
Abstract
Psoriasis and the spectrum of inflammatory bowel diseases (IBD) are chronic, inflammatory, organotropic conditions. The epidemiologic coexistence of these diseases is corroborated by findings at the level of disease, biogeography, and intrafamilial and intrapatient coincidence. The identification of shared susceptibility loci and DNA polymorphisms has confirmed this correlation at a genetic level. The pathogenesis of both diseases implicates the innate and adaptive segments of the immune system. Increased permeability of the epidermal barrier in skin and intestine underlies the augmented interaction of allergens and pathogens with inflammatory receptors of immune cells. The immune response between psoriasis and IBD is similar and comprises phagocytic, dendritic, and natural killer cell, along with a milieu of cytokines and antimicrobial peptides that stimulate T-cells. The interplay between dendritic cells and Th17 cells appears to be the core dysregulated immune pathway in all these conditions. The distinct similarities in the pathogenesis are also reflected in the wide overlapping of their therapeutic approaches. Small-molecule pharmacologic immunomodulators have been applied, and more recently, biologic treatments that target proinflammatory interleukins have been introduced or are currently being evaluated. However, the fact that some treatments are quite selective for either skin or gut conditions also highlights their crucial pathophysiologic differences. In the present review, a comprehensive comparison of risk factors, pathogenesis links, and therapeutic strategies for psoriasis and IBD is presented. Specific emphasis is placed on the role of the immune cell species and inflammatory mediators participating in the pathogenesis of these diseases.
Introduction
Psoriasis and the group of inflammatory bowel diseases (IBD) are chronic, inflammatory, organotropic conditions. The former affects the skin of 2%–3% of the population, with hyperproliferation of keratinocytes, impaired epidermal barrier function at the sites of skin lesions, and skin infiltration by activated inflammatory cells.Citation1 Ulcerative colitis (UC) and Crohn’s disease (CD) are the two most prevalent representatives of the IBD group. UC usually affects the rectum and may extend to the colon, with restriction of the inflammatory process to the mucosa and submucosa layers, while CD can affect any site of the digestive tract, with segmentary distribution of the lesions and inflammatory infiltration of all intestinal wall layers.Citation2
Immune dysregulation, determined by genetic predisposition and environmental assaults, underlies all three conditions. A coincidence of psoriasis and IBD has been observed in various clinical settings: they can appear as concomitant disease events in the same patient or as “paradoxical” treatment-related adverse events.Citation3,Citation4
Moreover, a wide spectrum of therapeutic modalities is used to treat psoriasis and IBD, a fact that further underscores pathophysiological disease similarities. There are also cases of distinct discrepancies in the effectiveness of certain modalities that highlight differences in the pathophysiology between skin and gastrointestinal (GI) diseases and even within the IBD themselves.
The objectives of this paper were to review the most relevant literature data on the role of microbiota, inflammatory cell species, and humoral inflammation mediators in psoriasis and IBD immunopathogenesis and treatment response. For this purpose, corresponding core review articles were compiled, and a focused literature search was performed for retrieving the updated information. The search was conducted periodically during progressing text editing, employing Medline (PubMed). Two search filters were applied (language “English” and field “Title/abstract”), and the identified material was explored for selecting papers with adequate content. The full text of selected articles was retrieved, each study was individually evaluated, and the resulting material was integrated in this descriptive report.
After a short comparison of the genetic collation, we will survey the role of microbiota and selected innate and adaptive immunity inflammatory cell species and humoral inflammation mediators in the pathogenesis of these diseases. Finally, we discuss similarities and discrepancies in the response of psoriasis and IBD patients to the established pharmacologic therapies of either to additionally highlight the nosologic relationships of these conditions.
Diseases coincidence
Psoriasis and IBD cluster at all genetic levels of human populations, ie, they share the same geographic/ethnic, kindred, and patient niches. These diseases are more frequent in Northern Europe and North America (psoriasis prevalence: ~2%; UC and CD incidences: 19.2–24.3 and 12.7–20.2 per 100,000 person-years, respectively) compared to most regions of Africa, Asia, and the Middle East (psoriasis prevalence: <0.5%; UC and CD incidences: 6.3 and 5.0 per 100,000 person-years, respectively).Citation5–Citation7
Both psoriasis and CD present with much higher incidence among family members of patients than in the general population.Citation8,Citation9 Almost one-third of patients with psoriasis also have a first-degree relative affected with the disease.Citation9 In contrast, the risk of the siblings of a CD patient to be affected is only ~5%.Citation8 Moreover, differences in concordance rates between monozygotic and dizygotic twins both in psoriasis (70% vs 23%, respectively) and CD (37% vs 7%) support the important role of genetic background.Citation10,Citation11
Psoriasis and CD also coexist in the same patient more often than expected by chance: the prevalence of psoriasis in patients with CD is 9.6% (vs 2.2% in controls).Citation12 The relative risks of psoriasis are significantly increased in both UC (1.56-fold) and CD (1.52-fold) patients and psoriasis patients are at increased risk to develop IBD (2.49-fold for CD and 1.64-fold for UC).Citation13,Citation14
Genetic collation
A shared genetic susceptibility background probably underlies the pathobiological and clinical overlap of psoriasis and IBD. To date, the literature describes 13 psoriasis susceptibility loci (designated PSORS1-13), and genome-wide association studies implicate 32 loci in the pathogenesis of CD and 17 in UC ().Citation15–Citation17
Table 1 Genetic susceptibility loci associated with psoriasis and IBD
The epidemiologic coincidence of the conditions is partly explained by the sharing of disease susceptibility loci: 20q13 corresponds to PSORS12 and IBD24, 19p13 to PSORS6 and IBD6, 6p21 to PSORS1 and IBD3, and 5q31 to PSORS11 and IBD5.Citation17 However, despite loci concordance, the involved genes are often different. For example, in the 6p21 region, psoriasis seems to be linked to the HLA-Cw*0602 allele, while IBD are mainly linked to polymorphisms in the TNF-α gene promoter.Citation17
Of note, a recent meta-analysis of genome-wide association studies that included >4,500 patients and 10,000 controls recognized seven susceptibility loci outside the human leukocyte antigen region (9p24 near JAK2, 10q22 at ZMIZ1, 11q13 near PRDX5, 16p13 near SOCS1, 17q21 at STAT3, 19p13 near FUT2, and 22q11 at YDJC) shared by psoriasis and CD and confirmed four already established common psoriasis and CD risk loci (IL23R, IL12B, REL, and TYK2).Citation18 Future functional studies that explore these genetic relationships will contribute to better understanding of the resonance of genetic colocalization to the pathophysiology of the diseases.
Microbiota
Microbiota play a significant role in the pathogenesis of different diseases.Citation19 Skin and intestine are the two major niches of prokaryotic and eukaryotic symbiotic microorganism flora in humans.Citation20,Citation21 The inflammatory diseases evaluated herein primarily affect the structure and function of the corresponding organism–environment interface linings, resulting in distinct sustained alterations in the respective microenvironments of exposed tissue surfaces and, simultaneously, also of the species composition of the microorganism populations (dysbiosis).
Commensal microbes produce numerous biologically active metabolites that impact the physiology and immune response of the underlying epithelia. Notably, members of the phylum Firmicutes, the number of which are decreased in the gut lumen of CD patients, produce short-chain fatty acid metabolites (acetate, butyrate) with anti-inflammatory actions in the normal gut that may fail in IBD patients.Citation22–Citation24 Aryl hydrocarbon receptor (AhR), the promiscuous receptor that mediates the recognition of xenobiotics and modifies immune responses, may play a distinct role in mediating these pathophysiologic alterations. AhR-deficient mice, a mutant known to develop enhanced Th17-driven inflammatory immune responses, are characterized by a high prevalence of segmented filamentous bacteria in their gut. Interestingly, the administration of antibiotics that target these bacteria results in the reduction of intestinal IL-17 production as well.Citation24
Microbiota act both as triggers and inhibitors of inflammation; to date, the balance of these effects have been better studied in IBD compared to psoriasis patients.Citation19 IBD patients are characterized by a decrease of anaerobic bacteria (Bacteroides, Eubacterium, Lactobacillus).Citation25 Particularly, CD patients present with a reduction in Firmicutes and Clostridium leptum populations, along with a simultaneous increase in Proteobacteria.Citation26,Citation27 These alterations have been linked to genetic determinants of the immune response (as the NOD2 gene) or genes that are associated with intracellular degradation of proteins, such as ATG16L1.Citation28 Like-wise, Paneth cell function and the FUT2 genotype (a gene involved in the expression of ABO blood group antigens in the GI mucosa) have been linked to substantial differences in the species composition of the microbial populations that colonize the gut lumen and modify the risk of developing CD.Citation29,Citation30 Interestingly, similarly to patients with a microbial infection, IBD are characterized by a substantial loss of microorganism species diversity in the gut and by a shift from an innocuous multispecies homeostatic flora to a narrower spectrum of proinflammatory and pathogenic microbial species.Citation31,Citation32 The impact of antibiotic use in this shift is a matter of debate, yet certain antibacterial agents (such as the 5-aminosalicylic acid) suppress the ability of gut bacteria to build adherent biofilms in patients with IBD, resulting in disease improvement.Citation33
Genes affecting epidermal barrier function and adaptive immune responses with subsequent alterations in bacterial colonization have been suspected to contribute to the pathogenesis of psoriasis.Citation34 The interrelationship between microbes and psoriasis pathogenesis is currently under intense investigation. Many studies agree that a certain degree of dysbiosis is a landmark of the skin lesions and that psoriasis may, at least in part, be associated with a substantial alteration in the composition of the cutaneous microflora.Citation35 The genus most frequently identified in diseased skin areas is Corynebacterium as opposed to Propionibacterium in healthy controls. In addition, the representation of Propionibacterium and Actinobacteria species is lower and that of Firmicutes is higher in affected skin.Citation36,Citation37 Infections also play a central role in the course of psoriasis. Bacteria have been suspected to be an important source of antigens that trigger the immune system activation, which is a characteristic of this condition.Citation38 Guttate psoriasis flares are usually preceded by streptococcal pharyngitis episodes. Moreover, the distinct differences in the prevalence of psoriasis in different populations have been attributed to the effect of natural selection for gene polymorphisms associated with more vigorous immunity against infectious agents such as invasive streptococci infections or leprosy pandemics in the past.Citation39,Citation40 T-cell clones primed by streptococcal tonsillitis or pharyngitis are supposed to be reactivated in the skin as a result of their exposure to cross-reactive epitopes expressed there (molecular mimicry).Citation41
Microbes seem to further interact with the cells of the innate immune system, resulting in increased expression of antimicrobial peptides, production of cytokines, and subsequently, stimulation of T-cells.Citation42,Citation43 As in the gut of IBD patients, the absence of AhR enhances skin inflammation both in the skin of patients with psoriasis and in a murine model of psoriasiform skin inflammation.Citation44 Notably, the potent AhR agonist indirubin, also produced on the surface of the skin by Malassezia yeasts, is an ingredient used in topical remedies for psoriasis in traditional Chinese medicine.Citation45,Citation46
In conclusion, alterations of the microbial flora in the gut and the skin may not only result from disease-associated tissue perturbations but may also exacerbate and maintain the disease state in a vicious self-perpetuating cycle.
The role of innate immune cells and the IL-23/Th17 axis
Innate and adaptive immune processes are expected to participate in the pathogenesis of both psoriasis and IBD (, ). Until recently, the prevailing opinion in the literature favored adaptive immunity as the major player in the pathogenesis of these diseases; however, current evidence highlights a more decisive role of the innate immunological mechanisms.
Figure 1 The epithelial barrier in both diseases appears more permeable than normal.
Abbreviation: IBDs, inflammatory bowel diseases.
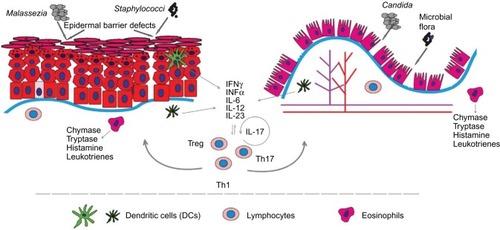
Table 2 Summary of the role of innate and adaptive immunity cell species in the pathophysiology of psoriasis and inflammatory bowel diseases (IBD)
The innate immune system includes the host’s primary response mechanisms against foreign agents: protective physical barriers, inflammation-related proteins like the complement system and C-reactive protein, antimicrobial peptides, such as defensins and cathelicidins, and pattern recognition receptors (PRRs), cytokines, phagocytic cells, dendritic cells (DCs), and natural killer (NK) cells.Citation22,Citation43
The intestinal epithelial barrier is a physical defense line that encompasses intestinal epithelial cells, tight junctions, and a layer of mucous. The resident microbiota can activate specific PRRs in the epithelial cells,Citation47 effecting downstream signaling that leads to proinflammatory protein synthesis and in the case of IBD to a more susceptible and permeable epithelial barrier.Citation48,Citation49 The anatomical and functional integrity of the barrier is further compromised by proinflammatory cytokines (such as TNF-α), which disturb the integrity of intercellular tight junctions by affecting the synthesis of occludins and other related proteins in the gut epithelium.Citation50 In addition, mucous production is either up- or downregulated in IBD patients, further contributing to disease processes.Citation51
Compared to healthy individuals, intestinal epithelial cells of IBD patients express an altered pattern of Toll-like receptors (TLRs): increased TLR4 expression in UC patients and decreased TLR4 and TLR3 expression in CD patients.Citation52 An overexpression of TLR4 and TLR2 in intestinal wall macrophages during inflammation also contributes to a state of gut hyperresponsiveness to xenobiotics in these patients.Citation53 Based on the aforementioned observations, in IBD patients, the defective epithelial barrier function facilitates intestinal antigens to reach and bind to PRRs, activate the immune system, and ultimately herald inflammation.
Likewise, defects in the structure and function of the epidermal barrier seem to play an important role in the pathogenesis of psoriasis. Similar to the aforementioned IBD findings, the expression of structural proteins such as claudin and zonula occludens-1 is reduced in the epidermis of psoriatic lesions, which results in alterations in the structure of epidermal tight junctions.Citation54 The overall pathophysiologic consequence is a partially compromised epidermal barrier capacity that enables enhanced invasion of microorganisms, their products, and other foreign molecules, ultimately leading to the stimulation of inflammatory skin processes.Citation55
On the other hand, the expression of TLRs is also modified in psoriasis.Citation56 TLR 2 is constitutively expressed in the suprabasal layers of normal skin, but it is limited to the basal cell layers of the epidermis in diseased skin. There is also a characteristic tissue shift in epidermal TLR 4 expression, with an inversion of the spatial expression gradient from a basal to superficial pattern in the normal skin to a more pronounced expression in more superficial layers in psoriasis lesions. These shifts are associated with the disturbed skin barrier, and are interpreted as an adaptation of the tissue to meet the need for enhanced immune surveillance and avoidance of overstimulation due to pathophysiological inflammation cascades in diseased skin.Citation56
Dendritic cells (DCs) are the main regulators of immunity since they are able to provoke inflammatory responses or impose immune tolerance.Citation22 They are equipped with a wide range of PRRs, including TLRs and Nod-like receptors (NLRs), allowing them to distinguish between microbiota and pathogens. So far DCs have not been stimulated by immunological insults their state corresponds to an “immature” phenotype that maintains the T-lymphocytes inactive.
In the intestine, submucosal DCs reach the intestinal lumen by projecting their dendrites through the tight junctions boundaries between epithelial cells.Citation57 In IBD, gut inflammation and the defective mucous membrane barrier allow an increased amount of intestinal lumen antigens to reach the DCs, resulting in their maturation and activation, thus enhancing immune responses.Citation58 The population of mucosal DCs and the number of CD40+ DCs is significantly increased in UC and CD, when compared to controls.Citation59 Among intestinal DCs, the CD103+ cell subpopulation seems to be essential for maintaining the homeostasis of the mucosa and for regulation of the balance between effector and regulatory T-lymphocytes.Citation60 During an IBD disease flare, DC subsets expressing E-cadherin (a CD103 receptor) in the intestine and the draining mesenteric lymph nodes and provide pro-inflammatory cytokines, such as IL-6 and IL-23, which are suggested to contribute toward Th17 cell maturation and colon damage in at least a subset of IBD patients.Citation61,Citation62
Also in psoriasis the cellular composition of cutaneous DC subsets is modified compared to healthy skin: Langerhans cells (LCs) are markedly reduced, whereas plasmacytoid DCs (pDCs) are increased in human psoriasis lesions and in the animal skin of a murine psoriasis model (DKO* mice).Citation63 Particularly, the depletion of LCs in the latter model aggravated the disease, while depletion of pDCs (before disease onset) resulted in an overall milder phenotype. The proposed mechanisms included IL-10 and IL-23 decrease. The modulating role of LCs in psoriasis is further highlighted by the fact that after treatment with adalimumab, the density of epidermal LCs increases rapidly (with a concomitant normalization of their spatial localization within the epidermis).Citation64
pDCs predominate among the immune cells of the dermis of lesions and uninvolved skin of psoriasis patients.Citation65 In healthy skin, pDCs are almost absent, but they are abundant in the skin of psoriatic plaques, particularly in early lesions, where they become activated and produce interferon-α (INF-α), an inflammatory mediator essential for the development of psoriasis lesions.Citation65 A less distinct role for pDCs is presumed for the chronic-stationary state of psoriasis lesions;Citation66 other dermal DC subsets appear to be more important for the stabilization of disease state and the persistence of these lesions.Citation67
Macrophages participate in innate and adaptive immune processes at the epithelium, acting as an environmental barrier through phagocytosis and antigen presentation.Citation68 Two major subtypes of macrophages and further cellular subsets are distinguished: inflammatory (M1) and anti-inflammatory (M2a, M2b, M2c), reflecting the vast cellular diversity and functional plasticity of this cell species in the skin and intestine.Citation69
In healthy individuals, the main intestinal population of macrophages bears the CX3CR1high phenotype and, although, nonresponsive to inflammatory stimuli, these cells preserve phagocytic capacity. Under the proinflammatory circumstances of the gut tissues in IBD, another subpopulation of CX3CR1low/int macrophages expands there due to the emigration and differentiation of precursor monocytes.Citation70 This M1 macrophage subset that overexpresses antigen receptors and PRRs augments the environmental signaling for the synthesis of proinflammatory cytokines (TNF, IL-1, IL-6) and contributes to local immune response exacerbations.Citation71
The M1 macrophages subset is also closely linked to the proinflammatory situation of the psoriatic plaques.Citation72 A variety of exogenous pathogen-associated molecular patterns and endogenous ligands, recognized through PRRs, are implicated in the molecular pathways by which macrophage activation is induced after the skin barrier is breached.Citation73 Thepen et alCitation74 showed that local elimination of macrophages led to resolution of focuses of cutaneous inflammation. A number of endogenous anti-inflammatory mediators produced by macrophages have also been identified, including IL-10, TGF-β, lipoxins, and prostaglandins.Citation75 In addition, tissue macrophages have been involved in the generation of T-regulatory cells.Citation76 Taken together, macrophage subsets in psoriatic skin may delineate both pro- and anti-inflammatory roles in the pathogenesis of psoriasis. Given the central role of macrophages in maintaining tissue inflammation, better understanding of their pathophysiological role is predicted to contribute innovative macrophage-targeting therapeutic modalities for psoriasis and IBD in the future.
Mast cells (MCs) are another cell species with a recognizable role in the pathogenesis of IBD and psoriasis. There are two subsets of MCs, mucosal and connective tissue MCs. The human mucosal MCs are a functionally T-cell-dependent population mainly found in the lungs and the intestine. Connective tissue MCs are not as much T-cell dependent and are found in the skin and the intestinal submucosa.Citation77
The largest number of MC progenitors are found in the intestine. These cells continue to differentiate, mature, and establish residence there.Citation78 Increased number of MCs are found in biopsies from UC- or CD-affected gut areas.Citation79,Citation80 Under conditions of tissue inflammation, intestinal MCs degranulate and release substances such as tryptase-β and chymase-1Citation81 leading to increased tissue levels of histamine, prostaglandin D2, and leukotrienes.Citation82 In the intestine, MCs also play an important homeostatic role by regulating the baseline permeability of the gut epitheliumCitation83 and by modulating epithelial–neuromuscular interactions in the gut. Thus, they participate in the pathogenesis of altered motility patterns seen in functional GI disorders, postoperative ileus, food allergy, and also IBD.Citation84
In the human skin, connective tissue MCs play an essential role in diverse physiological and pathological processes such as the mediation of type I hypersensitivity reactions and allergic diseases. Upon activation, they produce large amounts of TNF-α, IFN-γ, IL-8, IL-33, and multiple other mediators, such as VEGF, contributing to the creation of a tissue microenvironment essential for the recruitment of neutrophils and lymphocytes during innate and T-cell-mediated inflammatory processes.Citation85 The increased number of MC that are found in psoriasis skin, underscore the important role of these cells in the pathophysiology of this disease.Citation85,Citation86
In particular, a postulated interaction between stress and inflammatory processes in both the skin and the intestine is suggested to be mediated via the function of MCs.Citation87,Citation88 MC–neuronal interactions are thought to be involved in translating stress insults into psoriasis flares.Citation89
The natural killer (NK) cells are a specialized subset of CD56+CD16+ cells that can recognize injured cells and promote their death through a non-MHC-dependent manner.Citation90 They also produce cytokines, particularly IFN-γ, TNF-α, and TGF-β but also IL-2, IL-15, and IL-23, and affect the maturation of DCs.Citation91
In IBD, NK cells are characterized by increased IL-21R expression, which amplifies the effect of IL-21 and the downstream proinflammatory cytokine cascade.Citation92 In the intestinal mucosa of CD patients, there are alterations in the ratio of NKp44- and NKp46-expressing NK cells.Citation93 Increased numbers of IFN-γ-producing NKp46+ cells are found in CD-affected mucosa sections, whereas IL-22-producing NKp44+ cells are significantly decreased compared to UC patients and healthy controls.
In the acute state of psoriatic plaques, ~5%–8% of the inflammatory cellular infiltrate consists of NK cells expressing the CD56+CD3− phenotype and the activation antigen CD69. Compared to the uninvolved skin of psoriasis patients or healthy controls, NK cells in the lesional psoriasis skin produce large quantities of IFN-γ and express higher levels of perforin, a pore-forming protein found in the cytotoxic granules of NK cells and a key mediator of NK cells cytotoxicity.Citation94,Citation95
Finally, decreased number of circulating NK cells is found in patients with long-standing psoriasis. Decreased NK cell activity was also observed in the peripheral blood of IBD patients, but this could not be attributed to decreased NK cell number.Citation96
Another leukocyte species involved in IBD pathogenesis is the innate lymphoid cell (ILCs).Citation22 ILCs are abundant at barrier surfaces of the body such as the skin and the intestine.Citation97 These cells play a key role in tissue remodeling and controlling microbe tissue load, lymphoid tissue development, and tissue homeostasis.Citation98,Citation99 ILCs are divided into subtypes based on the patterns of synthesized cytokines and on the expression of specific transcription factors.Citation99,Citation100
Besides their important role in gut homeostasis, these cells are probably also involved in the pathogenesis of IBD, where increased numbers are found compared to controls.Citation101 In a proinflammatory environment, these cells produce IL-22; a pathophysiologic adaptation that limits apoptosis, preserves intestinal barrier, and protects the gut during inflammation.Citation101–Citation103
Blood and lesional skin biopsies of patients with psoriasis showed enrichment of NCR+ ILC3; however, similar frequencies of CD161+ ILC1 and CRTH2+ ILC2 compared to controls.Citation104 ILC3 is an innate source of IL-22 and IL-17 in the psoriatic skin, and an increased skin concentration of NKp44+ ILC3 cells has been associated with disease severity.Citation105 It is worth noting that treatment of psoriasis patients with adalimumab reversed the number of these cells in parallel with clinical disease improvement.Citation106
Regarding the role of the adaptive immunity, the latest pathophysiologic hypotheses consider an interaction of Th17, T-regulatory lymphocytes (Tregs), and Th1 cells crucial for the pathogenesis of both psoriasis and IBD.Citation107
Th17 cells comprise a subpopulation of T-helper cells that produce mainly IL-17 and IL-21.Citation108 They comprise a T-lymphocyte subset evolutionarily distinct from the Th1 and Th2 lymphocyte subpopulations, with a key role in chronic organotropic inflammatory processes such as psoriasis and CD.Citation109 Some Th17 subtypes also produce IL-22, which is associated with disease aggravations in psoriasis; however, it has a protective function in IBD. Inflammatory foci of the GI mucosa in IBD patients display a massive infiltration of Th17 cells, and Th17-related cytokines are produced in excess in both CD- and UC-affected tissues.Citation110 Genome-wide association studies have revealed increased frequencies of certain Th17-related gene polymorphisms (such as STAT3 or IL-23R) in IBD patients, thus supporting the involvement of the Th17 pathway in IBD pathogenesis.Citation111 Despite earlier findings, to date, targeting Th17 cells,Citation112 either by blocking their proliferation and differentiation or by inhibiting and neutralizing their specific cytokines, is a highly disputed, rather ineffective therapeutic pathway for IBD (see “Comparison of pharmacologic treatment modalities” section).
Recent advances in understanding the psoriasis pathogenesis indicate to an interaction of the IL-23/Th17 cells axis with keratinocytes and synovial cells as one of the main pathophysiologic events in the initiation and maintenance of tissue inflammation in this disease.Citation113 IL-17-producing Th17 lymphocytes promote the synthesis of inflammatory molecules and induce acanthosis, hyperkeratosis, and parakeratosis.Citation114,Citation115 As in the case of IBD, polymorphisms of genes have been observed in psoriasis that relate to development and functional polarization of Th17 lymphocytes. For example, polymorphisms in the aforementioned genes STAT3 and IL23 are strongly associated with the psoriasis phenotype.Citation116 The key role of IL-17 in psoriasis is further underlined by the distinct effectiveness of treatment modalities (contrary to IBD) that either target the IL-17 cytokine directly (secukinumab, bimekizumab, ixelkizumab) or block the IL-17 receptor (IL-17R: brodalumab).Citation113
Another lymphocyte subpopulation with increasing importance in IBD and psoriasis research is the Tregs. In various organs, including intestine and skin, these cells counteract the abnormal activation of the immune system, preventing excessive stimulation and contributing to self-tolerance.Citation117
Compared to controls, Tregs are reduced in peripheral blood in the active phase of both CD and UC; however, they normalize during disease remissions. This observation suggests that during the course of IBD, Tregs migrate from peripheral blood to the inflamed intestinal mucosal sites, the lamina propria, and mesenteric lymph nodes.Citation118,Citation119 It is worth noting that at the level of the intestine, the tissue concentration of Tregs is higher in IBD irrespective of the activity state of the disease, when compared to healthy controls.Citation120,Citation121
Tregs were significantly increased in the dermis and epidermis of psoriatic skin too, as compared to normal skin.Citation122 Functional and numerical abnormalities of Tregs have also been documented in the peripheral blood of psoriasis and IBD patients.Citation123 However, although Foxp3 polymorphisms appear to contribute to the risk of developing psoriasis (at least in certain patient subpopulations), a similar association could not be verified in IBD patients.Citation124,Citation125
Comorbidities
Chronic inflammatory conditions such as psoriasis and IBD also share a series of important comorbidities. Most of these connections have been attributed to the systemic action of sustainably increased tissue levels of inflammatory mediators, shared genetic risk factors, and, in some cases, predictable adverse effects of the employed treatments.Citation126 Patients with severe psoriasis are at increased risk of premature death from most leading mortality causes in the population, including cardiovascular (CV) disease, malignancies, chronic lower respiratory disease, diabetes, dementia, infection, and kidney disease.Citation127 Moreover, in psoriasis, besides the characteristic arthropathy and the concordance with IBD, variable evidence for a higher prevalence has been observed for CV disease, obesity, diabetes, hypertension, dyslipidemia, metabolic syndrome, nonalcoholic fatty liver disease, cancer, and anxiety/depression.Citation128 On the other hand, apart from psoriasis, usual comorbidities of IBD include arthritis, asthma, pericarditis, certain malignancies, and also psychiatric conditions. Notably, among IBD, patients with UC (but not with CD) are additionally at increased risk of developing chronic renal failure and multiple sclerosis.Citation129 It is worth noting that overall mortality rates are also slightly increased in IBD patients at a rate comparable to that observed in the case of severe psoriasis.Citation130 compares the evidence for selected major comorbidities in patients with psoriasis and IBD. Corresponding data concerning three selected major comorbidities (cancer, obesity, and CV diseases) will be briefly discussed.
Table 3 Psoriasis and IBD share a series of important comorbidities.
Besides epidemiologic evidence, the rationale for the search for possible connections of psoriasis and IBD, on one hand, and malignancies, on the other, is the bidirectional relationship between chronic inflammation and cancer. Chronic inflammatory conditions are frequently associated with the induction CD8+ cytotoxic T-lymphocytes and increased NK cell activities. Moreover, INF-γ and TNF-α produced by the activated CD4+ Th1 cells in inflammatory conditions may cause tumor cell senescence and tumor control. In addition, Th1 immunity may induce antiangiogenic chemokines that in certain circumstances could counteract cancer growth.Citation131 On the contrary, other studies indicate that inflammation contributes directly to tumorigenesis.Citation132 Chronic inflammation can initiate tumors directly by causing DNA alterations or by making cells more susceptible to mutagens. In addition, inflammation can also act as a tumor promoter since inflammatory mediators such as cytokines (TNF-α, IL-1, IL-6), growth factors, chemokines, and proteases produced by tumor-associated lymphocytes, and macrophages can enhance tumor cell growth and metastasis.Citation133,Citation134 However, taking available data together, there is no evidence of increased cancer incidence among patients with psoriasis and IBD, with the exception of the association of UC with certain GI malignancies. Probably these opposing mechanisms generally balance themselves in the case of the present chronic inflammatory conditions, resulting in overall unaffected cancer risks. Nonmelanoma skin cancer represents an exception among malignancies for both conditions; however, their increased incidence is most likely secondary to the application of therapeutic modalities with recognized tumor-promoting risks (ie, ultraviolet radiation and azathioprine in psoriasis and IBD, respectively).Citation135
From a pathophysiologic point of view, obesity is an interesting comorbidity that potentially highlights the shared pathogenesis mechanisms of psoriasis and IBD. Obesity is currently considered a chronic, low-grade inflammatory condition;Citation136 proinflammatory adipose tissue macrophages stimulate the secretion of proinflammatory mediators, such as TNF-α, IL-6, and leptin, which establish and maintain an inflammatory tissue state.Citation137 With a doubled odds ratio compared to controls, obesity is a recognized serious health risk factor in patients with psoriasis.Citation138 In addition a role for obesity in the pathogenesis of psoriasis is speculated.Citation139 More specific, significantly increased blood levels of leptin are found in patients with psoriasis, a mediator that might have participated to psoriasis induction by promoting Type 1 cytokines synthesis.Citation140 On the other hand, due to the nature of IBD (with abdominal pain and diarrhea, weight loss, and some degree of malnutrition affecting the majority of the patients), obesity was not predicted to be an important comorbidity of IBD patients.Citation141 However, it is surprising that a recent study finds an increasing prevalence of obesity in patients with IBD (15%–20%), with a further 40% of patients being overweight.Citation142 Chronic inflammation, the type of intestinal microbiota, the medication for controlling IBD, and the lack of physical activity are all discussed as putative factors that favor overweight and obesity in the IBD patients.Citation143–Citation145 Future studies should also clarify to what extent the improved efficacy of IBD treatment modalities might per se have contributed to increased obesity prevalence among these patients.
Finally, there is currently increasing interest in the literature concerning the interrelationship between psoriasis and CV morbidity, with particular emphasis in the role of the antipsoriatic therapeutic interventions. Most studies indicate an increased CV risk of patients with psoriasis that is mediated by endothelial dysfunction and is manifested by higher incidences of stroke, atherosclerosis, coronary artery disease, and myocardial infarction.Citation146 Interestingly, psoriasis and atherosclerosis share a common pattern of Th1 and Th17 cytokine upregulation, T-cell activation, local and systemic expression of adhesion molecules, and endothelins.Citation147 Moreover, increased amounts of vascular endothelial growth factor produced by proliferating keratinocytes and the hyperhomocysteinemia (a common finding in patients with psoriasis) provide additional possible mechanisms for increased atherosclerosis risk in these patients.Citation148,Citation149 On the other hand, CV is still a common cause of mortality among IBD patients although they have no different CV risk compared to the general population.Citation150–Citation152 And this is in spite of the increased prevalence of a series of risk factors in patients with IBD, known to promote CV risk (prothrombotic state, subclinical atherosclerosis).Citation153–Citation156 This controversy is still increasing when the role of therapeutic interventions is considered. Besides reports of decreased frequency and severity of CV events both in psoriasis and IBD patients under treatment with methotrexate and probably also TNF-α inhibitors, other studies found exactly the opposite, ie, increased myocardial infarction risks, with the same modalities.Citation157–Citation159
Taken together, probably with the exception of psychiatric comorbidities and increased nonmelanoma skin cancer risk, there is no conclusive evidence definitively linking both psoriasis and IBD with a certain pattern of comorbid conditions.
Comparison of pharmacologic treatment modalities
The wide overlap of approved modalities employed to treat psoriasis and IBD, particularly the more targeted newer biologics, underscore the pathophysiologic proximity of the mechanisms that underlie the pathogenesis of these conditions. However, distinct differences also exist that obviate core differences in the pathophysiology of these conditions, and the knowledge of these differences is significant for the understanding of core pathomechanistic peculiarities of each condition. depicts and compares the use of currently approved pharmacologic modalities for the systematic treatment of psoriasis and IBD.
Table 4 Comparison of the use of pharmacological treatment modalities for psoriasis and inflammatory bowel diseases (IBD)
Although a number of different small molecules are used to treat both psoriasis and IBD, we focus on the comparison of the effectiveness of the mechanistically more predictable targeted biologic modalities.
Generally, TNF-α-targeting biologics are effective in both psoriasis and IBD with a vast differentiation: etanercept, which is approved for the treatment of psoriasis, is not effective in IBD.Citation160,Citation161 Paradoxically, treatment with anti-TNF-α modalities has been implicated in de novo development of psoriasis and, less frequently, of IBD.Citation162–Citation165 The incidence of anti-TNF-α-associated psoriasis-like manifestations has been estimated at one case per 1,000 patient-years or 3%–10% of the treated patients.Citation107,Citation166,Citation167
More recently, monoclonal antibodies against IL-17 (sekukinumab, brodalimumab, ixekizumab) have been developed for the treatment of moderate-to-severe psoriasis, exhibiting exceptional efficacy.Citation168 Secukinumab and brodalimumab have also been evaluated in randomized trials for moderate-to-severe CD, but neither reached significant effectiveness compared to placebo.Citation169 The conflicting results provided by IL-17 inhibition verify the complex biology of this immune mechanism in CD as well as indicate the crucial differences with the role of Th-17 cells in the pathogenesis of psoriasis and IBD.Citation170,Citation171
Discussion
The concurrent existence of psoriasis and IBD in an increasing number of patients poses a new diagnostic and therapeutic challenge. Health professionals should be aware of the similarities and discrepancies in the pathogenesis and epidemiology of these diseases to successfully distinguish between their random coexistence, their causative concurrence, or their occurrence as a “paradoxical” side effect. IBD patients should be examined for skin lesions, as extraintestinal manifestations markedly increase the overall morbidity of these diseases.Citation172–Citation174
In this report, we also compared the role of immune cells in the pathophysiology of psoriasis and IBD. The anatomical and functional integrity of the tissue–environmental barriers is compromised in the skin and intestinal lumen of patients with psoriasis and IBD, respectively, allowing the invasion of allergens and immunomodulatory metabolites from an altered microflora. An increased number of DCs infiltrate the skin in psoriasis and the intestine in IBD. These cells are exposed there to a proinflammatory milieu that mainly favors a Th1 response. Through the interaction of M1 subset of macrophages with tissue MCs in both conditions, increased amounts of substances are released in the tissue environment that promotes the recruitment of neutrophils and lymphocytes. Recently, interest has focused on the role of IL-23/Th17 effector axis, as its interaction with keratinocytes and intestinal mucosa cells appears to be a central pathway for the pathogenesis of psoriasis and IBD and a promising target for treatment modalities.
The aforementioned immune similarities also form the basis for the wide overlap of treatment regimens that are used to treat psoriasis and IBD. However, there are also remarkable differences in the effectiveness of certain agents that highlight discrepancies in the pathophysiology of these conditions. Etanercept, for example, was not effective in IBD, and this has been attributed to a diminished ability of etanercept to induce T-cell apoptosis in the intestinal mucosa.Citation175 Correspondingly, the ineffectiveness of secukinumab in the treatment of CD has been related to the importance of mycobiome in the pathogenesis of this disease.Citation176 Given the high concordance of psoriasis and CD, it is legitimate to take into consideration the significant risk of CD flare inductions in patients receiving secukinumab, particularly as first-line treatment, for moderate-to-severe psoriasis.
It is similarly worth noting that the use of anti-TNF-α bio-logics to treat IBD, especially CD, has probably increased the prevalence of noninfectious dermatoses in these patients.Citation177 Next to xerosis and atopic eczema exacerbations, psoriasis is the third most common skin manifestation provoked by the treatment with anti-TNF-α agents in these patients.Citation177 The vast majority of the cases (76%) developed psoriasis while on infliximab, and the rest (24%) after switching to adalimumab or certolizumab, indicating that this phenomenon is not drug specific, but rather a pharmacological group effect.Citation107 Cases of psoriasis induced by etanercept have been also reported.Citation178 Regarding the management of paradoxical psoriasis, no specific guidelines are currently available. It has been hypothesized that individuals with newly developed psoriasis under treatment, whose cutaneous disease persists or recurs despite removal of the suspected agents, probably have an underlying previously unrecognized predisposition to psoriasis. However, those whose skin findings resolve completely after treatment modification are more likely to have suffered a true drug-induced psoriasis episode against the background of low genetic psoriasis preponderance.Citation179
Conclusion
Available data support a high degree of overlapping epidemiologic profiles, genetic substrate, disease risk factors, inflammatory pathogenesis cascades, and also therapeutic procedures between psoriasis and IBD, particularly CD. Further studies may unravel the common mechanism that underlies these common chronic inflammatory diseases of skin and gut and may provide valuable insights for the development of innovative interventions for both conditions.
Disclosure
The authors report no conflicts of interest in this work.
References
- NestleFOKaplanDHBarkerJPsoriasisN Engl J Med2009361549650919641206
- BaumgartDCSandbornWJInflammatory bowel disease: clinical aspects and established and evolving therapiesLancet20073691641165717499606
- LolliESaracenoRCalabreseEPsoriasis phenotype in inflammatory bowel disease: a case-control prospective studyJ Crohns Colitis20159969970725908719
- ZippiMCorradoCPicaRExtraintestinal manifestations in a large series of Italian inflammatory bowel disease patientsWorld J Gastroenterol20142046174631746725516659
- MolodeckyNASoonISRabiDMIncreasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic reviewGastroenterology2012142465422001864
- LoftusEVJrClinical epidemiology of inflammatory bowel disease: incidence, prevalence, and environmental influencesGastroenterology200412661504151715168363
- ParisiRSymmonsDPGriffithsCEGlobal epidemiology of psoriasis: a systematic review of incidence and prevalenceJ Invest Dermatol2013133237738523014338
- YangHPlevySETaylorKLinkage of Crohn’s disease to the major histocompatibility complex region is detected by multiple non-parametric analysesGut199944451952610075959
- OestreicherJWaltersIKikuchiTMolecular classification of psoriasis disease-associated genes through pharmacogenomic expression profilingPharmacogenomics J20011427228711911124
- FarberEMNallMLWatsonWNatural history of psoriasis in 61 twin pairsArch Dermatol197410922072114814926
- WattsDASatsangiJThe genetic jigsaw of inflammatory bowel diseaseGut200250Suppl 3III31III3611953330
- LeeFIBellarySVFrancisCIncreased occurrence of psoriasis in patients with Crohn’s disease and their relativesAm J Gastroenterol19908589629632375323
- BernsteinCNWajdaABlanchardJFThe clustering of other chronic inflammatory diseases in inflammatory bowel disease: a population-based studyGastroenterology2005129382783616143122
- CohenADDreiherJBirkenfeldSPsoriasis associated with ulcerative colitis and Crohn’s diseaseJ Eur Acad Dermatol Venereol200923556156519207663
- ChandraARayASenapatiSChatterjeeRGenetic and epigenetic basis of psoriasis pathogenesisMol Immunol201564231332325594889
- ImielinskiMBaldassanoRNGriffithsACommon variants at five new loci associated with early-onset inflammatory bowel diseaseNat Genet200941121335134019915574
- SkrozaNProiettiIPampenaRCorrelations between psoriasis and inflammatory bowel diseasesBiomed Res Int2013201398390223971052
- EllinghausDEllinghausENairRPCombined analysis of genome-wide association studies for Crohn disease and psoriasis identifies seven shared susceptibility lociAm J Hum Genet201290463664722482804
- DzutsevAGoldszmidRSViaudSZitvogelLTrinchieriGThe role of the microbiota in inflammation, carcinogenesis, and cancer therapyEur J Immunol2015451173125328099
- SekirovIRussellLAntunesCFinlayBGut microbiota in health and diseasePhysiol Rev201090385990420664075
- CaponeKADowdSEStamatasGNNikolovskiJDiversity of the human skin microbiome early in lifeJ Invest Dermatol2011131102026203221697884
- BassoPJFonsecaMTBonfaGAssociation among genetic predisposition, gut microbiota, and host immune response in the etiopathogenesis of inflammatory bowel diseaseBraz J Med Biol Res201447972773725075576
- FurusawaYObataYFukudaSCommensal microbe-derived butyrate induces the differentiation of colonic regulatory T cellsNature201350444645024226770
- QiuJGuoXChenZMGroup 3 innate lymphoid cells inhibit T-cell-mediated intestinal inflammation through aryl hydrocarbon receptor signaling and regulation of microfloraImmunity20133938639923954130
- OttSJMusfeldtMTimmisKNHampeJWenderothDFSchreiberSIn vitro alterations of intestinal bacterial microbiota in fecal samples during storageDiagn Microbiol Infect Dis200450423724515582296
- WalkerAWSandersonJDChurcherCHigh-throughput clone library analysis of the mucosa-associated microbiota reveals dysbiosis and differences between inflamed and non-inflamed regions of the intestine in inflammatory bowel diseaseBMC Microbiol201111721219646
- WillingBHalfvarsonJDicksvedJTwin studies reveal specific imbalances in the mucosa-associated microbiota of patients with ileal Crohn’s diseaseInflamm Bowel Dis20091565366019023901
- FrankDNRobertsonCEHammCMDisease phenotype and genotype are associated with shifts in intestinal-associated microbiota in inflammatory bowel diseasesInflamm Bowel Dis20111717918420839241
- WehkampJSalzmanNHPorterEReduced Paneth cell α-defensins in ileal Crohn’s diseaseProc Natl Acad Sci U S A2005102181291813416330776
- RauschPRehmanAKünzelSColonic mucosa-associated microbiota is influenced by an interaction of Crohn disease and FUT2 (Secretor) genotypeProc Natl Acad Sci U S A201110847190301903522068912
- TamboliCPNeutCDesreumauxPColompelJFDysbiosis as a prerequisite for IBDGut20045371057
- RookGARaisonCLLowryCAHaleLPLochsHMicrobiota, immunoregulatory old friends and psychiatric disordersAdv Exp Med Biol201481731935624997041
- SwidsinskiAWeberJLoening-BauckeVHaleLPLochsHSpatial organization and composition of the mucosal florain patients with inflammatory bowel diseaseJ Clin Microbiol20054373380338916000463
- OkaAMabuchiTOzawaAInokoHCurrent understanding of human genetics and genetic analysis of psoriasisJ Dermatol201239323124122352847
- GalloRLNakatsujiTMicrobial symbiosis with the innate immune defense system of the skinJ Invest Dermatol2011131101974198021697881
- GaoZTsengCHStroberBEPeiZBlaserMJSubstantial alterations of the cutaneous bacterial biota in psoriatic lesionsPLoS One200837e271918648509
- AlekseyenkoAVPerez-PerezGIDe SouzaACommunity differentiation of the cutaneous microbiota in psoriasisMicrobiome2013113124451201
- FryLBakerBSPowlesAVFahlenAEngstrandLIs chronic plaque psoriasis triggered by microbiota in the skin?Br J Dermatol20131691475223521130
- BassukasIDGaitanisGHundeikerMLeprosy and the natural selection for psoriasisMed Hypotheses201278118319022079652
- McFaddenJPBakerBSPowlesAVFryLPsoriasis and streptococci: the natural selection of psoriasis revisitedBr J Dermatol2009160592993719309365
- MakRKHundhausenCNestleFOProgress in understanding the immunopathogenesis of psoriasisActas Dermosifiliogr2009100Suppl 221320096156
- MorizaneSGalloRLAntimicrobial peptides in the pathogenesis of psoriasisJ Dermatol201239322
- SweeneyCMTobinAMKirbyBInnate immunity in the pathogenesis of psoriasisArch Dermatol Res20113031069170521863252
- Di MeglioPDuarteJHAhlforsHActivation of the aryl hydrocarbon receptor dampens the severity of inflammatory skin conditionsImmunity2014406989100124909886
- MagiatisPPappasPGaitanisGMalassezia yeasts produce a collection of exceptionally potent activators of the Ah (dioxin) receptor detected in diseased human skinJ Invest Dermatol201313382023203023448877
- LinYKLeuYLYangSHChenHWWangCTPangJHAnti-psoriatic effects of indigo naturalis on the proliferation and differentiation of keratinocytes within dirubin as the active componentJ Dermatol Sci200954316817419303259
- SalzmanNHMicrobiota-immune system interaction: an uneasy allianceCurr Opin Microbiol20111419910520971034
- GerovaVAStoynovSGKatsarovDSSvinarovDAIncreased intestinal permeability in inflammatory bowel diseases assessed by iohexol testWorld J Gastroenterol201117172211221521633531
- KiesslichRDuckworthCAMoussataDLocal barrier dysfunction identified by confocal laser endomicroscopy predicts relapse in inflammatory bowel diseaseGut20126181146115322115910
- MankertzJTavalaliSSchmitzHExpression from the human occludin promoter is affected by tumor necrosis factor α and interferon gammaJ Cell Sci2000113Pt 112085209010806119
- BuisineMPDesreumauxPLeteurtreEMucin gene expression in intestinal epithelial cells in Crohn’s diseaseGut200149454455111559653
- CarioEPodolskyDKDifferential alteration in intestinal epithelial cell expression of toll-like receptor 3 (TLR3) and TLR4 in inflammatory bowel diseaseInfect Immun200068127010701711083826
- HausmannMKiesslingSMestermannSToll-like receptors 2 and 4 are up-regulated during intestinal inflammationGastroenterology200212271987200012055604
- ViscontiBPaolinoGCarottiSImmunohistochemical expression of VDR is associated with reduced integrity of tight junction complex in psoriatic skinJ Eur Acad Dermatol Venereol201529102038204225220655
- RobersonEDBowcockAMPsoriasis genetics: breaking the barrierTrends Genet201026941542320692714
- PanzerRBlobelCFölster-HolstRProkschETLR2 and TLR4 expression in atopic dermatitis, contact dermatitis and psoriasisExp Dermatol201423536436624661005
- NiessJHBrandSGuXCX3CR1-mediated dendritic cell access to the intestinal lumen and bacterial clearanceScience200530725425815653504
- VarolCZigmondEJungSSecuring the immune tightrope: mononuclear phagocytes in the intestinal lamina propriaNat Rev Immunol201010641542620498668
- BaumgartDCThomasSPrzesdzingIExaggerated inflammatory response of primary human myeloid dendritic cells to lipopolysaccharide in patients with inflammatory bowel diseaseClin Exp Immunol2009157342343619664152
- AnnackerOCoombesJLMalmstromVEssential role for CD103 in the T cell-mediated regulation of experimental colitisJ Exp Med200520281051106116216886
- SiddiquiKRLaffontSPowrieFE-cadherin marks a subset of inflammatory dendritic cells that promote T cell-mediated colitisImmunity201032455756720399121
- LealMCDäbritzJImmunoregulatory role of myeloid-derived cells in inflammatory bowel diseaseInflamm Bowel Dis201521122936294726244650
- GlitznerEKorosecABrunnerPMSpecific roles for dendritic cell subsets during initiation and progression of psoriasisEMBO Mol Med20146101312132725216727
- GordonKBBonishBKPatelTLeonardiCLNickoloffBJThe tumour necrosis factor-α inhibitor adalimumab rapidly reverses the decrease in epidermal Langerhans cell density in psoriatic plaquesBr J Dermatol2005153594595316225604
- NestleFOConradCTun-KyiAPlasmacytoid predendritic cells initiate psoriasis through interferon-α productionJ Exp Med2005202113514315998792
- AlbanesiCScarponiCPallottaSChemerin expression marks early psoriatic skin lesions and correlates with plasmacytoid dendritic cell recruitmentJ Exp Med2009206124925819114666
- CerioRGriffithsCECooperKDNickoloffBJHeadingtonJTCharacterization of factor XIIIa positive dermal dendritic cells in normal and inflamed skinBr J Dermatol198912144214312576222
- WillenborgSEmingSAMacrophages – sensors and effectors coordinating skin damage and repairJ Dtsch Dermatol Ges201412321422324580874
- MantovaniAAllavenaPSicaATumour-associated macrophages as a prototypic type II polarised phagocyte population: role in tumour progressionEur J Cancer200440111660166715251154
- BainCCScottCLUronen-HanssonHResident and pro-inflammatory macrophages in the colon represent alternative context-dependent fates of the same Ly6Chi monocyte precursorsMucosal Immunol2013649851022990622
- SchenkMBouchonASeiboldFMuellerCTREM-1 – expressing intestinal macrophages crucially amplify chronic inflammation in experimental colitis and inflammatory bowel diseasesJ Clin Invest2007117103097310617853946
- NickoloffBJBonishBKMarbleDJLessons learned from psoriatic plaques concerning mechanisms of tissue repair, remodeling, and inflammationJ Investig Dermatol Symp Proc20061111629
- KarinMLawrenceTNizetVInnate immunity gone awry: linking microbial infections to chronic inflammation and cancerCell200612482383516497591
- ThepenTvan VuurenAJKiekensRCDamenCAVooijsWCvan De WinkelJGResolution of cutaneous inflammation after local elimination of macrophagesNat Biotechnol2000181485110625390
- GilroyDWNewsonJSawmynadenPWilloughbyDACroxtallJDA novel role for phospholipase A2 isoforms in the checkpoint control of acute inflammationFASEB J200418348949815003994
- LinHHFaunceDEStaceyMThe macrophage F4/80 receptor is required for the induction of antigen-specific efferent regulatory T cells in peripheral toleranceJ Exp Med2005201101615162515883173
- KritasSKSagginiAVarvaraGImpact of mast cells on the skinInt J Immunopathol Pharmacol201326485585924355220
- HamiltonMJFreiSMStevensRLThe multifaceted mast cell in inflammatory bowel diseaseInflamm Bowel Dis201420122364237825401721
- NishidaYMuraseKIsomotoHDifferent distribution of mast cells and macrophages in colonic mucosa of patients with collagenous colitis and inflammatory bowel diseaseHepatogastroenterology20024967868212063968
- NolteHSpjeldnaesNKruseAWindelborgBHistamine release from gut mast cells from patients with inflammatory bowel diseasesGut19903177917941695160
- BischoffSCWedemeyerJHerrmannAQuantitative assessment of intestinal eosinophils and mast cells in inflammatory bowel diseaseHistopathology19962811138838115
- FoxCCLazenbyAJMooreWCYardleyJHBaylessTMLichtensteinLMEnhancement of human intestinal mast cell mediator release in active ulcerative colitisGastroenterology1990991191241693122
- GroschwitzKRAhrensROsterfeldHMast cells regulate homeostatic intestinal epithelial migration and barrier function by a chymase/Mcpt4-dependent mechanismProc Natl Acad Sci U S A200910652223812238620018751
- WoutersMMVicarioMSantosJThe role of mast cells in functional GI disordersGut201665115516826194403
- HarvimaITNilssonGSuttleMMNaukkarinenAIs there a role for mast cells in psoriasis?Arch Dermatol Res2008300946147818719932
- CoxAJMast cells in psoriasisCoxAJFarberEMPsoriasis, Proceedings of the Second International Symposium, Stanford UniversityNew York, NYYorke Medical Books19773643
- ArckPCSlominskiATheoharidesTCPetersEMPausRNeuroimmunology of stress: skin takes center stageJ Invest Dermatol200612681697170416845409
- RijnierseANijkampFPKraneveldADMast cells and nerves tickle in the tummy: implications for inflammatory bowel disease and irritable bowel syndromePharmacol Ther2007116220723517719089
- TheoharidesTCThe mast cell: a neuroimmunoendocrine master playerInt J Tissue React19961811218880375
- DunphySGardinerCMNK cells and psoriasisJ Biomed Biotechnol2011201124831721687543
- YadavPKChenCLiuZPotential role of NK cells in the pathogenesis of inflammatory bowel diseaseJ Biomed Biotechnol2011201134853021687547
- LiuZYangLCuiYIL-21 enhances NK cell activation and cytolytic activity and induces Th17 cell differentiation in inflammatory bowel diseaseInflamm Bowel Dis20091581133114419322899
- TakayamaTKamadaNChinenHImbalance of NKp44(+) NKp46(−) and NKp44(NKp46+) natural killer cells in the intestinal mucosa of patients with Crohn’s diseaseGastroenterology20101393882892892.e1320638936
- OttavianiCNasorriFBediniCde PitàOGirolomoniGCavaniACD56 bright CD16(−) NK cells accumulate in psoriatic skin in response to CXCL10 and CCL5 and exacerbate skin inflammationEur J Immunol200636111812816323244
- YawalkarNSchmidSBraathenLRPichlerWJPerforin and granzyme B may contribute to skin inflammation in atopic dermatitis and psoriasisBr J Dermatol200114461133113911422032
- GiacomelliRPassacantandoAFrieriGCirculating soluble factor-inhibiting natural killer (NK) activity of fresh peripheral blood mononuclear cells (PBMC) from inflammatory bowel disease (IBD) patientsClin Exp Immunol1999115172779933422
- SonnenbergGFMjösbergJSpitsHArtisDSnapShot: innate lymphoid cellsImmunity2013393622622.e124012419
- CupedoTCrellinNKPapazianNHuman fetal lymphoid tissue-inducer cells are interleukin 17-producing precursors to RORC+ CD127+ natural killer-like cellsNat Immunol2009101667419029905
- BuonocoreSAhernPPUhligHHInnate lymphoid cells drive interleukin-23-dependent innate intestinal pathologyNature201046472931371137520393462
- LeeJSCellaMMcDonaldKGAHR drives the development of gut ILC22 cells and postnatal lymphoid tissues via pathways dependent on and independent of NotchNat Immunol201213144151
- LongmanRSDiehlGEVictorioDACX3CR1+ mononuclear phagocytes support colitis-associated innate lymphoid cell production of IL-22J Exp Med201421181571158325024136
- HanashAMDudakovJAHuaGInterleukin-22 protects intestinal stem cells from immune-mediated tissue damage and regulates sensitivity to graft versus host diseaseImmunity201224339350
- ZenewiczLAYancopoulosGDValenzuelaDMMurphyAJStevensSFlavellRAInnate and adaptive interleukin-22 protects mice from inflammatory bowel diseaseImmunity200819947957
- VillanovaFFlutterBTosiICharacterization of innate lymphoid cells in human skin and blood demonstrates increase of NKp44+ ILC3 in psoriasisJ Invest Dermatol2014134498499124352038
- TeunissenMBMunnekeJMBerninkJHComposition of innate lymphoid cell subsets in the human skin: enrichment of NCR(+) ILC3 in lesional skin and blood of psoriasis patientsJ Invest Dermatol201413492351236024658504
- SalimiMOggGInnate lymphoid cells and the skinBMC Dermatol2014141825427661
- FiorinoGOmodeiPDPsoriasis and inflammatory bowel disease: two sides of the same coin?J Crohns Colitis20159969769826079725
- OuyangWKollsJKZhengYThe biological functions of T helper 17 cell effector cytokines in inflammationImmunity200828445446718400188
- SteinmanLA brief history of TH17, the first major revision in the TH1/TH2 hypothesis of T cell-mediated tissue damageNat Med200713213914517290272
- ZenewiczLAAntovAFlavellRACD4 T-cell differentiation and inflammatory bowel diseaseTrends Mol Med200915519920719362058
- ThompsonILeesCWGenetics of ulcerative colitisInflamm Bowel Dis201117383184821319274
- GalvezJRole of Th17 cells in the pathogenesis of human IBDISRN Inflamm201425928461
- MarinoniBCeribelliAMassarottiMSelmiCThe Th17 axis in psoriatic disease: pathogenetic and therapeutic implicationsAuto Immun Highlights20145191926000152
- FitchEHarperESkorchevaIKurtzSEBlauveltAPathophysiology of psoriasis: recent advances on IL-23 and TH17 cytokinesCurr Rheumatol Rep20079646146718177599
- AsarchABarakOLooDSGottliebABTh17 cells: a new paradigm for cutaneous inflammationJ Dermatolog Treat200819525926618629676
- HardenJLKruegerJGBowcockAMThe immunogenetics of psoriasis: a comprehensive reviewJ Autoimmun201564667326215033
- SakaguchiSWingKMiyaraMRegulatory T cells – a brief history and perspectiveEur J Immunol200737Suppl 1S116S12317972355
- SarutaMYuQTFleshnerPRCharacterization of FOXP3+CD4+ regulatory T cells in Crohn’s diseaseClin Immunol2007125328129017897887
- YuQTSarutaMAvanesyanAFleshnerPRBanhamAHPapadakisKAExpression and functional characterization of FOXP3+CD4+ regulatory T cells in ulcerative colitisInflamm Bowel Dis200713219119917206665
- MaulJLoddenkemperCMundtPPeripheral and intestinal regulatory CD4+ CD25(high) T cells in inflammatory bowel diseaseGastroenterology200512871868187815940622
- WangYLiuXPZhaoZBExpression of CD4+ forkhead box P3 (FOXP3)+ regulatory T cells in inflammatory bowel diseaseJ Dig Dis201112428629421791023
- HiraharaKLiuLClarkRAYamanakaKFuhlbriggeRCKupperTSThe majority of human peripheral blood CD4+CD25highFoxp3+ regulatory T cells bear functional skin-homing receptorsJ Immunol200617774488449416982885
- BovenschenHJvan Vlijmen-WillemsIMvan de KerkhofPCvan ErpPEIdentification of lesional CD4+ CD25+ Foxp3+ regulatory T cells in PsoriasisDermatology2006213211111716902287
- GaoLLiKLiFPolymorphisms in the FOXP3 gene in Han Chinese psoriasis patientsJ Dermatol Sci2010571515619880293
- ParkOGrishinaILeungPSGershwinMEPrindivilleTAnalysis of the Foxp3/scurfin gene in Crohn’s diseaseAnn N Y Acad Sci2005105121822816126962
- BinusAMHanJQamarAAModyEAHoltEWQureshiAAAssociated comorbidities in psoriasis and inflammatory bowel diseaseJ Eur Acad Dermatol Venereol201226564465021689167
- AbuabaraKAzfarRSShinDBNeimannALTroxelABGelfandJMCause-specific mortality in patients with severe psoriasis: a population-based cohort study in the UKBr J Dermatol201016358659220633008
- OnumahNKircikLHPsoriasis and its comorbiditiesJ Drugs Dermatol2012115 SupplS5S10
- CasellaGTontiniGEBassottiGNeurological disorders and inflammatory bowel diseasesWorld J Gastroenterol201420278764878225083051
- CardTHubbardRLoganRFMortality in inflammatory bowel disease: a population-based cohort studyGastroenterology200312561583159014724808
- Müller-HermelinkNBraumüllerHPichlerBTNFR1 signaling and IFN-gamma signaling determine whether T cells induce tumor dormancy or promote multistage carcinogenesisCancer Cell200813650751818538734
- MantovaniAAllavenaPSicaABalkwillFCancer-related inflammationNature200845443644418650914
- ZumstegAChristoforiGCorrupt policemen: inflammatory cells promote tumor angiogenesisCurr Opin Oncol200921607019125020
- ZamarronBFChenWDual roles of immune cells and their factors in cancer development and progressionInt J Biol Sci2011765165821647333
- BassukasIDGaitanisGTsianosEAzathioprine: an explanation for the risk of skin SCC among patients with Crohn’s disease?Ann Rheum Dis200968 eLetter June 15, 2009; Available from: http://ard.bmj.com/content/68/12/1863.full/reply#annrheumdis_el_5801Accessed May 3, 2016
- MonteiroRAzevedoIChronic inflammation in obesity and the metabolic syndromeMediators Inflamm2010201028964520706689
- HammingaEAvan der LelyAJNeumannHAThioHBChronic inflammation in psoriasis and obesity: implications for therapyMed Hypotheses200667476877316781085
- ArmstrongAWHarskampCTArmstrongEJThe association between psoriasis and obesity: a systematic review and meta-analysis of observational studiesNutr Diabetes20122e5423208415
- MattioliBStrafaceEQuarantaMGGiordaniLVioraMLeptin promotes differentiation and survival of human dendritic cells and licenses them for Th1 primingJ Immunol2005174116820682815905523
- WangYChenJZhaoYGengLSongFChenHDPsoriasis is associated with increased levels of serum leptinBr J Dermatol200815851134113518294316
- LomerMCCookWBJan-MohamedHJIron requirements based upon iron absorption tests are poorly predicted by haematological indices in patients with inactive inflammatory bowel diseaseBr J Nutr20121071218061122152498
- SteedHWalshSReynoldsNA brief report of the epidemiology of obesity in the inflammatory bowel disease population of Tayside, ScotlandObes Facts20092637037220090388
- AndradeMMaioRDouradoKFMacêdoPFBarreto NetoACExcessive weight muscle – depletion paradox and cardiovascular risk factors in outpatients with inflammatory bowel diseaseArg Gastroenterol20155213745
- BertinBDesreumauxPDubuquoyLObesity, visceral fat and Crohn’s diseaseCurr Opin Clin Nutr Metab Care201013557458020625283
- Chapman-KiddellCADaviesPSGillenLRadford-SmithGLRole of diet in the development of inflammatory bowel diseaseInflamm Bowel Dis201016113715119462428
- MehtaNNYuYPinnelasRAttributable risk estimate of severe psoriasis on major cardiovascular eventsAm J Med20111248775.e1e621787906
- BaltaIBaltaSDemirkolSAortic arterial stiffness is a moderate predictor of cardiovascular disease in patients with psoriasis vulgarisAngiology2014651747823636854
- NofalAAl-MakhzangyIAttwaENassarAAbdalmoatiAVascular endothelial growth factor in psoriasis: an indicator of disease severity and controlJ Eur Acad Dermatol Venereol200923780380619309427
- McDonaldIConnollyMTobinAMA review of psoriasis, a known risk factor for cardiovascular disease and its impact on folate and homocysteine metabolismJ Nutr Metab2012201296538522690330
- DornSDSandlerRSInflammatory bowel disease is not a risk factor for cardiovascular disease mortality: results from a systematic review and meta-analysisAm J Gastroenterol2007102366266717156143
- GraefVBaggenstossAHSauerWGSpittellJAJrVenous thrombosis occurring in nonspecific ulcerative colitis. A necropsy studyArch Intern Med1966117377382
- RuisiPMakaryusJNRuisiMMakaryusANInflammatory bowel disease as a risk factor for premature coronary artery diseaseJ Clin Med Res20157425726125699123
- GisondiPCotenaCTessariGGirolomoniGAnti-tumour necrosis factor-α therapy increases body weight in patients with chronic plaque psoriasis: a retrospective cohort studyJ Eur Acad Dermatol Venereol200822334134418005022
- RhoYHChungCPOeserAInflammatory mediators and premature coronary atherosclerosis in rheumatoid arthritisArthritis Rheum200961111580158519877084
- DagliNPoyrazogluOKDagliAFIs inflammatory bowel disease a risk factor for early atherosclerosis?Angiology20106119820419398421
- MitchellGFArterial stiffness and wave reflection: biomarkers of cardiovascular riskArtery Res20093566420161241
- MichaRImamuraFWyler von BallmoosMSystematic review and meta-analysis of methotrexate use and risk of cardiovascular diseaseAm J Cardiol201110891362137021855836
- FameniniSSakoEYWuJJEffect of treating psoriasis on cardiovascular co-morbidities: focus on TNF inhibitorsAm J Clin Dermatol2014151455024281789
- AbuabaraKLeeHKimballABThe effect of systemic psoriasis therapies on the incidence of myocardial infarction: a cohort studyBr J Dermatol20111651066107321777216
- SaracenoRSagginiAPietroleonardoLChimentiSInfliximab in the treatment of plaque type psoriasisClin Cosmet Investig Dermatol200922737
- AkobengAKZachosMTumor necrosis factor-α antibody for induction of remission in Crohn’s diseaseCochrane Database Syst Rev20041CD00357414974022
- FiorinoGAllezMMalesciADaneseSReview article: anti TNF-α induced psoriasis in patients with inflammatory bowel diseaseAliment Pharmacol Ther200929992192719210297
- MocciaroFRennaSOrlandoACottoneMSevere cutaneous psoriasis after certolizumab pegol treatment: report of a caseAm J Gastroenterol20091042867286819888257
- HarrisMDRichardsRFirst case report of adalimumab-induced psoriasis in Crohn’s diseaseAm J Gastroenterol200910479279319262532
- VereaMMDel PozoJYebra-PimentelMTPortaAFonsecaEPsoriasiform eruption induced by infliximabAnn Pharmacother200438545714742794
- TichyMHercogovaJManifestation of Crohn’s disease in a young woman during the course of treatment for severe form of chronic plaque psoriasis with etanerceptDermatol Ther201427421121424548537
- HarrisonMJDixonWGWatsonKDRates of new-onset psoriasis in patients with rheumatoid arthritis receiving anti-TNF-α therapy: results from the British Society for Rheumatology Biologics RegisterAnn Rheum Dis20096820921518385277
- YiuZZGriffithsCEInterleukin 17-A inhibition in the treatment of psoriasisExpert Rev Clin Immunol20161211426561053
- TarganSFeaganBVermeireSMo2083 a randomized, double-blind, placebo-controlled study to evaluate the safety, tolerability, and efficacy of AMG 827 in subjects with moderate to severe Crohn’s diseaseGastroenterology20121433e26
- OgawaAAndohAArakiYBambaTFujiyamaYNeutralization of interleukin-17 aggravates dextran sulfate sodium-induced colitis in miceClin Immunol2004110556214962796
- YenDCheungJScheerensHIL-23 is essential for T cell-mediated colitis and promotes inflammation via IL-17 and IL-6J Clin Invest20061161310131616670770
- MonsenUSorstadJHellersGJohanssonCExtracolonic diagnoses in ulcerative colitis: an epidemiological studyAm J Gastroenterol1990857117162353691
- DasKMRelationship of extraintestinal involvements in inflammatory bowel disease: new insights into autoimmune pathogenesisDig Dis Sci19994411139952216
- VavrickaSRBrunLBallabeniPFrequency and risk factors for extraintestinal manifestations in the Swiss inflammatory bowel disease cohortAm J Gastroenterol2011106111011920808297
- AtreyaRZimmerMBartschBAntibodies against tumor necrosis factor (TNF) induce T-cell apoptosis in patients with inflammatory bowel diseases via TNF receptor 2 and intestinal CD14+ macrophagesGastroenterology201114162026203821875498
- ColombelJFSendidBJouaultTPoulainDSecukinumab failure in Crohn’s disease: the yeast connection?Gut201362800801
- Eligius HellströmAFärkkiläMKolhoKLInfliximab-induced skin manifestations in patients with inflammatory bowel diseaseScand J Gastroenterol201651556357126728295
- DenadaiRTeixeiraFVSaad-HossneRManagement of psoriatic lesions associated with anti-TNF therapy in patients with IBDNat Rev Gastroenterol Hepatol201291274423147656
- CullenGKroshinskyDCheifetzASKorzenikJRPsoriasis associated with anti-tumour necrosis factor therapy in inflammatory bowel disease: a new series and a review of 120 cases from the literatureAliment Pharmacol Ther20113411–121318132721957906
- GudjonssonJEKarasonARunarsdottirEHDistinct clinical differences between HLA-Cw*0602 positive and negative psoriasis patients – an analysis of 1019 HLA-C- and HLAB-typed patientsJ Invest Dermatol2006126474074516439971
- AndersonCAMasseyDCBarrettJCInvestigation of Crohn’s disease risk loci in ulcerative colitis further defines their molecular relationshipGastroenterology20091362523529.e319068216
- CargillMSchrodiSJChangMA large-scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis-risk genesAm J Hum Genet200780227329017236132
- SafranyESzaboMSzellMDifference of interleukin-23 receptor gene haplotype variants in ulcerative colitis compared to Crohn’s disease and psoriasisInflamm Res201362219520023093364
- CaponFDi MeglioPSzaubJSequence variants in the genes for the interleukin-23 receptor (IL23R) and its ligand (IL12B) confer protection against psoriasisHum Genet2007122220120617587057
- WolfNQuarantaMPrescottNJPsoriasis is associated with pleiotropic susceptibility loci identified in type II diabetes and Crohn diseaseJ Med Genet200845211411617993580
- CaponFBijlmakersMJWolfNIdentification of ZNF313/RNF114 as a novel psoriasis susceptibility geneHum Mol Genet200817131938194518364390
- KugathasanSBaldassanoRNBradfieldJPLoci on 20q13 and 21q22 are associated with pediatric-onset inflammatory bowel diseaseNature Genet2008401211121518758464
- HüffmeierULascorzJBeckerTCharacterisation of psoriasis susceptibility locus 6 (PSORS6) in patients with early onset psoriasis and evidence for interaction with PSORS1J Med Genet2009461173674419525279
- RiouxJDSilverbergMSDalyMJGenomewide search in Canadian families with inflammatory bowel disease reveals two novel susceptibility lociAm J Hum Genet20006661863187010777714
- HampeJShawSHSaizRLinkage of inflammatory bowel disease to human chromosome 6pAm J Hum Genet19996561647165510577918
- RiouxJDDalyMJSilverbergMSGenetic variation in the 5q31 cytokine gene cluster confers susceptibility to Crohn diseaseNature Genet20012922322811586304
- StalderJFTennstedtDDeleuranMFragility of epidermis and its consequence in dermatologyJ Eur Acad Dermatol Venereol201428Suppl 4118
- CameronALKirbyBGriffithsCECirculating natural killer cells in psoriasisBr J Dermatol2003149116016412890211
- HueberWSandsBELewitzkySSecukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: unexpected results of a randomised, double-blind placebo-controlled trialGut201261121693170022595313
- GladmanDDPsoriatic arthritisRheum Dis Clin North Am1998248298449891713
- AtzeniFDefendentiCDittoMCRheumatic manifestations in inflammatory bowel diseaseAutoimmun Rev2014131202323774109
- LemosLLde Oliveira CostaJAlmeidaAMTreatment of psoriatic arthritis with anti-TNF agents: a systematic review and meta-analysis of efficacy, effectiveness and safetyRheumatol Int201434101345136024728068
- TrikudanathanGVenkateshPGNavaneethanUDiagnosis and therapeutic management of extra-intestinal manifestations of inflammatory bowel diseaseDrugs201272182333234923181971
- ThapaSHadidHSchairerJImamWJafriSMEffect of inflammatory bowel disease-related characteristics and treatment interventions on cardiovascular disease incidenceAm J Med Sci2015350317518026226548
- HughJVan VoorheesASNijhawanRIFrom the Medical Board of the National Psoriasis Foundation: the risk of cardiovascular disease in individuals with psoriasis and the potential impact of current therapiesJ Am Acad Dermatol201470116817724184141
- BasavarajKHAshokNMRashmiRPraveenTKThe role of drugs in the induction and/or exacerbation of psoriasisInt J Dermatol201049121351136121091671
- DubeauMFIacucciMBeckPLDrug-induced inflammatory bowel disease and IBD-like conditionsInflamm Bowel Dis201319244545622573536
- MieleLValloneSCefaloCPrevalence, characteristics and severity of non-alcoholic fatty liver disease in patients with chronic plaque psoriasisJ Hepatol200951477878619664838
- WenkKSArringtonKCEhrlichAPsoriasis and non-alcoholic fatty liver diseaseJ Eur Acad Dermatol Venereol201125438339120840346
- TsaitasCSemertzidouASinakosEUpdate on inflammatory bowel disease in patients with primary sclerosing cholangitisWorld J Hepatol20146417818724799986
- GisbertJPGonzález-LamaYMatéJThiopurine-induced liver injury in patients with inflammatory bowel disease: a systematic reviewAm J Gastroenterol20071021518152717391318
- BangemannKSchulzWWohllebenJDepression and anxiety disorders among psoriasis patients: protective and exacerbating factorsHautarzt201465121056106125376619
- WalkerJRGraffLADutzJPBernsteinCNPsychiatric disorders in patients with immune-mediated inflammatory diseases: prevalence, association with disease activity, and overall patient well-beingJ Rheumatol Suppl201188313522045976
- LereboursEGower-RousseauCMerleVStressful life events as a risk factor for inflammatory bowel disease onset: a population based case-control studyAm J Gastroenterol200710212213117100973
- BernsteinCNBlanchardJFKliewerEWajdaACancer risk in patients with inflammatory bowel disease: a population-based studyCancer20019185486211241255
- BeyaertRBeaugerieLVan AsscheGCancer risk in immune-mediated inflammatory diseases (IMID)Mol Cancer20131219823987103
- PedersenNDuricovaDElkjaerMGamborgMMunkholmPJessTRisk of extra-intestinal cancer in inflammatory bowel disease: meta-analysis of population-based cohort studiesAm J Gastroenterol20101051480148720332773
- LaukoetterMGMennigenRHannigCMIntestinal cancer risk in Crohn’s disease: a meta-analysisJ Gastrointest Surg201115457658321152994
- CanavanCAbramsKRMayberryJMeta-analysis: colorectal and small bowel cancer risk in patients with Crohn’s diseaseAliment Pharmacol Ther2006231097111016611269
- DignassAVan AsscheGLindsayJOThe second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: current managementJ Crohns Colitis201041286221122489
- AkihoHYokoyamaAAbeSPromising biological therapies for ulcerative colitis: A review of the literatureWorld J Gastrointest Pathophysiol20156421922726600980
- OlteanuRZotaAParadoxical reactions induced by tumor necrosis factor-α antagonists: a literature review based on 46 casesIndian J Dermatol Venereol Leprol201682171226728803
- KivelevitchDMansouriBMenterALong term efficacy and safety of etanercept in the treatment of psoriasis and psoriatic arthritisBiologics2014816918224790410
- KaserANot all monoclonals are created equal – lessons from failed drug trials in Crohn’s diseaseBest Pract Res Clin Gastroenterol201428343744924913383
- MozaffariSNikfarSAbdolghaffariAHAbdollahiMNew biologic therapeutics for ulcerative colitis and Crohn’s diseaseExpert Opin Biol Ther201414558360024502344
- PuigLLópezAVilarrasaEGarcíaIEfficacy of biologics in the treatment of moderate-to-severe plaque psoriasis: a systematic review and meta-analysis of randomized controlled trials with different time pointsJ Eur Acad Dermatol Venereol201428121633165324033851
- WatanabeMHibiTMostafaNMLong-term safety and efficacy of adalimumab in Japanese patients with moderate to severe Crohn’s diseaseJ Crohns Colitis20148111407141624874893
- ThorlundKDruytsEMillsEJFedorakRNMarshallJKAdalimumab versus infliximab for the treatment of moderate to severe ulcerative colitis in adult patients naïve to anti-TNF therapy: an indirect treatment comparison meta-analysisJ Crohns Colitis20148757158124491514
- CauliAPigaMLubranoEMarchesoniAFlorisAMathieuANew approaches in tumor necrosis factor antagonism for the treatment of psoriatic arthritis: certolizumab pegolJ Rheumatol Suppl201593707226523062
- MoonWPestanaLBeckerBEfficacy and safety of certolizumab pegol for Crohn’s disease in clinical practiceAliment Pharmacol Ther201542442844026081839
- AroraZShenBBiological therapy for ulcerative colitisGastroenterol Rep201532103109
- CampanatiAGanzettiGGiuliodoriKMolinelliEOffidaniABiologic therapy in psoriasis: safety profileCurr Drug Saf201611141126463245
- SimonEGGhoshSIacucciMMoranGWUstekinumab for the treatment of Crohn’s disease: can it find its niche?Therap Adv Gastroenterol2016912636
- Cote-DaigneaultJBouinMLahaieRColombelJFPoitrasPBiologics in inflammatory bowel disease: what are the data?United European Gastroenterol J201535419428
- JaleelTElmetsCWeinkleAKassiraSElewskiBSecukinumab (AIN-457) for the treatment of psoriasisExpert Rev Clin Pharmacol20169218720226647300
- HueberWSandsBELewitzkySSecukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: unexpected results of a randomised, double-blind placebo-controlled trialGut201261121693170022595313
- GenentechVoluntary U.S. Market Withdrawal of Raptiva® (Efalizumab)2009 Available from: www.fda.gov/downloads/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/UCM149681.pdfAccessed May 2, 2016
- MrowietzUDommSSystemic steroids in the treatment of psoriasis: what is fact, what is fiction?J Eur Acad Dermatol Venereol20132781022102522830601
- NunesTBarreiro-de AcostaMMarin-JimenezINosPSansMOral locally active steroids in inflammatory bowel diseaseJ Crohns Colitis20137318319122784947
- Czarnecka-OperaczMSadowska-PrzytockaAThe possibilities and principles of methotrexate treatment of psoriasis – the updated knowledgePostepy Dermatol Alergol201431639240025610355
- VaysseTCarbonnelFMethotrexate in IBD: the return of the prodigal sonJ Crohns Colitis20159430330425814523
- KanwarAJYadavSDograSPsoriasis: what is new in nonbiologic systemic therapy in the era of biologics?Indian J Dermatol Venereol Leprol201076662263321079305
- AtwanAIngramJRAbbottROral fumaric acid esters for psoriasisCochrane Database Syst Rev20158CD010497
- CasiliGCordaroMImpellizzeriDDimethyl fumarate reduces inflammatory responses in experimental colitisJ Crohns Colitis201610447248326690241
- SoleymaniTVassantachartJMWuJJComparison of guidelines for the use of cyclosporine for psoriasis: a critical appraisal and comprehensive reviewJ Drugs Dermatol201615329330126954314
- ThinLWMurrayKLawranceICOral tacrolimus for the treatment of refractory inflammatory bowel disease in the biologic eraInflamm Bowel Dis20131971490149823615528
- YamammotoTShimoyamaTUmegaeSMatsumotoKTacrolimus vs antitumor necrosis factor agents for moderately to severely active ulcerative colitis: a retrospective observational studyAliment Pharmacol Ther201643670571626762838
- HoentjenFSakurabaAHanauerSUpdate on the management of ulcerative colitisCurr Gastroenterol Rep201113547548521789495
- BhartiRMesalazine in treatment of psoriasisIndian J Dermatol Venereol Leprol199662423123220948062
- MojaLDaneseSFiorinoGDel GiovaneCBonovasSSystematic review with network meta-analysis: comparative efficacy and safety of budesnide and mesalazine for Crohns diseaseAliment Pahrmacol Ther2015411110551065
- FeaganBGMacdonaldJKOral 5-aminosalicylic acid for maintenance of remission in ulcerative colitisCochrane Database Syst Rev201210CD00054423076890
- Du VivierAMunroDDVerbovJTreatment of psoriasis with aza-thioprineBr Med J1974149514812392
- ChandeNPattonPHTsoulisDJThomasBSMacDonaldJKAza-thioprine or 6-mercaptopurine for maintenance of remission in Crohn’s diseaseCochrane Database Syst Rev201510CD000067
- SoodRAnsariSClarkTHamlinPJFordACLong-term efficacy and safety of azathioprine in ulcerative colitisJ Crohns Colitis20159219119725518053
- FalaLOtezla (Apremilast), an oral PDE-4 inhibitor, receives FDA approval for the treatment of patients with active psoriatic arthritis and plaque psoriasisAm Health Drug Benefits20158Spec Feature10511026629274
- GordonJNProtheroJDThorntonCACC-10004 but not thalidomide or lenalidomide inhibits lamina propria mononuclear cell TNF-α and MMP-3 production in patients with inflammatory bowel diseaseJ Crohns Colitis20093317518221172267