
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Present medical practice encourages management according to written guidelines, protocols, and structured procedures (GPPs). Daily medical practice includes instances in which “leaping” from one patient management routine to another is a must. We define “frozen patient management”, when patient management leaping was required but was not performed. Frozen patient management may cause significant damage to patient safety and health and the treatment quality. This paper discusses the advantages and disadvantages of GPP-guided medical practice and gives an explanation of the problem of frozen patient management in light of quality engineering, control engineering, and learning processes. Our analysis of frozen patient management is based on consideration of medical care as a process. By considering medical care processes as a closed-loop control process, it is possible to explain why, when an indication for deviation from the expected occurs, it does not necessarily attract the medical teams’ attention, thereby preventing the realization that leaping to an alternative patient management is needed. We suggest that working according to GPPs intensifies the frozen patient management problem since working according to GPPs relates to “exploitation learning behavior”, while leaping to new patient management relates to “exploration learning behavior”. We indicate practice routines to be incorporated into GPP-guided medical care, to reduce frozen patient management.
Introduction
One of many
One of the court rulings on medical negligence in Israel was the subject of delayed diagnosis of retinal detachment, which resulted in severe visual loss in the patient. The patient was diagnosed with infectious conjunctivitis that deteriorated. The doctors (diagnosticians and those who provided care) were captive by the diagnosis and guidelines for infectious conjunctivitis and did not consider other reasons for the patient’s visual deterioration. The end result was that they did not leap to the retina separation diagnosis and guideline until the damage became irreversible. When finally the retinal detachment was discovered, the visual loss was irreversible (case A51694/04).
The primary purpose of this paper is to introduce quality engineering terminology and techniques into medical practice. Specifically, we aimed to discuss the advantages and disadvantages of medical practice following written guidelines, protocols, and structured procedures (GPPs) and the problem of “frozen patient management (PM)” that inhibits timely “leaping” from one PM routine to another. The above scenario is an example of a medical team that continued with a selected PM, without replacing it with a more appropriate one (ie, leaping from one PM routine to another). While there is no doubt about the benefits and importance of working according to written GPP, our approach is that there are cases where leaping from one PM routine to another is a must.
Present medical practice encourages management according to written GPPs. The GPPs are based on current evidence and experience, providing a sense of security, organization, and order to the work. In most instances, working according to GPPs results in the optimization of patient care. It also gives peace of mind to the caregiving team. Nevertheless there are cases where replacing the chosen GPP by an alternative one may be required (ie, leaping from one PM routine to another). For instance, leaping may be required when the initial PM was based on data of high uncertainty and was created before additional, clearer data or data validation was available, thus leading to choice of the wrong GPP. Moreover, even when the chosen GPP is correct, the specific patient may not react as expected to the treatment. This may happen since GPPs fit most of the patients with the specific problem but not all.
Despite the importance of timely leaping from a decided GPP to another, there are events when medical teams fail to do so. We define “frozen PM” as a failure to leap. Frozen PM may cause significant damage to patient safety, health, and the treatment quality.
The following discussion is an attempt to analyze the problem of frozen PM in light of quality engineering, control engineering, and learning processes that have been shown to improve function in industries. The adaptation of quality and engineering concepts to the health care domain started in the 1980s, with a main emphasis on the structural process and outcome aspects of medical care, by several researchersCitation1–Citation6 who shared the view that: “The current American healthcare system is in crisis … engineering can be used to transform the healthcare system into one that is safe, effective, patient centered, timely, efficient, and equitable”.Citation7 It is important to notice that attention was given to structural process and outcome aspects of medical care and not to the medical care professionals’ decisions and processes. The following includes our suggestion to adapt the concepts of quality engineering, control engineering, and learning to medical care.
Our explanation for frozen PM is based on consideration of medical care as a process. By considering medical care processes as closed-loop control processes, it is possible to explain why, when an indication for deviation from expected occurs, it does not necessarily attract the medical teams’ attention, thereby preventing the realization that leaping to an alternative PM is needed. We call these indications gaps – rifts between expected and actual output results. Here, we adopt an approach based on analysis of closed-loop control systemsCitation8 demonstrating that when gaps occur, the controller compensates for it (ie, indicating “false alarm”) and prevents its realization. Only extremely large gaps may really be realized as failures that require response.
We suggest that frozen PM occurs since PM is a closed-loop process it suffers from the problem of not realizing gaps as failures. Although in principle, the problem seems to be similar, ie, not recognizing gaps as failures, the mechanisms to explain it are different. Frozen PM occurs when gaps are considered to be part of the current PM without raising explicit attention to anomalies – even if the actual state is, in fact, quite different. In the medical care closed-loop process, the “controller” is the human mind.
Moreover, working according to GPPs intensifies the frozen PM problem since working according to GPP relates to an “exploitation” learning behavior, while leaping to new PM relates to an “exploration” learning behavior. Traditionally, exploration and exploitation learning behaviors are related to research and development. We adapt these terms to patient care. Organizational learning is “the process of improving actions through better knowledge and understanding”,Citation9,Citation10 while learning behavior consists of activities through which data are obtained and processed.Citation11 Exploitation is defined as the “ongoing use of a firm’s knowledge base”;Citation12 therefore exploitative behavior emphasizes standardization, uniformity, low risk, consistency, and low variance. Exploration is defined as “search for new knowledge”;Citation12 therefore explorative behavior emphasizes discretion, high variability, and high risks.
We suggest that although GPPs emphasize exploitative behavior, they enfeeble exploration learning behavior.Citation13,Citation14 As a result, working according to GPPs intensifies the frozen PM problem.
Doctors in a closed loop
A closed-loop system is a system in which the controller is used to automatically modify the control input of a plant in such a way that the process remains stable, and the output remains as close as possible to its desired value.Citation14 For example, for engineering a closed-loop system one could envision a heat exchanger that should heat water to a specific temperature. If the water temperature is lower than the target value, more heated steam is made to flow.
In order to explain unidentified failures in medical care, we modeled the medical care process as a closed-loop one (), based on Wagner’s logical model of medical diagnosis.Citation15
Figure 1 Medical care process modeled as a closed-loop process.
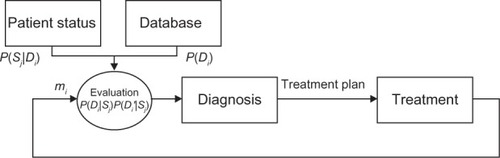
The process model contains the following blocks:
Database: The teams evaluate P(Di), the probability that the patient has a particular set of diseases Di
Patient status: The teams evaluate P(Sj|Di), the probability of the occurrence of a syndrome Sj, given a particular set of diseases Di
Evaluation block: The medical team evaluates P(Di|Sj), the probability of the patient having the set of diseases Di, expressed by the syndrome Sj; and
, the probability that the patient does not have the set of diseases
Diagnosis block: The medical team determines the patient diagnosis, derived from the evaluation block
Treatment block: The medical team treats the patient according to the treatment plan. The patient manifestation mi is received from this block. The patient manifestations at t = 0 are the initial ones.
As time progresses, the manifestations change with the treatment, as is the patient’s response to it. The patient’s manifestation mi returns to the evaluation block as an input to the decision of whether the PM should remain unchanged and stay in the closed-loop or leap to another PM (different closed-loop). When frozen PM occurs, ie, when the manifestations mi deviate from the expected values
, it should not necessarily be considered as relating to failure.
Relating to the heat exchanger example, if a hole occurs in one of the steam pipes, additional steam is made to flow, and the output water temperature is kept at the temperature target value. When monitoring the water temperature, it is not identified as a clear deviation from the temperature target unless several deviations occur; the reason is that the controller has compensated by increasing the released steam. Similarly, the medical team may relate to a deviated manifestation (ie, gap) as resulting from other reasons, such as technical problems (equipment mishaps) or delay in the patient’s response to treatment. Only when the gap is extremely large or the medical manifestations are very unexpected and unambiguous, will the team reconsider the gap as a failure.
In medical care processes, the “controller” is the human mind, which does not identify the gaps as failures, mainly due to factors such as biases and habitual routine. Anchoring bias is the common human tendency to rely too heavily, or “anchor”, on one trait or piece of information when deciding on the PM, locking on to salient features in a PM too early and failing to adjust in light of later information.Citation16 Furthermore, the wrong PM can even drive the medical team to look for tests that will support its PM rather than searching for additional options, creating the “confirmation bias”: Looking for evidence to support a PM rather than looking for evidence that might rebut it.Citation17 “Ego bias is manifested in the warping of probability estimates in a self-serving way”.Citation18 Recent study has shown that both individual physicians and medical teams show great confidence in their judgments, even when it can be shown to be incorrect.Citation18 A physician’s ego is affected by patients, who often need to consider their physician as someone who never fails, especially in critical situations involving a patient’s life. Since physicians often believe that they will beat the overall odds of success for any venture in which they participateCitation18 and that they are always right, they fail to ask for a second opinion, even in risky cases. Medical teams may not change the PM since this can be perceived as admitting a failure to predict the correct PM.
“A habitual routine exists when a group repeatedly exhibits a functionally similar pattern of behavior in a given stimulus situation without explicitly selecting it over alternative ways of behaving”.Citation19,Citation20 We claim that frozen PM is a specific aspect of habitual routine. It relates to a medical team that is not aware of the need to leap to an alternative PM, even when the results indicate that the current PM is inappropriate and irrelevant. Teams, like individuals, often develop habitual routines for dealing with frequently encountered stimuli. Habitual routine drives teams to ignore alternative behavior since automatically, new or different data are considered to comply with the same PM, without giving explicit attention to anomalies.Citation19,Citation20 This phenomenon is very prevalent in medical teams since habitual routine often occurs when dealing with a process subjected to frequently changing stimuli, as happens in medical care.
Frozen PM, GPPs, and learning
GPPs, in which organizations store knowledge,Citation21 emphasize controlling the variance in processes and outcomes.Citation22 They reduce the variance and the personnel’s ambiguity,Citation23 and as a result, emphasize low-variance establishment and ensure uniform execution. GPPs are based on knowledge and experience, are considered fit, and the general advice they proffer is thought to be applicable to a broad range of cases.Citation24 Working according to GPPs relates to exploitation learning behavior.
While GPPs relate to exploitation learning behavior, which emphasizes standardization, uniformity, low risk, consistency, and low variance, leaping to an alternative PM requires discretion, high variability, flexibility, experimentation, and divergent thinking. Leaping to an alternative PM is largely dependent on the ability of the medical team to be continuously aware of the importance of updating and expanding knowledge and data in light of changing data and environmental conditions, as well as the essentiality of PM changing with time. This can and should use internal as well as external options and ideas. It means that the medical team cannot afford to rely entirely on their “inside” subdivision knowledge; they should also look for “outside” options. In patient care, the treating medical teams are usually experts in one discipline, with a limited set of information, and thus are bound to a lower level of flexibility. The medical team should be open to incorporating an outsider’s input. Leaping to an alternative PM requires exploration learning behavior. Exploration learning behavior consists of activities such as searching for, discovering, creating, and experimenting with new opportunities;Citation20 experimenting with new approaches;Citation25 innovating;Citation25–Citation28 and reconsidering existing beliefs and decisions.Citation29–Citation31
GPPs restrict exploration learning behavior since their structured nature makes adaptation difficult.Citation14 The variation-reducing focus restricts the development of alternatives,Citation13 hampers the discretion of the employees,Citation32 leads to resistance to change and momentum, and thus, inhibits variability,Citation13 thereby leading to an “easy road” of habitual routines. Moreover, well-learned guidelines and procedures generally contribute to individual members’ comfort with the department – well-learned guidelines and procedures increase members’ confidence about their roles in the department, and reduce the risk of “doing the wrong thing” and being perceived as a deviant.
Integration of exploitation and exploration learned behavior applied to medical practice
Two approaches have been introduced to provide explanations of how organizations can achieve both exploration and exploitation learning behaviors. The first approach, “ambidextrous”, refers to highly differentiated but weakly integrated subunits.Citation30 According to this approach, organizational units should specialize in either exploration or exploitation learning behaviors. Exploration units should be located in different places, have different personnel, and even be related to suborganizations that are distinct from the “mother firm”.Citation13 In medicine, this may be analogous to different functions characterizing academic and nonacademic institutions. The second approach, “punctuated equilibrium”, refers to temporal rather than organizational structure differentiation. It suggests organizational transformation through cycles of long time periods of exploitation learning behavior and short bursts of exploration learning behavior.Citation33 This approach enables organizations to balance between exploration and exploitation learning behaviors as they shift from one activity to another.Citation34 This approach is difficult to apply to medical practice, which needs an overall continuous, uninterrupted practice routine. Yet perhaps focal, pointed organizational leaping may occur.
Unfortunately, medicine requires a new approach that combines the two accepted and contradictory approaches, both of which deal with the balance between exploration and exploitation learning behaviors. On the one hand, in line with the ambidextrous approach, we posit that exploitation and exploration learning behaviors are separate and derive from the PM leaping. On the other hand, since the interplay is generally short (in terms of time) and dynamic, it can be said that the two learning behaviors exist simultaneously, as in the punctuated equilibrium approach. Moreover, while the existence of interplay has been discussed in several studies,Citation33,Citation35–Citation37 other authors believe that interplay occurs over a relatively long period of time. We, on the other hand, suggest that the interplay (ie, leaping) can occur over very short time periods: days or even hours. In order to reduce frozen PM occurrence, daily routine clinical practice should be able to incorporate exploration into its routine exploitation infrastructure. Further research is still needed before appropriate guidelines can be written on the subject.
Conclusion
In most cases, working in closed-loop systems according to GPPs results in the optimization of patient care and maximization of treatment quality and safety. In some cases, leaping from one PM to another may be required. Despite the importance and benefits of the introduction of GPP into the PM routine, some disadvantages will be incorporated. Working according to GPPs intensifies the problem of frozen PM. Consequently, working according to GPPs must be established with a methodology that will ensure PM leaping when required. Further research is needed to achieve the goal of introducing structured integration of exploitation and exploration learning behavior into medical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
- DonabedianAAn Introduction to Quality Assurance in Health CareOxfordOxford University Press2002
- CareyRGLloydRCMeasuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsMilwaukee, WIAmerican Society for Quality2001
- NemethCO’ConnorMKlockPACookRDiscovering healthcare cognition: the use of cognitive artifacts to reveal cognitive workOrgan Stud200627710111035
- LynnJBailyMABottrellMThe ethics of using quality improvement methods in health careAnn Intern Med2007146966667317438310
- NelsonECBataldenPBPatient-based quality measurement systemsQual Manag Health Care199321183010131017
- GardnerGGardnerAO’ConnellJUsing the Donabedian framework to examine the quality and safety of nursing service innovationJ Clin Nurs2014231–214515523834585
- GreenMNembhardHBLiterature Review of Healthcare DeliveryState College, PAPenn State University2009 Available from: http://www.cihds.psu.edu/pdf/literature%20review%20of%20healthcare%20delivery.pdfAccessed October 13, 2014
- Kobo-GreenhutAIntegration of Feedback Control and Statistical Process Control [master’s thesis]HaifaTechnion2009
- FiolMCLylesMAOrganizational learningAcad Manage Rev198510803810
- ArgoteLOrganization Learning: Creating, Retaining and Transferring KnowledgeNew York, NYSpringer2013
- EdmondsonAPsychological safety and learning behavior in work teamsAdmin Sci Quart1999442350383
- VermeulenFBarkemaHLearning through acquisitionAcad Manage J2001443457478
- BennerMJTushmanMLExploitation, exploration, and process management: The productivity dilemma revisitedAcad Manage Rev2003282238256
- BrownSLEisenhardtKMCompeting on the Edge – Strategy as Structured ChaosBoston, MAHarvard Business Press1998
- WagnerHNJrRegional ventilation and perfusionWagnerHNJrSzaboZBuchananJWPrinciples of Nuclear MedicinePhiladelphia, PASaunders1995881895
- CroskerryPThe importance of cognitive errors in diagnosis and strategies to minimize themAcad Med200378877578012915363
- OgataKModern Control Engineering3rd edUpper Saddle River, NJPrentice Hall1996
- DawsonNVArkesHRSystematic errors in medical decision making: judgment limitationsJ Gen Intern Med1987231831873295150
- GersickCJHackmanJRHabitual routines in task-performing groupsOrgan Behav Hum Decis Process199047659711538273
- DayRDLeading and Managing People in the Dynamic OrganizationPsychology Press2014
- MarchJGExploration and exploitation in organizational learningOrgan Sci1991217187
- JuranJMGodfreyABJuran’s Quality Handbook5th edNew York, NYMcGraw-Hill1998
- TatikondaMVMontoya-WeissMMIntegrating operations and marketing perspectives of product innovation: The influence of organizational process factors and capabilities on development performanceManage Sci2001471151172
- MatusikSFHillCWLThe utilization of contingent work, knowledge creation, and competitive advantageAcad Manage Rev1998234680697
- McGrathRGExploratory learning, innovative capacity, and managerial oversightAcad Manage J2001441118131
- DuncanRBModifications in decision structure in adapting to the environment: Some implications for organizational learningDecision Sci197454705725
- MartiniAGastaldiLCorsoMLaugenBTContinuous innovation: towards a paradoxical, ambidextrous combination of exploration and exploitationInt J Technol Manage2013611122
- TushmanMO’ReillyCAmbidextrous organizations: managing evolutionary and revolutionary changeCalif Manage Rev1996384830
- FloydSWLanePJStrategizing throughout the organization: Managing role conflict in strategic renewalAcad Manage Rev2000251154177
- GhemawatPRicart CostaJEIThe organizational tension between static and dynamic efficiencyStrategic Manage J199314S2S59S73
- RivkinJWSiggelkowNBalancing search and stability: Interdependencies among elements of organizational designManage Sci2003493290311
- CropanzanoRByrneZSBobocelDRRuppDEMoral virtues, fairness heuristics, social entities, and other denizens of organizationalv justiceJ Vocat Behav2001582164209
- GuptaAKSmithKGShalleyCEThe interplay between exploration and exploitationAcad Manage J2006494693706
- RomanelliETushmanMLOrganizational transformation as punctuated equilibrium: An empirical testAcad Manage J199437511411166
- LewisMWWalshMADehlerGEGreenSGProduct development tensions: exploring contrasting styles of project managementAcad Manage J2002453546564
- RaischSBirkinshawJProbstGTushmanMLOrganizational ambidexterity: balancing exploitation and exploration for sustained performanceOrgan Sci2009204685695
- HjelmgrenDDuboisAOrganising the interplay between exploitation and exploration: The case of interactive development of an information systemInd Market Manag201342196105