
Abstract
Background
Community screening for SARS-CoV-2 Omicron variant plays a significant role in controlling the spread of infection. However, loopholes may exist in the current management of community screening in Shanghai, China. The objective of this study was to discover loopholes in the management of community screening for SARS-CoV-2 Omicron variant in Shanghai, China and provide targeted solutions.
Methods
The cross-sectional study was carried out April 4 to April 30, 2021, among residential committee directors from the Putuo District, Pudong District, and Minhang District of Shanghai, China. Data were collected using a self-designed questionnaire about the management of nucleic acid testing (NAT) sampling in communities through the network platform powered by www.wjx.cn.
Results
A total of 203 residential committee directors responded to the survey. Of them, 47.3% were not accepted training and 40.4% were not aware of cross-infection. Comparison among sampling sites and communities, high-risk group contained lower proportion of community training (P = 0.093~0.200), higher awareness of cross-infection (P = 0.039~0.777), more medical workers (P = 0.007~0.724) and more tests performed (P = 0.001~0.992). Larger communities had more medical workers, sampling sites, sampling tables (P = 0.000) and higher awareness of cross-infection (P = 0.009), but lower proportion of community training (P = 0.051).
Conclusion
Overall, community training and awareness of infection control were inadequate. Government or institutions should organize the community training and raise the awareness of infection control. Significant differences exist in NAT management patterns between sampling sites, as well as communities of different sizes. Residential community directors minimize high-risk sampling point settings in the future. Special personnel designated by the government or institutions should tour to guide each sampling site.
Introduction
COVID-19 is a disease caused by a novel coronavirus called severe acute respiratory syndrome coronavirus (SARS-CoV-2) that is liable for causing the global pandemic. On December 31, 2019, WHO first learned of this new virus from a group of viral pneumonia cases reported in Wuhan, China.Citation1 It was 26 November 2021 that WHO declared that the world was facing Omicron variant of concern.Citation2 Omicron has been identified as being significantly more transmissible, which altered the trajectory of the COVID-19 pandemic and replaced Delta as the dominant variant.Citation2
Confirmed transmission routes of COVID-19 are direct transmission, aerosol transmission and contact transmission.Citation3 The main clinical manifestations of COVID-19 are fever, malaise and dry cough. According to data released by WHO, there have been more than 600 million confirmed cases of COVID-19 and approximately 15 million direct and indirect deaths due to COVID-19 globally in 2020 and 2021, which is nearly three times the number of deaths reported by countries worldwide.Citation4,Citation5
COVID-19 pandemic particularly the variant strains has hugely impacted all aspects of life. The impact of this pandemic is so severe that it has shaken most countries’ s economies.Citation6,Citation7 Problems and difficulties were quite outstanding in areas such as employment, social security, income, education, medical service, housing and production safety.Citation8–10
Health professionals were discovering SARS-COV-2’s traits, whereas with the evolving understanding of the disease, initiatives and interventions also needed to be continuously evaluated and updated.Citation11 Hence, the Chinese government adopted a “Dynamic COVID-zero” strategy to control Omicron variant spreading for the safety of people’s lives and property, which includes early identifying infections, rapid containment and breaking the transmission chain through community screening.Citation12 From March 1 to April 26, 2022, a total of 535,600 local SARS-CoV-2 Omicron variant infections were reported in Shanghai, China. Community screening has proven effective in epidemic prevention and control in Shanghai’s fight against the SARS-CoV-2 Omicron variant.Citation13 However, the number of confirmed cases of the Omicron variant remained high for almost two months, indicating some possible loopholes in community screening. Therefore, this study aimed to analyze the weak links of the management of NAT sampling in communities in Shanghai, China, through a cross-sectional survey and provide targeted solutions for improving the efficacy of community screening in preventing and controlling SARS-CoV-2 Omicron variant infection.
Materials and Methods
Participants
Convenience sampling was used to conduct a cross-section study from April 4 to April 30, 2021, that included residential committee directors from the Putuo District, Pudong District, and Minhang District of Shanghai, China, who were invited to answer the questionnaire by telephone. They organized NAT sampling in their own community. The sample size is usually calculated based on 5–10 times of the number of independent variables.Citation14 Considering the loss of follow-up of 20%, the final confirmed sample size is 220.
Questionnaire About Community Screening with Nucleic Acid Testing
Respiratory physicians, infection-control physicians, and nurses designed the questionnaire used in this study. The questionnaire covered 20 items related to community screening management efforts during the SARS-CoV-2 Omicron variant pandemic and included questions about community NAT sampling, such as the number of community logistic staff members, sampling sites, sampling table spacing, sampling interval, site layout, and related training.
Procedures
The self-designed questionnaire was uploaded to the online platform powered by www.wjx.cn, a platform functionally equivalent to Amazon Mechanical Turk. Participants filled the questionnaire through a Chinese social media platform called WeChat. A fully completed questionnaire was regarded as valid. All questionnaire results were anonymous and confidential. This study was performed in accordance with the tenets of the Declaration of Helsinki and was approved by the ethics committee of The Second Hospital of Nanjing.
Data Analysis
Raw data were downloaded through www.wjx.cn and data analysis was carried out using the Chinese version of SPSS 22.0. A value of P < 0.05 was taken as statistically significant. Normally distributed measurement data were shown as the mean ± standard deviation, and non-normally distributed measurement data were shown as the median and interquartile range. Enumeration data were shown as the number (n) and percentage (%). The chi-square and rank sum tests were used to analyze the differences between different patterns of community screening.
Results
Sample Characteristics
A total of 220 questionnaires were distributed to 220 participants, and 203 valid questionnaires were finally collected from 203 participants (response rate: 92.27%). shows participant characteristics.
Table 1 Characteristics of 203 Residential Committee Directors
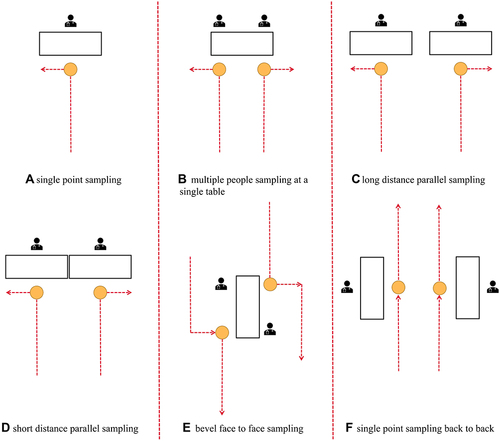
shows community management patterns during the SARS-CoV-2 Omicron variant pandemic identified from 203 participants. Most study participants had a bachelor’s degree, and 12.3% had a medical education background. To our surprise, 47.3% were not trained in NAT procedures, and 40.4% were not aware of cross-infection, which might be due to the suddenness of the SARS-CoV-2 Omicron variant outbreak. shows the common layouts of community NAT sites.
Table 2 Infection Prevention and Control Management Patterns During the SARS-CoV-2 Omicron Variant Pandemic: Results from 203 Valid Questionnaires
Figure 1 The common layouts of community NAT sites.
Comparison Among Sampling Sites
When comparing sampling sites, if multiple medical workers served at one sampling table, they were classified into the high-risk group; if one medical worker served at one sampling table, they were classified into the low-risk group. The number of tables at different sampling sites is displayed in . With more sampling tables in a single sampling site, more health care workers sampled (P = 0.000), it may mean more people lived here. The number of total sampling tables was significantly higher in cases of fewer sampling sites (P = 0.035). Restricted by the area of the community, the number of tables at each sampling site increased to strike a balance, as the number of sampling points was reduced.
Table 3 Comparison of Number of Tables per Sampling Site
The number of medical workers serving one table per sampling site is displayed in . Compared with the low-risk group, the high-risk group contained a significantly lower proportion of trained community logistic staff members (P = 0.093) and higher awareness of cross-infection (P = 0.159). These results may be due to sample size.
Table 4 Comparison of Low-Risk and High-Risk Groups in One-Table Sampling Sites
The medical workers classified according to the distance between two tables per sampling site are displayed in . The results showed that the high-risk group performed significantly more tests (P = 0.001) and contained significantly more medical workers (P = 0.007) than the low-risk group. Furthermore, compared with the low-risk group, the high-risk group had a lower proportion of trained community logistic staff members (P = 0.194) and a higher awareness of cross-infection (P = 0.777), although these were not statistically significant.
Table 5 Comparison of Low-Risk and High-Risk Groups in Sampling Sites with Two Tables Spaced 1.5m Apart
Comparison Among Communities
According to the distance between sampling tables, those serving at tables separated by ≥1.5 m were classified into the low-risk group, otherwise they were classified into the high-risk group.Citation15 Comparisons among communities of different sizes are displayed in . The results indicated that larger communities had significantly more medical workers, sampling sites, and sampling tables than smaller communities (P = 0.000). It was interesting that increasing community size was significantly associated with a smaller proportion of trained community members (P = 0.051) but a higher awareness of cross-infection (P = 0.009).
Table 6 Comparisons Among Communities of Different Sizes
In communities with a residential population <1000, the high-risk group showed a significantly higher awareness of cross-infection than the low-risk group (P = 0.039) ().
Table 7 Comparison of Low-Risk and High-Risk Groups in Communities with Less Than 1000 Residents
In communities with 1000–3000 residents, there were more medical workers in the high-risk group (P = 0.023) ().
Table 8 Comparison of Low-Risk and High-Risk Groups in Communities with 1000~3000 Residents
In communities with >3000 residents, there were significantly less sampling sites in the high-risk groups (P = 0.024) ().
Table 9 Comparison of Low-Risk and High-Risk Groups in Communities with More Than 3000 Residents
Discussion
As the government reported on April 26, 2022, the majority of COVID-19 cases in Shanghai were caused by the Omicron BA.2 and BA.2.2 variants. Early identification and isolation of infected patients are the key to controlling SARS-CoV-2 infection by the Omicron variant. NAT is the standard diagnostic criterion for the disease. On March 18, 2022, the Chinese government released the guidelines for organizing regional COVID-19 screening (the third edition).Citation13 From March 10 to April 17, 2022, Shanghai conducted 13 community screening rounds involving more than 200 million people.Citation16 By unswervingly adhering to the general policy of “Dynamic COVID-zero”, the number of new daily infections in Shanghai has continued to decline. The authors of the present study had accomplished 14 community screening rounds in Shanghai from April 4 to May 7, 2022. Through this study, we discovered loopholes in the community screening organization.
SARS-CoV-2 is most likely transmitted via droplets, aerosols, or direct person-to-person contact.Citation17,Citation18 How to properly wear and remove protective equipment, including hazmat suits and N95 masks, is critical for the prevention of cross-infection between medical workers or between patients and medical workers. N95 masks protect the wearer from droplets or aerosols that contain infectious agents.Citation19–21 Studies found that 27% of health workers who deviated from the training protocol and 79% of healthcare workers were contaminated in doffing personal protective equipment.Citation22,Citation23 The risk of contamination was closely related to inappropriate hand hygiene and mishandled or compromised personal protective equipment (especially exposed hands and wrists). In less experienced personnel, the incidence of contamination was even greater.Citation8
Community logistic staff are mainly responsible for on-site management of NAT sampling, such as setting warnings and guidance signs. The results of this survey showed that nearly half of the community logistic staff had received no professional training, particularly in big communities, and 40.4% had no awareness of cross-infection. The risk of infection increased in NAT sampling organized by community workers who lacked training. To solve this problem, training programs should be provided, including operation of personal protective equipment, disinfection, isolation, biosafety, sampling procedures and precautions, emergency treatment of occupational exposure, and early prevention in crowds.Citation4 Only after passing the training program can the community staff take their post.
A perfect allocation of medical workers should take full account of the number of residents in the community and the distribution of sampling sites. Communities should set up sampling sites according to the number of residents, the number of medical workers, and geographical transportation. The present study showed that in larger communities, the number of community logistic staff members, medical workers, sampling sites, and sampling tables were significantly greater than in smaller communities (P = 0.000). Sampling should be performed in open, well-ventilated and relatively independent sites, such as gymnasiums, exhibition halls, and school playgrounds. Outdoor sampling sites are encouraged when natural conditions permit. Each sampling site should be divided into a waiting area, sampling area, buffer zone, or others, to effectively disperse the residents. An area with hand hygiene facilities, full-length mirrors, and other protective devices for medical workers should be isolated from the sampling site. Each sampling site should provide clear guidelines concerning the one-way flow of personnel, sampling process, and other matters. In the present study, we observed risk of cross-infection at 19.78% of the sampling sites, due to <1.5 m distance between sampling tables and multiple medical workers at one table According to an expert consensus, the distance between sampling tables should be >1.5 m, and one person samples alone, or two people sample alternately at each sampling table.
This study had some limitations. As a cross-section study, the sample size was small, and the measurement data showed a skewed distribution, which may cause some bias in the results. All data in this study were obtained from community directors rather than volunteers, which may have affected the data. Furthermore, the study covered only three districts in Shanghai. Due to the lack of actual positive cases of infection in the community, no indexes were used to analyze the impact of NAT sampling management on positive infection in the community.
Conclusions
Overall, community training and awareness of infection control were inadequate. It is necessary for the government or institutions to organize the community training and raise the awareness of infection control. Significant differences exist in NAT management patterns between sampling sites, as well as communities of different sizes, such as the number of medical workers, awareness of cross-infection and the proportion of community training, etc. It indicates that residential community directors should organize NAT sampling according to the conditions of each community to minimize high-risk sampling point settings as much as possible in the future. Special personnel designated by the government or institutions should tour to guide each sampling site, standardize sampling operation, personal protection, cross infection prevention and control and other related work, and guide each sampling site to maintain on-site order.
Abbreviations
COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Data Sharing Statement
Authors can provide the data of this study upon reasonable request.
Ethics Approval and Consent to Participate
The study had been performed in accordance with the principles stated in the Declaration of Helsinki and approved by the Medical Ethics Committee of The Second Hospital of Nanjing (2021-LS-ky030). All participants were briefed on the purpose of the study, provided written informed consent for the questionnaire survey before the study started and had the right to stop or discontinue from the study at any time. This study will not disclose participants' personal identity and treated gathered information confidentially.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- World Health Organization. Pneumonia of unknown cause-China. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON229. Accessed January 5, 2020.
- World Health Organization. One year since the emergence of COVID-19 virus variant omicron. Available from: https://www.who.int/news-room/feature-stories/detail/one-year-since-The-emergence-of-omicron. Accessed November 25, 2022.
- Jiang JK, Vincent Fu Y, Liu L, Kulmala M. Transmission via aerosols: plausible differences among emerging coronaviruses. Aerosol Sci Technol. 2020;54(8):865–868. doi:10.1080/02786826.2020.1769020
- World Health Organization. Coronavirus disease (COVID-19) pandemic. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed December 5, 2022.
- World Health Organization. Global excess deaths associated with COVID-19 (modelled estimates). Available from: https://www.who.int/data/sets/global-excess-deaths-associated-with-covid-19-modelled-estimates. Accessed May 5, 2022.
- World Economic Forum. Global gender gap report 2021. Available from: https://www.weforum.org/reports/global-gender-gap-report-2021. Accessed March 30, 2021.
- Power K. The COVID-19 pandemic has increased the care burden of women and families. Sustainability. 2020;16:67–73. doi:10.1080/15487733.2020.1776561
- Pinchoff J, Austrian K, Rajshekhar N, et al. Gendered economic, social and health effects of the COVID-19 pandemic and mitigation policies in Kenya: evidence from a prospective cohort survey in Nairobi informal settlements. BMJ Open. 2021;11(3):e042749. doi:10.1136/bmjopen-2020-042749
- Burzynska K, Contreras G. Gendered effects of school closures during the COVID-19 pandemic. Lancet. 2020;395(10242):1968. doi:10.1016/S0140-6736(20)31377-5
- UN Women. The COVID-19 pandemic has increased the care burden, but by how much? Available from: https://data.unwomen.org/features/covid-19-pandemic-has-increased-care-burden-how-much-0. Accessed December 2, 2021.
- The state council information office, P.R.C. press conference held on situation regarding strict prevention and control of COVID-19 epidemic. Available from: http://www.gov.cn/xinwen/gwylflkjz193/index.htm. Accessed April 30, 2022.
- Liu J, Liu M, Liang W. The dynamic COVID-zero strategy in China. China CDC Wkly. 2022;4:74–75. doi:10.46234/ccdcw2022.015
- Joint prevention and control mechanism of the state council. Notice on the publication of guidelines for the implementation of regional novel coronavirus nucleic acid testing organizations (third edition). Available from: http://www.nhc.gov.cn/xcs/zhengcwj/202203/b5aaa96dfe1b4f14b19bf2f888a10673.shtml. Accessed April 30, 2022.
- Ni P, Chen JL, Liu N. Sample size estimation for quantitative studies in nursing research. Chin J Nurs. 2010;45(4):378–380. doi:10.3761/j.issn.0254-1769.2010.04.037
- Liu YL, Jin Y, Chen Q, et al. Expert consensus on hospital participation in population-wide specimen collection for COVID-19 testing. J Nurs Sci. 2022;37(5):1–5. doi:10.3870/j.issn.1001-4152.2022.05.001
- Shanghai has completed 13 rounds of nucleic acid tests for more than 200 million people. Available from: https://m.gmw.cn/baijia/2022-04/17/1302904384.html. Accessed April 30, 2022.
- Sharma A, Ahmad Farouk I, Lal SK. COVID-19: a review on the novel coronavirus disease evolution, transmission, detection, control and prevention. Viruses. 2021;13(2):202. doi:10.3390/v13020202
- Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis, and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96:753–758. doi:10.1136/postgradmedj-2020-138234
- Ruskin KJ, Ruskin AC, Musselman BT, et al. COVID-19, personal protective equipment, and human performance. Anesthesiology. 2021;134:518–525. doi:10.1097/ALN.0000000000003684
- Centers for Disease Control and Prevention. CDC calls on Americans to wear masks to prevent COVID-19 spread. Available from: https://www.cdc.gov/media/releases/2020/p0714-americans-to-wear-masks.html. Accessed April 30, 2022.
- World Health Organization. Coronavirus disease (COVID-19) advice for the public: when and how to use masks. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks. Accessed April 30, 2022.
- Kwon JH, Burnham CD, Reske KA, et al. Assessment of healthcare worker protocol deviations and self-contamination during personal protective equipment donning and doffing. Infect Control Hosp Epidemiol. 2017;38(9):1077–1083. doi:10.1017/ice.2017.121
- Kang J, Kim EJ, Choi JH, et al. Difficulties in using personal protective equipment: training experiences with the 2015 outbreak of middle east respiratory syndrome in Korea. Am J Infect Control. 2018;46(2):235–237. doi:10.1016/j.ajic.2017.08.04