
Abstract
Background
Healthcare professionals are at the frontline facing the pandemic. Since the pandemic is new with sophisticated needs of resources, identifying perceived barriers of the healthcare institutions has an important input for the government in slowing the viral spread and prevents healthcare professionals from infection.
Objective
The study was aimed to assessperceived barriers and preventive measures of corona virus disease among healthcare providers in Debretabor Town, north central Ethiopia.
Methods
An institution-based cross-sectional survey was conducted among healthcare providers working in Debretabor town, north central Ethiopia from May 1 to 15, 2020. Data were collected using a self-administered questionnaire. Data were coded, entered, cleaned, and checked using Epi data statistical software version 4.2.0.0 and analysis using STATA Version 14 statistical software. Descriptive statistics of different variables were presented in figures, text, and tables. Chi-square (chi2) test of independence was considered to examine the nonparametric association of factors with preventive practice, and association was considered at a P-value of less than 0.05.
Results
A total of 183 healthcare providers participated in the survey, of which 67.76% were males, and 80.87% were in the age range of 25–35 years. About 45% of participants were nurses. In the current study, overall preventive practice was 68.3%. Despite recommendations by the World Health Organization, avoidance of outdoor, physical distancing, and avoiding meeting a person with a coughwere not implemented by 32.24%, 24.18%, and 13.11% of healthcare providers, respectively. Insufficient training, lack of policy, less commitment to infection control, and limitations of resources were perceived as major barriers for practicing preventive measures during the pandemic.
Conclusion
Preventive measures taken by healthcare providers were poor. Multiple barriers, such as insufficient training related to the pandemic, limitation of resources, and less commitment of healthcare providers to infection prevention measures were reported. So, the government should work on reducing the pandemic propagation by fulfilling the barriers using different means or strategies.
Introduction
Based on current evidence, COVID-19 is primarily transmitted by respiratory droplets and contact.Citation1,Citation2 It has a tremendous strain on resources in the healthcare setting. The burden is high in low and middle income countries like Ethiopia.Citation3
The acquisition of occupationally-acquired infections may pose a risk to healthcare providers, patients, families, and the community at large. On top of that, outbreaks result in significant cost to health organizations, high cost of modifications, and lack of time/space.Citation4,Citation5 One of the most persistent issues is the rapid depletion of personal protective equipment (PPE).
The World Health Organization and Center of Disease Control (CDC) recommend preventive measures during the pandemic such as canceling elective procedures, isolating symptomatic patients earlier, protecting healthcare personnel through implementation of hand hygiene, install barriers to limit contact with patients at triage, cohort COVID-19 patients, limit the numbers of staff providing their care, risk communication, and prioritize respirators.Citation6,Citation7 Based on reports, implementing preventive and control measures in China during the first seasons of COVID-19 pandemic prevented more than 700,000 infections across the country.Citation8
Despite the recommendations to prevent the transmission of COVID-19, different barriers were reported by healthcare personnel. Accordingly, the shortage of personal protective equipment, poor quality PPE, scarce diagnostic kits, turnover of staffingCitation9–Citation12 inadequate training, poor adherence, poor practice to infection prevention (IP) measures, rumors and social stigma,Citation13,Citation14 risk of violence,Citation15 poor compliance to physical distancing,Citation16 and fears about unpaid sick leaveCitation17 were reported.
In addition, overcrowding of healthcare institutions in a totally new context, heavy workload, fear of becoming infected and infecting others, feeling powerless to handle the patient’s condition.Citation17 Insufficient scientific data on SARS-COV-2,Citation18 working in high-risk departments, longer duty hours, and suboptimal hand hygiene,Citation19 inadequate knowledge of COVID-19, deviations from the recommended PPE donning and doffing protocolCitation12,Citation20 and increase the risk of acquiring the infection. A recent study showed that 90% of observed doffing was incorrect, common errors were doffing gown from the front, removing face shield of the mask, and touching potentially contaminated surfaces and PPE.Citation21 Subsequently, professional supervision, guidance, monitoring mechanism, and routine daily environmental disinfection were also lacking as the COVID-19 pandemic disseminates all over the world.Citation20,Citation22,Citation23
Studies showed that infection prevention measures were 88.7% in Pakistan,Citation24 Gondar, 47.3%,Citation25 in Amhara region, 62%,Citation26 Debre Markos, Addis Ababa, and Mekele, 57.3%, 66.1%, and 42.9%, respectively.Citation27–Citation29 The study conducted in Ethiopia showed that 42.1% had low perception to the efficacy of COVID-19 prevention measures and 28.3% had lower intention to carry out those prevention measures.Citation30 Poor practice of IP add up to the challenges facing healthcare workers in the COVID-19 pandemic in Ethiopia.
Infection prevention could be the primary focus during pandemic season, even if facing a shortage of resources. This could be alleviated by rational use and successful reuse of PPE;Citation31,Citation32 improving the logistics of PPE distribution to wards; maintaining written PPE use protocols; and providing structured donning and doffing training with practical simulation;Citation11,Citation33,Citation34 improving knowledge; positive attitudes and practicesCitation35 hopefully can control the spread of COVID-19. Therefore, this study was aimed to assess perceived barriers and preventive measures during the COVID-19 pandemic among healthcare professionals at South Gondar zone, North Central Ethiopia.
Materials and Methods
Study Design, Period, Setting, and Population
An institution-based cross-sectional survey was employed in north central Ethiopia from May 1–15/2020. Debre Tabor town is located in South Gondar Administrative Zone of the Amhara regional state, at a distance of 667 kilometers away from Addis Ababa, the capital city of Ethiopia, and 50 kilometers east of Lake Tana.Citation36 The town has one general hospital and three health centers. All Healthcare professionals (HCPs) working in governmental healthcare institutions (Medical Doctors, nurses, medical lab, pharmacists, anesthetists, midwifery, physiotherapy, optometry, public health officer, and psychiatrist) working in Debretabor town were the source population. A total of 183 HCWs were included during the survey.
Sample Size Calculation and Sampling Technique
The sample size for the study was calculated using a single proportion formula by assuming 95% CL, 5% marginal error, and 50% proportion.
no=(Za/2)2p(1-p)/d2=384
Since the total population is less than 10,000 we used reduction formula.
So, . Where n is the sample size (384) and N is the population size (432).
The final sample size was n=203.
Healthcare providers working in Debretabor town were involved in the study. Since the data collection time at state of emergency and staff reduction, the study participants were those healthcare professional found at healthcare institutions during the data collection period, selected by convenience sampling technique.
Data Collection
Data were collected by using self-administered questionnaire which was adopted from World Health Organization (WHO), and previous researches,Citation7,Citation24,Citation26,Citation37,Citation38 with some adjustment. The tool was composed of three parts, ie, Socio-demographic and work related characteristics, perceived barriers related factors, and preventive measures related factors. The data were collected by two BSc Nurses and one MSC supervisor. Completeness of each recording format was checked before collecting the data. Convenience sampling method was used to select the study participants.
Variables
Dependent Variable
Preventive practice (Good, Poor).
Independent Variable
Socio-demographic and personal related factors (age, sex, marital status, monthly income, profession, year of experience), and perceived barriers.
Operational Definitions
Good preventive practice – if the score is above or equal to mean score.
Data Quality Control
Training was given for 1 day on how to administer questionnaires, handling ethical issues and maintaining confidentiality and privacy. Pretest was done on 5% of the sample size. Cronbach’s alpha was used to check the internal validity of the tool and the value of “α” was 0.73. Completeness of each data collection tools was checked by the principal investigator and the supervisors in a daily base. Double data entry was done by two data clerks and consistency of the entered data was cross-checked.
Data Processing and Analysis
Data were entered, coded, cleaned, and checked by Epi-Data statistical software version 4.2.0.0 and analysis using STATA Version 14 statistical software. Chi square test was used to test show the non-parametric association of factors with preventive practice. Independent Variables with P-value less than 0.05 in chi-square test were considered as significantly associated. Finally, the data were presented in texts, figures, and tables.
Results
Sociodemographic Characteristics of the Participants
In the current study, a total of 183 healthcare professionals participated in the survey with response rate of 90.15%. Two thirds (67.76%) of healthcare providers were males. Four fifths (80.87%) of HCWs were in the age range of 25–35 years. More than half (53.85%) participants married and almost half (45.36%) of the participants were nurses followed by medical doctors (13.66%). Eighty-seven (47.54%) of the participants had a monthly income of greater than 6,500 Ethiopian Birr (ETB) ().
Table 1 Sociodemographic and Work-Related Characteristics of Healthcare Professional in Debretabor Town, North Central Ethiopia
Preventive Measures Among Healthcare Professionals
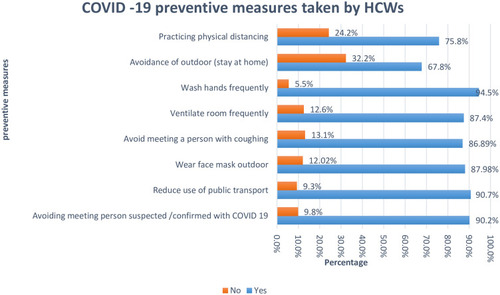
Healthcare professionals are required to practice infection prevention measures of corona virus disease. A total of eight preventive measure questions were asked. The mean (±SD) score was 9.2±1.47. Overall, good preventive practice among HCWs was 68.31% (95% CI=67.6–69). In the current study, the majority (90.16%) of HCWs avoid meeting person suspected/confirmed of COVID-19 and reduce use of public transportation. One hundred and sixty-one (87.985%) HCWs wear a facemask outdoors and similarly ventilate the room frequently as one preventive measure of COVID-19. About 32.24% and 24% of healthcare professional did not stay at home, and did not practice physical distancing, respectively ().
Figure 1 COVID-19 preventive measures practiced by HCWs in, North Central Ethiopia.
Perceived Barriers Reported by Healthcare Providers
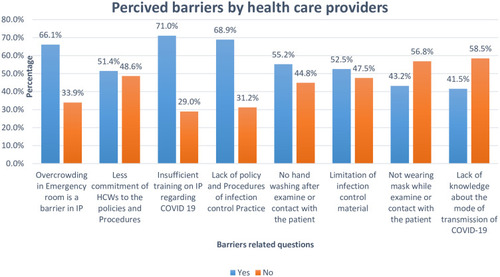
A total of eight questions related to perceived barriers that the healthcare institution may face during the rapid expansion of corona virus pandemic were included. Two thirds (66.12%) of healthcare professionals perceive overcrowding in the Emergency room as a barrier in infection control practice. Almost half (51.37%) reported less commitment of the providers as a barrier. Insufficient training, lack of policy, no handwashing after contacting patients, limitation of infection control materials, and not wearing a mask were reported as barriers of practicing preventive measures by 71.04%, 68.85%, 55.2%, 52.46% and 43.17% of healthcare professionals, respectively ().
Figure 2 Perceived barriers reported by HCWs in implementing COVID-19 preventive measures in North Central Ethiopia, 2020.
Factor Associated with Preventive Practice
In this study, based on the cross-tabulation; sex, age, profession, and work experience were found to be significantly associated with preventive practice as evidenced by chi-square values of 4.10, 11.71, 7.27, 7.08, and P-values of 0.043, 0.026, and 0.029, respectively. Male HCWs were 4-times more likely to practice preventive measures than female HCWs (chi2=4.10 at a P-value of 0.043) ().
Table 2 Chi-Square Test of Independence for Practice of Preventive Measures Among HCWs in North Central Ethiopia, 2020.
Discussion
During the pandemic, healthcare professionals have implemented different preventive measures of coronavirus disease as of World Health Organization recommendations. However, not all healthcare professional are practicing those preventive measures. In the current study, good preventive measures were implemented by 68.31%. This is higher than a study conducted in Ethiopia (62%).Citation26 The possible reason could be the difference in sample size, way of data collection, and area coverage, but lower than a studies conducted in China (89.7%)Citation39 and Pakistan (88.7%).Citation24 This could be due to those studies being conducted in the country where the pandemic was first detected. In addition, China had previous experience of the pandemic. In another way there is a big difference in socio economical and healthcare system.
The majority, of participants’ practice the recommended preventive measures, however low in implementing physical distancing, and stay home (). Physical distancing and movement restrictionCitation40–Citation42 had been declared as one of the most effective for mitigating the pandemics. The study conducted in ChinaCitation43 revealed that implementing social/physical distancing was sufficient to control COVID-19. Another study showed that implementation of any physical distancing intervention reduced Covid-19 incidence by 13%.Citation44 In this study, only three quarters (75.82%) of participants practice physical distancing. Evidence from EthiopiaCitation37 at the beginning of the epidemic showed physical distancing was less implemented. This increased mass gathering and transmission of coronavirus.
A low level of practicing preventive measures may be associated with different barriers. Two thirds (66.12%) of healthcare professionals perceived overcrowding in the Emergency room as a barrier in infection control practice. This is higher than a study conducted in Pakistan, where it was only 52.9%.Citation24 HCWs perceive overcrowding in the Emergency room is a barrier in infection control practice. The possible difference could be Pakistan had an experience of previous pandemic like influenza so had a better clinical setup for the pandemic.
More than half (52.46%) reported the limitation of infection control material to be a barrier during the pandemic. A similar study in Pakistan showed that 50.7%Citation24 of HCWs reported limited infection control materials. This was also reported by similar studies done in Ethiopia,Citation45,Citation46 where resource scarcity was the main reason to practice preventive measures. This is true that provide intense education and training on use of personal protective equipment, hand hygiene, ward disinfection, medical waste management, and sterilization of patient-care devices and management of occupational exposureCitation20,Citation47 reduce the burden of pandemic infection. In addition, a shortage of PPECitation46 is the main headache for Ethiopia during the pandemic season.
More than half (55.19%) reported that no hand washing after examinations or contact with the patient was a barrier for preventive measures of coronavirus disease. This is higher than the studies conducted in Gondar hospital (14.9%),Citation48 and central Gondar (16.5%).Citation49 The possible reasons could be the current study is conducted during the pandemic. Poor accessibility of hand washing facilities, knowledge of infection prevention, and workover loadCitation50 were reported as barriers for poor hand hygiene compliance in developing countries. Future studies should be conducted by including behavioral (attitudinal) factors, cultural factors, socioeconomical and work satisfaction related factors which may have a great impact on those preventive measure. Since the study was conducted during a state of emergency, a limited number of healthcare professionals were included.
Conclusions
Lessons learned from the current COVID-19 pandemic offer hospital preparedness and response with the goal of protecting the front-line healthcare workers. The majority of HCWs practice preventive measures of COVID-19, however it was shown that HCWs had a gap in practicing physical distancing, stay at homeing, and ventilating the room frequently. The finding showed that there are different perceived barriers which hinder preventive practices in the study setting, some of which were: overcrowding in the emergency room, lack of infection prevention and control materials, insufficient training in infection control measures, and no hand washing after examinations or contact with the patient. The government and healthcare institution should work in strengthening infection prevention practices by reducing the barriers. Attention should be given for the safety of healthcare professionals and the community at large. In addition, frequent supervision, monitoring, and communication are important.
Abbreviations
BSc, Bachelor of Science; COVID-19, coronavirus disease 19; ETB, Ethiopian Birr; HCWs, health-care workers; PPE, personal protective equipment; SD, standard deviation; SARS, severe acute respiratory syndrome; WHO, World Health Organization.
Data Sharing Statement
All relevant data are within the manuscript.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from Debre Tabor University, College of Health Sciences, and Institutional Health Research Ethics Review Committee (IHRERC). Information regarding the purpose of the study, voluntary nature of participation, and risk imposed due to involvement presented in the information section of the survey. Informed written consent was taken. Confidentiality of the information was maintained and the data were recorded anonymously throughout the study. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors acknowledged healthcare providers who participate in the study and data collectors.
Disclosure
The authors declare that they have no competing interests.
Additional information
Funding
References
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Geneva; 2020.
- World Health Organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March 2020. World Health Organization; 2020.
- Allegranzi B, Nejad SB, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–241. doi:10.1016/S0140-6736(10)61458-421146207
- Gailienė G, Gierasimovič Z, Petruševičienė D, et al. The prevalence of health care-associated infections and risk factors in a university hospital. Medicina. 2012;48(8):59. doi:10.3390/medicina48080059
- Gignon M, Schmit JL, Farcy S, et al. Prevention of healthcare-associated infections in general practice: current practice and drivers for change in a French study. Indian J Med Microbiol. 2012;30(1):69. doi:10.4103/0255-0857.9304022361764
- HCP HP. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. 2019.
- World Health Organization. Infection Prevention and Control Guidance for Long-Term Care Facilities in the Context of COVID-19: Interim Guidance, 21 March 2020. World Health Organization; 2020.
- Tian H, Liu Y, Li Y, et al. An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science. 2020;368(6491):638–642. doi:10.1126/science.abb610532234804
- McGarry BE, Grabowski DC, Barnett ML. Severe staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic: study examines staffing and personal protective equipment shortages faced by nursing homes during the COVID-19 pandemic. Health Aff. 2020;39(10):1812–1821. doi:10.1377/hlthaff.2020.01269
- Vilakati PN, Villa S, Alagna R, et al. The Neglected Role of Faith-Based Organizations in Prevention and Control of COVID-19 in Africa. Transactions of the Royal Society of Tropical Medicine and Hygiene; 2020.
- Houghton C, Meskell P, Delaney H, et al. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: a rapid qualitative evidence synthesis. Cochrane Database Syst Rev. 2020;(4).
- Ali S, Noreen S, Farooq I, et al. Risk assessment of healthcare workers at the frontline against COVID-19. PaK J Med Sci. 2020;36(COVID19–S4). doi:10.12669/pjms.36.COVID19-S4.2790.
- Huda MN, Islam R, Qureshi MO, et al. Rumour and social stigma as barriers to the prevention of coronavirus disease (COVID-19): what solutions to consider? Global Biosecur. 2020;1(4). doi:10.31646/gbio.78.
- Bruns DP, Kraguljac NV, Bruns TR. COVID-19: facts, cultural considerations, and risk of stigmatization. J Transcult Nurs. 2020;31(4):326. doi:10.1177/104365962091772432316872
- Sharifi F, Larki M, Latifnejad Roudsari R. COVID-19 outbreak as threat of violence against women. J Midwifery Women's Health. 2020;8(3):2376–2379.
- Hailu W, Derseh L, Hunegnaw MT, Tesfaye T, Abebaw D. Compliance, Barriers, and Facilitators to Social Distancing Measures for Prevention of COVID-19 in Northwest Ethiopia, 2020. 2020.
- Liu Q, Luo D, Haase JE, et al. The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob Health. 2020;8(6):e790–e798. doi:10.1016/S2214-109X(20)30204-732573443
- Xiang Y-T, Jin Y, Wang Y, et al. Tribute to health workers in China: a group of respectable population during the outbreak of the COVID-19. Int J Biol Sci. 2020;16(10):1739. doi:10.7150/ijbs.4513532226292
- Ran L, Chen X, Wang Y, et al. Risk factors of healthcare workers with corona virus disease 2019: a retrospective cohort study in a designated hospital of Wuhan in China. Clin Infect Dis. 2020. doi:10.1093/cid/ciaa287
- Wang J, Zhou M, Liu F. Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect. 2020;105(1):100–101. doi:10.1016/j.jhin.2020.03.00232147406
- Phan LT, Maita D, Mortiz DC, et al. Personal protective equipment doffing practices of healthcare workers. J Occup Environ Hyg. 2019;16(8):575–581. doi:10.1080/15459624.2019.162835031291152
- Schwartz J, King -C-C, Yen M-Y. Protecting healthcare workers during the coronavirus disease 2019 (COVID-19) outbreak: lessons from Taiwan’s severe acute respiratory syndrome response. Clin Infect Dis. 2020;71(15):858–860. doi:10.1093/cid/ciaa25532166318
- Otter JA, Yezli S, French GL. The Role of Contaminated Surfaces in the Transmission of Nosocomial Pathogens, in Use of Biocidal Surfaces for Reduction of Healthcare Acquired Infections. Springer; 2014:27–58.
- Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare professionals regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.00732437822
- Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S25873632612371
- Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48(1):1–11. doi:10.1186/s41182-020-00254-331920458
- Sahiledengle B, Gebresilassie A, Getahun T, et al. Infection prevention practices and associated factors among healthcare workers in governmental healthcare facilities in Addis Ababa. Ethiop J Health Sci. 2018;28(2):177–186. doi:10.4314/ejhs.v28i2.929983515
- Desta M, Ayenew T, Sitotaw N, et al. Knowledge, practice and associated factors of infection prevention among healthcare workers in Debre Markos referral hospital, Northwest Ethiopia. BMC Health Serv Res. 2018;18(1):465. doi:10.1186/s12913-018-3277-529914477
- Gebresilassie A, Kumei A, Yemane D. Standard precautions practice among health care workers in public health facilities of Mekelle special zone, Northern Ethiopia. J Community Med Health Educ. 2014;4(3):286.
- Dires A, Addis SG, Tesema YG. Perceived Efficacy of COVID-19 Prevention Measures and Intention to Use Among Chronic Disease Patients in Northeast Ethiopia, 2020. 2020.
- Boškoski I, Gallo C, Wallace MB, et al. COVID-19 pandemic and personal protective equipment shortage: protective efficacy comparing masks and scientific methods for respirator reuse. Gastrointest Endosc. 2020;92(3):519–523. doi:10.1016/j.gie.2020.04.04832353457
- Mahmood SU, Crimbly F, Khan S, Choudry E, Mehwish S. Strategies for rational use of personal protective equipment (PPE) among healthcare providers during the COVID-19 crisis. Cureus. 2020;12(5).
- Miethke-Morais A, Perondi B, Harima L, et al. Overcoming barriers to providing comprehensive inpatient care during the COVID-19 pandemic. Clinics. 2020;75.
- Ranney ML, Griffeth V, Jha AK. Critical supply shortages—the need for ventilators and personal protective equipment during the Covid-19 pandemic. N Engl J Med. 2020;382(18):e41. doi:10.1056/NEJMp200614132212516
- Puspitasari IM, Yusuf L, Sinuraya RK, et al. Knowledge, attitude, and practice during the COVID-19 pandemic: a review. J Multidiscip Healthc. 2020;13:727–733. doi:10.2147/JMDH.S26552732801735
- Macro O, Measure D. Ethiopia Demographic and Health Survey, 2011: Preliminary Report. Central Statistical Agency; 2011.
- Tolu LB, Ezeh A, Feyissa GT. How prepared is Africa for the COVID-19 pandemic response? The case of Ethiopia. Risk Manag Healthc Policy. 2020;13:771. doi:10.2147/RMHP.S25827332753990
- Maabreh R, Al-Doghaim R, Alhusban R, Bateha R, Awawdwh N. Knowledge, practices, and barriers towards COVID-19 infection prevention strategies among University Students in Northern Jordan. Int Med J. 2020;27(5).
- Zhou M, Tang F, Wang Y, et al. Knowledge, attitude and practice regarding COVID-19 among health care workers in Henan, China. J Hosp Infect. 2020.
- Anderson RM, Heesterbeek H, Klinkenberg D, et al. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet. 2020;395(10228):931–934. doi:10.1016/S0140-6736(20)30567-532164834
- Chinazzi M, Davis JT, Ajelli M, et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. 2020;368(6489):395–400. doi:10.1126/science.aba975732144116
- Chu DK, Akl EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. doi:10.1016/S0140-6736(20)31142-932497510
- Zhang J, Litvinova M, Liang Y, et al. Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science. 2020.
- Islam N, Sharp SJ, Chowell G, et al. Physical distancing interventions and incidence of coronavirus disease 2019: natural experiment in 149 countries. BMJ. 2020;370.
- Tesfaye ZT, Yismaw MB, Negash Z, et al. COVID-19-related knowledge, attitude and practice among hospital and community pharmacists in Addis Ababa, Ethiopia. Integr Pharm Res Pract. 2020;9:105. doi:10.2147/IPRP.S26127532904494
- Ayenew B, Pandey D. Challenges and opportunities to tackle COVID-19 spread in Ethiopia. J Peer Sci. 2020;2(2):e1000014.
- Huang L, Lin G, Tang L, Yu L, Zhou Z. Special Attention to Nurses’ Protection During the COVID-19 Epidemic. BioMed Central; 2020.
- Engdaw GT, Gebrehiwot M, Andualem Z. Hand hygiene compliance and associated factors among health care providers in Central Gondar zone public primary hospitals, Northwest Ethiopia. Antimicrob Resist Infect Control. 2019;8(1):190. doi:10.1186/s13756-019-0634-z31788237
- Abdella NM, Tefera MA, Eredie AE, et al. Hand hygiene compliance and associated factors among health care providers in Gondar University Hospital, Gondar, North West Ethiopia. BMC Public Health. 2014;14(1):96. doi:10.1186/1471-2458-14-9624479696
- Ataiyero Y, Dyson J, Graham M. Barriers to hand hygiene practices among health care workers in sub-Saharan African countries: a narrative review. Am J Infect Control. 2019;47(5):565–573. doi:10.1016/j.ajic.2018.09.01430470526