
Abstract
Medication nonadherence is an important public health consideration, affecting health outcomes and overall health care costs. This review considers the most recent developments in adherence research with a focus on the impact of medication adherence on health care costs in the US health system. We describe the magnitude of the nonadherence problem and related costs, with an extensive discussion of the mechanisms underlying the impact of nonadherence on costs. Specifically, we summarize the impact of nonadherence on health care costs in several chronic diseases, such as diabetes and asthma. A brief analysis of existing research study designs, along with suggestions for future research focus, is provided. Finally, given the ongoing changes in the US health care system, we also address some of the most relevant and current trends in health care, including pharmacist-led medication therapy management and electronic (e)-prescribing.
Introduction
In 2010 the costs of health care in the US exceeded $2.7 trillion and accounted for 17.9% of the gross domestic product. Projections indicate health care will account for 20% of the US gross domestic product by 2020.Citation1–Citation4 Twenty percent to 30% of dollars spent in the US health care system have been identified as wasteful.Citation1,Citation2,Citation5 Providers and administrators have been challenged to contain costs by reducing waste and by improving the effectiveness of care delivered. Patient nonadherence to prescribed medications is associated with poor therapeutic outcomes, progression of disease, and an estimated burden of billions per year in avoidable direct health care costs.Citation6–Citation8 This review provides a general overview of nonadherence, its cost in specific illnesses, and approaches to improving medication adherence.
Definition and measurement of medication adherence
Patients are considered adherent to medications when they take prescribed agents at doses and times recommended by a health care provider and agreed to by the patient.Citation9 As the health care community adopts the concepts of patient centeredness and activation, it is moving away from the term “compliance”, which implies patient passivity in following the prescriber’s recommendations.Citation10 Medication persistence is the length of time from initiation to discontinuation of therapy.Citation11,Citation12
Adherence may be measured indirectly or directly as shown in . Two indirect adherence metrics used in research and administrative work are the medication possession ratio (MPR) and the proportion of days covered (PDC). MPR is calculated as the total number of days supplied, divided by the number of days between the first and last refills; while PDC is calculated as the total number of days supplied during an interval, divided by the total number of days during that interval.Citation13 An MPR of 80% is often used as the cut off between adherence and nonadherence based on its ability to predict hospitalizations across selected high prevalence chronic diseases.Citation14 These measures rely on pharmacy claims data, which does not account for the use of free drug samples, can miss coverage through a different insurance plans, and is insensitive to therapy changes.Citation15,Citation16 Insurance claims data also do not assess whether patients time doses, or use delivery devices, correctly. These protocols are important in conditions like COPD and asthma, where the way a patient uses inhaled therapy can also affect outcomes significantly.Citation17
Table 1 Methods of measuring adherence
In clinical settings, adherence may be indirectly assessed using patient recall. Because patients may significantly overestimate adherence during self-reports,Citation18 patient recall is more effectively interpreted when combined with a validated questionnaire to assess adherence barriers.Citation19–Citation21 Other methods such as pill counting and reviewing pill bottles against medication lists may provide important clinician insights and an opportunity for patient education.Citation22 Bidirectional electronic (e)-prescribing interfaces which provide clinicians data on medication refill intervals at the time of care, are available in settings with electronic medical records.Citation23 Electronic and mechanical dose counters provide estimates of adherence that can be reviewed during clinician visits; these may also improve adherence by providing patient reminders.Citation24 Finally, clinicians may assume patients are adherent with medications when therapeutic goals are achieved. Like claims data, clinical setting measures lack the ability to verify doses are taken but require less time and expense to implement, compared to directly measured adherence.
Direct methods, including observed therapy, and blood or urine drug and metabolite concentrations are most commonly used in research when therapy involves high risk medications, or when public health needs merit the additional costs, invasiveness, and resources required to implement them.Citation9,Citation25
Optimizing expenditures and outcomes
In 2010 spending for prescription drugs in the US was US$259 billion.Citation26 Considering the prevalent rates of nonadherence, drug-related expenses could increase substantially if adherence improved. Medication nonadherence is widespread and varied by disease, patient characteristics, and insurance coverage, with nonadherence rates ranging from 25% to 50%.Citation6,Citation27 In the US, nearly half of all adults have at least one chronic diseaseCitation28 and the percentage of Americans taking at least one prescription drug increased from 38% in the period 1988–1994 to 49% in the period 2007–2010; during the same time the number of adults taking three or more prescription drugs doubled.Citation26 Prescription medication use will increase as the population ages. Based on these statistics, increasing adherence from current levels could increase medication expenses by billions of dollars.
Strategies to enhance adherence should consider the impact on overall health care costs, weighing increased drug expenditures against savings from improved outcomes. The majority of the costs attributed to medication nonadherence result from avoidable hospitalization.Citation7 Additional direct costs are incurred by progression of controllable disease with: 1) increased service utilization at physician offices, emergency rooms, and urgent care and treatment facilities such as nursing homes, hospice, or dialysis centers; 2) avoidable pharmacy costs related to therapy intensification as comorbid conditions develop; and 3) diagnostic testing that could be avoided by controlling the primary illness.
Because the adverse consequences of most chronic illnesses may not present for years, it is argued that additional expenditure to increase medication adherence might not be economically attractive to payers. Even in illnesses where total health care costs are lower in adherent patients, savings might reflect the impact of patient characteristics, other than adherence, that make them healthier overall than nonadherers.Citation29 If this were true, investing resources in activating “unhealthy nonadherers” might not be cost effective. However, as discussed in our review, there is substantial evidence that the long term costs of poor outcomes exceed costs of medications in many chronic illnesses.Citation7
In contrast, increasing adherence in mild illness may not save costs. If the cost of the medication is relatively high, while the baseline rate of hospitalizations and emergency department visits is low (eg, mild asthma or early human immunodeficiency infection), total health care costs may increase with better adherence.Citation17,Citation30 In cases like these, using low-cost generic medications and targeting higher severity patients may shift the balance towards cost savings.
Increasing adherence in patients with higher acuity may be a better investment, especially when rates of hospitalization are high. An estimated 10% of hospitalizations in older adults may be caused by medication nonadherence.Citation29,Citation31 To prevent admissions and readmissions, payers and hospitals have implemented programs to improve medication adherence after discharge.Citation32,Citation33
Medication adherence and health care costs
The relationship between nonadherence and associated health care costs is shown in . Medication nonadherence leads to poor outcomes, which then increase health care service utilization and overall health care costs. The financial pressure is passed to patients by payers through higher copayments, or via higher costs to employers for coverage. Increased patient cost sharing beyond a threshold negatively impacts the level of medication adherence.Citation34 does not include other important drivers, such as the impact of reduced productivity, absenteeism, and increased disability on employers or society. It has been estimated that health-related productivity loss costs are 2.3 times higher than the direct health care costs.Citation35 Therefore, the benefits of improved medication adherence may be even greater when considered at a societal level. However, most of the existing studies consider only direct health care costs when estimating the impact of nonadherence, and typically do not include productivity and disability costs.Citation17 Medication waste accounts for a small percentage of these costs.Citation36,Citation37
Figure 1 Conceptual diagram displaying a mechanism that may contribute to the maintenance of the medication nonadherence problem within the US health care system.
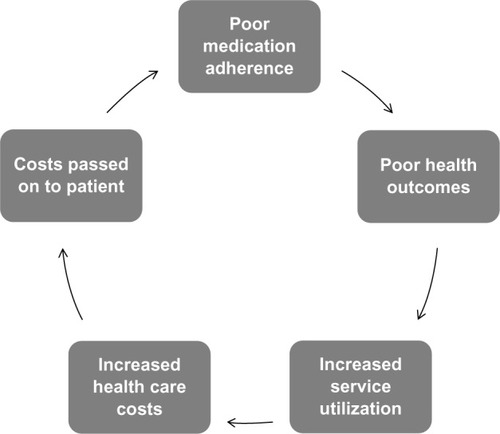
Between $100 and $300 billion of avoidable health care costs have been attributed to nonadherence in the US annually, representing 3% to 10% of total US health care costs.Citation7,Citation38 While there is substantial information relating nonadherence to poor patient outcomes, relatively few high quality studies report the impact on costs. The cost of nonadherence is generally determined by using administrative data to evaluate health care costs in populations of patients who are adherent compared to costs of populations of patients who are nonadherent. Systematic reviews of adherence note that differences in design, cost definitions, and included diagnosis (International Classification of Diseases [ICD]-9) groups, have varying levels of attributable-cost and make comparison of outcomes challenging. Over the last decade, the impact of adherence has been evaluated in association with numerous illnesses, including cardiovascular, pulmonary, gastrointestinal, metabolic, infectious, and psychiatric diseases. Representative findings are presented in our review, including summaries of systematic reviews when available.
Cardiovascular disease
Approximately 50% of patients with cardiovascular disease have poor adherence to their prescribed medications.Citation39 In a 2009 review, Ho et al concluded “Surprisingly little is known about the association between medication adherence and health care costs in cardiovascular populations”.Citation12 In Medicare and Medicaid beneficiaries with congestive heart failure, Esposito et al found that total health care costs showed a graded relationship to adherence measured by MPR, and, were as much as 23% less per year for adherent compared with nonadherent patients.Citation40 A retrospective longitudinal analyses by Sun et al, of more than 1,300 patients with heart failure or myocardial infarction after acute hospitalization revealed that adherence and persistence with angiotensin receptor blockers and angiotensin converting enzyme inhibitors resulted in lower risk of rehospitalization and lower health care costs.Citation41 Several studies have found strong associations between statin adherence and costs. In a retrospective cohort study of 381,422 patients using an integrated pharmacy and medical claims database, higher MPR was associated with reductions in subsequent total health care costs and cardiovascular disease-related hospitalizations.Citation42 Another retrospective claims-based study of 1,705 patients with diabetes and hyperlipidemia showed that adherence decreased all-cause medical costs by 15%.Citation43 Sokol et al reported that in a retrospective cohort observation of 137,277 benefit plan patients, high levels of adherence were significantly associated with lower overall health care costs for diabetes, hypercholesterolemia, and hypertension, but not with congestive heart failure.Citation29
COPD
In a 7-year retrospective administrative claims study of 55,076 chronic obstructive pulmonary disease (COPD) patients, Toy et al demonstrated an association between a high proportion of days covered (PDC) and fewer emergency department visits, and hospitalizations, resulting in a 2.2% reduction in overall costs.Citation44 A similar study of 33,816 Medicare beneficiaries diagnosed with COPD by Simoni-Wastila et al found a reduction (−$2,185 per patient) in the annual Medicare spending for patients with PDC higher than 80%, compared to patients with PDC below 80%.Citation45 Stuart et al compared users and nonusers of maintenance medication for COPD, and found use of maintenance therapy was associated with significantly lower risks of hospitalization and rehospitalization and reduced Medicare expenditures.Citation46
Asthma
In contrast to COPD, the studies have shown better adherence in asthma cohorts was associated with higher total health care costs. For example, a retrospective observational study of 18,456 Medicaid children aged 2–18 years diagnosed with asthma found lower rates of emergency room utilization, but did not demonstrate improved health care costs.Citation17 A retrospective observational study using 2 years of claims data for 41,234 commercially insured asthmatics found overall costs increased with better adherence, except for patients in high-risk subgroups with past emergency department visits or hospital admission.Citation30 Both studies suggest that improving medication adherence is cost saving in patients with severe disease, but increases overall costs in patients with mild disease, and a corresponding lower baseline rate of hospitalizations.Citation17,Citation30
Depression
In a retrospective study of patients initiating selective serotonin reuptake inhibitor (SSRI) therapy for depression and/or anxiety between July 2001 and June 2002, in a large national managed care database, Cantrell et al found approximately 43% of patients were adherent to antidepressant therapy, and adherent patients were associated with the lowest yearly medical costs.Citation48 Conversely, a study of 65,753 managed care patients between 2001 and 2002, found medical charges (mainly related to inpatient treatment), excluding pharmacy charges, were lower for patients remaining on antidepressant drug therapy for at least 90 days, but that when drug costs were added there was no difference between adherent and nonadherent patients.Citation49 Another study of 60,386 adult patients with depression studies showed adherent patients incurred an additional $806 in overall health care expenditures compared to nonadherent patients, in the 6 months following initiation of antidepressant therapy.Citation50
Diabetes
Multiple studies have evaluated the relationship of costs to diabetes, and generally support a correlation of increased adherence and reduced cost. One systematic review by Salas et al identified 209 studies, of which ten met inclusion criteria, and evidenced that despite significant methodological discrepancies among studies, low adherence was generally associated with higher costs.Citation51 Another systematic review identified 449 relevant articles (12 met criteria) and reached similar conclusions.Citation52 In a retrospective study of 57,687 patients, Hepke et al reported that overall health care costs were not lower among diabetic patients who were adherent with medications due to increased pharmaceutical costs, but suggested a threshold effect above which adherence was associated with reduced costs.Citation16 Balkrishan et al found that each 10% increase in adherence was associated with an 8.6% to 28.9% decrease in total annual health care costs.Citation47 More recently, in a longitudinal 4 year study of 740,195 veterans with type II diabetes, Egede found that nonadherent patients can have annual inpatient costs 41% higher compared to adherent patients, and concluded that significant costs could be avoided by increasing adherence.Citation53 The level of cost savings varies with the type of diabetes medication considered.Citation16,Citation54
HIV/AIDS
In a retrospective cohort study of 325 previously antiretroviral medication-naïve human immunodeficiency virus (HIV)-infected individuals initiating first antiretroviral therapy from 1997 through 2003, Gardner et al showed that better adherence to antiretroviral medication was associated with decreased health care utilization and associated costs; however, because of the high cost of antiretroviral therapy, total medical costs were increased.Citation55 A cohort study of 2,234 Medi-Cal patients with HIV reviewed outcomes in a patient subset served by medication therapy management (MTM) pharmacies versus other pharmacies; this documented higher medication adherence in MTM patients but no significant differences in total cost per patient per group.Citation56 Among HIV-infected veterans, some with drug resistant HIV and multiple comorbid conditions, high adherence with antiretroviral therapy was associated with lower rates of inpatient hospitalization but no difference in total annual health care costs.Citation57
Other illnesses
Studies of adherence and its impact on health care costs have been completed for other illnesses including musculoskeletal conditions, gastrointestinal and metabolic disorders, neurologic conditions, and others, and suggest varying levels of impact.Citation6,Citation9,Citation30,Citation58
Determinants of patient adherence
In order to improve medication adherence, clinicians must understand why patients fail to take prescribed medications. There is a large body of literature that investigates the determinants of medication nonadherence. These determinants can be categorized as patient related, provider related, and external factors.Citation9,Citation11 Patient related factors can be further divided into demographic, sociocultural and behavioral factors.Citation59 External factors include disease characteristics, medication properties and system components.Citation9,Citation11 depicts the relationship of patient, provider and external factors.
Figure 2 Selected determinants of medication adherence.
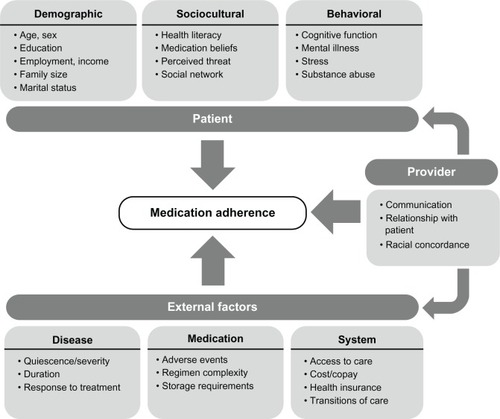
Among patients, forgetting is the most frequently reported reason for nonadherence.Citation60,Citation61 In a survey of 10,000 patients, the most common reported reason for missing medications was forgetfulness (24%), followed by perceived side effects (20%), high drug costs (17%), and perception that a prescribed medication would have little effect on their disease (14%).Citation62 In another survey of 14,464 Medicare beneficiaries, patients who did not fill at least one prescription reported the following reasons: “thought it would cost too much” (55.5%), “medicine not covered by insurance” (20.2%), “didn’t think medicine was necessary for the condition” (18.0%), and “was afraid of medicine reactions/contraindications” (11.8%).Citation63 More sophisticated patient assessment tools can elucidate psychological determinants such as self-reported medication self-efficacy, beliefs about medications and motivation that may impact adherence.Citation19,Citation64
In , providers are positioned as connectors between patient and external factors. In an effective provider–patient relationship, providers will engage patients in shared decision making regarding medication needs and expected efficacy. Communication is central to the effectiveness of this relationship. Zolnierek et al estimated in a recent meta-analysis, that poor communication results in a 19% higher risk of nonadherence.Citation65 Conversely, training physicians to improve their communication abilities leads to an improved chance of patient adherence.Citation65 Factors like racial concordance can affect physician–patient communication and clinical decision making. A qualitative study conducted by Snipes et al concluded that black physicians were more inclined than white physicians to take into account a patient’s race and cultural beliefs about disease when deciding among treatment alternatives.Citation66 From a provider perspective, inadequate time and communication tools were perceived to be the most important barriers to enhancing adherence.Citation67
Health care systems determine adherence in a number of ways. Restrictive formularies may limit access to prescribed medications and magnify patient barriers.Citation68 Systems should ensure patient benefits support appropriate access and utilization, and develop provider payment models and patient management services that encourage adherence. The impact of out-of-pocket patient cost on adherence is discussed below.
Numerous interdependencies exist between patient, provider, and system. For example, a perceived threat from a specific disease may be influenced by a patient’s sociocultural background, as well as the patient’s personal experience with the disease and its severity. Patient perceptions may be further influenced by clinician–patient communication, the strength of which may be a function of the patient’s cultural concordance and by system and provider factors. These relationships also suggest strategies that may enhance adherence.
Strategies to increase patient adherence
Strategies that may be used to increase medication adherence are presented in . These can be seen as targeting the patient, provider, and external determinants of adherence. A 2012 systematic review by Viswanathan et al evaluated interventions to improve adherence to self-administered medications for chronic disease, and found that reduced out-of-pocket patient costs (ROPC), case management and patient education improved adherence in more than one condition.Citation57 The review also found strong evidence for interventions such as collaborative care (in depression) and self-management (of asthma), but cautioned that benefits might not extend to other conditions. Disease self-management, patient engagement or “activation”, as measured by the validated questionnaires, has been linked to better health outcomes.Citation69,Citation70
Table 2 Selected strategies for improving medication adherence
Reducing out-of-pocket costs leads to better medication adherence across many diagnoses.Citation58 There is a linear relationship between the magnitude of patient cost sharing and the level of adherence.Citation34
This relationship persists from low to higher income levels. A large survey found that a significant percentage (14%) of high-income respondents also indicated cost-related nonadherence, despite relatively affordable copayments.Citation71
Whether ROPC will result in overall reductions in health care costs is less clear. Choudhry et al demonstrated that providing full prescription coverage to patients discharged after acute myocardial infarction improved mediation adherence by 4 to 6 percentage points but did not affect total health care costs despite some improvement in rates of subsequent first major vascular events.Citation72 A 2013 consensus panel review called for additional work to assess the effectiveness of ROPC studies.Citation73
Several studies have specifically reviewed use of financial incentives to increase medication adherence. A recent systematic review by DeFulio and Silverman identified 692 articles, 13 of which met inclusion criteria; across all studies, incentives increased adherence by a mean of 20 percentage points, but effects varied widely.Citation74 Providing incentives that are at risk for nonadherence may be an effective strategy, based on the behavioral construct of “loss aversion” which states that people experience more dissatisfaction from the loss of a certain dollar amount than the satisfaction from the gain of the same amount.Citation75 Two studies looking at the effect of lottery based incentives on anticoagulant adherence have had mixed results, but this concept needs further assessment. The impact on long term adherence has not yet been investigated.Citation76,Citation77
In contrast to population-based approaches, patient-specific approaches to nonadherence have been suggested. Marcum et al recently described use of validated adherence assessment tools to “diagnose” patient specific reasons for nonadherence, with subsequent effort directed at the specific barriers represented by that diagnosis.Citation20 This strategy suggests benefit for incorporating standard screening tools into patient interviews and reflects a need for patient centeredness in care delivery.
The way forward
Additional work is needed to elucidate the cost and impact of effort to improve adherence of patients. Because many reports studying the impact of medication adherence on health care costs are based on retrospective observational studies; it is difficult to prove causality between changes in medication adherence and corresponding effects on health care costs. Studies may be affected by the “healthy adherer” phenomenon, which occurs because healthier people may be more adherent, but also have better outcomes independent of the drug’s therapeutic impact.Citation54 As a consequence, it has been argued that more clinical trials, where randomization could remove some sources of bias, should be designed to directly investigate the cost impact.Citation29 Because of the insensitivity of current diagnosis groups to disease severity or stage, as in congestive heart failure or asthma, the planned national implementation of ICD-10, which has much more specificity, may improve identification of specific populations where efforts to increase adherence would achieve greatest gains.
Team-based case management is already recognized as an effective care strategy that improves adherence and health outcomes, and can decrease overall medical care costs. The guiding principles of patient-centered medical homes include the maintenance of a longitudinal patient relationship with a personal physician together with a multidisciplinary care team who together take a whole-person approach and coordinate care across settings is also a key component.Citation78 Since the “medical home” model is relatively new and still under assessment, its impact on health care costs as related to improvements in medication adherence remains to be fully demonstrated.
Pharmacists can play integral roles within medical homes.Citation79 Pharmacist led multi-pronged interventions have indeed been demonstrated to improve outcomes.Citation58 From a legislative perspective, the Medicare Modernization Act of 2003 required Medicare part D plans to implement medication therapy management services provided by clinical pharmacists, while the 2010 Affordable Care Act provided more guidance and expanded patient eligibility.Citation80 These services include a comprehensive assessment of current medications, which includes counseling regarding the importance of adherence, and the design of a medication related action plan.Citation81 A recent review of studies evaluating medication therapy management programs has identified key elements that improve outcomes, such as providing services to patients with specific therapeutic problems, having routine communications with primary care providers, and having regular follow-up to encourage medications adherence after changes in the medication regimen.Citation82
E-prescribing is another intervention with the potential to improve medication adherence and total health care costs, and is becoming more widely used as electronic medical records are integrated into medical practices. E-prescribing differs from simple transmission of prescriptions directly to pharmacies and allows prescribers to receive an electronic notice from the pharmacy telling them that a patient’s prescription has been picked up, not picked up, or has been partially filled, to help monitor medication adherence in patients with chronic conditions. A recent study, conducted by Surescripts in collaboration with pharmacies and pharmacy benefit managers, analyzed over 40 million prescription records, observing that e-prescribing increased the percentage of new prescriptions that were picked up by patients from the pharmacy by 10%, compared to paper prescriptions. In the absence of e-prescribing, only 73.2% of paper prescriptions make it to the pharmacy and an even smaller percentage of the total prescriptions written are picked up by patients. The same study estimated that e-prescribing and the corresponding increase in first-fill medication adherence would save at least $140 billion over the following decade.Citation83 Additional studies to validate the impact of e-prescribing systems and electronic medical records on adherence and related cost savings are needed.Citation84
Conclusion
Medication nonadherence is a significant contributor to avoidable health care costs in this country. While impact on disease outcome and cost is more pronounced in some illnesses than others, stakeholders agree that increasing medication adherence would improve health outcomes and save billions of dollars. Improved adherence can be achieved through better education, value-based insurance designs, and thoughtful use of patient incentives. Ultimately collaboration between patients, payers, policy makers and providers, and redesigning systems to employ more team-based care, use lower cost medications, and target highest cost illnesses, will be needed to achieve better adherence and optimize spending.
Disclosure
The authors report no conflicts of interest in this work.
References
- Centers for Medicare and Medicaid ServicesNHE Projections 2010–2020Washington, DCUS Department of Health and Human Services2011
- Kaiser Family FoundationHealth care costs: a primer Available from: http:www.kff.org/insurance/upload/7670-7603.pdfAccessed August 7, 2013
- SchroederSAShattuck lecture. We can do better – improving the health of the American peopleN Engl J Med20073571212211228
- The US Department of TreasuryThe 2012 annual report of the boards of trustees of the federal hospital insurance and federal supplementary medical insurance trust funds2012 Available from: http://www.treasury.gov/resource-center/economic-policy/ss-medicare/Documents/TR_2012_Medicare.pdfAccessed August 7, 2013
- BerwickDMHackbarthADEliminating waste in US health careJAMA20123071415131516
- DiMatteoMRVariations in patients’ adherence to medical recommendations: a quantitative review of 50 years of researchMed Care2004423200209
- IMS Institute for Healthcare InformaticsAvoidable costs in US health care2013 Available at: http://www.imshealth.com/deployedfiles/imshealth/Global/Content/Corporate/IMS%20Institute/RUOM-2013/IHII_Responsible_Use_Medicines_2013.pdf Accessed September 10, 2013
- DiMatteoMREvidence-based strategies to foster adherence and improve patient outcomesJAAPA200417111821
- OsterbergLBlaschkeTAdherence to medicationN Engl J Med20053535487497
- HansenRAFarleyJFDroegeMMaciejewskiMLA retrospective cohort study of economic outcomes and adherence to monotherapy with metformin, pioglitazone, or a sulfonylurea among patients with type 2 diabetes mellitus in the United States from 2003 to 2005Clin Ther201032713081319
- BosworthHBGrangerBBMendysPMedication adherence: A call for actionAm Heart J20111623412424
- HoPMBrysonCLRumsfeldJSMedication adherence: Its importance in cardiovascular outcomesCirculation20091192330283035
- LaFleurJOderdaGMMethods to measure patient compliance with medication regimensJ Pain Palliat Care Pharmacother20041838187
- KarveSClevesMAHelmMHudsonTJWestDSMartinBCGood and poor adherence: Optimal cut-point for adherence measures using administrative claims dataCurr Med Res Opin200925923032310
- SikkaRXiaFAubertREEstimating medication persistency using administrative claims dataAm J Manag Care2005117449457
- HepkeKLMartusMTShareDACosts and utilization associated with pharmaceutical adherence in a diabetic populationAm J Manag Care2004102 Pt 2144151
- HerndonJBMattkeSEvans CuellarAHongSYShenkmanEAAnti-inflammatory medication adherence, health care utilization and expenditures among medicaid and children’s health insurance program enrollees with asthmaPharmacoeconomics2012305397412
- Express Scripts2011 drug trend report2012 Available from: http://www.drugtrendreport.com/docs/DTR-2011.pdfAccessed September 21, 2013
- LavsaSMHolzworthAAnsaniNTSelection of a validated scale for measuring medication adherenceJ Am Pharm Assoc (2003)20115119094
- MarcumZASevickMAHandlerSMMedication nonadherence: A diagnosable and treatable medical conditionJAMA20133092021052106
- MoriskyDEGreenLWLevineDMConcurrent and predictive validity of a self-reported measure of medication adherenceMed Care19862416774
- MartinezMLVande GriendJPLinneburSAMedication management: A case of brown bag-identified medication hoardingConsult Pharm20122710729736
- HarbigPBaratILund NielsenPDamsgaardEMInstantaneous detection of nonadherence: Quality, strength, and weakness of an electronic prescription databasePharmacoepidemiol Drug Saf2012213323328
- RandCSWiseRAMeasuring adherence to asthma medication regimensAm J Respir Crit Care Med19941492 Pt 2S69S76 discussion S77–S78
- LauzardoMPeloquinCAAntituberculosis therapy for 2012 and beyondExpert Opin Pharmacother2012134511526
- National Center for Health StatisticsHealth, United States, 2012: With special feature on emergency care2013 Available from: http://www.cdc.gov/nchs/data/hus/hus12.pdfAccessed September 21, 2013
- HaynesRBMontaguePOliverTMcKibbonKABrouwersMCKananiRInterventions for helping patients to follow prescriptions for medicationsCochrane Database Syst Rev20002CD000011
- Centers for Disease Control and PreventionChronic diseases and health promotion2013 Available from: http://www.cdc.gov/chronicdisease/overview/index.htmAccessed September 21, 2013
- SokolMCMcGuiganKAVerbruggeRREpsteinRSImpact of medication adherence on hospitalization risk and health care costMed Care2005436521530
- MattkeSMartorellFHongSYSharmaPCuellarALurieNAnti-inflammatory medication adherence and cost and utilization of asthma care in a commercially insured populationJ Asthma2010473323329
- VermiereEAvontsDVan RoyenPBuntinxFDenekensJContext and health outcomesLancet2001357927320592060
- SarangarmPLondonMSSnowdenSSImpact of pharmacist discharge medication therapy counseling and disease state education: Pharmacist assisting at routine medical discharge (project PhARMD)Am J Med Qual2013284292300
- HesselinkGSchoonhovenLBarachPImproving patient handovers from hospital to primary care: A systematic reviewAnn Intern Med2012157641742822986379
- EaddyMTCookCLO’DayKBurchSPCantrellCRHow patient cost-sharing trends affect adherence and outcomes: A literature reviewP T2012371455522346336
- LoeppkeRTaitelMHaufleVParryTKesslerRCJinnettKHealth and productivity as a business strategy: A multiemployer studyJ Occup Environ Med2009514411428
- MorganTMThe economic impact of wasted prescription medication in an outpatient population of older adultsJ Fam Pract2001509779781
- BainTPublic health implications of household pharmaceutical waste in the United StatesHealth Services Insights2010321
- BenjaminRMMedication adherence: Helping patients take their medicines as directedPublic Health Rep2012127123
- KronishIMYeSAdherence to cardiovascular medications: Lessons learned and future directionsProg Cardiovasc Dis2013556590600
- EspositoDBagchiADVerdierJMBencioDSKimMSMedicaid beneficiaries with congestive heart failure: Association of medication adherence with health care use and costsAm J Manag Care2009157437445
- SunSXYeXLeeKYDupclayLJrPlauschinatCRetrospective claims database analysis to determine relationship between renin-angiotensin system agents, rehospitalization, and health care costs in patients with heart failure or myocardial infarctionClin Ther200830Pt 222172227
- PittmanDGChenWBowlinSJFoodyJMAdherence to statins, subsequent health care costs, and cardiovascular hospitalizationsAm J Cardiol20111071116621666
- WuJSeiberELacombeVANahataMCBalkrishnanRMedical utilization and costs associated with statin adherence in medicaid enrollees with type 2 diabetesAnn Pharmacother2011453342349
- ToyELBeaulieuNUMcHaleJMTreatment of COPD: Relationships between daily dosing frequency, adherence, resource use, and costsRespir Med20111053435441
- Simoni-WastilaLWeiYJQianJAssociation of chronic obstructive pulmonary disease maintenance medication adherence with all-cause hospitalization and spending in a medicare populationAm J Geriatr Pharmacother2012103201210
- StuartBCSimoni-WastilaLZuckermanIHImpact of maintenance therapy on hospitalization and expenditures for medicare beneficiaries with chronic obstructive pulmonary diseaseAm J Geriatr Pharmacother201085441453
- BalkrishnanRRajagopalanRCamachoFTPredictors of medication adherence and associated health care costs in an older population with type 2 diabetes mellitus: a longitudinal cohort studyClin Ther200311251129582971
- CantrellCREaddyMTShahMBReganTSSokolMCMethods for evaluating patient adherence to antidepressant therapy: A real-world comparison of adherence and economic outcomesMed Care2006444300303
- EaddyMTDrussBGSarnesMWReganTSFrankumLERelationship of total health care charges to selective serotonin reuptake inhibitor utilization patterns including the length of antidepressant therapy – results from a managed care administrative claims databaseJ Manag Care Pharm2005112145150
- RobinsonRLLongSRChangSHigher costs and therapeutic factors associated with adherence to NCQA HEDIS antidepressant medication management measures: Analysis of administrative claimsJ Manag Care Pharm20061214354
- SalasMHughesDZuluagaAVardevaKLebmeierMCosts of medication nonadherence in patients with diabetes mellitus: A systematic review and critical analysis of the literatureValue Health2009126915922
- BreitscheidelLStamenitisSDippelFWSchoffskiOEconomic impact of compliance to treatment with antidiabetes medication in type 2 diabetes mellitus: A review paperJ Med Econ2010131815
- EgedeLEGebregziabherMDismukeCEMedication nonadherence in diabetes: Longitudinal effects on costs and potential cost savings from improvementDiabetes Care2012351225332539
- StuartBDavidoffALopertRShafferTSamantha ShoemakerJLloydJDoes medication adherence lower medicare spending among beneficiaries with diabetes?Health Serv Res20114641180119921413981
- GardnerEMMaraviMERietmeijerCDavidsonAJBurmanWJThe association of adherence to antiretroviral therapy with health care utilization and costs for medical careAppl Health Econ Health Policy200862–3145155
- HirschJDGonzalesMRosenquistAMillerTAGilmerTPBestBMAntiretroviral therapy adherence, medication use, and health care costs during 3 years of a community pharmacy medication therapy management program for medi-cal beneficiaries with HIV/AIDSJ Manag Care Pharm2011173213223
- BarnettPGChowAJoyceVRDeterminants of the cost of health services used by veterans with HIVMed Care2011499848856
- ViswanathanMGolinCEJonesCDInterventions to improve adherence to self-administered medications for chronic diseases in the United States: A systematic reviewAnn Intern Med2012
- KruegerKPBergerBAFelkeyBMedication adherence and persistence: A comprehensive reviewAdv Ther2005224313356
- BoskovicJLeppeeMCuligJEricMPatient self-reported adherence for the most common chronic medication therapyScand J Public Health2013414333335
- BarfodTSSorensenHTNielsenHRodkjaerLObelN‘Simply forgot’ is the most frequently stated reason for missed doses of HAART irrespective of degree of adherenceHIV Med200675285290
- Boston Consulting GroupThe hidden epidemic: finding a cure for unfilled prescriptions and missed doses2003 Available from: http://www.bcg.com/documents/file14265.pdfAccessed September 10, 2013
- KennedyJTuleuIMackayKUnfilled prescriptions of medicare beneficiaries: Prevalence, reasons, and types of medicines prescribedJ Manag Care Pharm2008146553560
- VoilsCIMaciejewskiMLHoyleRHInitial validation of a self-report measure of the extent of and reasons for medication nonadherenceMed Care2012501210131019
- ZolnierekKBDimatteoMRPhysician communication and patient adherence to treatment: A meta-analysisMed Care2009478826834
- SnipesSASellersSLTafawaAOCooperLAFieldsJCBonhamVLIs race medically relevant? A qualitative study of physicians’ attitudes about the role of race in treatment decision-makingBMC Health Serv Res2011111836963
- BruntonSAImproving medication adherence in chronic disease managementJ Fam Pract2011604S1S8
- BraithwaiteSShirkhorshidianIJonesKJohnsrudMThe role of medication adherence in the US healthcare system2013 Available from: http://static.correofarmaceutico.com/docs/2013/06/24/adher.pdfAccessed September 10, 2013
- GreeneJHibbardJHWhy does patient activation matter? an examination of the relationships between patient activation and health-related outcomesJ Gen Intern Med2012275520526
- HibbardJHStockardJMahoneyERTuslerMDevelopment of the patient activation measure (PAM): Conceptualizing and measuring activation in patients and consumersHealth Serv Res2004394 Pt 110051026
- PietteJDBeardARoslandAMMcHorneyCABeliefs that influence cost-related medication non-adherence among the “haves” and “have nots” with chronic diseasesPatient Prefer Adherence20115389396
- ChoudhryNKAvornJGlynnRJFull coverage for preventive medications after myocardial infarctionN Engl J Med20113652220882097
- Community Preventive Services Task ForceAnnual report to congress2013 Available from: http://www.thecommunityguide.org/annualreport/2013-congress-report-full.pdfAccessed September 21, 2013
- DeFulioASilvermanKThe use of incentives to reinforce medication adherencePrev Med201255SupplS86S94
- KimmelSETroxelABNovel incentive-based approaches to adherenceClin Trials201296689695
- VolppKGLoewensteinGTroxelABA test of financial incentives to improve warfarin adherenceBMC Health Serv Res20088272
- KimmelSETroxelABLoewensteinGRandomized trial of lottery-based incentives to improve warfarin adherenceAm Heart J20121642268274
- RosenthalTCThe medical home: Growing evidence to support a new approach to primary careJ Am Board Fam Med2008215427440
- SmithMBatesDWBodenheimerTClearyPDWhy pharmacists belong in the medical homeHealth Aff (Millwood)201029590691320439879
- Lee-WilsonCMAEstablishing a medication therapy management (MTM) practice: Obtaining compensation for clinical servicesMaryland Pharmacist20113
- National Conference of State LegislaturesMedication therapy management: Pharmaceutical safety and savingsNational Conference of State Legislatures Web site http://www.ncsl.org/issues-research/health/medication-therapy-management.aspxAccessed December 19, 2012
- KucukarslanSNHaganAMShimpLAGaitherCALewisNJIntegrating medication therapy management in the primary care medical home: A review of randomized controlled trialsAm J Health Syst Pharm2011684335345
- E-prescribing shown to improve outcomes, save billions. Study quantifies relationship between e-prescribing and medication adherence, with potential savings of $140 billion over the next 10 yearsHealth Manag Technol20123342223
- BlumenthalDTavennerMThe “meaningful use” regulation for electronic health recordsN Engl J Med20103636501504
- McDonaldHPGargAXHaynesRBInterventions to enhance patient adherence to medication prescriptions: Scientific reviewJAMA20022882228682879
- GrangerBBBosworthHBMedication adherence: Emerging use of technologyCurr Opin Cardiol201126427928721597368
- CooperLARoterDLCarsonKAA randomized trial to improve patient-centered care and hypertension control in underserved primary care patientsJ Gen Intern Med2011261112971304
- KripalaniSYaoXHaynesRBInterventions to enhance medication adherence in chronic medical conditions: A systematic reviewArch Intern Med20071676540550
- GolayAPharmacoeconomic aspects of poor adherence: can better adherence reduce healthcare costs?J Med Econ2011145594608