
Abstract
Pediatric sepsis is a leading cause of morbidity and mortality in children globally. Children who require the pediatric intensive care unit (PICU) are at high risk for new or worsening co-morbidities, as well as readmission. This review describes the current state of protocolized follow-up after pediatric sepsis requiring PICU admission. We searched Medline and EMBASE databases for studies published in English from 2005 to date. Duplicates, review articles, abstracts and poster presentations were excluded; neonatal intensive care unit (NICU) patients were also excluded since neonatal sepsis is variably defined and differs from the pediatric consensus definition. The search yielded 418 studies of which 55 were duplicates; the subsequent 363 studies were screened for inclusion criteria, yielding 31 studies for which full article screening was completed. Subsequently, 23 studies were excluded due to wrong population (9), wrong publication type (10), duplicate data (3) or wrong outcome (1). In total, nine studies were included for which we described study design, setting, population, sample size, outcomes, PICU core outcome domain, and results. There were 4 retrospective cohort studies, 4 prospective cohort studies, 1 retrospective case series and no prospective trials. These studies show the varying trajectories of recovery after discharge, with the common finding that new or worsening morbidities are worse within months of discharge, but may persist. Sepsis survivors may have distinct needs and a different post-PICU trajectory compared to other critically ill children, particularly in quality of life and neurocognitive outcomes. Future research should focus on developing screening protocols and studying protocolized follow-up trials to reduce morbidity after pediatric sepsis.
Keywords:
Introduction
Pediatric sepsis is a leading cause of morbidity and mortality in children globally.Citation1–4 Pediatric sepsis, as defined by the 2005 International Pediatric Sepsis Consensus Conference (IPSCC), is systemic inflammatory response syndrome (SIRS) in the presence of infection.Citation5 Though sepsis mortality has decreased over the past decade, due in part to improvements in early recognition and timely initial management, it is estimated that mortality is still 10–20% for severe sepsisCitation1,Citation6 and that over one-third of children that die in pediatric intensive care units (PICUs) have sepsis.Citation6 Of those that survive, children with sepsis are at high risk of readmissionCitation7,Citation8 as well as new or worsening cognitive, physical and psychosocial deficits.Citation9
The presence of new comorbidities after pediatric sepsis raises the question of whether protocolized screening and follow-up should exist for these patients and, if so, how to structure this follow-up to optimally identify and manage new medical conditions and decrease readmissions. In adults, there exists a framework for screening patients after sepsis, including evaluation for new functional disability, swallowing impairment, or mental health concern, along with reviewing medications and screening for common, preventable causes of medical deterioration.Citation10 Within adult sepsis, observational data suggests referral to rehabilitation within 90 days of discharge is associated with lower 10-year mortality (compared to propensity matched controls).Citation11 Additionally, there have been multiple trials of post-discharge rehabilitation interventions for survivors after critical illness in general, with some benefit.Citation10 One trial, in which patients were randomized to bundled primary care intervention versus usual care, patients receiving the intervention demonstrated improvement in 5 out of 64 functional outcomes.Citation12 Another trial, in which patients were randomized patients to usual care or nurse navigator program after discharge, showed that patients receiving the intervention had lower rate of either mortality or re-hospitalization within 30 days of dischargeCitation13 and 1 year of discharge.Citation14
Pediatric patients similarly have shown new or worsening functional outcomes after sepsis requiring intensive care.Citation9 However, much of post-ICU follow-up in children has focused on post-intensive care syndrome in children (PICS-p) among the general PICU population.Citation15 PICS-p describes the physical, emotional, cognitive and social domains of health which may be affected after critical illness. Multidisciplinary post-PICU follow-up has been shown to decrease psychiatric morbidity.Citation16 Additional research is needed to identify the highest risk patients and effectiveness of interventions.Citation17 While PICS-p may account for some of the new or worsening functional status after pediatric sepsis, comparisons of PICU sepsis vs non-sepsis patients demonstrated increased odds of new respiratory failure, nutritional dependence, and chronic kidney disease after sepsis.Citation9 Moreover, there is physiologic plausibility for worsened neurocognitive outcomes in sepsis due to neuroinflammation, increased blood-brain-barrier permeability, delirium, and abnormal cerebral perfusion.Citation18 Given the particular vulnerability of pediatric sepsis patients, the aim of this review is to describe the current state of protocolized follow-up after pediatric sepsis requiring ICU admission.
Materials and Methods
We searched MEDLINE and Embase for full-text articles published in English from 2005 to February 3, 2023. We intentionally selected articles published from 2005 onwards not only to focus on current literature, but also to select studies which reflect the 2005 IPSCC consensus definition of pediatric sepsis.Citation5 We used the search terms “pediatric”, “child*”, “adolescent*” AND “sepsis” AND “critical care”, “intensive care” AND “follow-up” “post-intensive” “survivor” found in titles or abstracts.
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)Citation19 to report the study search, screening, and selection process. We used the following search phrases in Medline and EMBASE databases:
Medline search phrase:
(((pediatric OR child OR adolescent[Title/Abstract]) AND (sepsis[Title/Abstract]) AND (intensive care OR critical care [Title/Abstract])) AND (post-intensive OR follow-up OR survivor[Title/Abstract]))
EMBASE search phrase:
(pediatric:ab OR child:ab OR adolescent:ab) AND sepsis:ab AND ((‘pediatric’/exp OR pediatric) AND intensive AND (‘care’/exp OR care) OR critical) AND (‘care’/exp OR care) AND ((‘post intensive’:ab OR follow:ab) AND up:ab OR survivor:ab)
The studies identified in these databases were then assessed for duplicates, which were removed. The remaining studies were screened by two authors for inclusion (ARR and JCF); items flagged for inclusion by either reviewer then underwent full article screening. All authors participated in full article screening and discussion of final studies to include. We excluded review articles, abstracts, poster presentations and articles published in languages other than English. We excluded neonatal intensive care unit (NICU) patients since neonatal sepsis is variably defined and differs from the pediatric consensus definition.Citation20 We also excluded secondary analyses of studies that were already included, in order to avoid duplicating data. Citations included in key publications were manually reviewed to supplement literature search. Articles were assessed for quality, design, size, and incorporation of post-ICU follow-up for pediatric sepsis patients. Studies were evaluated for risk of bias based on Quality in Prognosis Studies (QUIPS) criteria.Citation21 We described the study design, setting, population, sample size, outcomes, and results of the final studies. We additionally specified the core outcome domain of each study, to align with efforts in the PICU community to define a core set of outcomes.Citation22 Given the variability of follow-up intervals, we additionally mapped the findings of the included studies by follow-up interval (in relation to hospital discharge), to better visualize the time-course of new or worsening co-morbidities.
Results
Overview
Our search yielded 418 studies (Medline 167, EMBASE 251), of which 55 were duplicates (). The subsequent 363 studies were screened for inclusion criteria, yielding 31 studies for which full article screening was completed. Subsequently, 23 studies were excluded due to wrong population (9), wrong publication type (10), duplicate data (3) or wrong outcome (1). Citations included in key publications were manually reviewed to supplement literature search, yielding one additional study. In total, nine studies were included in the final version of this review, for which we describe study design, setting, population, sample size, outcomes, PICU core outcome domain, and results (). There were 4 retrospective cohort studies, 4 prospective cohort studies, 1 retrospective case series and no prospective trials. Six studies were single center and three were multicenter, with inclusion of data from 18 countries. The sample size ranged from 45 to 5150 patients. Regarding outcome measures, seven studies used formal assessments such as intelligence quotient (IQ) testing, Pediatric Quality of Life Inventory, Pediatric Overall Performance Category (POPC) scale, Pediatric Cerebral Performance Category (PCPC) scale, and Functional Status Scale (FSS). Two studies used institution- or study-specific measures of new or worsening functional status. Time to follow-up ranged from hospital discharge to fourteen years post-discharge (). We further categorized the outcomes by PICU core outcome domains of cognitive function (3), emotional function (0), physical function (1) and overall health (6). Only one study described a protocol for clinical follow-up after sepsis in the PICU.Citation23
Figure 1 PRISMA flow diagram of study identification, screening and selection.
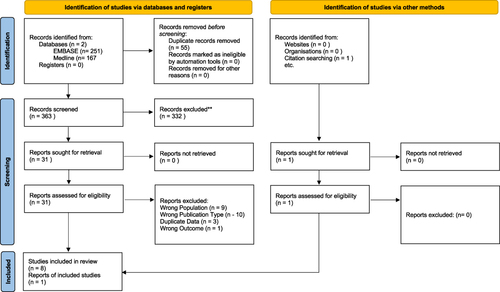
Figure 2 Follow-up intervals & outcomes of included studies.
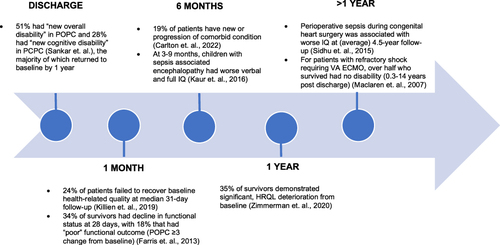
Table 1 Studies Describing Follow-Up After Pediatric Sepsis Requiring Intensive Care
Single Center Studies
The single center studies in this review included populations in the United States, Australia, Canada, and India. The oldest included studyCitation25 was a retrospective case series, over nearly two decades, of children in Australia with refractory septic shock which required venoarterial extracorporeal membrane oxygenation (VA ECMO). The range of follow up was also the largest of included studies (0.3–14 years). Of 45 patients, approximately half (24) died, 13 had no disability, 5 had mild disability, and 3 had moderate disability based on POPC at time of follow up.
Sidhu et alCitation27 specifically investigated infants with congenital heart disease who developed perioperative sepsis. The study included 502 infants in Western Canada who were less than 6 weeks of age and underwent cardiopulmonary bypass for congenital heart disease, 97 of whom developed perioperative sepsis. Using multivariable regression, the study found that perioperative sepsis was associated with adverse neurocognitive outcomes, as measured on full-scale, performance, and verbal IQ (using Wechsler Preschool and Primary Scale of Intelligence) 4.5 years after surgery.
There were two prospective cohort studies in India, one of which investigated POPC and PCPC up to 1 year after sepsis requiring intensive careCitation31 and another which looked specifically at children with sepsis-associated encephalopathy.Citation28 The former found that 51% had “new overall disability” (≥1 change from baseline) in POPC and 28% had “new cognitive disability” in PCPC at discharge, which decreased at 3 months and 1 year. At 1 year, only 5% had residual disability using POPC and 14% using PCPC. The latter studyCitation28 compared 50 cases of children with sepsis associated encephalopathy (defined as Glasgow Coma Scale <13 in the absence of seizures or abnormal lumbar puncture) to healthy age-matched controls. Using Malin’s Intelligence Scale for Indian Children (inclusive of full IQ, verbal IQ and performance IQ), the investigators found that children with sepsis-associated encephalopathy had significantly worse mean verbal IQ and full IQ scores at 3–9 months post discharge.
In the United States, a single center study of children with sepsis (both inpatient and in the PICU) showed that 24% of patients failed to recover baseline health-related quality at median follow-up of 1 month.Citation29 ICU admission was associated with failure to recover baseline health-related quality, with 38.5% of ICU patients failing to recover as compared to 21.9% of those without an ICU stay.
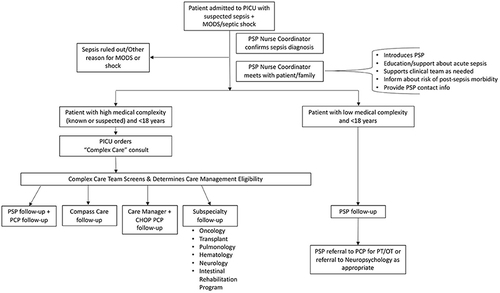
Lastly, Fitzgerald et alCitation23 published a prospective analysis of protocolized follow up of retrospectively identified sepsis patients in a quaternary PICU in the US. The study identified 80 children with sepsis requiring PICU care and outlined a workflow for structured follow-up (), stratified by medical complexity, in order to identify and treat new co-morbidities. Of the 80 patients, 20 were referred to care coordination, 13 had subspecialty follow-up; 20 had follow-up with the institutional Pediatric Sepsis Program (remainder were inpatient, followed elsewhere, lost to follow-up, or died).
Figure 3 Screening and Follow-up for PICU Sepsis Survivors.
Multi-Center Studies
There were three large, multicenter studies which investigated functional outcomes in pediatric sepsis patients. The earliest multi-center study included in this reviewCitation32 was a sub-analysis of 363 patients enrolled in RESOLVE: REsearching severe Sepsis and Organ dysfunction in children: a gLobal perspectiVE. The study included children from 104 pediatric centers in 18 countries from 2002 to 2005. Using decline in POPC (≥3 change from baseline), the study found 34% of survivors had decline in functional status at 28 days. In 2020, Zimmerman et alCitation30 prospectively assessed health related quality of life (HRQL) using Pediatric Quality of Life Inventory (PedsQL) or Functional Status Scale (FSS) after community acquired septic shock. The study included 389 children from 12 academic PICUs in the United States from 2013 to 2017. The investigators found that at 1-, 3-, 6-, and 12-months post-discharge, 50%, 37%, 30%, and 35% (respectively) of children had not returned to baseline. Finally, Carlton et alCitation9 completed a retrospective comparison of PICU sepsis patients to non-sepsis PICU patients in the US using a national administrative claims database. They compared 5150 sepsis survivors to 96,361 non-sepsis survivors and found 19% reported development and/or progression of a co-morbid condition (defined as one of the following: chronic respiratory failure, seizure disorder, supplemental nutritional dependence, and chronic kidney disease) within 6 months of discharge.
Discussion
These nine studies describe structured follow-up after pediatric sepsis requiring intensive care, in order to identify new or worsening medical conditions. The majority of these studies illustrate the persistence of functional decline in a proportion of survivors up to weeks, months, or years after discharge despite improvements with time. This is in keeping with prior assessments of the burden of sepsis-related morbidity; however, it appears the true trajectory after sepsis is quite variable. Based on the largest multicenter study evaluating health-related quality of life (HRQL) after sepsis, three-month follow was proposed as the optimal time since decline of HRQL peaked at 1 month, decreased by 3 months and then persisted to one year.Citation30 Similar trends were observed by Sankar et alCitation31 at three months, however at one year the majority of patients had returned to baseline, compared with nearly one-third of patients in the multicenter study who had deterioration of HRQL from baseline at 1 year.Citation30 The trajectory observed in critically ill children is also variable, but seems to peak a few months after discharge and improve after one year.Citation33,Citation34 We mapped the follow-up interval and findings from the included studies to show persistence of deficits at all time points (). Although there were deficits noted at >1 year, these two studies were in congenital heart disease patientsCitation27 and children requiring VA ECMO,Citation25 populations which have additional risk factors. A limitation of these all these studies is that some of the sickest patients may die during the follow-up period or be lost to follow-up. Moreover, we know that many patients with sepsis are readmitted, thus incurring additional risk of functional decline. A recent single center study found that approximately 33% of patients hospitalized with sepsis were readmitted within 90 days.Citation7 Of those, almost half (45%) were readmitted with an infectious diagnosis (namely respiratory infection or sepsis). The high rate of readmission with an infectious etiology prompts the question of whether these children should undergo workup for primary immunodeficiency, which puts them at risk for repeat infection. While there are not specific guidelines for immunology/immunodeficiency workup, this is an area of active investigationCitation35 and warrants additional study.
Not surprisingly, most of the studies used outcomes which correspond to the PICU core outcome domain of overall health (ie health-related quality of life). Cognitive outcomes were the second most common core outcome domain, which may be related to the unique pathophysiology of sepsis including neuroinflammation, permeability of blood–brain barrier and abnormal cerebral perfusion.Citation18 Additionally, the management of shock includes decreasing metabolic demand, often with intubation and sedation, which can increase risk for delirium.Citation36 Sepsis-associated encephalopathy is well characterized in adults,Citation37 with emerging pediatric data. Thus far there are no specific diagnostic criteria for sepsis associated encephalopathy in children, however there are studies demonstrating biomarker, EEG, and imaging abnormalities in pediatric sepsis patients.Citation38–40 Given this, it appears that neurocognitive outcomes may require special attention, distinct from general “overall health” metrics. The relative under-representation of emotional or physical core outcomes, while somewhat captured in the “overall health” domain, may represent additional areas for further research.
There was only one study which described prospective screening and protocolized follow-up of sepsis survivors,Citation23 which aimed to coordinate post-discharge follow-up based on medical complexity (). Patients with high medical complexity underwent “Complex Care” team consultation to determine whether they should follow-up with primary care, subspecialists, or a clinic devoted to high medical complexity patients (Compass Care). The remaining low complexity children were followed up by the Pediatric Sepsis Program (PSP), which used a telephone assessment 2–3 months after discharge to screen for new morbidity. The assessment was institution-specific with input from PICU providers, Physical Medicine & Rehabilitation physicians, physical, occupational, and speech therapists, a hospital-school liaison, a family advocate, a neuropsychologist, and program coordinators. Domains assessed included feeding, school participation and performance, social functioning, communication, attention, endurance, developmental milestones, emotions, and pain. Patients with a positive screen were referred to the appropriate therapy. This was a small pilot study so outcomes were not compared to usual care, however this would be an important next step.
This review has several limitations including a small number of studies and only one structured screening/follow-up protocol for pediatric sepsis survivors. We intentionally excluded neonatal studies given the differences in sepsis diagnosis and management, but there is opportunity to learn from implementation of screening and follow-up in this high-risk group. The establishment of NICU follow-up clinics to support families after dischargeCitation41 is much more prevalent compared to emerging PICU follow-up clinics.Citation42 Utilization of PICU follow-up clinics is one potential mechanism that may reduce morbidity after sepsis. Clinical trials are needed to determine the optimal type and timing of follow-up as well as to compare outcomes with protocolized follow-up to usual care.
Another limitation is that the constructs of post-intensive care syndrome (PICS-p) and the PICU core outcomes are relatively new and understudied. We intentionally used these constructs to align with our field and to help frame the elements of post-sepsis follow-up. However, sepsis may differ from general critical illness and sepsis-specific outcomes may be needed. While we intentionally excluded screening/protocols for general post-PICU follow-up, this may be starting point for intervention, while acknowledging that sepsis survivors may have distinct needs and a different post-PICU trajectory. The included studies clearly show the increased risk of sepsis patients for worse neurocognitive and overall health, which should be key outcomes considered in future development of screening and follow-up.
Conclusion
This review synthesizes the current state of post-sepsis outcomes, reflecting the need to focus on preventing and reducing sepsis morbidity. The included studies show the varying trajectories of recovery after discharge, with the common finding that new or worsening morbidities are worse within months of discharge, but may persist. Sepsis survivors may have distinct needs and a different post-PICU trajectory compared to other critically ill children, particularly in quality of life and neurocognitive outcomes. Future research should focus on developing screening protocols and studying protocolized follow-up trials to reduce morbidity after pediatric sepsis.
Abbreviations
IPSCC, International Pediatric Sepsis Consensus Conference; IQ, intelligence quotient; FSS, Functional Status Scale; GCS, Glasgow Coma Scale; NICU, neonatal intensive care unit; QUIPS, Quality in Prognosis Studies; PCPC, Pediatric Cerebral Performance Category; PICs-p, Post-Intensive Care Syndrome in children; PICU, Pediatric Intensive Care Unit; POPC, Pediatric Overall Performance Category; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis; SIRS, systemic inflammatory response syndrome; VA ECMO, venoarterial extracorporeal membrane oxygenation.
Disclosure
Julie C Fitzgerald reports grants from NIH, during the conduct of the study. The authors report no other conflicts of interest in this work.
Additional information
Funding
References
- Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. 2018;6(3):223–230. doi:10.1016/s2213-2600(18)30063-8
- Schlapbach LJ. Paediatric sepsis. Curr Opin Infect Dis. 2019;32(5):497–504. doi:10.1097/QCO.0000000000000583
- Weiss SL, Fitzgerald JC, Pappachan J, et al. Global epidemiology of pediatric severe sepsis: the Sepsis Prevalence, Outcomes, and Therapies Study. Am J Respir Crit Care Med. 2015;191(10):1147–1157. doi:10.1164/rccm.201412-2323OC
- Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–211. doi:10.1016/s0140-6736(19)32989-7
- Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi:10.1097/01.PCC.0000149131.72248.E6
- Ruth A, McCracken CE, Fortenberry JD, Hall M, Simon HK, Hebbar KB. Pediatric severe sepsis: current trends and outcomes from the pediatric health information systems database. Pediatr Crit Care Med. 2014;15(9):828–838. doi:10.1097/pcc.0000000000000254
- Dashefsky HS, Liu H, Hayes K, et al. Frequency of and risk factors associated with hospital readmission after sepsis. Pediatrics. 2023;152(1). doi:10.1542/peds.2022-060819
- Maddux AB, Zimmerman JJ, Banks RK, et al. Health resource use in survivors of pediatric septic shock in the United States. Pediatr Crit Care Med. 2022;23(6):e277–e288. doi:10.1097/PCC.0000000000002932
- Carlton EF, Gebremariam A, Maddux AB, et al. New and progressive medical conditions after pediatric sepsis hospitalization requiring critical care. JAMA Pediatr. 2022;176(11):e223554. doi:10.1001/jamapediatrics.2022.3554
- Prescott HC, Angus DC. Enhancing recovery from sepsis: a review. JAMA. 2018;319(1):62–75. doi:10.1001/jama.2017.17687
- Chao PW, Shih C-J, Lee Y-J, et al. Association of postdischarge rehabilitation with mortality in intensive care unit survivors of sepsis. Am J Respir Crit Care Med. 2014;190(9):1003–1011. doi:10.1164/rccm.201406-1170OC
- Schmidt K, Worrack S, Von Korff M, et al. Effect of a primary care management intervention on mental health–related quality of life among survivors of sepsis: a randomized clinical trial. JAMA. 2016;315(24):2703–2711. doi:10.1001/jama.2016.7207
- Taylor SP, Murphy S, Rios A, et al. Effect of a multicomponent sepsis transition and recovery program on mortality and readmissions after sepsis: the improving morbidity during post-acute care transitions for sepsis randomized clinical trial*. Crit Care Med. 2022;50(3):469–479. doi:10.1097/CCM.0000000000005300
- Kowalkowski MA, Rios A, McSweeney J, et al. Effect of a transitional care intervention on rehospitalization and mortality after sepsis: a 12-month follow-up of a randomized clinical trial. Am J Respir Crit Care Med. 2022;206(6):783–786. doi:10.1164/rccm.202203-0590LE
- Manning JC, Pinto NP, Rennick JE, Colville G, Curley MAQ. Conceptualizing post intensive care syndrome in children-the PICS-p framework. Pediatr Crit Care Med. 2018;19(4):298–300. doi:10.1097/pcc.0000000000001476
- Baker SC, Gledhill JA. Systematic review of interventions to reduce psychiatric morbidity in parents and children after PICU admissions*. Pediatr Crit Care Med. 2017;18(4):343–348. doi:10.1097/PCC.0000000000001096
- Woodruff AG, Choong K. Long-term outcomes and the post-intensive care syndrome in critically ill children: a North American perspective. Children. 2021;8(4):254. doi:10.3390/children8040254
- Barichello T, Sayana P, Giridharan VV, et al. Long-term cognitive outcomes after sepsis: a translational systematic review. Mol Neurobiol. 2019;56(1):186–251. doi:10.1007/s12035-018-1048-2
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group* t. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
- Wynn JL. Defining neonatal sepsis. Curr Opin Pediatr. 2016;28(2):135–140. doi:10.1097/mop.0000000000000315
- Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158(4):280–286. doi:10.7326/0003-4819-158-4-201302190-00009
- Fink EL, Maddux AB, Pinto N, et al. A core outcome set for pediatric critical care*. Crit Care Med. 2020;48(12):1819–1828. doi:10.1097/CCM.0000000000004660
- Fitzgerald JC, Kelly N-A, Hickey C, et al. Implementation of a follow-up system for pediatric sepsis survivors in a large academic pediatric intensive care unit. Original research. Front Pediatr. 2021;9:691692. doi:10.3389/fped.2021.691692
- Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and open synthesis. Campbell Syst Rev. 2022;18(2):e1230. doi:10.1002/cl2.1230
- MacLaren G, Butt W, Best D, Donath S, Taylor A. Extracorporeal membrane oxygenation for refractory septic shock in children: one institutionʼs experience. Pediatr Crit Care Med. 2007;8(5):447–451. doi:10.1097/01.PCC.0000282155.25974.8F
- Farris RW, Weiss NS, Zimmerman JJ. Functional outcomes in pediatric severe sepsis: further analysis of the researching severe sepsis and organ dysfunction in children: a global perspective trial. Pediatr Crit Care Med. 2013;14(9):835–842. doi:10.1097/PCC.0b013e3182a551c8
- Sidhu N, Joffe AR, Doughty P, et al. Sepsis after cardiac surgery early in infancy and adverse 4.5-year neurocognitive outcomes. J Am Heart Assoc. 2015;4(8):e001954. doi:10.1161/jaha.115.001954
- Kaur J, Singhi P, Singhi S, Malhi P, Saini AG. Neurodevelopmental and behavioral outcomes in children with sepsis-associated encephalopathy admitted to pediatric intensive care unit: a Prospective Case Control Study. J Child Neurol. 2016;31(6):683–690. doi:10.1177/0883073815610431
- Killien EY, Farris RWD, Watson RS, Dervan LA, Zimmerman JJ. Health-related quality of life among survivors of pediatric sepsis*. Pediatr Crit Care Med. 2019;20(6):501–509. doi:10.1097/pcc.0000000000001886
- Zimmerman JJ, Banks R, Berg RA, et al. Trajectory of mortality and health-related quality of life morbidity following community-acquired pediatric septic shock. Crit Care Med. 2020;48(3):329–337. doi:10.1097/ccm.0000000000004123
- Sankar J, Moodu S, Kumar K, Sankar MJ, Kabra SK, Lodha R. Functional outcomes at 1 year after PICU discharge in critically ill children with severe sepsis. Pediatr Crit Care Med. 2021;22(1):40–49. doi:10.1097/pcc.0000000000002592
- Farris RW, Weiss NS, Zimmerman JJ. Functional outcomes in pediatric severe sepsis; further analysis of the RESOLVE trial. Pediatr Crit Care Med. 2013;14(9):835. doi:10.1097/PCC.0b013e3182a551c8
- Volakli E, Sdougka M, Mantzafleri P, Tsonidis C, Kontopoulos E, Tsikoulas I. Functional outcome following pediatric intensive care: pediatric Cerebral Performance Category (PCPC) and Pediatric Overall Performance Category (POPC) during a prospective two years follow-up period. Greek e J Perioper Med. 2015;13:2–15.
- Knoester H, Bronner MB, Bos AP. Surviving pediatric intensive care: physical outcome after 3 months. Intensive Care Med. 2008;34(6):1076–1082. doi:10.1007/s00134-008-1061-4
- Borghesi A, Trück J, Asgari S, et al. Whole-exome sequencing for the identification of rare variants in primary immunodeficiency genes in children with sepsis: a Prospective, Population-based Cohort Study. Clin Infect Dis. 2020;71(10):e614–e623. doi:10.1093/cid/ciaa290
- Kalvas LB, Harrison TM. State of the science in pediatric ICU delirium: an integrative review. Res Nurs Health. 2020;43(4):341–355. doi:10.1002/nur.22054
- Chung H-Y, Wickel J, Brunkhorst FM, Geis C. Sepsis-associated encephalopathy: from delirium to dementia? J Clin Med. 2020;9(3):703. doi:10.3390/jcm9030703
- de Araújo BES, Da silva fontana R, De magalhães-barbosa MC, et al. Clinical features, electroencephalogram, and biomarkers in pediatric sepsis-associated encephalopathy. Sci Rep. 2022;12(1):10673. doi:10.1038/s41598-022-14853-z
- Becker AE, Teixeira SR, Lunig NA, et al. Sepsis-related brain MRI abnormalities are associated with mortality and poor neurological outcome in pediatric sepsis. Pediatr Neurol. 2022;128:1–8. doi:10.1016/j.pediatrneurol.2021.12.001
- Algebaly H, ElSherbini S, Galal A, Hamdi R, Baz A, Elbeleidy A. Transcranial Doppler can predict development and outcome of sepsis-associated encephalopathy in pediatrics with severe sepsis or septic shock. Front Pediatr. 2020;8:450. doi:10.3389/fped.2020.00450
- Bockli K, Andrews B, Pellerite M, Meadow W. Trends and challenges in United States neonatal intensive care units follow-up clinics. J Perinatol. 2014;34(1):71–74. doi:10.1038/jp.2013.136
- Ducharme-Crevier L, K-a L, Francois T, et al. PICU follow-up clinic: patient and family outcomes 2 months after discharge. Pediatr Crit Care Med. 2021;22(11):935–943. doi:10.1097/PCC.0000000000002789