
Abstract
Objective
To explore the risk factors of atrial fibrillation (AF) in patients with coronary heart disease (CHD), and to construct a risk prediction model.
Methods
The participants in this case-control study were from the cardiovascular Department of Changzhou Affiliated Hospital of Nanjing University of Chinese Medicine from June 2016 to June 2023, and they were divided into AF group and non-AF group according to whether AF occurred during hospitalization. The clinical data of the two groups were compared by retrospective analysis. Multivariate Logistic regression analysis was used to investigate the risk factors of AF occurrence in CHD patients. The nomogram model was constructed with R 4.2.6 language “rms” package, and the model’s differentiation, calibration and effectiveness were evaluated by drawing ROC curve, calibration curve and decision curve.
Results
A total of 1258 patients with CHD were included, and they were divided into AF group (n=92) and non-AF group (n=1166) according to whether AF was complicated. Logistic regression analysis showed that age, coronary multiple branch lesion, history of heart failure, history of drinking, pulmonary hypertension, left atrial diameter, left ventricular end-diastolic diameter and diabetes mellitus were independent risk factors for the occurrence of AF in CHD patients (P < 0.05). The ROC curve showed that the AUC of this model was 0.956 (95% CI (0.916, 0.995)) and the consistency index was 0.966. The calibration curve of the model is close to the ideal curve. The analysis of decision curve shows that the prediction value of the model is better when the probability threshold of the model is 0.042~0.963.
Conclusion
The nomogram model established in this study for predicting the risk of AF in patients with CHD has better predictive performance and has certain reference value for clinical identification of high-risk groups prone to AF in patients with CHD.
Coronary heart disease (CHD) refers to the heart disease caused by coronary artery stenosis or occlusion caused by coronary artery atherosclerosis, resulting in myocardial ischemia, hypoxia and even necrosis. In 2018, the CHD mortality rate of urban residents was 120.18/100,000, and that of rural residents was 128.24/100,000.Citation1 Atrial fibrillation (AF) is one of the common types of arrhythmia in clinical practice. During the onset of AF, the atrial frequency can reach 300 ~ 600 times/min and the ventricular rate can reach 100 ~ 160 times/min, and the heart rhythm is disturbed, making it difficult to maintain the normal physiological function of the heart.Citation2 AF is positively correlated with age, and the incidence of the elderly over 75 years old can reach 10%, and the incidence and fatality rate of the disease are increasing year by year and tend to be younger.Citation3 Studies have shown that the occurrence of AF is closely related to CHD, and the pathogenesis may be related to the myocardial ischemia in the corresponding part caused by coronary artery stenosis in CHD patients, resulting in atrial remodeling, the disturbance of ischemic myocardial fiber structure, the formation of abnormal retracting ring, and then the onset of AF.Citation4 Moreover, repeated attacks of AF will further aggravate myocardial ischemia in CHD patients, cause imbalance of myocardial oxygen supply, and even induce myocardial infarction, which will increase the disability and mortality of CHD patients.Citation5,Citation6
At present, the phenomenon of CHD patients with AF is becoming more and more common, and the two affect each other, forming a vicious circle.Citation7 Therefore, early detection of the risk factors of AF in CHD patients and effective countermeasures are of positive significance for reducing and preventing AF in CHD patients and improving the prognosis of CHD and AF patients.Citation8
In present study, a retrospective analysis method was adopted to explore the risk factors for AF in CHD patients by constructing a Logistic regression analysis model, and the risk prediction nomogram model was constructed, in order to provide certain clinical reference for reducing the risk of AF in CHD patients.
Materials and Methods
Participants
The participants in this case-control study were from the cardiovascular Department of Changzhou Affiliated Hospital of Nanjing University of Chinese Medicine from June 2016 to June 2023. The diagnostic criteria were referred to the Guidelines for the Diagnosis and Treatment of Coronary Atherosclerotic Heart Disease, A patient was deemed to have CHD if at least one of the three major coronary arteries or major branches had significant coronary stenosis ≥50%.Citation9 The participants were divided into AF group and non-AF group according to whether AF was complicated or not, and the diagnostic criteria were referred to the Chinese Guidelines for the Diagnosis and Treatment of Atrial Fibrillation.Citation10 This study complied with the norms of medical research and was approved by the Medical Ethics Committee of Changzhou Affiliated Hospital of Nanjing University of Chinese Medicine (ethics batch number: CZYLL20230126), and complied with the Declaration of Helsinki. Since the study was a retrospective analysis, the Medical Ethics Committee of Changzhou Affiliated Hospital of Nanjing University of Chinese Medicine did not require the consent of all patients for the study, but requested that the patient’s medical data be kept confidential throughout the process, including the patient’s name, contact information, home address and other information.
Inclusion Criteria
(1) Patients meeting the diagnostic criteria for CHD; (2) Persons aged 18 years and above.
Exclusion Criteria
(1) Clinical laboratory examination and other medical records are incomplete; (2) Poor compliance or lack of contact information, unable to complete the interview.
Study Methods
Retrospective analysis was used to collect relevant clinical data of patients in the two groups. Including age, sex, history of hypertension (HP), history of diabetes (DM), history of hyperlipidemia, history of coronary multiple branch lesion (CMBL), history of heart failure (HF), history of valvular heart disease (VHD), history of drinking (drink), history of smoking (smoke), pulmonary hypertension (PH), mean ventricular rate (MVR), left atrial inner diameter (LAD), left ventricular end-diastolic inner diameter (LVEDD), blood potassium less than 4.0 mmol/L (K+< 4.0 mmol/L), long course of disease (course), ventricular septal thickness (VST), C-reactive protein (CRP), Body Mass Index (BMI), haemoglobin (HGB), white blood cell count (WBC), aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine (Cr). Drink was defined as having an average of at least one drink per month in the past 12 months, regardless of the type of alcohol consumed. Course was defined as coronary heart disease course greater than 5 years. Smoke was defined as ≥1 cigarette a day, and the cumulative smoking time was ≥6 months.
Statistical Analysis
R software (4.2.1) and SPSS 24.0 were used for statistical analysis. Continuous variable data were expressed as mean and standard deviation (SD) and were compared using a two-tailed T-test. Categorical variables are expressed in percentages and numbers and compared using chi-square tests. The data were then feature screened using minimum absolute contraction and selection operator (LASSO) regression analysis. Multivariate logistic regression was used to calculate the odds ratio (OR) of each factor and the corresponding 95% confidence interval (95% CI). Then the p values corresponding to each factor are obtained. We selected risk factors with p values <0.05 for logistic regression, constructed prediction models and plotted modal plots. c index was calculated by R software, receiver operating characteristic (ROC) curve and correction curve were drawn, and decision curve analysis (DCA) was performed to check the accuracy of the prediction model.Citation11
Results
Comparison of General Data Between the Two Groups
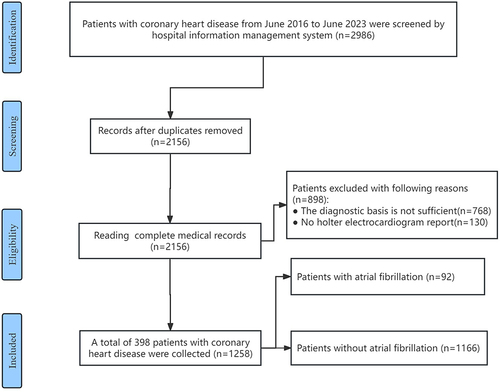
According to inclusion and exclusion criteria, a total of 1258 patients with CHD were collected clinical data, and they were divided into AF group (n=92) and non-AF group (n=1166) according to whether AF was complicated, the selection process of patients is shown in . There were statistically significant differences between the two groups in age, DM, CMBL, HF, VHD, drink, smoke, PH, MVR, LAD, LVEDD, K+< 4.0 mmol/L, course, and ALT, as shown in .
Table 1 Comparison of Clinical Data Between the Two Groups
Figure 1 Flowchart of research subject screening.
Screening of Risk Factors of AF Co-Occurrence in CHD Patients
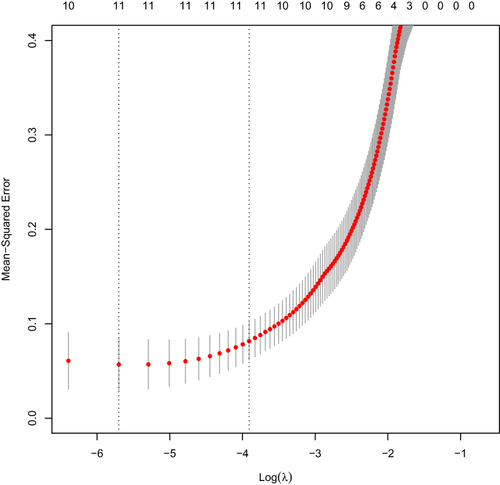
The independent variable of whether AF co-occurrence in CHD patients was taken as the dependent variable, and the data with differences between the two groups were the independent variable. Through LASSO regression analysis (70% cross-validation), 11 potential risk factors were initially screened out. They are age, DM, CMBL, HF, VHD, smoke, drink, PH, LAD, LVEDD, and course, as shown in and .
Figure 2 Coefficient path of LASSO regression.
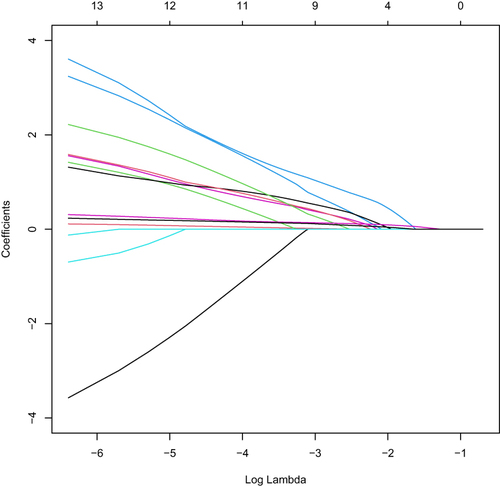
Figure 3 LASSO regression verification results.
Logistic Regression Analysis of Risk Factors of AF Occurrence in CHD Patients
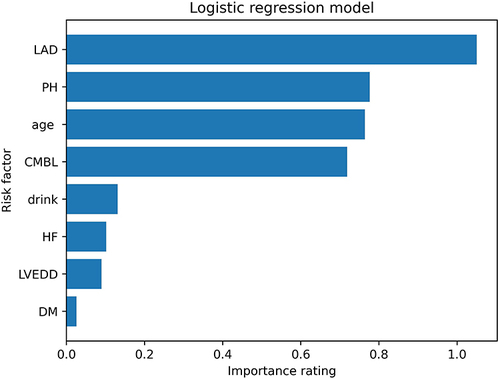
Logistic regression analysis was performed with whether CHD patients developed AF as the dependent variable and risk factors, such as age, DM, CMBL, HF, VHD, smoke, drink, PH, LAD, LVEDD, and course selected by LASSO regression as independent variables. The results showed that age, DM, CMBL, HF, drink, PH, LAD, and LVEDD were independent risk factors for the occurrence of AF in CHD patients (P < 0.05), as shown in . The feature_importances_function of the logistic regression model was used to calculate the relative importance scores of the 8 risk factors obtained by logistic regression analysis. The importance of risk factors was ranked as follows: LAD, PH, age, CMBL, drink, HF, LVEDD, and DM as shown in .
Table 2 Multi-Factor Logistic Regression Analysis
Figure 4 Importance ranking of risk factors.
Nomogram Model Construction and Verification
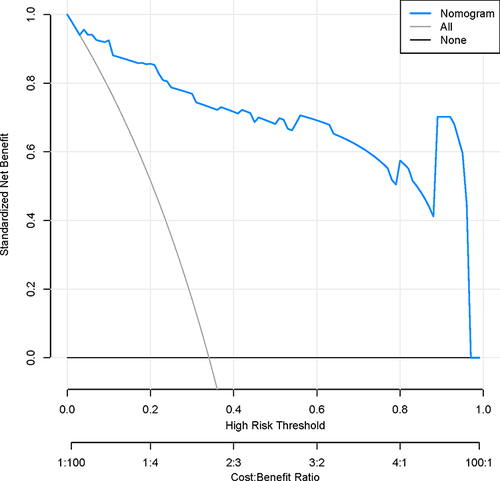
Based on nine influential factors, including age, DM, CMBL, HF, drink, PH, LAD, and LVEDD, a column graph model was constructed to predict the risk of AF in CHD patients, as shown in . As shown in , ROC curve analysis suggested that the AUC of the model was 0.956 (95% CI (0.916, 0.995)). Bootstrap analysis shows that the consistency coefficient of the model is 0.966. As shown in , the calibration curve of the model is close to the ideal curve. As shown in , the analysis of decision curve indicates that the prediction value of the model is superior when the prediction probability threshold of the model is 0.042~0.982. In addition, we built a more interactive and user-friendly dynamic nomogram model for the risk of atrial fibrillation in patients with coronary heart disease to facilitate its use in clinical settings. The link to the dynamic nomogram webpage is as follows: https://cxf12345.shinyapps.io/AF-CHD/
Figure 5 The nomogram model for predicting AF risk in CHD patients.
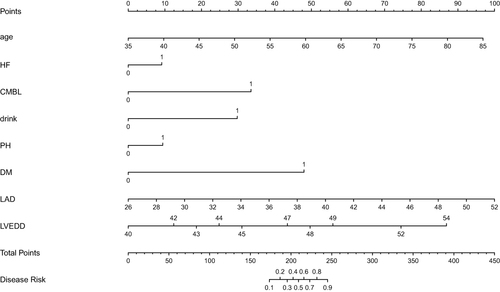
Figure 6 AUC curve of the nomogram model.
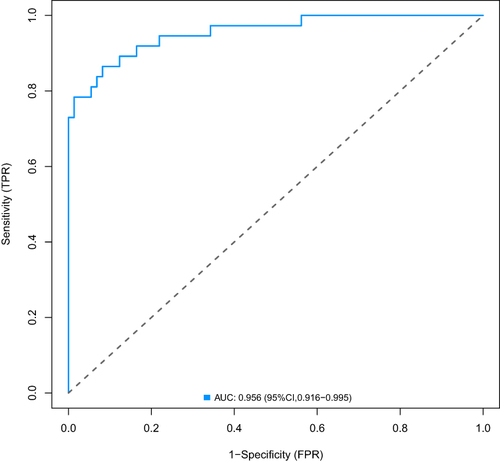
Figure 7 Calibration curve of the nomogram model.
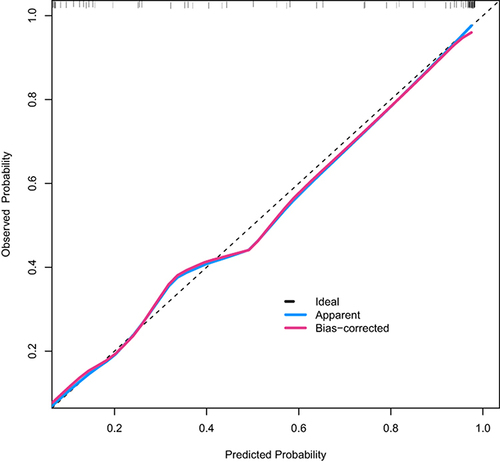
Figure 8 Decision curve of the nomogram model.
Subgroup Analysis of Logistic Regression Models
According to the age of the subjects, the subjects were divided into the young group (less than 60 years old) and the elderly group (greater than or equal to 60 years old). The results of subgroup analysis showed that the risk factors for atrial fibrillation in both groups of patients with coronary heart disease included heart failure HF, LAD, LVEDD, CMBL, drinking and PH. The difference was that the risk factors in the elderly group also included DM, while the young group did not. In addition, the prediction accuracy of the prediction model constructed in both groups was high, 0.938 in the young group and 0.944 in the elderly group. According to the coronary artery lesions of the subjects, they were divided into single coronary artery lesion group, double coronary artery lesion group and triple coronary artery lesion group. The results of subgroup analysis showed that the risk factors for atrial fibrillation in the three groups of patients with coronary heart disease included heart failure HF, LAD, age, drinking and PH. The difference was that the risk factors in the single coronary artery lesion group also included LVEDD, the risk factors in the double coronary artery lesion group also included DM, and the risk factors in the triple coronary artery lesion group also included LVEDD and DM. In addition, the prediction accuracy of the prediction models constructed in the three groups was high, which was 0.937 in the single coronary artery lesion group, 0.918 in the double coronary artery lesion group, and 0.926 in the triple coronary artery lesion group.
Discussion
Summary of Findings
CHD is still one of the major causes of death in both developed and developing countries, and the prevalence of both CHD and AF is increasing year by year globally, and the coexistence of both is increasingly common.Citation12 Studies have reported that AF is associated with 6% to 15% of patients with stable CHD,Citation13 and the risk of AF in patients with acute coronary syndrome is as high as 10% to 37%.Citation14 New AF is a common arrhythmia in patients with CHD, which will increase the length of hospital stay and all-cause mortality of patients.Citation15 Although some studies suggest that the occurrence of CHD and AF share many common risk factors,Citation16 there are few studies on the risk factors for the occurrence of AF in CHD patients. In this study, the possible risk factors of AF in CHD patients were preliminarily discussed by establishing a Logistic model, and the risk prediction nomogram model was constructed and the prediction efficiency of the model was verified.
LASSO regression model can effectively compress the regression coefficient while preserving the subset contraction, which can solve the biased estimation caused by collinear data in univariate Logistic regression analysis.Citation17 In this study, LASSO regression was used to screen out 11 risk factors of AF occurrence in CHD patients, and multi-factor Logistic regression analysis was further performed. The results showed that age, CMBL, HF, DM, drink, PH, LAD, and LVEDD were independent risk factors for AF in CHD patients. Some studies have suggested that the incidence of AF is proportional to age, which may be related to the elderly’s susceptibility to heart structure and electrical remodeling.Citation18 Due to myocardial ischemia in patients with CHD reduced left ventricular compliance, thereby increasing the load before and after the left ventricle, the longer it is easy to cause the left atrium and the left ventricular myocardial hypertrophy, resulting in left atrium and the LVEDD increases, leading to heart cavity expansion, eventually forming abnormal turn-back ring induced AF.Citation19,Citation20 Patients with multi-vessel CHD are more likely than ordinary people to have atrial and ventricular remodeling due to long-term ischemia and hypoxia in a large area of myocardium, and electrical disturbance and electrical reentry caused by atrial ventricular remodeling are important risk factors for AF.Citation21 CHD patients often have HF, and left ventricular failure will increase the pressure load of the left atrium, and long-term increase in left atrial pressure will easily lead to structural and electrical remodeling of the left atrium, thus increasing the risk of AF.Citation22 Studies have shown that the incidence of atrial fibrillation is higher in patients with coronary heart disease who have diabetes. Diabetes is an independent risk factor for atrial fibrillation in patients with coronary heart disease, which is consistent with the results of this study.Citation23 The mechanism by which diabetes makes patients with coronary heart disease more susceptible to atrial fibrillation may be related to the blood sugar fluctuations, autonomic dysfunction and atrial structural remodeling that it causes in patients with coronary heart disease.Citation24 Our study suggests that alcohol consumption is an independent risk factor for AF in CHD patients. Studies have shown that long-term alcohol consumption, even moderate intake, is also an important risk factor for the occurrence of AF,Citation25 which may be related to myocardial degeneration and hypertrophy caused by long-term alcohol intake, and then left atrial remodeling.Citation26 Studies have suggested that patients with pulmonary hypertension may experience structural and electrical remodeling of the right atrium due to the increased load on the right heart, which may easily induce the onset of AF.Citation27,Citation28 Therefore, taking effective measures to improve coronary blood supply in patients with CHD stabilize patients’ blood sugar levels, improve atrial and ventricular remodeling in patients with coronary heart disease, reduce the inner diameter of the left atrium and ventricle in patients with CHD, prevent and correct HF, effectively reduce patients’ pulmonary artery pressure, and avoid drinking alcohol are the key to reducing the risk of AF in patients with CHD.
In present study, a nomogram model for risk prediction of AF in CHD patients was constructed. ROC curve analysis indicated that the AUC of this nomogram model for predicting AF in CHD patients was 0.956, with good differentiation. The calibration curve indicated that the nomogram model had a high calibration degree. The analysis of decision curve shows that the prediction value of the model is better when the probability threshold of the model is 0.042~0.963.
Strengths and Limitations
This study has some strengths. First of all, a key strength of this study is our ability to simultaneously assess a wide range of predictors of the risk factors for the occurrence of AF in CHD patients, including objective examination of laboratory indicators, lifestyle and dietary habits, and disease history. Second, this study takes patients with CHD as the research object, which is more targeted. In addition, visualization of the model into a nomogram will be more practical in clinical practice, and will be helpful for early identification and intervention of high-risk groups of occurring AF among the CHD population, which is of great significance for the prevention and treatment of CHD population for occurring AF. Third, we included new risk factors such as LAD, LVEDD, drink, which are more readily available clinically and reduce the pain of invasive testing. Finally, we use clinical decision curves and clinical impact curves to assess the model’s clinical decision making ability, not just the AUC. The AUC is only concerned with the accuracy of the model’s predictions and cannot tell us whether the model is worth using. The clinical decision curve can help physicians make better decisions by evaluating the net benefits of patients under different prediction probabilities.Citation29
However, there are several limitations to our study that need to be noted. First, as with previous retrospective case-control studies, causal inference is limited. Therefore, our results and conclusions can only be used to assess the risk of AF in a CHD population, and this nomogram model needs to be validated by further rigorously designed external validation. Secondly, there are many risk factors affecting the incidence of AF in patients with CHD. Although we considered 24 variables, this does not cover all variables associated with AF in patients with CHD, and future studies will need a wider range of variables to further validate our findings. In addition, this was a study with only Chinese patients from a single region, which may limit its generalizability. Finally, this study is a single-center study with a small sample size and a relatively inadequate representation of the research sample. A multi-center study should be conducted to further improve the results with a larger sample size.
Conclusion
The nomogram model established in this study for predicting the risk of AF in patients with CHD has better predictive performance and has certain reference value for clinical identification of high-risk groups prone to AF in patients with CHD.
KEY MESSAGES
1. The present study is the first report on a nomogram that predicts the risk factors for the occurrence of AF in CHD patients.
2. In our series, age, DM, LAD, LVEDD, CMBL, HF, drink, and PH were the risk factors for the occurrence of AF in CHD patients, in which LAD was the most important risk factor.
Author Contributions
XF Cao, ZH Gu, and XL Li designed this study. Y Sun, YQ Chen, C Tang, and HW Yu acquired and analyzed data for this work. XF Cao wrote the manuscript. ZH Gu and XL Li revised the manuscript. XF Cao is the guarantor of the study and made the major contribution to the conception and design of the study, revised the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing interests for this work.
Acknowledgments
The authors would like to thank Daohai Chen, Shirun Shan, Huiwen Gu, and Chunqin Zhang from Changzhou Affiliated Hospital of Nanjing University of Chinese Medicine for their assistance on data extraction.
Data Sharing Statement
Data and any appendix material related to this article can be obtained from the corresponding author on request.
Additional information
Funding
References
- Hu SS, Wang ZW. Overview of China cardiovascular health and disease report 2022. Chin J Card Dise. 2019;21(07):577–600.
- Hohendanner F, Heinzel FR, Blaschke F, et al. Pathophysiological and therapeutic implications in patients with atrial fibrillation and heart failure. Heart Fail Rev. 2018;23:27–28. doi:10.1007/s10741-017-9657-9
- Zhao ZH, Zhang XG. Atrial fibrillation epidemiological investigation 20 years China [J]. Chin J Card Pacem Elect Phys. 2023;5(3):232–235.
- Huang C. Atrial fibrillation: current understanding and treatment recommendations-2018. Chin J Card Pac Elect. 2018;32(04):333.
- Zhang YY, Qiu C, Davis PJ, et al. Predictors of progression of recently diagnosed atrial fibrillation in registry on cardiac rhythm disorders assessing the control of atrial fibrillation (RecordAF)-United States cohort. Am J Cardio. 2013;112(1):79–84. doi:10.1016/j.amjcard.2013.02.056
- Fu DJ, He J, Zhang XY. Analysis of risk factors for thrombosis in patients with nonvalvular atrial fibrillation. Chin J Circ. 201227(4):282.
- Xu YY. Correlation analysis of plasma D-D, Fg levels and left atrial size in patients with coronary heart disease and atrial fibrillation. J Bengbu Med Colle. 2019;48(2):226–229.
- Yin YH LJY, Liu JW. The relationship and significance of red blood cell distribution width, galactose agglutinin 3 and neutrophil lymphocyte ratio with coronary heart disease complicated with atrial fibrillation. Chin J Card Dise. 2023;21(01):40–44.
- Han YL, Gao W, Fu XH. Guidelines for diagnosis and treatment of stable coronary heart disease. Chin J Cardio. 2018;46(9):680–694.
- Ma CS, Wu SL, Liu SW, et al. Chinese guidelines for diagnosis and treatment of atrial fibrillation. Chin J Cardio. 2019;51(6):572–618.
- Zeng Y, Zhao J, Zhang J, et al. Development of a Nomogram That Predicts the Risk of Coronary Heart Disease in Patients With Hyperlipidemia. J Cardiovasc Pharmacol Ther. 2023;28(107424842311677):54. doi:10.1177/10742484231167754
- Wang YB, Wu YJ. Clinical characteristics and related progress of stroke prevention and treatment in patients with coronary heart disease complicated with atrial fibrillation. Chin J Circu. 2018;33(12):1239–1241.
- Gizurarson S, Stahlman M, Jeppsson A, et al. Atrial fibrillation in patients admitted to coronary care units in western Sweden-focus on obesity and lipotoxicity. J Elect. 2015;48(5):853–860.
- Lamblin N, Meurice T, Tricot O, et al. First hospitalization for heart Failure in outpatients with stable coronary artery disease: Determinants, Role of incident myocardial infarction, and prognosis. J Card Fail. 2018;24(12):815–822. doi:10.1016/j.cardfail.2018.09.013
- Tian Y, Wei XY, Chen YL, et al. Meta-analysis of risk factors for new atrial fibrillation after acute myocardial infarction. J Card Vasc Dis. 2019;38(12):1275–1279.
- Mallikarjuna R, Edupuganti M, Marmagkiolis K, et al. Optimizing selection of antithrombotic therapy in patients requiring PCI and long term anticoagulation. Card Rev Med. 2014;15(8):414–420.
- Zhang LJ, Wei XY, Lu JQ, et al. Lasso regression: from Interpretation to Prediction. Adv Psych Sci. 2020;28(10):1777–1791. doi:10.3724/SP.J.1042.2020.01777
- Zhang J, Johnsen SP, Guo Y, et al. Epidemiology of atrial fibrillation: Geographic/ecological risk factors, age, sex, genetics. Card Elect Clin. 2021;13(1):1–23.
- Menichelli D, Sciacqua A, Cangemi R, et al. ATHERO-AF study group. Atrial fibrillation pattern, left atrial diameter and risk of cardiovascular events and mortality. A prospective multicenter cohort study. Int J Clin Pract. 2021;75(3):e13771. doi:10.1111/ijcp.13771
- Chou H, Chen H, Xie J, et al. Higher Incidence of Atrial Fibrillation in Left Ventricular-to-Right Atrial Shunt Patients. Front Physiol. 2020;11:580624. doi:10.3389/fphys.2020.580624
- Rezaei Y, MM P, Naghshbandi S, et al. Postoperative atrial fibrillation following cardiac surgery: from pathogenesis to potential therapies. Am J Card Drug. 2020;20(1):19–49.
- Carlisle MA, Fudim M, DeVore AD, et al. Heart Failure and Atrial Fibrillation. JACC Heart Fail. 2019;7(6):447–456. doi:10.1016/j.jchf.2019.03.005
- Xu Q, Peng Y, Tan J, et al. Prediction of atrial fibrillation in hospitalized elderly patients with coronary heart disease and type 2 diabetes mellitus using machine learning: a multicenter retrospective study. Front Public Health. 2022;10:842104. doi:10.3389/fpubh.2022.842104
- Brundel BJJM, Ai X, Hills MT, Kuipers MF, Lip GYH, de Groot NMS. Atrial fibrillation. Nat Rev Dis Primers. 2022;8(1):21. doi:10.1038/s41572-022-00347-9
- Larsson SC, Drca N, Wolk A. Alcohol consumption and risk of atrial fibrillation: a prospective study and dose-response meta-analysis. J Am Coll Card. 2014;64(3):281–289. doi:10.1016/j.jacc.2014.03.048
- Elliott AD, Gallagher C, Middeldorp ME, et al. Drinking to atrial fibrillation: alcohol and atrial fibrillation incidence. Europ. 2020;22(2):177–178.
- Nattel S, Dobrev D. Deciphering the fundamental mechanisms of atrial fibrillation: a quest for over a century. Card Res. 2016;109(4):465–466. doi:10.1093/cvr/cvw028
- Hiram R, Provencher S. Pulmonary Disease, Pulmonary Hypertension and Atrial Fibrillation. Card Elect Clin. 2021;13(1):141–153.
- Chalkou K, Vickers AJ, Pellegrini F, Manca A, Salanti G. Decision curve analysis for personalized treatment choice between multiple options. Med Decis Making. 2023;43(3):337–349. doi:10.1177/0272989X221143058