
Abstract
Purpose
Coronavirus disease 2019 (COVID-19) has evolved into a worldwide pandemic and continues to escalate exponentially in many countries across the globe. Recently, higher rates of psychological distress have been reported in several countries during the pandemic. Accordingly, the study aim was to investigate the relationship between public mental health and immune status during the COVID-19 pandemic.
Methods
Participants of this cross-sectional study were 2252 national and foreign residents of Saudi Arabia. We used a web-based self-rated questionnaire to measure the association between psychological distress (Depression, Anxiety and Stress Scales [DASS-21]) and immune status (Immune Status Questionnaire [ISQ]) during the COVID-19 pandemic. We also investigated predictors of reduced immune status using binary logistic regression analyses.
Results
Data from 1721 respondents showed that 17.5% of participants scored below the immune status cutoff (ISQ ˂ 6). Mean (± standard deviation) depression, anxiety, and stress scores in the reduced immune status group (ISQ ˂ 6) indicated moderate depression, anxiety, and stress (19.1 ± 11.4; 15.0 ± 9.6; 21.8 ± 11.2, respectively) and were significantly higher than scores in the normal immune status group (ISQ ≥ 6) (8.6 ± 9.1, P ˂ 0.0001; 5.0 ± 6.7, P ˂ 0.0001; 9.3 ± 9.3, P ˂ 0.0001, respectively). The regression analysis showed that age, anxiety, and stress were the only factors that significantly predicted the presence of reduced immune status.
Conclusion
There is an association between mental health problems during the COVID-19 pandemic and immune response in the public, especially in elderly people.
Introduction
The concept of a connection between the brain and peripheral organs (a body–mind network), particularly between the endocrine and immune system, can be traced back to antiquity. The new scientific research field of neuroimmunomodulation or psychoneuroimmunology is attracting increasing attention. There is evidence that neuroinflammation plays a crucial role in the pathophysiology of psychiatric disorders, including major depression, and in medical conditions often associated with mental illness, such as cardiovascular and autoimmune diseases, cancer, diabetes mellitus, and arthritis.Citation1 Major depression is typically associated with increased rates of morbidity, disability, and suicidal behaviors, and imposes a heavy socioeconomic burden on patients, caregivers, and society. For this reason, the World Health Organization has identified major depression as a leading cause of disability worldwide.
Depression is associated with chronic psychosocial stress.Citation2 Research has identified a wide range of stressors that disrupt the bidirectional network connection between the brain and immune system, causing neuropsychiatric and immunological disorders.Citation3 These stressors can be classified as physical stressors (eg burns, trauma, ischemia, infections, pregnancy, and postpartum) and psychological stressors (eg major life events or environmental events). The effect of stress on the immune system varies according to the nature, intensity, and duration of the stressor.Citation3 Moreover, age, sex, psychological status, and genetic factors may affect the immune system response to stress and depression.Citation2
Several clinical and experimental studies have reported strong associations between immune dysfunction (both cellular and humoral immunity), stress, and depression.Citation4 Chronic stress and depression are associated with increases in inflammatory biomarkers and cortisol levels, leading to changes in serotonergic neurotransmission that may induce mood disorders.Citation5,Citation6 One study found that the proinflammatory cytokine interleukin-6 (IL-6) is highly expressed in the blood of depressed patients.Citation7 A meta-analysis of 24 studies reported substantially higher levels of IL-6 and tumor-necrosis factor in patients with major depressive disorder.Citation8 These data suggest that immune dysfunction and an increase in inflammatory cytokines contribute to the pathophysiology of stress and depressive disorders.
The current coronavirus disease 2019 (COVID-19) pandemic has spread worldwide and has negatively affected mental health. Several recent studies have demonstrated high rates of psychological distress during the pandemic in populations from many countries. A study comparing public health before and during the COVID-19 pandemic found that participants reported an increase in negative emotions and a decrease in positive feelings and life satisfaction.Citation9 In a Chinese study, 58.3% of participants reported psychological distress following COVID-19-related imposed restrictions on social distancing and shutdowns.Citation10 A study of the Iranian population showed higher levels of psychological distress during the COVID-19 pandemic and identified several contributing predictors, including work status.Citation11 A Brazilian study found moderate mental health distress and identified age and workplace attendance as predictors of distress.Citation12 An Italian study also reported higher levels of psychological distress, and identified stressful situations, medical problems, and infected family members as predictors of distress.Citation13
Owing to COVID-19 curfews, quarantine, social distancing, shutdowns, and stay-at-home orders, many individuals have experienced profound psychological stress. Such stress may negatively affect the immune system, particularly in individuals experiencing greater psychological distress. There is evidence that patients with a pre-existing mental illness have a higher risk of severe clinical complications from COVID-19 than patients with no previous history of mental illness.Citation14 There are no public health studies investigating immune status (IS) and its relation to mental health during the COVID-19 pandemic. In this study, we investigated the effect of COVID-19-induced psychological distress (depression, anxiety, and stress) on IS in a sample of population in Saudi Arabia.
Methods
Design and Sample
This study was approved by the research ethics committee of King Abdulaziz University (approval no. 234–20) and conducted in accordance with the Declaration of Helsinki. All participants provided electronic informed consent before participation. We recruited a convenience sample of adult (>18 years old) citizens and residents of Saudi Arabia. Web-based digital data collection is an effective way to obtain insights into the physical and psychological well-being of individuals during pandemics. Therefore, given the travel restrictions and enforcement of social distancing, citizens and residents of Saudi Arabia were recruited via the Internet by distributing a study questionnaire on social media platforms (WhatsApp, Facebook, and Twitter) and institutional email services. Using the institutional account of one of the authors, the questionnaire was generated in Google Forms, a secure online data collection survey tool that allows participants to answer questions conveniently and anonymously. The questionnaire was distributed on May 6, 2020, after 1 month of a nationwide 24-hour curfew. Data collection continued for 1 week, at which point the target sample size was reached.
Inclusion/Exclusion Criteria
Responses collected from citizens and residents of Saudi Arabia older than 18 years were included in the study. We excluded data from participants who were younger than 18 years, had a confirmed diagnosis of COVID-19, had direct contact with COVID-19 patients, had a family history of COVID-19 infection, or had inconsistent questionnaire responses.
Measures
We constructed a simple, self-report questionnaire for this study. The survey was disseminated in both English and Arabic to facilitate the participation of individuals skilled in either language. Subjects were informed about how the collected data would be used and provided informed consent to participate in the study. The survey consisted of three sections. The first section contained questions about sociodemographic variables (age, education, marital status, employment status, income, nationality, and region of residence in Saudi Arabia).
The second section contained questions from the Depression, Anxiety and Stress Scales-21 (DASS-21).Citation15 The DASS-21 is a simple validated tool used to assess psychological distress in both clinical settings and the community.Citation16,Citation17 It consists of 21 questions, seven questions for each of the three targeted disorders (depression, anxiety, and stress), Supplementary file 1. Each subscale has cutoff values to categorize symptoms as mild, moderate, severe, or extremely severe. The total DASS-21 score indicates the presence/absence of substantial psychological distress. Previous studies have demonstrated the validity of the DASS-21 in screening for depression, anxiety, and stress with reasonable sensitivity and specificity compared with clinical psychiatric interviews.Citation18 The Arabic version of the DASS-21 has been used in previous published studies.Citation19 The DASS-21 was recently used in several studies in other countries to assess mental health in the context of the COVID-19 pandemic and has yielded meaningful results.Citation10
The third section of the questionnaire contained questions from the Immune Status Questionnaire (ISQ), Supplementary file 2. The ISQ is a simple, validated, and reliable (r = 0.796) tool that assesses perceived IS in the public.Citation20 It is a shorter form of the Immune Fitness Questionnaire. The ISQ is a self-rated questionnaire and consists of seven symptom items. Participants indicated on a 5-point Likert scale how often they had experienced these symptoms during April 2020 (during the complete curfew period in Saudi Arabia).Citation20 The total raw scores were then converted into a final scale score with a cutoff value of 6 (ISQ ˂ 6 indicates reduced IS).Citation20
Statistical Analysis
We used frequencies, percentages, means, and standard deviations as descriptive statistics. We categorized participants according to their ISQ score as showing reduced IS (ISQ < 6) or normal IS (ISQ ≥ 6). The chi-square test was used to explore the associations between sociodemographic variables and IS groups. We used Student’s t-test to explore the differences in means between IS groups. Additionally, we performed stepwise binary logistic regression analysis to independently examine sociodemographic and DASS-21 variables as predictors of IS. We calculated the odds ratios (OR) and 95% confidence intervals (CI) based on the probability of having an ISQ score of less than 6. We set the threshold for statistical significance at P < 0.05. We performed statistical analysis using SAS University Edition.
Results
We collected 2252 survey responses. We excluded 473 responses from healthcare workers to eliminate any chance of direct contact with infected patients. Another 58 responses were excluded because the participants were younger than 18 years or had a confirmed COVID-19 diagnosis, contact with COVID-19 patients, family history of COVID-19 cases, or inconsistent responses. We then analyzed data from the remaining 1721 respondents. shows the sociodemographic characteristics of all groups. Most participants were women (68.16%) and aged 28 years or younger (34.5%). Only 8.5% were 59 years or older. Almost 77% of the sample had a bachelor’s degree or higher. Almost 25% of our participants were unemployed. Most participants (62.81%) resided in the western region of Saudi Arabia. Only 9.2% were foreign nationals residing in Saudi Arabia.
Table 1 Sociodemographic Characteristics of the Study Sample
Dividing the participants into two groups according to ISQ score showed that 17.5% of participants had reduced IS (ISQ ˂ 6), with a mean and standard deviation of 3.3 ± 1.8, and 82.5% had normal IS (ISQ ≥ 6), with a mean and standard deviation of 9.2 ± 1.2. There were statistically significant differences between sociodemographic characteristics and IS groups (P < 0.05), except for citizenship and residential region ().
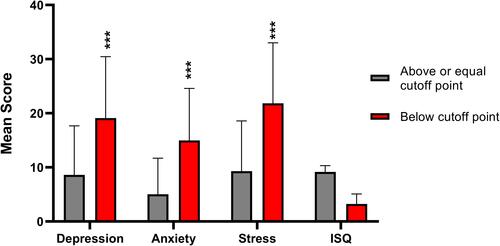
shows the proportion of different DASS-21 category scores and indicates that approximately one-third of participants experienced psychological distress in the form of depression, anxiety, or stress. IS was associated with severity of psychological distress in a dose–response pattern (). shows that the mean scores for depression, anxiety, and stress in the reduced IS group were in the range of moderate depression, anxiety, and stress (19.11 ± 11.35, 14.96 ± 9.64, and 21.82 ± 11.21, respectively). These DASS-21 scores were significantly higher than those for the normal IS group (8.6 ± 9.06, P ˂ 0.0001; 5.04 ± 6.66, P ˂ 0.0001; 9.29 ± 9.28, P ˂ 0.0001, respectively).
Figure 1 The proportion of participants in different score categories (normal, mild, moderate, severe, and extremely severe) for each psychological disorder for the whole sample (pie chart) and proportions in each immune status category (below or above cutoff point) for each DASS-21 subscale are shown in the column graph. (A) The proportion of participants in depression score categories. (B) Proportions in each immune status category for depression subscale. (C) The proportion of participants in anxiety score categories. (D) Proportions in each immune status category for anxiety subscale. (E) The proportion of participants in different stress score categories. (F) Proportions in each immune status category for stress subscale.
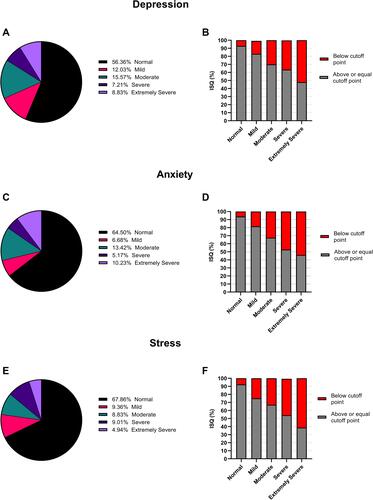
Figure 2 Mean scores for depression, anxiety, stress, and ISQ in two subpopulations. Data are mean ± standard deviations. Student’s t-test was used to compare the two subpopulations. ***P < 0.0001.
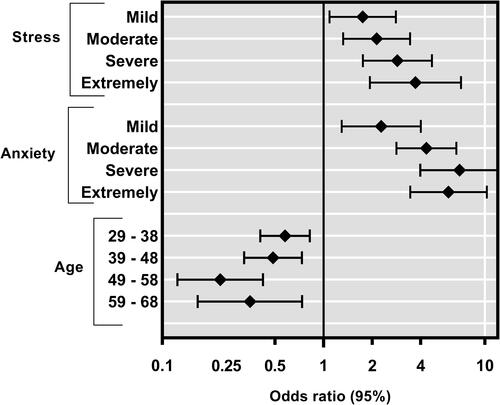
Using stepwise binary logistic regression analysis, we investigated the contributions of the different independent sociodemographic variables and DASS-21 subscales of interest to IS (). Age, anxiety, and stress were the only factors that significantly predicted the presence of reduced IS (ISQ ˂ 6) in the study sample. For instance, participants who reported mild to moderate anxiety were two to four times more likely to have reduced IS than those who did not report anxiety (OR = 2.3, 95% CI = 1.3–4.0 and OR = 4.3, 95% CI = 2.8–6.7, respectively). In addition, participants who reported mild to moderate stress were also more likely to have reduced IS than those who did not report stress (OR = 1.8, 95% CI = 1.1–2.8 and OR = 2.1, 95% CI = 1.3–3.4, respectively).
Figure 3 Forest plot of odds ratios and 95% confidence intervals. The plot represents the correlations between predictors and reduced immune status (ISQ score cutoff point). Each row represents a specific predictor with the corresponding odds ratio (dot) and 95% confidence intervals (horizontal line).
Discussion
The COVID-19 pandemic has caused profound psychological and emotional distress in many individuals worldwide. The results from this study show that approximately 33%–50% of subjects reported substantial levels of psychological distress, with approximately 5%–10% reporting the most severe symptoms. These data from participants in Saudi Arabia are in line with data collected from other countries during the COVID-19 pandemic.Citation21 However, the effects of psychological distress are not restricted to mental health, but can also affect somatic and physical health, as well as non-health-related factors. For example, psychological distress has a substantial negative effect on factors such as pain perception, incidence of arthritis, cardiovascular disease, chronic obstructive pulmonary disease, diabetes, and even mortality rate.Citation22,Citation23
Many studies support the hypothesis that there is a bidirectional relationship between the immune system and psychological states, in which psychological distress promotes immune dysfunction and inflammation worsens psychological distress. Several preclinical studies have reported that different types of stressors (eg social isolation, social defeat, unpredictable stress) can induce immune dysfunction in experimental rodents.Citation24–Citation26 There is also evidence of an increase in proinflammatory cytokine levels in psychologically distressed patientsCitation7,Citation27–Citation31 and animal models of depression.Citation32,Citation33 These results reflect our own findings, which showed that reduced IS (below the ISQ cutoff point) was positively correlated with the severity of psychological distress, with approximately 50% of participants in the most severe DASS-21 categories experiencing poor immune response. Moreover, we found that 17.5% of participants had reduced IS and scored below the immune cutoff point (ISQ ˂ 6) during the COVID-19 pandemic curfew. This is consistent with findings from a previous study indicating anegative correlation between ISQ scores and stress, anxiety, depression, and fatigue.Citation20 These findings may explain the higher risk of COVID-19 complications in patients with pre-existing mental illness compared with patients with no previous history of mental illness.Citation14
The stepwise analysis indicated a potential contribution of independent sociodemographic variables and DASS-21 subscale scores to IS. Age was one potential contributor to poor immune response. This is consistent with previous findings of an age-related decline in immune system function, which increases susceptibility to infections and reduces vaccine efficacy.Citation34 Moreover, we showed that anxiety and stress contributed to a decline in IS. This is in line with other studies showing that stress and anxiety can affect the immune system and therefore lead to greater vulnerability to infections and disease.Citation35
Previous study findings suggest factors that should be taken into consideration during pandemics to reduce the effect of psychological distress on the immune system. One meta-analysis showed that physical activity can protect from anxiety regardless of demographic factors.Citation36 The same study also reported that greater physical activity can confer protection against stress-induced disorders.Citation36 Moreover, another meta-analysis reported that yoga may be an effective intervention for individuals with elevated levels of anxiety.Citation37 Cognitive behavioral therapy is another effective way to reduce anxiety and psychological distress.Citation38 This evidence should guide health policymakers in different countries in generating strategies to overcome or minimize the severe negative effects of national psychological distress during pandemics. A good example is that during the complete curfew, the Saudi government allowed a 1-hour daily walk within a specific radius around the place of residence. There is an urgent need for the implementation of psychological or social interventions in different countries to lessen the negative effects of curfew, quarantine, and social distancing on stress, anxiety, and depression during pandemics.
This study has some limitations. First, owing to the cross-sectional nature of the study, the data cannot be used to infer causality. Second, we used a convenience sampling method. This may have resulted in selection bias if people with very low or very high anxiety levels refrained from participating in the study because they avoided accessing the news media through which the study tool was disseminated. Third, the study was sufficiently powered to detect major differences in psychological distress scores but may have not been sufficiently sensitive to detect small differences between specific subgroups (such as older adults, who constituted a relatively small proportion of our sample). Fourth, we did not investigate the medical history of participants and did not exclude any immune-compromised patients or patients with a history of stress-induced disorders. Fifth, we relied on the ISQ survey to predict IS and did not quantify levels of inflammatory biomarkers for each participant.
Conclusion
To our knowledge, the survey data presented here are the first to demonstrate a relationship between psychological distress and public IS during the COVID-19 pandemic in Saudi Arabia. We showed that the pandemic has resulted in a stressful psychological burden that may negatively affect the IS of the public. This study highlights the harmful effects of pandemic-induced psychological distress on the public. It also identifies an urgent need to implement psychological or social interventions to reduce the negative psychosocial effect of the pandemic on public mental health and to reverse the observed immune system dysfunction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
Additional information
Funding
References
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349(9063):1436–1442. doi:10.1016/S0140-6736(96)07495-8
- Leonard B. Stress, depression and the activation of the immune system. World J Biol Psychiatry. 2000;1(1):17–25. doi:10.3109/15622970009150562
- Reiche E, Morimoto H, Nunes S. Stress and depression-induced immune dysfunction: implications for the development and progression of cancer. Int Rev Psychiatry. 2006;17(6):515–527. doi:10.1080/02646830500382102
- Raison CL, Capuron L, Miller AH. Cytokines sing the blues: inflammation and the pathogenesis of depression. Trends Immunol. 2006;27(1):24–31. doi:10.1016/j.it.2005.11.006
- Maddock C, Pariante CM. How does stress affect you? An overview of stress, immunity, depression and disease. Epidemiol Psichiatr Soc. 2001;10(3):153–162. doi:10.1017/S1121189X00005285
- Tafet GE, Toister-Achituv M, Shinitzky M. Enhancement of serotonin uptake by cortisol: a possible link between stress and depression. Cogn Affect Behav Neurosci. 2001;1(1):96–104. doi:10.3758/CABN.1.1.96
- Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46–56. doi:10.1038/nrn2297
- Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67(5):446–457. doi:10.1016/j.biopsych.2009.09.033
- Li S, Wang Y, Xue J, Zhao N, Zhu T. The impact of COVID-19 epidemic declaration on psychological consequences: a study on active Weibo users. Int J Environ Res Public Health. 2020;17(6):2032. doi:10.3390/ijerph17062032
- Wang C, Pan R, Wan X, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020;87:40–48. doi:10.1016/j.bbi.2020.04.028
- Jahanshahi AA, Dinani MM, Madavani AN, Li J, Zhang SX. The distress of Iranian adults during the Covid-19 pandemic - More distressed than the Chinese and with different predictors. Brain Behav Immun. 2020;87:124–125. doi:10.1016/j.bbi.2020.04.081
- Zhang S, Wang Y, Afshar Jahanshahi A, Jia J, Schmitt V. First study on mental distress in Brazil during the COVID-19 crisis. Preprint. 2020.
- Mazza C, Ricci E, Biondi S, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020;17(9):3165. doi:10.3390/ijerph17093165
- Lee SW, Yang JM, Moon SY, et al. Association between mental illness and COVID-19 susceptibility and clinical outcomes in South Korea: a nationwide cohort study. Lancet Psychiatry. 2020;7(12):1025–1031. doi:10.1016/S2215-0366(20)30421-1
- Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(2):227–239. doi:10.1348/014466505X29657
- Lovibond PF. Long-term stability of depression, anxiety, and stress syndromes. J Abnorm Psychol. 1998;107(3):520–526. doi:10.1037/0021-843X.107.3.520
- Norton PJ. Depression Anxiety and Stress Scales (DASS-21): psychometric analysis across four racial groups. Anxiety Stress Coping. 2007;20(3):253–265. doi:10.1080/10615800701309279
- Tran TD, Tran T, Fisher J. Validation of the depression anxiety stress scales (DASS) 21 as a screening instrument for depression and anxiety in a rural community-based cohort of northern Vietnamese women. BMC Psychiatry. 2013;13(1):24. doi:10.1186/1471-244X-13-24
- Alzahrani A, Alghamdi A, Alqarni T, Alshareef R, Alzahrani A. Prevalence and predictors of depression, anxiety, and stress symptoms among patients with type II diabetes attending primary healthcare centers in the western region of Saudi Arabia: a cross-sectional study. Int J Ment Health Syst. 2019;13(1):48. doi:10.1186/s13033-019-0307-6
- Wilod Versprille LJF, van de Loo AJAE, Mackus M, et al. Development and validation of the Immune Status Questionnaire (ISQ). Int J Environ Res Public Health. 2019;16(23):4743. doi:10.3390/ijerph16234743
- Alghamdi BS, AlAtawi Y, AlShehri FS, et al. Psychological distress during COVID-19 curfews and social distancing in Saudi Arabia: a cross-sectional study. Res Sq. 2020. doi:10.21203/rs.3.rs-40296/v1
- Lingard EA, Riddle DL. Impact of psychological distress on pain and function following knee arthroplasty. JBJS. 2007;89(6):1161–1169. doi:10.2106/00004623-200706000-00002
- de Burgos-lunar C, Gómez-Campelo P, Cárdenas-Valladolid J, et al. Effect of depression on mortality and cardiovascular morbidity in type 2 diabetes mellitus after 3 years follow up. The DIADEMA study protocol. BMC Psychiatry. 2012;12(1):95. doi:10.1186/1471-244X-12-95
- Grippo AJ, Sullivan NR, Damjanoska KJ, et al. Chronic mild stress induces behavioral and physiological changes, and may alter serotonin 1A receptor function, in male and cycling female rats. Psychopharmacology. 2005;179(4):769–780. doi:10.1007/s00213-004-2103-4
- Audet MC, Jacobson-Pick S, Wann BP, Anisman H. Social defeat promotes specific cytokine variations within the prefrontal cortex upon subsequent aggressive or endotoxin challenges. Brain Behav Immun. 2011;25(6):1197–1205. doi:10.1016/j.bbi.2011.03.010
- Möller M, Du Preez JL, Viljoen FP, Berk M, Emsley R, Harvey BH. Social isolation rearing induces mitochondrial, immunological, neurochemical and behavioural deficits in rats, and is reversed by clozapine or N-acetyl cysteine. Brain Behav Immun. 2013;30:156–167. doi:10.1016/j.bbi.2012.12.011
- Tuglu C, Kara SH, Caliyurt O, Vardar E, Abay E. Increased serum tumor necrosis factor-alpha levels and treatment response in major depressive disorder. Psychopharmacology. 2003;170(4):429–433. doi:10.1007/s00213-003-1566-z
- Basterzi A, Aydemir C, Kisa C, et al. IL-6 levels decrease with SSRI treatment in patients with major depression. Hum Psychopharmacol. 2005;20(7):473–476. doi:10.1002/hup.717
- Tsao CW, Lin YS, Chen CC, Bai CH, Wu SR. Cytokines and serotonin transporter in patients with major depression. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(5):899–905. doi:10.1016/j.pnpbp.2006.01.029
- Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732–741. doi:10.1016/j.biopsych.2008.11.029
- Steptoe A, Willemsen G, Owen N, Flower L, Mohamed-Ali V. Acute mental stress elicits delayed increase in circulating inflammatory cytokine levels. Clin Sci. 2001;101:185–192.
- Elgarf AS, Aboul-Fotouh S, Abd-Alkhalek HA, et al. Lipopolysaccharide repeated challenge followed by chronic mild stress protocol introduces a combined model of depression in rats: reversibility by imipramine and pentoxifylline. Pharmacol Biochem Behav. 2014;126:152–162. doi:10.1016/j.pbb.2014.09.014
- Lu Y, Ho CS, Liu X, et al. Chronic administration of fluoxetine and pro-inflammatory cytokine change in a rat model of depression. PLoS One. 2017;12(10):e0186700. doi:10.1371/journal.pone.0186700
- Fuentes E, Fuentes M, Alarcón M, Palomo I. Immune system dysfunction in the elderly. An Acad Bras Cienc. 2017;89(1):285–299. doi:10.1590/0001-3765201720160487
- Segerstrom SC, Miller GE. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull. 2004;130(4):601–630. doi:10.1037/0033-2909.130.4.601
- Schuch FB, Stubbs B, Meyer J, et al. Physical activity protects from incident anxiety: a meta-analysis of prospective cohort studies. Depress Anxiety. 2019;36(9):846–858. doi:10.1002/da.22915
- Cramer H, Lauche R, Anheyer D, et al. Yoga for anxiety: a systematic review and meta-analysis of randomized controlled trials. Depress Anxiety. 2018;35(9):830–843. doi:10.1002/da.22762
- Carpenter JK, Andrews LA, Witcraft SM, Powers MB, Smits JAJ, Hofmann SG. Cognitive behavioral therapy for anxiety and related disorders: a meta-analysis of randomized placebo-controlled trials. Depress Anxiety. 2018;35(6):502–514. doi:10.1002/da.22728