subungual hyperkeratosis in nail bed psoriasis. Hence, pits, though often being rather inconspicuous, are the most resistant to treatment. Nevertheless, a 3-month trial of a potent antipsoriatic topical preparation is warranted (). The less nail is left the easier the penetration of the drug to the very psoriatic lesion is. Clipping the onycholytic nail over the nail bed is essential to reach nail bed psoriasis. Thinning the nail by filing or grinding, or drilling holes into the nail plate with mechanical burrsCitation23 or with ablative lasers, is often used to enhance nail penetration.Citation24
Corticosteroids are often used in nail psoriasis. They have to be class IV (high potency) and applied once or twice a day on the proximal nail fold in case of matrix and on the nail plate in nail bed affection. Although probably still the most commonly used drugs, corticosteroids were rarely tested in controlled studies. Both clobetasol and betamethasone dipropionate were tested in clinical trials and showed comparable resultsCitation11 concerning pitting, salmon patches, subungual hyperkeratosis, and onycholysis.Citation25,Citation26 All high-potency steroids carry the risk of skin atrophy when used on the proximal nail fold, often associated with hypopigmentation. Whether or not using them for 4–5 days a week as a “pulse” treatment is equally effective and reduces this risk remains to be proven. Clobetasol 8% was tested as a nail lacquer with good results depending of the duration of the treatment.Citation27
Perilesional injections are another type of local treatment. This increases the concentration of the drug at the site of disease while minimizing the dose for the whole organism. Perilesional injection of corticosteroids is by far the most often performed (), either by injection with a needle or by high air-pressure devices.Citation28 Injection with a 30 G needle and using some distraction techniques such as vibration and pressure around the area to be injected make the procedure tolerable although some patients prefer the needle-less technique. Apparently, the efficacy of different high-pressure injectors varies considerably (O Correia, Inst CUF, personal communication, 2014). We inject 0.1 mL of a triamcinolone acetonide suspension (10 mg/mL) into both sides of the proximal nail fold; injection into or under the nail bed is extremely painful and requires prior anesthesia.Citation29,Citation30 The injections are repeated on a monthly basis for 6 months and, then, followed by every 6 weeks and later every other months. However, not all patients tolerate the injections. Matrix and nail bed signs of psoriasis respond slightly differently with salmon spots and subungual hyperkeratosis usually showing the best effect. Adverse effects are not uncommon with subungual hematoma and temporary nail deformation being relatively frequentCitation29,Citation30 and the disappearing digit, atrophy of the terminal phalanx bone, and rupture of the extensor tendon being the most serious ones.Citation31–Citation34 Epidermoid inclusion cysts were observed after jet injections necessitating amputation.Citation35
The combination of the vitamin D3 derivate calcipotriol and a potent corticosteroid, such as betamethasone dipropionate, has shown good results;Citation26,Citation27 personal experience has shown that twice or even thrice daily application may be worth trying. Another vitamin D derivative, such as tacalcitol, was used alternatively with 8% clobetasol nail lacquer.Citation33
Vitamin D3 (calcitriol) and its analogs calcipotriol and tacalcitol are well established in the therapy of psoriasis vulgaris due to their effects on epidermal differentiation and proliferation and regulation of production and release of proinflammatory cytokines.Citation11 Most studies were done with calcipotriol and tacalcitol.Citation36,Citation37 Apparently, their effect on nail bed lesions is more marked than on matrix signs.
Calcineurin inhibitors have a profound inhibitory effect on T-cell functions that are implicated in the pathogenesis of psoriasis. Used systemically, cyclosporin A (CyA) is highly active against psoriasis, but topical application of CyA showed ambiguous results.Citation11 The new calcineurin inhibitor tacrolimus shows much better skin and nail penetration. It demonstrated good activity on nail bed and matrix psoriasis in a controlled study.Citation38 No studies with pimecrolimus were published until now.Citation11
Tazarotene is a synthetic retinoid with antiinflammatory and antiproliferative actions on keratinocytes. Tazarotene 0.1% was used for the treatment of nail psoriasis. The results were variable, but one study compared it with clobetasol showing equal results.Citation25 It was also used in childhood nail psoriasis.Citation39 Side effects are mainly skin irritation with redness and desquamation.Citation11
5-Fluorouracil (5-FU) is an antimitotic and antiproliferative agent, which is active against disorders with a high proliferative activity, such as psoriasis. Only one study of topical 5-FU with 20% urea as a penetration enhancer showed good effects on nail psoriasis, but inflammation, infection, onycholysis, and discoloration were observed as adverse effects.Citation40 Other investigators did not see a beneficial response. This does not make 5-FU a favorite nail psoriasis agent.Citation11
Dithranol was once the most commonly used antipsoriatic topical, but because of its unpleasant cosmesis, it is rarely used nowadays. One study reported some improvement of nail bed lesions, but the staining of the nails made it unacceptable.Citation41
Indigo naturalis extract regulates proliferation and differentiation of epidermal keratinocytes, restores the epidermal barrier function, and inhibits inflammatory reactions. Twice daily application of an oily extract reduced nail bed lesions such as hyperkeratosis and onycholysis by about one half; it was thus more effective than calcipotriol solution.Citation42,Citation43 Studies are in progress to make it colorless and cosmetically more acceptable (CH Yang, Chang Gung Memorial Hospital, personal communication, May 8, 2017).
Methotrexate was also used for perimatrical and nail bed injections with acceptable results. The dose was 0.1 mL of a 25 mg/mL solution. Good results were seen after 6 months and 15 weeks, respectively.Citation44,Citation45
Systemic treatments are indicated in widespread psoriasis. Those therapies proven successful for skin lesions usually also improve nail psoriasis. However, many physicians and patients are reluctant to treat isolated ungual psoriasis systemically. A European Consensus Paper on the treatment of psoriasis defines the involvement of particularly sensitive areas such as the head and neck, genito-anal area, and nails as moderate to severe. The selection of the mode of treatment then depends on the severity of the nail disease, its impact on quality of life, on professional, sports, and social activities, and in particular on potential associated psoriatic arthritis.
Systemic corticosteroids are not a good option for psoriasis vulgaris and in particular for nail psoriasis. High doses are necessary with a considerable risk of serious side effects, break-through phenomena, and development of pustulation of hitherto not pustular psoriasis.
Methotrexate has been introduced into the treatment of cutaneous psoriasis and psoriatic arthritis in the 1960s. It is an inexpensive drug with good efficacy in skin lesions; however, as an antimetabolite, it slows down the nail growth rate and improvement in nail lesions is therefore often slow and seen very late (). Furthermore, there is a risk of severe side effects such as hepatotoxicity, lymphopenia, lekopenia, nausea, and erosive stomatitis. Long-term toxicity includes liver, lung, and heart fibrosis. The dose is usually slowly increased to reach ~10–20 mg/week. Both oral and injection therapies are possible with virtually equal doses as the bioavailability of methotrexate is very good.Citation46–Citation48 NAPSI improvement is between 25 and maximally 50%. Methotrexate has also been injected intralesionally with a good result.Citation44,Citation45
Ciclosporin A is another established systemic antipsoriatic drug. It is a calcineurin inhibitor with strong immunosuppressive action. Its positive effect on cutaneous and ungual psoriasis is well established, both in single-drug studies as well as in comparative ones.Citation49,Citation50 The dose is usually 3–5 mg/kg daily, but half the dose is often given in Japan after initial improvement.Citation51 Although ciclosporin is probably the most active “classical” systemic antipsoriatic drug, it is limited to a treatment period of 6–12 months because of potentially serious adverse effects such as disturbance of renal function, arterial hypertension, diabetes mellitus, nausea, hypertrichosis, gingival hyperplasia, paresthesia, fatigue, and headache.
Synthetic retinoids have been used to treat extensive skin psoriasis. The first of these drugs was etretinate. Although it had a good effect on nail changes in some cases,Citation52,Citation53 etretinate is no longer used and substituted by its derivative acitretin.
Acitretin is the follower product of etretinate with a shorter half-life in the body. It is usually given in a dose of 0.5–1 mg/kg/day.Citation54,Citation55 Its action is slow and, in most cases, does not reach >50% improvement of nail psoriasis.Citation56 All retinoids have a number of side effects, particularly when given in a dose >0.5 mg/kg/day, such as dry and cracking lips, dry mouth, hair loss, and in children ossification disturbances. High-dose retinoids can have an onychodestructive effect and are no longer recommended as the first-line nail psoriasis treatment;Citation57 however, good results were seen in generalized pustular psoriasis and acrodermatitis continua suppurativa.Citation57 Acitretin is occasionally used in combination with photochemotherapy with ultraviolet (UV) A and narrow band UV B.
Fumaric acid esters are used for psoriasis treatment in some countries, mainly in Europe, but their use was somewhat controversial. A case report described a good effect on nail psoriasis.Citation58 Side effects are mainly gastrointestinal, flushing, lymphopenia, and rarely renal dysfunction.
Leflunomide is a disease-modifying antirheumatic agent with an effect on psoriatic arthritis and also a modest action on nail psoriasis.Citation59 Sulfasalazine was used in one patient with a beneficial effect.Citation60 Silicic acid was given orally and topically on skin lesions. Ten of the 12 patients treated had nail lesions, and five of them cleared completely, although the nails were not treated with the silicic acid gel; thus, a systemic effect was postulated.Citation61
Apremilast is a new small-molecule oral phosphodiesterase 4 inhibitor reducing the expression of several proinflammatory mediators; it is more an antiinflammatory than immunosuppressive agent distinguishing it from most other systemic antipsoriatic compounds. It has an excellent safety profile with no known organ toxicity, thus obviating the need for laboratory controls.Citation62 It is approved for the treatment of cutaneous psoriasis and psoriatic arthritis and has shown a good effect in nail psoriasis, although only after 32 weeks. Its cost may, however, limit its widespread use.Citation63,Citation64 A nail lacquer containing apremilast is being developed;Citation65 however, human studies on nail psoriasis have not yet been published.
Tofacitinib is a small-molecule oral Janus kinase inhibitor interfering in the JAK–STAT pathway. It is active against psoriasis and alopecia areata including their nail manifestations. In four Phase III randomized controlled studies and compared to etanercept, a twice daily dose of 5 or 10 mg was shown to be noninferior to etanercept injected subcutaneously twice weekly with sustained effects up to 52 weeks.Citation66–Citation69
Biologicals are a new development in the treatment of many, mainly immunologically mediated diseases, among them also psoriasis. There are several classes, both concerning the nature of the antibody as well as their target, such as humanized and fully human antibodies and antibodies to tumor necrosis factor-α, various interleukins, and T-cell inhibitors, respectively. They all have profound immunosuppressive actions and are thus not without risk, particularly concerning infections and re-activation of tuberculosis, to mention but a few.Citation11 Biologicals are usually considered second- or third-line treatments when other established topical and systemic antipsoriatic drugs were not or not sufficiently active in suppressing nail lesions.Citation70 In contrast, nail psoriasis was found to be an indicator of poor prognosis for the treatment of psoriasis with biologicals independent of the specific substance used.Citation71 In most cases, nail psoriasis responses lag behind those of cutaneous psoriasis, which can in part be explained by the slow growth of nails as nail plate changes have to grow out, whereas nail bed changes may be seen earlier. In comparison with “classical” systemic drugs, eg, methotrexate and cyclosporin, biologicals often show a dramatic and more rapid improvement. However, only 20–57% of the patients reach a 90% improvement of their NAPSI score with biologicals and the effect is lost after 47 months in average.Citation72,Citation73 The most likely mechanism is the formation of antidrug antibodies, but compensatory production of other proinflammatory cytokines and a particular individual reaction may be the cause that many patients stop this treatment.Citation74 In many countries, biologicals are not automatically reimbursed by the social health insurance and patients and physicians have to give evidence that previous, less expensive treatments were not sufficiently efficacious.
TNF-α inhibitors were the first biologicals developed for psoriasis treatment. TNF-α is a cytokine with proinflammatory action that induces keratinocyte proliferation and prevents apoptosis. Most experience was gained with infliximab, the first of this group, but in general, the efficacy of all TNF-α inhibitors currently available for psoriasis treatment is virtually comparable. Also their side effects and limitations are the same. Activation of opportunistic infections, congestive heart failure, demyelinating disorder, antibodies against TNF-α inhibitors, and rarely lupus erythematosus may occur.Citation11
Infliximab is a chimeric human-mouse IgG1 antibody binding membrane-bound and soluble TNF-α. This reduces epidermal T-lymphocyte infiltration. It exhibits certain antigenicity and may thus induce autoantibodies that may reduce its effectiveness thus requiring higher doses with time. It has to be given intravenously, and ~16% of the patients develop infusion reactions such as fever, chills, flush, urticaria, myalgia, arthralgia, nausea, hypotension, and dyspnea.Citation75 Infliximab was associated with a higher rate of onychomycosis compared to the other TNF-α inhibitors.Citation76 Patients with a high psoriasis area severity index (PASI) response also show a good NAPSI response. Almost one half of the patients demonstrated complete nail clearance after 50 weeks. NAPSI reduction by 50% was achieved by almost all patients, 80% reached NAPSI-75, 30% reached NAPSI-90, and 10% cleared completely.Citation77 Infliximab appears to be the fastest acting TNF-α inhibitor. Its dosage is usually 5 mg/kg given on weeks 0, 2, and 6 and if necessary 8.
Adalimumab is a human monoclonal IgG1 antibody against TNF-α. It binds to cell surface proteins of the TNF-α receptor preventing its action. Its mechanism of action is similar to that of infliximab. Roughly 50–60% of NAPSI improvement are achieved.Citation11,Citation78
The combination with cyclosporin was shown to be particularly effective reaching a reduction of the NAPSI score of 100%.Citation79 Adalimumab did not increase the rate of onychomycoses.Citation76 The dose is 80 mg at baseline, then 40 mg every 2 weeks, but some authors gave 40 mg from the beginning ().Citation11
Certolizumab pegol is a PEGylated TNF-α inhibitor that is Fc free. It is effective in the treatment of rheumatoid arthritis and psoriasis with efficacy in nail psoriasis, enthesitis, and dactylitis.Citation80,Citation81
Being a fusion of the TNF receptor with the Fc part of the IgG1 antibody etanercept blocks the action of TNF-α. Thus, its mechanism of action is similar to that of infliximab and adalimumab. Several reports on its use in nail psoriasis demonstrated good results.Citation82 There was no statistically different outcome with 50 mg once or twice weekly after 12 weeks and target NAPSI improvement between 71 and 76%.Citation83 It was also effective in refractory acrodermatitis continua suppurativa.Citation84
Golimumab is another TNF-α inhibitor approved for psoriatic arthritis with an effect on nail psoriasis. Target NAPSI improvement was over 40% after 24 weeks and 52% after 52 weeks of treatment with 50 mg every 4 weeks.Citation85,Citation86
All TNF-α inhibitors have the potential to paradoxically worsen psoriasis or even induce it.Citation87,Citation88 In many cases, this regresses despite continuation of the therapy or when another biological is used. This is apparently independent from the condition for which TNF-α inhibitors were administered.Citation88–Citation91 The mechanism of action may be an unabated interferon-α production by plasmacytoid dendritic cells, which might result in psoriasis flares and induction of psoriasiform lesions.Citation91,Citation92
T-cell inhibitors such as alefacept and efalizumab are not widely used because of their considerable adverse effect profile.Citation93 Efalizumab is a monoclonal CD11a antibody and was withdrawn from the market because of cases of leukencephalopathy observed under treatment with this molecule. Alefacept is a fusion protein binding at the CD2 portion of the leukocyte function antigen-3 linked to the Fc portion of human IgG1 and targets T lymphocytes. No studies to evaluate the efficacy of these drugs in nail psoriasis were published.
Rituximab causes B-cell depletion. Its role in the treatment of nail psoriasis is not yet examined.Citation93,Citation94
New biologicals focus on the inhibition of interleukins involved in the propagation of the psoriatic process. Their nonspecific immunosuppressive action is less pronounced compared with the TNF-α inhibitors. The targets are mainly IL-12/IL-23 and IL-17. However, it was shown that anti-IL-12 action might be proinflammatory under certain circumstances and thus counterproductive for the therapy of psoriasis.Citation95
Anti-interleukin 17 therapy is based on the fact that IL-17 plays a central role in the development of psoriatic lesions, but IL-17 is also important for the defense against extracellular pathogens and recruits neutrophils.
IL-17 inhibitors are secukinumab, ixekizumab, and brodalimumab, but there are no ongoing studies with the last one.
Secukinumab is a human monoclonal IL-17A antibody approved for plaque psoriasis and psoriatic arthritis that has also shown good efficacy in nail psoriasis. It has an early onset action and a sustained effect. Its safety profile is acceptable. It is administered subcutaneously with a 300 mg dose at weeks 0, 1, 2, 3, 4, and then every 4 weeks. At 16 weeks, both 150 and 300 mg secukinumab were superior to placebo with further improvement with longer treatment periods.Citation96,Citation97
Ixekizumab is another humanized monoclonal antibody directed against IL-17A recently approved for psoriasis. It demonstrated significant improvement of the NAPSI score as early as 2 weeks after start of the treatment, which sustained to week 20 when given in a dose of 75 mg at weeks 0, 2, 4, 8, and 12 and then 120 mg every 4 weeks from week 20 onward.Citation98,Citation99
Brodalumab is a human monoclonal IL-17A antibody active against plaque psoriasis. It was more active than ustekinumab in a head-to-head comparison. Although approved in the US and Japan, the clinical development was terminated as suicidal ideation and behavior were observed.Citation100
IL-23 is another important proinflammatory cytokine involved in the pathogenesis of psoriasis.
Antibodies targeting the p40 subunit of IL-23 also have an action against IL-12 as they both share this subunit. Antibodies directed against the p19 subunit are selective for IL-23.
Ustekinumab is a monoclonal antibody directed against the p40 subunit of IL-12/23. It is active against psoriasis and psoriatic arthritis and was also shown to have a good action on nail psoriasis. Nail improvement was observed from week 4 onward with significant improvement of 90% at week 40. NAPSI and PASI improvement ran parallel. The dose is 45 and 90 mg if the weight is over 100 kg, usually at weeks 0, 4, 16, and 28.Citation101–Citation103 Efficacy and side effects are comparable to the other IL inhibitors.
Briakinumab was another monoclonal antibody directed at p40. After showing good clinical results, its development was stopped because of severe infections and a higher incidence of other severe side effects.Citation104
Guselkumab is a fully human IgG1k monoclonal IL-23 antagonist directed against the unique p19 subunit of IL-23; it has no anti-IL-12 component. It has a profound action on moderate-to-severe plaque psoriasis and was superior to adalimumab.Citation105 The dose given was 100 mg at weeks 0, 4, 12, 16, and 20 and then every 8 weeks.
Tildrakizumab and BI-655066 are also targeting the p19 subunit of IL-23. They are currently being studied for various indications including psoriasis.Citation106,Citation107 No results are yet available concerning nail psoriasis.
In summary, most new biological drugs have a good and reliable action on nail psoriasis with an acceptable adverse effect profile. They are more active than most of the classical systemic antipsoriatic drugs.
Radiotherapy is an “old“ treatment modality, which has come out of time not only because of potential long-term adverse effects but also because most dermatologists no longer operate X-ray machines because of the difficulties to comply with the bureaucratic challenges associated with the use of therapeutic ionizing rays. However, some studies report favorable results with Grenz rays,Citation108 superficial X-rays,Citation109,Citation110 and electron beam therapy.Citation111
Light has been used for a long time, but as nails are virtually impermeable for UV B and allow <2% of UV A to penetrate, the effect is rather limited.Citation112 Potentiation of UV by specific photosensitizers, called photochemotherapy, was beneficial in some studiesCitation48,Citation113 but is often associated with multiple melanonychias.Citation114
Intense pulsed light (IPL) is a broad-spectrum light source with a high-energy intensity. With a 550 nm filter, it has been used for the treatment of plaque psoriasis. A trial on 20 patients with finger and toenail psoriasis using IPL with a cutoff filter of 550 nm and a median of 8.6 sessions resulted in significant improvement in the NAPSI with nail bed lesions showing a reduction of 71% and matrix lesions of 32%. A relapse was seen in three patients after 6 months.Citation115
Lasers have also been used to treat nail psoriasis. The pulsed dye laser (PDL) is the device of choice as it targets the dilated capillaries in the matrix and nail bed. In many studies, 1.5–6 ms pulses were used with a good effect on matrix and nail bed lesions.Citation116,Citation117 A comparative study using 6 ms pulse length and 9 J/cm2 and 0.45 ms and 6 J/cm2 gave almost the same improvement of matrix and nail bed lesions with significantly less pain with the shorter pulse.Citation118 Side effects are mainly pain, hemorrhage, and pigmentation. These results were confirmed in another trial.Citation119 PDL with tazarotene was significantly more effective than tazarotene alone.Citation120 A comparison of the PDL with the excimer laser gave significantly better improvement with the PDL.Citation121 In another comparative study, PDL was compared with the Nd:YAG laser. Both groups were treated with calcipotriol betamethasone in addition. Whereas the results were comparably good, the Nd–YAG was significantly more painful.Citation122
Photodynamic therapy (PDT) uses light and a photoactive substance that both generate reactive oxygen species able to kill those cells that accumulated the photosensitizer. In a comparative study, no difference was found between PDL and PDT.Citation117 However, there is considerable heat development during the illumination of the target and this is often not tolerated by the patients.
Conclusion
Nail involvement in psoriasis is common. It is an indicator of poor prognosis and of a higher risk to develop psoriatic arthritis. Surprisingly, nail psoriasis is only briefly mentioned in most national and European guidelines on the diagnosis and treatment of psoriasis; however, the European Nail Society is now working on recommendations for the treatment of nail psoriasis.
The many treatments available give evidence that hitherto none is the ideal therapy. Topicals have to fight with the difficulties to get through the nail and nail fold to the diseased structures. Injections that bring the remedy to the site of the disease process and greatly avoid systemic effects are painful and carry the risk of local side effects. Systemic drugs are often not used for isolated nail psoriasis, although this is accepted as a severe psoriasis considerably impairing quality of life. However, it is known that virtually all systemic treatments that improve the skin lesions are also beneficial for the nails, although often with a delayed and less pronounced response. The potential systemic adverse effects have to be kept in mind before and during such a therapy. The development of new biologicals has revolutionized psoriasis treatment and thus also that of ungual psoriasis. Finally, there are some physical modalities such as ionizing rays, various light qualities including photodynamic treatment, and lasers.
Many treatment possibilities may make it delicate to choose the right approach. It is certainly wise to begin with a topical antipsoriatic preparation (). This has to be used for a minimum of 4–6 months before its efficacy can be evaluated. If this does not help sufficiently, a classical antipsoriatic drug such as methotrexate, fumaric acid ester, and cyclosporine would be the second choice while keeping in mind all potential contraindications. If the results are not satisfying a biological may be chosen. Again, there are many contraindications that have to be carefully looked for before starting such a treatment. The choice is huge now, and the treating physician has to select among TNF-α blockers, agents interfering with T-lymphocyte functions, and IL-23 and IL-17 inhibitors.
Table 2 Treatment algorithm for nail psoriasis
In summary, nail psoriasis is still an underestimated part of psoriasis, but the outlook is bright with many new treatments available.
Disclosure
The author reports no conflicts of interest in this work.
References
- HanekeENail disordersGoldsmithLAKatzSIGilchrestBAPallerASLeffelDJWolffKFitzpatrick’s Dermatology in General Medicine9th edNew YorkMcGraw-HillIn press2017
- McGonagleDTanALBenjaminMThe nail as a musculoskeletal appendage-implications for an improved understanding of the link between psoriasis and arthritisDermatology20092189710219060455
- YokotaAHukazawaMNakasekoCResolution of psoriasis vulgaris following allogeneic bone marrow transplantation for aplastic anemiaRinsho Ketsueki199637135398683865
- Peña-RomeroAToussaint-CaireSDomínguez-CheritJMottled lunulae in nail psoriasis: report of three casesSkin Appendage Disord201621–2707127843929
- MarrakchiSGuiguePRenshawBRInterleukin-36-receptor antagonist deficiency and generalized pustular psoriasisN Engl J Med2011365762062821848462
- KelatiABaybayHNajdiAZinouneSMernissiFZPediatric psoriasis: should we be concerned with comorbidities? A cross sectional studyPediatr Int201759892392828452100
- Misiak-GalazkaMWolskaHRudnickaLWhat do we know about palmoplantar pustulosis?J Eur Acad Dermatol Venereol2017311384427521275
- JiaravuthisanMMSassevilleDVenderRBMurphyFMuhnCYPsoriasis of the nail: anatomy, pathology, clinical presentation, and a review of the literature on therapyJ Am Acad Dermatol200757112717572277
- ZaiasNRebellGEscovarSAsymmetric gait nail unit syndrome: the most common worldwide toenail abnormality and onychomycosisSkinmed201412421722325335350
- HanekeENon infectious inflammatory disorders of the nail apparatusJ Dtsch Dermatol Ges2009778779719386022
- PaschMCNail psoriasis: a review of treatment optionsDrugs201676667570527041288
- RichPScherRKNail psoriasis severity index: a useful tool for evaluation of nail psoriasisJ Am Acad Dermatol200349220621212894066
- KlaassenKMvan de KerkhofPCBastiaensMTPlusjeLGBaranRLPaschMCScoring nail psoriasisJ Am Acad Dermatol20147061061106624698704
- AugustinMBlomeCCostanzoANail assessment in psoriasis and psoriatic arthritis (NAPPA): development and validation of a tool for assessment of nail psoriasis outcomesBr J Dermatol2014170359159824117393
- KlaassenKMDulakMGvan de KerkhofPCPaschMCThe prevalence of onychomycosis in psoriatic patients: a systematic reviewJ Eur Acad Dermatol Venereol201428553354124033871
- AlpsoyEPolatMFettahlıoğlu-KaramanBInternalized stigma in psoriasis: a multicenter studyJ Dermatol201744888589128407292
- MalakoutiMBrownGELeonAThe dermatologic intimacy scale: quantitatively measuring the impact of skin disease on intimacyJ Dermatolog Treat201728434735227764972
- PaekSYThompsonJMQureshiAAMerolaJFHusniMEComprehensive assessment of the psoriasis patient (CAPP): a report from the GRAPPA 2015 annual meetingJ Rheumatol201643596196427134270
- de JongEMSeegersBAGulinckMKBoezemanJBvan de KerkhofPCPsoriasis of the nails associated with disability in a large number of patients: results of a recent interview with 1728 patientsDermatology199619343003038993953
- van der VeldenHMKlaassenKMvan de KerkhofPCPaschMCThe impact of fingernail psoriasis on patients’ health-related and disease-specific quality of lifeDermatology20142292768225171519
- de VriesACBogaardsNAHooftLInterventions for nail psoriasisCochrane Database Syst Rev20131CD00763323440816
- HanekeEHistopathology of the Nail – OnychopathologyBoca RatonCRC Press2017
- BremJEffective topical method of therapy for onychomycosisCutis198127169766451356
- TsaiMTTsaiTYShenSCEvaluation of laser-assisted trans-nail drug delivery with optical coherence tomographySensors (Basel)20161612iiE2111
- RigopoulosDGregoriouSKatsambasATreatment of psoriatic nails with tazarotene cream 0.1% vs. clobetasol propionate 0.05% cream: a double-blind studyActa Derm Venereol200787216716817340027
- TostiAPiracciniBMCameliNCalcipotriol ointment in nail psoriasis: a controlled double-blind comparison with betamethasone dipropionate and salicylic acidBr J Dermatol199813946556599892909
- BaranRTostiATopical treatment of nail psoriasis with a new corticoid-containing nail lacquer formulationJ Dermatol Treat199910201204
- Nantel-BattistaMRicherVMarcilIBenohanianATreatment of nail psoriasis with intralesional triamcinolone acetonide using a needle-free jet injector: a prospective trialJ Cutan Med Surg2014181384224377472
- de BerkerDALawrenceCMA simplified protocol of steroid injection for psoriatic nail dystrophyBr J Dermatol1998138190959536228
- SaleemKAzimWTreatment of nail psoriasis with a modified regimen of steroid injectionsJ Coll Physicians Surg Pak2008182788118454890
- WolfRTurEBrennerSCorticosteroid-induced ‘disappearing digit’J Am Acad Dermatol1990234 pt 17557562229508
- DefferTAGoetteDKDistal phalangeal atrophy secondary to topical steroid therapyArch Dermatol19871235571572
- BjorkmanAJorgsholmPRupture of the extensor pollicis longus tendon: a study of aetiological factorsScand J Plast Reconstr Surg Hand Surg2004381323515074721
- JakubikJFinger tendon rupture following local application of triamcinolone-acetonide (Kenalog A-40)Acta Chir Plast19812331801886169243
- MascaróJMEpidermoid cyst formation after jet injection of triamcinolone for nail psoriasis29th Conf Coll Ibero Latino Am Dermatol CILADSevillaSeptember 16–19, 2012
- Sanchez RegañaMMartin EzquerraGUmbert MilletPNail psoriasis: a combined treatment with 8% clobetasol nail lacquer and tacalcitol ointmentJ Eur Acad Dermatol Venereol200822896396918410337
- TzungTYChenCYYangCYLoPYChenYHCalcipotriol used as monotherapy or combination therapy with betamethasone dipropionate in the treatment of nail psoriasisActa Derm Venereol200888327928018480933
- De SimoneCMaiorinoATassoneFD’AgostinoMCaldarolaGTacrolimus 0.1% ointment in nail psoriasis: a randomized controlled open-label studyJ Eur Acad Dermatol Venereol20132781003100622788697
- DiluvioLCampioneEPaternòEJMordentiCEl HachemMChimentiSChildhood nail psoriasis: a useful treatment with tazarotene 0.05%Pediatr Dermatol200724333233317542899
- FritzKSuccessful local treatment of nail psoriasis with 5-fluorouracil [in German]Z Hautkr19896412108310882633509
- YamamotoTKatayamaINishiokaKTopical anthralin therapy for refractory nail psoriasisJ Dermatol19982542312339609979
- LinYKChangYCHuiRCA Chinese herb, Indigo naturalis, extracted in oil (Lindioil) used topically to treat psoriatic nails: a randomized clinical trialJAMA Dermatol2015151667267425738921
- LinYKSeeLCHuangYHEfficacy and safety of Indigo naturalis extract in oil (Lindioil) in treating nail psoriasis: a randomized, observer-blind, vehicle-controlled trialPhytomedicine20142171015102024680615
- SarıcaogluHOzATuranHNail psoriasis successfully treated with intralesional methotrexate: case reportDermatology201122215721228554
- DaulatabadDGroverCSingalARole of nail bed methotrexate injections in isolated nail psoriasis: conventional drug via an unconventional routeClin Exp Dermatol Epub201741010.1111/ced.13087
- BauzáARedondoPAquerretaDPsoriatic onycho-pachydermo periostitis: treatment with methotrexateBr J Dermatol2000143490190211069487
- GümüşelMÖzdemirMMevlitoğluIBodurSEvaluation of the efficacy of methotrexate and cyclosporine therapies on psoriatic nails: a one-blind, randomized studyJ Eur Acad Dermatol Venereol20112591080108421118309
- Sanchez-ReganaMSola-OrtigosaJAlsina-GibertMVidal-FernandezMUmbert-MilletPNail psoriasis: a retrospective study on the effectiveness of systemic treatments (classical and biological therapy)J Eur Acad Dermatol Venereol201125557958621198950
- ArnoldWPGerritsenMJvan de KerkhofPCResponse of nail psoriasis to cyclosporinBr J Dermatol199312967507518286269
- MahrleGSchulzeHJFarberLWeidingerGSteiglederGKLow-dose short-term cyclosporine versus etretinate in psoriasis: improvement of skin, nail, and joint involvementJ Am Acad Dermatol199532178887822521
- SyutoTAbeMIshibuchiHIshikawaOSuccessful treatment of psoriatic nails with low-dose cyclosporine administrationEur J Dermatol2007173248249
- RabinovitzHSScherRKShupackJLResponse of psoriatic nails to the aromatic retinoid etretinateArch Dermatol19831198627628
- GajardoJExperiencia clinica con etretinato (Tigason) en 26 pacientes portadores de psoriasis. [Clinical experience with etretinate (Tigason) in 26 patients with psoriasis] [Spanish]Rev Med Chil198911755165222519162
- MurrayHEAnhaltAWLessardRA 12-month treatment of severe psoriasis with acitretin: results of a Canadian open multicenter studyJ Am Acad Dermatol19912445986021827800
- BrazzelliVMartinoliSPrestinariFBorroniGAn impressive therapeutic result of nail psoriasis to acitretinJ Eur Acad Dermatol Venereol200418222923015009317
- TostiARicottiCRomanelliPCameliNPiracciniBMEvaluation of the efficacy of acitretin therapy for nail psoriasisArch Dermatol2009145326927119289755
- BaranRTherapeutic assessment and side-effects of the aromatic retinoid on the nail apparatus (French)Ann Dermatol Venereol198210943673717125489
- VlachouCBerth-JonesJNail psoriasis improvement in a patient treated with fumaric acid estersJ Dermatolog Treat200718317517717538807
- BehrensFFinkenwirthCPavelkaKLeflunomide in psoriatic arthritis: results from a large European prospective observational studyArthritis Care Res (Hoboken)201365346447023042698
- GersterJCHohlDNail lesions in psoriatic arthritis: recovery with sulfasalazine treatmentAnn Rheum Dis2002613277
- LassusAColloidal silicic acid for the treatment of psoriatic skin lesions, arthropathy and onychopathy. A pilot studyJ Int Med Res19972542062099283994
- TorresTPuigLApremilast: a novel oral treatment for psoriasis and psoriatic arthritisAm J Clin Dermatol Epub20176810.1007/s40257-017-0302-0
- PappKReichKLeonardiCLApremilast, an oral phosphodiesterase 4 (PDE4) inhibitor, in patients with moderate to severe plaque psoriasis: results of a phase III, randomized, controlled trial (efficacy and safety trial evaluating the effects of apremilast in psoriasis [ESTEEM] 1)J Am Acad Dermatol2015731374926089047
- PaulCCatherJGooderhamMEfficacy and safety of apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate-to-severe plaque psoriasis over 52 weeks: a phase III, randomized controlled trial (ESTEEM 2)Br J Dermatol201517361387139926357944
- KushwahaASRepkaMANarasimha MurthySA novel apremilast nail lacquer formulation for the treatment of nail psoriasisAAPS PharmSciTech Epub201742810.1208/s12249-017-0776-3
- Di LerniaVBardazziFProfile of tofacitinib citrate and its potential in the treatment of moderate-to-severe chronic plaque psoriasisDrug Des Devel Ther201610533539
- PappKAMenterMAAbeMTofacitinib, an oral Janus kinase inhibitor, for the treatment of chronic plaque psoriasis: results from two, randomised, placebo-controlled, phase 3 trialsBr J Dermatol201517394996126149717
- BachelezHvan de KerkhofPCStrohalRTofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a phase 3 randomised non-inferiority trialLancet2015386999355256126051365
- MerolaJFElewskiBTatulychSLanSTallmanAKaurMEfficacy of tofacitinib for the treatment of nail psoriasis: two 52-week, randomized, controlled phase 3 studies in patients with moderate-to-severe plaque psoriasisJ Am Acad Dermatol201777179.e87.e28396102
- LangleyRGSauratJHReichKon behalf of the Nail Psoriasis Delphi Expert PanelRecommendations for the treatment of nail psoriasis in patients with moderate to severe psoriasis: a dermatology expert group consensusJ Eur Acad Dermatol Venereol201226337338122151734
- BardazziFLambertiniMChessaMAMagnanoMPatriziAPiracciniBMNail involvement as a negative prognostic facor in biological therapy for psoriasis: a retrospective studyJ Eur Acad Dermatol Venereol20173184384627658350
- GniadeckiRKragballeKDamTNSkovLComparison of drug survival rates for adalimumab, etanercept and infliximab in patients with psoriasis vulgarisBr J Dermatol201116451091109621219290
- GniadeckiRBangBBryldLEIversenLLastheinSSkovLComparison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgarisBr J Dermatol2015172124425225132294
- ArnoldTSchaarschmidtMLHerrRFischerJEGoerdtSPeitschWKDrug survival rates and reasons for drug discontinuation in psoriasisJ Dtsch Dermatol Ges201614111089109927879076
- CallenJPComplications and adverse reactions in the use of newer biologic agentsSemin Cutan Med Surg200726161417349557
- Al-MutairiNNourTAl-RqobahDOnychomycosis in patients of nail psoriasis on biologic therapy: a randomized, prospective open label study comparing etanercept, infliximab and adalimumabExpert Opin Biol Ther201313562562923527597
- FabroniCGoriATroianoMPrignanoFLottiTInfliximab efficacy in nail psoriasis. A retrospective study in 48 patientsJ Eur Acad Dermatol Venereol201125554955320707829
- IrlaNYawalkarNMarked improvement in nail psoriasis during treatment with adalimumabDermatology2009219435335619851059
- KaranikolasGNKoukliEMKatsaliraAAdalimumab or cyclosporine as monotherapy and in combination in severe psoriatic arthritis: results from a prospective 12-month nonrandomized unblinded clinical trialJ Rheumatol201138112466247421885499
- ReichKOrtonneJPGottliebABSuccessful treatment of moderate to severe plaque psoriasis with the PEGylated Fab0 certolizumab pegol: results of a phase II randomized, lacebo-controlled trial with a re-treatment extensionBr J Dermatol201216718019022413944
- MeasePJFleischmannRDeodharAAEffect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis: 24-week results of a Phase 3 double-blind randomised placebo-controlled study (RAPID-PsA)Ann Rheum Dis2014731485523942868
- RallisEStavropoulouERigopoulosDVerrosCRapid response of nail psoriasis to etanerceptJ Rheumatol200835354454518322982
- OrtonneJPPaulCBerardescaEA 24-week randomized clinical trial investigating the efficacy and safety of two doses of etanercept in nail psoriasisBr J Dermatol201316851080108723013207
- WeisshaarEDiepgenTLSuccessful etanercept therapy in therapy-refractory acrodermatitis continua suppurativa HallopeauJ Dtsch Dermatol Ges20075648949217537042
- KavanaughAMcInnesIMeasePGolimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a sub-cutaneous injection in psoriatic arthritis: twenty-four-week efficacy and safety results of a randomized, placebo-controlled studyArthritis Rheum200960497698619333944
- KavanaughAvan der HeijdeDMcInnesIBGolimumab in psoriatic arthritis: one-year clinical efficacy, radiographic, and safety results from a phase III, randomized, placebo-controlled trialArthritis Rheum20126482504251722378566
- SfikakisPPIliopoulosAElezoglouAKittasCStratigosAPsoriasis induced by antitumor necrosis factor therapy: a paradoxical adverse reactionArthritis Rheum2005522513251816052599
- WollinaUHanselGKochASchönlebeJKöstlerEHaroskeGTumor necrosis factor-α inhibitor-induced psoriasis or psoriasiform exanthemata. First 120 cases from the literature including a series of 6 new casesAm J Clin Dermatol2008911418092839
- PinkAEFoniASmithCHBarkerJNWNThe development of sarcoidosis on antitumour necrosis factor therapy: a paradoxBr J Dermatol201016364166620491760
- PirardDArcoDDebrouckereVHeenemMAnti-tumor necrosis factor alpha-induced psoriasiform eruptions: three further cases and current overview. Dermatology current overviewDermatology200621318218617033165
- ConradCLapointeAKGillietMParadoxic psoriasis induced by anti-TNF treatment – a report of 8 cases and evidence for a new pathogenic mechanism93rd Ann Meet Swiss Soc Dermatol VenereolGeneva2011 FC 11Dermatol Helv2011630
- HanekeENail psoriasisSoungJKooBPsoriasisRijekaIntech2011141186
- MenterAThe status of biologic therapies in the treatment of moderate to severe psoriasisCutis200984suppl 4142419916298
- Wcisło-DziadeckaDZbiciakMBrzezińska-WcisłoMMazurekUAnti-cytokine therapy for psoriasis – not only TNF-α blockers. Overview of reports on the effectiveness of therapy with IL-12/IL-23 and T and B lymphocyte inhibitorsPostepy Hig Med Dosw (online)2016701198120528026823
- PuigLThe role of IL 23 in the treatment of psoriasisExpert Rev Clin Immunol201713652553428165883
- ReichKSullivanJArenbergerPSecukinumab is effective in subjects with moderate to severe plaque psoriasis with significant nail involvement: 16 week results from the TRANSFIGURE studyPresented at: 23rd World Congress of DermatologyVancouver, CanadaJune 8–15, 2015
- PaulCReichKGottliebABCAIN457A2211 Study GroupSecukinumab improves hand, foot and nail lesions in moderate-to-severe plaque psoriasis: subanalysis of a randomized, double-blind, placebo-controlled, regimen-finding phase 2 trialJ Eur Acad Dermatol Venereol201428121670167524393602
- LeonardiCMathesonRZachariaeCAnti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasisN Engl J Med2012366131190119922455413
- LangleyRGRichPMenterAImprovement of scalp and nail lesions with ixekizumab in a phase 2 trial in patients with chronic plaque psoriasisJ Eur Acad Dermatol Venereol20152991763177025693783
- PuigLBrodalumab: the first anti-IL-17 receptor agent for psoriasisDrugs Today (Barc)201753528329728650001
- RallisEKintzoglouSVerrosCUstekinumab for rapid treatment of nail psoriasisArch Dermatol2010146111315131621079083
- VitielloMTostiAAbucharAZaiacMKerdelFAUstekinumab for the treatment of nail psoriasis in heavily treated psoriatic patientsInt J Dermatol201352335836223330782
- RichPBourcierMSofenHPHOENIX 1 InvestigatorsUstekinumab improves nail disease in patients with moderate-to-severe psoriasis: results from PHOENIX 1Br J Dermatol2014170239840724117389
- GordonKBLangleyRGGottliebABA phase III, randomized, controlled trial of the fully human IL-12/23 mAb briakinumab in moderate-to-severe psoriasisJ Invest Dermatol2012132230431422011907
- BlauveltAPappKAGriffithsCEEfficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trialJ Am Acad Dermatol201776340541728057360
- ReichKPappKABlauveltATildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): results from two randomised controlled, phase 3 trialsLancet20173901009127628828596043
- KruegerJGFerrisLKMenterAAnti-IL-23A mAb BI 655066 for treatment of moderate-to-severe psoriasis: safety, efficacy, pharmacokinetics, and biomarker results of a single-rising-dose, randomized, double-blind, placebo-controlled trialJ Allergy Clin Immunol20151361116.e124.e25769911
- LindelofBRadiotherapy is rarely used in daily clinical care of patients suffering from nail psoriasisActa Derm Venereol198969180822563616
- FinnertyEFSuccessful treatment of psoriasis of the nailsCutis19792314344759120
- YuRCKingCMA double-blind study of superficial radiotherapy in psoriatic nail dystrophyActa Derm Venereol19927221341361350400
- KwangTYNeeTSSengKTA therapeutic study of nail psoriasis using electron beamsActa Derm Venereol1995751907747554
- SternDKCreaseyAAQuijijeJLebwohlMGUV-A and UV- B penetration of normal human cadaveric fingernail plateArch Dermatol2011147443944121173303
- MarxJLScherRKResponse of psoriatic nails to oral photochemotherapyArch Dermatol19801169102310247416754
- MacDonaldKJHargreavesGKEadRDLongitudinal melanonychia during photochemotherapyBr J Dermatol19861143395396
- TawfikAANovel treatment of nail psoriasis using the intense pulsed light: a one-year follow-up studyDermatol Surg201440776376825111349
- OramYKarincaogluYKoyuncuEKaharamanFPulsed dye laser in the treatment of nail psoriasisDermatol Surg201036337738120100261
- Fernández-GuarinoMHartoASánchez-RoncoMGarcía-MoralesIJaénPPulsed dye laser vs. photodynamic therapy in the treatment of refractory nail psoriasis: a comparative pilot studyJ Eur Acad Dermatol Venereol200923889189519470064
- TreewittayapoomCSingvahanontPChanprapaphKHanekeEThe effect of different pulse durations in the treatment of nail psoriasis with 595-nm pulsed dye laser: a randomized, double- blind, intrapatient left-to-right studyJ Am Acad Dermatol201266580781222243768
- GoldustMRaghifarRClinical trial study in the treatment of nail psoriasis with pulsed dye laserJ Cosmet Laser Ther Epub20131016
- HuangYCChouCLChiangYYEfficacy of pulsed dye laser plus topical tazarotene versus topical tazarotene alone in psoriatic nail disease: a single-blind, intrapatient left-to-right controlled studyLasers Surg Med201345210210723423871
- Al-MutairiNNoorTAl-HaddadASingle blinded left-to-right comparison study of excimer laser versus pulsed dye laser for the treatment of nail psoriasisDermatol Ther (Heidelb)20144219720524990703
- Arango-DuqueLCRoncero-RiescoMUsero BárcenaTPalacios ÁlvarezIFernández LópezETreatment of nail psoriasis with pulse dye laser plus calcipotriol betametasona gel vs. Nd:YAG plus calcipotriol betamethasone gel: an intrapatient left-to-right controlled studyActas Dermosifiliogr2017108214014428118926