
Abstract
Leprosy is a complex infectious disease caused by Mycobacterium leprae that is a leading cause of nontraumatic peripheral neuropathy. Current control strategies, with a goal of early diagnosis and treatment in the form of multidrug therapy, have maintained new case reports at ~225,000 per year. Diagnostic capabilities are limited and even with revisions to multidrug therapy regimen, treatment can still require up to a year of daily drug intake. Although alternate chemotherapies or adjunct immune therapies that could provide shorter or simpler treatment regimen appear possible, only a limited number of trials have been conducted. More proactive strategies appear necessary in the drive to elimination. As a prevention strategy, most chemoprophylaxis campaigns to date have provided about a 2-year protective window. Vaccination, in the form of a single bacillus Calmette–Guérin (BCG) immunization, generally provides ~50% reduction in leprosy cases. Adapting control strategies to provide both chemoprophylaxis and immunoprophylaxis has distinct appeal, with chemoprophylaxis theoretically buttressed by vaccination to generate immediate protection that can be sustained in the long term. We also discuss simple assays measuring biomarkers as surrogates for disease development or replacements for invasive, but not particularly sensitive, direct measures of M. leprae infection. Such assays could facilitate the clinical trials required to develop these new chemoprophylaxis, immunoprophylaxis strategies, and transition into wider use.
Epidemiology and etiology of leprosy
Leprosy, also known as Hansen’s disease, is historically associated with disfigurement, social ostracization, and removal of basic human rights. These situations have now thankfully been improved and legally rectified in most countries. Although it is now known that leprosy is a chronic infectious disease caused by Mycobacterium leprae, various myths such as the disease being a divine curse, karma for past misdeeds, or a genetic predisposition, among others, persist. Leprosy can, however, be controlled and is curable.
Leprosy is an extremely complex disease as it manifests across a wide array of symptoms, and various forms can be distinguished and characterized. M. leprae has a predilection for the skin and, uniquely, also the nerves. The World Health Organization (WHO) has established diagnostic criteria as the presence of one or more of the following key signs: appearance of hypopigmented or reddish lesion with hypoesthesia, presence of acid-fast bacilli in lymph node smears, and compatible skin lesion histopathology. Although nonfatal and typically characterized by the appearance of skin lesions, leprosy is one of the most common worldwide causes of nontraumatic peripheral neuropathy. Neuropathy arises not only from the infection and damage of peripheral nerves by M. leprae itself but also from the inflammatory and immunologic responses to the infection. In addition, as many as half of all patients may be affected by one of the two major clinical types of leprosy reactions, which are acute inflammatory complications that can develop during the course of leprosy irrespective of treatment status. The inflammation associated with reactions can be a medical emergency that often requires hospitalization. If nerve damage is allowed to progress, it can become disabling or, through sensory loss, lead to traumatic injury.Citation1–Citation3
Once diagnosed, leprosy is treatable and patients are operationally defined into one of two categories, paucibacillary (PB) and multibacillary (MB), for treatment purposes. The Ridley–Jopling scale characterizes five forms of leprosy through the use of clinical, histopathological, and immunological methods: lepromatous leprosy (LL), borderline lepromatous, mid-borderline, borderline tuberculoid (BT), and tuberculoid leprosy (TT).Citation4,Citation5 A pure neural leprosy presentation, which is PB, also exists. PB leprosy patients, encompassing TT and a number of BT forms, are characterized as having one or few skin lesions and granulomatous dermatopathology with low or absent bacterial indices (BI). At the extreme PB pole, TT patients demonstrate a specific cell-mediated immunity against M. leprae and have an absent, or low, BI. Control of bacterial growth by PB patients indicates that these individuals mount a strong, but not necessarily curative, immune response against M. leprae. MB leprosy encompasses LL, borderline lepromatous, mid-borderline, and a number of BT forms. At the extreme MB pole, LL patients demonstrate high titers of anti-M. leprae antibodies but an absence of specific cell-mediated immunity.Citation4 In the absence of a strong cellular immune response, LL patients do not control bacterial replication and have high BI. Because most of the clinicians and health care workers who are seeing patients typically have limited facilities that cannot readily determine Ridley–Jopling classification, the simplified WHO diagnostic criteria have been widely adopted as the preferred diagnostic strategy. Reliance on only one key criterion for the operational MB/PB diagnosis presents limitations; however, because not all lesions are obviously hypopigmented or erythematous, and they are not always anaesthetic. The clinical diagnosis may be supported by the histopathological analysis of a skin lesion, especially when bacilli and/or a neural infiltration are found, but these methods do not have good sensitivity. This is especially true for patients with indeterminate or TT presentations.
Treatment for leprosy has evolved over time. Since 1995, based upon the annual reporting of new cases, WHO has disseminated a cocktail of antibiotics for free of charge in the form of multidrug therapy (MDT). The widespread provision of MDT and revised shortened treatment regimens have been major contributors to the massive reduction of registered leprosy cases. Although 16 countries reported > 1,000 new cases during 2009, all but a handful have yet to achieve a prevalence rate of less than one case per 10,000 persons, the threshold considered indicative of eliminating leprosy as a public health problem.Citation6 In all WHO regions and at a global level, the number of new cases reported during the reporting year has stabilized in recent years, and continued or renewed vigilance appears necessaryCitation7 Leprosy is not evenly spread and localized regions with higher incidence rates can generally be distinguished within most reporting countries.Citation8–Citation11 Several Indian states are reporting the maintenance of, or reemergence of prevalence rates to, levels above the national target, and an abundance of new cases are now being detected in the Amazon region of Brazil.Citation12–Citation14 Many cases are likely not being diagnosed and the reported numbers probably significantly underrepresent the real leprosy situation.Citation15
Interestingly, conditions with which to culture M. leprae in vitro have not been determined and how M. leprae enters the body to establish infection is not definitively known. Many patients anecdotally connect the site of their first obvious lesion with some previous injury or skin break, and entry through the skin is implied. Similarly, it is unclear how transmission occurs, although person-to-person transmission and subsequent expulsion of M leprae directly in the skin and nasal epithelia are strongly suggested.Citation16 MB cases typically have large numbers of acid-fast bacilli deep in the dermis, and although there are reports of M leprae in the desquamating epithelium, there are no reports of acid-fast bacilli being found in the epidermis. It is, therefore, unclear if M leprae reach the skin surface in large enough numbers to represent a meaningful mechanism of transmission.Citation17 LL patients have relatively large amounts of M leprae in the superficial keratin layer of the skin, suggesting that the bacteria may exit along with the sebaceous secretions.Citation18 The quantity of M leprae within nasal mucosal lesions of LL patients can be as high as 1 × 107 bacilli, and most lepromatous patients have bacilli that are expelled into their nasal secretions by simply blowing the nose.Citation19–Citation21 Research, therefore, increasingly favors the respiratory route as the major mode of expulsion and potential transmission to others.Citation22,Citation23 Alongside genetic factors, one of the most significant risk factors for developing leprosy is long-term contact, typically through sharing the same residence, with an untreated MB leprosy patient.
Treatment strategies
In order to develop preventative strategies to reduce the incidence of leprosy, it is instructive to understand how the disease is treated and to consider the current limitations and potential complications that may arise.
Chemotherapy
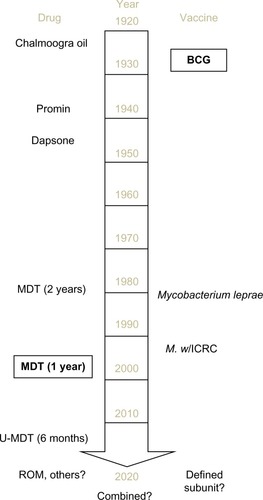
Treatments for leprosy have undergone considerable evolution in the past century: from chaulmoogra oil in 1915 to promin, a sulfone drug that successfully treated leprosy but required many painful injections in the 1940s, to dapsone monotherapy in 1946, and then eventually to MDT in 1982 (). By the 1960s, resistance to dapsone had started to develop, and dapsone-resistant M. leprae strains are now prevalent. In 1981, a WHO study group recommended MDT, a combination of dapsone, rifampicin (RIF), and clofazimine. This cocktail is safe and effective and provided in convenient monthly calendar blister packs. Since 1995, WHO has been providing free MDT for all patients in the world initially through the drug fund provided by the Nippon Foundation and since 2000, through Novartis and the Novartis Foundation. As part of Novartis’s commitment to the 2012 London Declaration on Neglected Tropical Diseases, the company renewed its pledge to work to end leprosy by extending its donation of MDT through 2020. This includes MDT and support costs, to aid WHO with the donation and logistics, worth >US$40 million with an overall expectation of reaching an estimated 1.3 million patients.
Figure 1 Timeline of the major treatment and prevention strategies for leprosy.
Abbreviations: BCG, bacillus Calmette–Guérin; MDT, multidrug therapy; ROM, rifampicin, ofloxacin, and minocycline; U-MDT, uniform multidrug therapy; M. w, Mycobacterium w; ICRC, Indian Cancer Research Center.
MDT, consisting of RIF, clofazimine, and dapsone for MB leprosy patients and RIF and dapsone for PB leprosy patients, alters the course of disease in leprosy patients and is the most common way to limit the dissemination of M leprae to others. Interestingly, RIF is the only component that is strongly bactericidal for M. leprae.Citation24,Citation25 Dapsone is a sulfone antibiotic for which anti-inflammatory and immunomodulatory effects have been recognized but the precise mechanism of action is not known. Clofazimine has a weakly bactericidal action against M. leprae. Because clofazimine is an orange-colored iminophenazine dye, it often causes discoloring of the skin. This skin pigmentation gradually resolves, but it may require up to 2 years once the drug is discontinued to return to pretreatment levels, and patients often feel marked and stigmatized by this and withdraw clofazimine from their treatments as a consequence.
Although MDT is effective in the majority of current cases, as mentioned, dapsone resistance is relatively widespread. When combined with clofazimine noncompliance, this means that many patients may unwittingly be taking RIF monotherapy. This has the potential to be highly conducive for the emergence of resistance and several investigators have indeed observed multidrug-resistant strains of M. leprae.Citation26–Citation31 The WHO Global Leprosy Programme initiated a Sentinel Surveillance Network to monitor drug resistance in leprosy to proactively monitor the situation.Citation32 The widespread emergence of drug-resistant M. leprae would undermine the efforts of the WHO-MDT campaign.Citation29,Citation33–Citation36
Relapse rates after taking MDT are generally low (~1%), but wide variations are reported in different regions and can be unacceptably high in some areas.Citation37,Citation38 Relapse rates are dependent on several operational factors. A 10-year prospective study in the Philippines noted a significant difference in the relapse rates of MB patients followed at a referral center versus those observed in field clinics (9% and 3%, respectively).Citation39 In southern India, a much higher relapse rate, equivalent to 20/1,000 person-years, was observed among MB patients given MDT for 2 years. This rate was reduced to 10/1,000 person-years in patients who were treated until they became smear negative.Citation40 In general, higher relapse rates are observed in patients with a high BI at the time of diagnosis, indicating that these patients likely require longer treatment.Citation37,Citation41 When relapse does occur, it is often related to poor MDT compliance.
Over time, the duration of leprosy treatments has gradually been shortened: dapsone was given over many years; when first introduced, MDT was administered to MB and PB patients for 2 and 6 months, respectively; since 1998, MDT has been given to MB patients for 1 year.Citation42 Even with shortening treatment times, patients can become weary with the length of treatment and may also experience intolerance, side effects, and toxicity from each of the components of the regimen.Citation38,Citation43 Despite concerns that a uniform MDT regimen provided to all patients for 6 months may undertreat MB patients, especially those with a high initial BI, and simultaneously overtreat PB leprosy patients, such a regimen has been trialed on the basis that it is operationally more convenient and could therefore be more effective in the context of the integration into general health care services.
While there appears to be a need for alternative bactericidal agents and more combinations that can be used to treat leprosy, these are currently limited. Ofloxacin, as well as other quinolones, has been reported to have a rapid and highly bactericidal activity against M. leprae in mouse experiments and human trials. Although moxifloxacin/pefloxacin/ofloxacin, minocycline, and clarithromycin have all demonstrated greater activity than both dapsone and clofazimine in clinical trials, clinical application of these has been largely confined to the use of single-dose RIF, ofloxacin, and minocycline for single-lesion PB leprosy patients in trials.Citation44–Citation51 To evaluate the efficacy of a 4-week ofloxacin-containing regimen for PB leprosy, we enrolled PB patients in a randomized, double-blind trial.Citation52 One group received the standard 6-month WHO-MDT regimen, whereas the other received 28 daily supervised doses of RIF 600 mg + ofloxacin 400 mg, plus 5 months of placebo. Both regimens appeared generally efficacious and resulted in few relapses. While the addition of ofloxacin and minocycline as secondary treatments could attenuate the spread of drug resistance among M. leprae, it is noteworthy that ofloxacin resistance has been found in at least two relapses.Citation32,Citation34,Citation44,Citation49,Citation53–Citation56 Moxifloxacin, gatifloxacin, and linezolid are all licensed for human use and are used to treat several bacterial infections. PA 824, now called pretomanid, is in an advanced stage of development. Although the efficacy of moxifloxacin, gatifloxacin, linezolid, and PA 824 as antimycobacterials has been demonstrated in tuberculosis (TB) models, these drugs have had only limited amounts of testing in the mouse footpad model of M. leprae infection.Citation57,Citation58 Evaluations of these agents against replicating M. leprae have been undertaken in the mouse footpad model.Citation59 A dose–response curve was observed for linezolid activity against M. leprae: 25 mg/kg five times weekly was bacteriostatic, 50 mg/kg five times weekly was partially bactericidal, and 100 mg/kg was fully bactericidal. The strong bactericidal activity of moxifloxacin against stationary M. leprae was extended by demonstrating activity against “rapidly” multiplying M. leprae. PA 824 was found to lack any activity against rapidly multiplying M. leprae. Thus, experimental evaluations of emerging antimycobacterials that are being driven by TB research provide an important transition to inform their potential, or lack thereof, for treating leprosy.
Immunotherapy
Another strategy with which to reduce the duration of treatment is to adjunct chemotherapy with immune therapy, and the concept of using a vaccine in conjunction with drugs for treatment of leprosy has already been studied. Katoch et alCitation60 evaluated untreated high BI cases that were allocated to one of three treatment groups. All patients received a modified MDT regimen; but in addition, one control group received distilled water, another group received bacillus Calmette–Guérin (BCG), and yet another group received killed Mycobacterium w (M. w) every 6 months, until M. leprae was no longer observed in skin slit smears. Despite inducing cell-mediated immunity, the incidence of reactions was not increased by provision of the vaccines. Viable bacteria were detected by outgrowth in mouse footpads in samples from patients on MDT alone up to 24 months of therapy, whereas there was no indication of living M. leprae in either of the two immunotherapy groups after 12 months. Patients in both the immunochemotherapy groups showed histological upgrading and accelerated granuloma clearance.
In a similar study, untreated MB patients with moderate BI were provided MDT for 12 months and one of three treatments (saline, intradermal BCG, or M. w, each administered at 3-month intervals for four total doses).Citation61 By 12 and 24 months, the patients in BCG group demonstrated a significantly greater improvement in clinical score compared to those in the M. w group, with both the BCG and M. w groups showing reduced clinical scores compared to the MDT only control group. BI declined by 2.40 units per year in patients receiving BCG, 2.05 units per year in the M. w group, and 0.85 units per year in the control group. The incidence of type 2 reactions, neuritis, and development of new deformities was decreased compared to the controls.
These studies indicate that cellular responses can be induced even in leprosy patients with high BI without exacerbating disease and that the addition of immunotherapy to MDT can reduce the effective treatment period required for bacterial clearance.
Preventative strategies
Although the free, widespread provision of MDT has massively impacted and reduced the global prevalence of leprosy, there are many indications that further effort is required to maintain control and continue onward toward eradication. Active case-finding programs generally record case numbers at rates many fold greater than those detected and reported by the current, passive detection strategies. M. leprae infection does not always cause disease, and estimates are that up to 75% of infections may be spontaneously cleared without causing significant symptoms.Citation62,Citation63 Together, these indicate that reliance on the appearance of clinical symptoms to prompt treatment leaves a large population of M. leprae infected individuals with the potential to transmit infection to others who could propagate disease. Focusing on immediate contacts of patients as recruits within trials aiming to reduce the incidence of leprosy is a logical and practical strategy, although large enrollments are still necessary to provide the statistical power required to interpret efficacy.
Chemoprophylaxis
Various chemoprophylaxis trials have demonstrated a benefit to treating individuals lacking the symptoms of leprosy, especially in those at the highest risk of infection.Citation64–Citation72 RIF treatment had a significant impact in Indonesian communities where everybody was given the drug but had no effect in similar communities where only household contacts and direct neighbors were treated.Citation64,Citation73 Single-dose RIF treatment showed a protective effect of 57% in household and other contacts when used as a prophylactic strategy in Bangladesh.Citation74 These results are in line with older dapsone prophylaxis programs, which were also found to be more effective when provided to everyone residing in affected communities.Citation70 Although generally successful, the relative failure of this approach in a subset of seropositive contacts of MB patients could be that their bacillary load may have been too high to be eliminated by a single dose (or as in Indonesia, two doses) of RIF by the time the chemoprophylaxis is given.
Although each chemoprophylaxis trial has reported a benefit, different magnitudes and the relatively short duration of protection indicate functional limitations. This cannot be entirely unexpected because drugs can only protect those already harboring M. leprae, and thus, while chemoprophylactic strategies can reduce the incidence of leprosy in some situations, the nature of drug activity restricts efficacy to a subset of individuals: anyone infected after the chemoprophylaxis is given is not protected. There are also indications that a more extensive regimen may be needed for those nondiseased individuals harboring higher levels of M. leprae.
Vaccines
By promoting a lasting adaptive immune response, a vaccine, unlike drug treatment, has the potential to provide active and sustained protection. Consistent with exposure or low-level infection, many contacts of leprosy patients exhibit M. leprae antigen-specific inflammatory responses and the majority do not develop disease. Thus, the ideal vaccine against leprosy would induce strong, long-lasting T-cell responses directed against M. leprae antigens that would limit infection, prevent disease, and, furthermore, reduce bacterial transmission to others.
Although attempts have been made to develop a vaccine based on whole mycobacteria, at present, the BCG vaccine more typically associated with TB is the only vaccine administered for the prevention of leprosy. The presence of a BCG scar has been recognized as a protective factor for leprosy, but, as clearly indicated by the persistence of leprosy in countries where BCG use is widespread, BCG vaccination does not provide perfect protection against the disease.Citation10 The degree of protection afforded by BCG against leprosy has varied dramatically between studies. Systematic meta-analyses indicate that BCG has a wide-ranging protective efficacy with an average ~50% and protection appears to be better against the MB than the PB form.Citation75,Citation76 The use of different BCG strains may be a factor in the varied protection reported across various studies, although this remains unclear.Citation77 As with TB, the protection afforded by BCG against leprosy is greatest in children and wanes with aging.Citation78–Citation80 Computer modeling, based on the 2003 leprosy situation in hyperendemic districts of Bangladesh, indicated that the incidence of leprosy would be substantially reduced by, among various other factors, good BCG vaccine coverage of infants.Citation81
Some studies indicate that multiple BCG vaccinations enhance protection and it has been relatively common to recommend the immunization (or reimmunization) of leprosy patients and their contacts.Citation82,Citation83 Because no substantial benefit of BCG revaccination is observed against TB; however, WHO guidelines for TB do not support BCG revaccination.Citation84–Citation86 Models including a second BCG vaccination for the prevention of leprosy have not been generated and the efficacy of this approach is debated.Citation75,Citation87–Citation89
A major research and development area in the TB field is the refinement of BCG to make it more immunogenic and to provide protection over a longer period. Investigators have genetically refined the bacteria and several recombinant BCG (rBCG) vaccines are being evaluated. The protection that most of these rBCG vaccines can afford against leprosy has not been evaluated, and it is therefore unclear what impact they could have on the incidence of leprosy. Only some rBCG vaccines have been produced with consideration of leprosy.Citation90–Citation94
M. leprae itself has been assessed in various trials, often to see if it can add to the protective effect of BCG. Large-scale human trials were conducted in Venezuela, Malawi, and India to measure the efficacy of BCG with and without killed M. leprae.Citation82,Citation83 In Venezuela and Malawi, 5–9 years after vaccination, the incidence rate of all new leprosy cases was reduced across all ages, but the BCG/M. leprae vaccine did not enhance the protection afforded by a primary BCG vaccination alone. Although the observed leprosy incidence rates in a similar trial in South India were not high enough to ascertain the protective efficacy of the vaccines in surveys conducted within the 8 years following immunization, it was determined that BCG/M. leprae improved protection to 64% whereas BCG alone provided 34.1% protection.Citation95 The reason for this discrepancy is unclear, but it is noteworthy that even if M. leprae contributed to protection over BCG, further development of a killed M. leprae-containing vaccine would be enormously constrained by the difficulties associated with mass production. Reproducibly generating a consistent product in immune-compromised mice or armadillos would appear to be extremely difficult, if not impossible, although the data do suggest vaccine improvements over BCG are possible.
Several alternate, cultivatable mycobacteria have also been evaluated as leprosy vaccines. In the aforementioned South India trial, one additional group was immunized with the alternative mycobacteria M. w, while another group was immunized with Indian Cancer Research Center (ICRC) bacilli.Citation95 Both M. w and ICRC bacilli have been demonstrated to protect mice against experimental inoculation of M. leprae.Citation96,Citation97 Of all the immunization groups in the South India trial, ICRC bacilli provided the best protection at 65.5%. Despite evaluations indicating that M. w provided the lowest protective efficacy (25.7%) of all the vaccines evaluated, a large-scale, double-blind trial of a M. w vaccine in index cases and their household contacts was conducted in Uttar Pradesh, India.Citation98 When index cases, and not the contacts, received the M. w vaccine, surveys at 3, 6, and 9 years after the initial vaccination indicated protective efficacies of 43%, 31%, and 3%, respectively. When only contacts received the vaccine, protective efficacies of 69%, 59%, and 39% were observed. When both patients and contacts received the M. w vaccine, the protective efficacy was 68%, 60%, and 28% at each follow-up time. Thus, the protective effect of the M. w vaccine in that follow-up trial was sustained for a period of ~7–8 years. However, M. w has either become widely used in India nor has been evaluated in other leprosy-affected regions.
Combined strategies
As indicated by combined treatment strategies, the simultaneous provision of chemoprophylaxis and immunoprophylaxis is suggested as an active control strategy with the greatest potential of reducing the incidence of leprosy. Given the live mycobacterial basis of the BCG vaccine, it cannot be administered at the same time as any chemoprophylaxis. A combined strategy involving the staggered provision of RIF and BCG is, however, currently under evaluation.Citation99 Unlike BCG, immunization with nonliving vaccines, such as a killed whole mycobacterium or a subunit vaccine, could be provided at the same time as drug treatment. A defined (subunit) vaccine produced by standard methods could negate the quality control concerns associated with whole bacterial vaccines, but such a vaccine is still lacking for leprosy. Experimental immunizations with crude antigens have demonstrated that proteins within the M. leprae cell wall, cell membrane, and cytosol all provide protection when administered with an adjuvant before infection.Citation100,Citation101 The 35 kDa Ag85B and hsp65 antigens have all been shown to confer protection when expressed in a DNA vaccine.Citation102–Citation104 Purified and/or recombinant 10, 25, and 65 kDa proteins have also provided protection in the experimental mouse footpad model.Citation105 Vaccination of mice with the Ag85 proteins purified from BCG culture filtrate, in conjunction with Freund’s incomplete adjuvant, protected by inhibiting M. leprae growth.Citation106 In a conflicting report, however, recombinant Ag85A/B did not protect when administered with either Freund’s incomplete adjuvant or monophosphoryl lipid A.Citation107 As with the use of killed M. leprae, the use of crude M. leprae antigens in a vaccine is severely constrained by the need to cultivate large quantities of M. leprae. Selection and production of recombinant antigens have, however, been simplified by the completion and publication of the M. leprae genome in 2001, and a defined subunit vaccine appears within reach.Citation108–Citation110
Interpreting protection
While the primary goal of any intervention is to reduce overall leprosy incidence, slow development of the disease and the relatively low incidence rates (even in leprosy hyperendemic regions) pose logistical problems for statistically powered evaluations. Leprosy incidence rates are typically reported earlier historically reported levels in trials, probably because of both increased awareness of leprosy within the study population and the requirement for closer observance leading to active case finding.Citation11,Citation73,Citation111 This, and variance in year-to-year leprosy incidence rates, suggests that experimental trials are better suited to distinguish protective strategies than observational studies.Citation75 Observational studies do, however, yield results more quickly. Past studies have either relied on long-term follow-up and comparison of new case detection between untreated and treated groups or on skin slit smears and biopsy to determine how bacterial burden and histological responses of patients have been affected. Surrogate endpoints predictive of response could significantly shorten trials and expedite the adoption of new strategies. The identification of surrogate endpoints indicated by simple biomarkers that could replace, reduce, or negate the need for invasive skin slit or biopsy procedures would also make trials more tractable over larger populations.
The majority of untreated MB leprosy patients can be identified by robust antibody responses at the time of diagnosis and, similar to anti-phenolic glycolipid (PGL)-I IgM responses, IgG responses against protein antigens appear to correlate well with bacterial burden.Citation112–Citation117 This suggests that as M. leprae are killed and removed from the body, these responses should diminish. Accordingly, the IgM responses against PGL-I, as well as the IgG responses to the 35 kDa Ag85A and Ag85B proteins, are all documented to decline during treatment.Citation118–Citation125 Decreases during and after MDT in the antibody responses to recombinant protein antigens, including leprosy IDRI diagnostic-1 (LID-1), which is now being used in rapid diagnostic test formats, have also been reported.Citation126–Citation130 Significant declines in IgG levels are observed among MB patients after completion of MDT, but declines appear to be less pronounced for anti-PGL-I IgM.Citation126,Citation131,Citation132 The rate of decay of anti-PGL-I levels after the initiation of treatment has been reported to range from a linear decline and quick conversion to seronegative through to the retention of positive responses for many years.Citation121,Citation124 While it is unclear how antigen-specific antibodies emerge, develop, and retreat in nondiseased individuals, long-term follow-up of serum antibody responses in a large population, such as is desired for vaccine trails, appears entirely feasible.
Interferon-γ (IFN-γ) release assays are now commonly used for TB and have tended to demonstrate high antigen-specific IFN-γ levels at the time of diagnosis that subsequently decline with treatment. We have identified multiple antigens that are recognized in whole blood assays for leprosy patients.Citation115,Citation133 It is well documented through the use of whole M. leprae or crude antigen fractions that PB patients have strong antigen-specific cellular responses, and this has been corroborated by the observation of IFN-γ secretion in whole blood assay (WBA) involving the incubation of untreated PB patient blood with either peptides or recombinant proteins.Citation115,Citation117,Citation134–Citation138 Although MB patients are usually considered anergic because they have low or absent cell-mediated immunity to crude fractions of M. leprae, “upgrading” of responses upon vaccination or treatment indicates otherwise. The decreased IFN-γ production seen ~2 years after MDT completion in a recent study of PB patients could possibly be explained by the elimination of bacilli and clearance of antigen from the body.Citation131 Indeed, an IFN-γ recall response to LID-1 has been observed among MB patients shortly after the conclusion of MDT.Citation131 Among the recombinant proteins assessed, this property was unique to LID-1, indicating that the cellular responses of MB patients are antigenically restricted. Why the cellular response against LID-1 emerges in MB leprosy patients after MDT is unclear, but an improved understanding of how successful, and even unsuccessful, treatment affects antigen-specific responses of leprosy patients holds the potential to identify markers that could be used to expedite the introduction of treatments and interventions.
Conclusion
Leprosy can be treated, and the disfiguring disabilities associated with advanced nerve damage can be prevented. The most effective treatment requires early diagnosis; however, and this requires continued vigilance. In addition, although current MDT regimens are highly effective, compliance issues and the potential emergence of drug resistance will continue to be of concern. Although alternate drug or adjunct immune therapies with the potential for use in new, shorter, or simpler treatment regimen appear possible, trials to support their widespread use are limited. As a strategy to reduce the incidence of leprosy, even though estimates show that chemoprophylaxis alone provides a 2-year protective window, chemoprophylaxis appears as the best currently available strategy. While effective vaccination programs have the potential to provide a more sustained protective window, adapting control strategies to provide both chemoprophylaxis and immunization has distinct appeal and likely provides the greatest opportunity for sustained reductions in the incidence of leprosy. Further research on alternative therapies and new leprosy control strategies need to overcome economic, political, or operational barriers and require advocacy and sponsorship from pertinent stakeholders. Chemoprophylaxis could provide an immediate, short-term protection, with immunization generating a longer-term protection. Simple assays measuring biomarkers as surrogates for disease development or invasive, but not particularly sensitive, direct measures of M. leprae infection could facilitate the trials required to transition these new control strategies into wider use.
Acknowledgments
Leprosy programs under the supervision of the authors have been supported by funding from Leprosy Research Initiative, Philippines Department of Health, Novartis Foundation, Netherlands Leprosy Relief, The Order of Malta, New York Community Trust Heiser Foundation, and American Leprosy Missions.
Disclosure
The authors report no conflicts of interest in this work.
References
- VisschedijkJvan de BroekJEggensHLeverPvan BeersSKlatserPMycobacterium leprae – millennium resistant! Leprosy control on the threshold of a new eraTrop Med Int Health20005638839910929137
- JacobJTFranco-ParedesCThe stigmatization of leprosy in India and its impact on future approaches to elimination and controlPLoS Negl Trop Dis200821e11318235845
- CrossHInterventions to address the stigma associated with leprosy: a perspective on the issuesPsychol Health Med200611336737317130073
- RidleyDSJoplingWHClassification of leprosy according to immunity. A five-group systemInt J Lepr Other Mycobact Dis19663432552735950347
- ScollardDMClassification of leprosy: a full color spectrum, or black and white?Int J Lepr Other Mycobact Dis200472216616815301586
- WHOGlobal leprosy situation, 2010Wkly Epidemiol Rec2010853533734820830851
- Global leprosy update, 2014: need for early case detectionWkly Epidemiol Rec2015903646147426343055
- BakkerMIHattaMKwenangARisk factors for developing leprosy – a population-based cohort study in IndonesiaLepr Rev2006771486116715690
- MoetFJPahanDSchuringRPOskamLRichardusJHPhysical distance, genetic relationship, age, and leprosy classification are independent risk factors for leprosy in contacts of patients with leprosyJ Infect Dis2006193334635316388481
- GoulartIMBernardes SouzaDOMarquesCRPimentaVLGoncalvesMAGoulartLRRisk and protective factors for leprosy development determined by epidemiological surveillance of household contactsClin Vaccine Immunol200815110110517989339
- BakkerMIHattaMKwenangAKlatserPROskamLEpidemiology of leprosy on five isolated islands in the Flores Sea, IndonesiaTrop Med Int Health20027978078712225510
- BrookCEBeauclairRNgwenyaOSpatial heterogeneity in projected leprosy trends in IndiaParasit Vectors2015854226490137
- SalgadoCGFerreiraDVFradeMAGuimarães LdeSda SilvaMBBarretoJGHigh anti-phenolic glycolipid-I IgM titers and hidden leprosy cases, Amazon regionEmerg Infect Dis201218588989022515845
- BarretoJGGuimaraes LdeSFradeMARosaPSSalgadoCGHigh rates of undiagnosed leprosy and subclinical infection amongst school children in the Amazon RegionMem Inst Oswaldo Cruz2012107Suppl 1606723283455
- SmithWCvan BrakelWGillisTSaundersonPRichardusJHThe missing millions: a threat to the elimination of leprosyPLoS Negl Trop Dis201594e000365825905706
- JobCKJayakumarJKearneyMGillisTPTransmission of leprosy: a study of skin and nasal secretions of household contacts of leprosy patients using PCRAm J Trop Med Hyg200878351852118337353
- WeddellGPalmerEThe pathogenesis of leprosy. An experimental approachLepr Rev196334576113999438
- JobCKJayakumarJAschhoffM“Large numbers” of Mycobacterium leprae are discharged from the intact skin of lepromatous patients; a preliminary reportInt J Lepr Other Mycobact Dis199967216416710472371
- ShepardCCAcid-fast bacilli in nasal excretions in leprosy, and results of inoculation of miceAm J Hyg19607114715714445823
- PedleyJCThe nasal mucus in leprosyLepr Rev197344133354584261
- Naves MdeMRibeiroFAPatrocinioLGPatrocinioJAFleuryRNGoulartIMBacterial load in the nose and its correlation to the immune response in leprosy patientsLepr Rev2013841859123741885
- ReesRJMcDougallACAirborne infection with Mycobacterium leprae in miceJ Med Microbiol19771016368320339
- AraujoSLobatoJReis EdeMUnveiling healthy carriers and subclinical infections among household contacts of leprosy patients who play potential roles in the disease chain of transmissionMem Inst Oswaldo Cruz2012107Suppl 1555923283454
- ShepardCCLevyLFasalPRapid bactericidal effect of rifampin on Mycobacterium lepraeAm J Trop Med Hyg19722144464494559066
- ShepardCCLevyLFasalPFurther experience with the rapid bactericidal effect of rifampin on Mycobacterium lepraeAm J Trop Med Hyg1974236112011244611256
- GrossetJHGuelpa-LaurasCCBobinPStudy of 39 documented relapses of multibacillary leprosy after treatment with rifampinInt J Lepr Other Mycobact Dis19895736076142674301
- WilliamsDLGillisTPMolecular detection of drug resistance in Mycobacterium lepraeLepr Rev200475211813015282962
- MatsuokaMBudiawanTAyeKSThe frequency of drug resistance mutations in Mycobacterium leprae isolates in untreated and relapsed leprosy patients from Myanmar, Indonesia and the PhilippinesLepr Rev200778434335218309708
- MatsuokaMKashiwabaraYNamisatoMA Mycobacterium leprae isolate resistant to dapsone, rifampin, ofloxacin and sparfloxacinInt J Lepr Other Mycobact Dis200068445245511332288
- ManjunathaUHLahiriRRandhawaBDowdCSKrahenbuhlJLBarryCE3rdMycobacterium leprae is naturally resistant to PA-824Antimicrob Agents Chemother200650103350335417005816
- YouEYKangTJKimSKLeeSBChaeGTMutations in genes related to drug resistance in Mycobacterium leprae isolates from leprosy patients in KoreaJ Infect200550161115603834
- WHOMeeting on Sentinel Surveillance for Drug Resistance in LeprosyGenevaWorld Health Organization2011
- JiBJametPSowSPeraniEGTraoreIGrossetJHHigh relapse rate among lepromatous leprosy patients treated with rifampin plus ofloxacin daily for 4 weeksAntimicrob Agents Chemother1997419195319569303392
- CambauEBonnafousPPeraniESougakoffWJiBJarlierVMolecular detection of rifampin and ofloxacin resistance for patients who experience relapse of multibacillary leprosyClin Infect Dis2002341394511731943
- MaedaSMatsuokaMNakataNMultidrug resistant Mycobacterium leprae from patients with leprosyAntimicrob Agents Chemother200145123635363911709358
- MatsuokaMKashiwabaraYLiangfenZGotoMKitajimaSA second case of multidrug-resistant Mycobacterium leprae isolated from a Japanese patient with relapsed lepromatous leprosyInt J Lepr Other Mycobact Dis200371324024314608820
- GelberRHBalagonVFCellonaRVThe relapse rate in MB leprosy patients treated with 2-years of WHO-MDT is not lowInt J Lepr Other Mycobact Dis200472449350015755209
- HonradoERTalloVBalisACChanGPChoSNNoncompliance with the world health organization-multidrug therapy among leprosy patients in Cebu, Philippines: its causes and implications on the leprosy control programDermatol Clin200826222122918346553
- CellonaRVBalagonMFdela CruzECLong-term efficacy of 2 year WHO multiple drug therapy (MDT) in multibacillary (MB) leprosy patientsInt J Lepr Other Mycobact Dis200371430831914763888
- GirdharBKGirdharAKumarARelapses in multibacillary leprosy patients: effect of length of therapyLepr Rev200071214415310920610
- NormanGJosephGRichardJRelapses in multibacillary patients treated with multi-drug therapy until smear negativity: findings after twenty yearsInt J Lepr Other Mycobact Dis20047211715217321
- MalathiMThappaDMFixed-duration therapy in leprosy: limitations and opportunitiesIndian J Dermatol20135829310023716796
- RajuMSJohnASKuipersPWhat stops people completing multi-drug therapy? Ranked perspectives of people with leprosy, their head of family and neighbours – across four Indian statesLepr Rev201586162026065144
- JiBGrossetJCombination of rifapentine-moxifloxacin-minocycline (PMM) for the treatment of leprosyLepr Rev2000Suppl 71S81S8711201894
- JiBJametPPeraniEGBactericidal activity of single dose of clarithromycin plus minocycline, with or without ofloxacin, against Mycobacterium leprae in patientsAntimicrob Agents Chemother1996409213721418878595
- ChanGPGarcia-IgnacioBYChavezVEClinical trial of clarithromycin for lepromatous leprosyAntimicrob Agents Chemother19943835155178203847
- CostaMBCavalcanti NetoPFMartelliCMDistinct histopathological patterns in single lesion leprosy patients treated with single dose therapy (ROM) in the Brazilian Multicentric StudyInt J Lepr Other Mycobact Dis200169317718611875761
- FajardoTTJrVillahermosaLGdela CruzECAbalosRMFranzblauSGWalshGPMinocycline in lepromatous leprosyInt J Lepr Other Mycobact Dis19956318177730723
- GelberRHMurrayLPSiuPTsangMReaTHEfficacy of minocycline in single dose and at 100 mg twice daily for lepromatous leprosyInt J Lepr Other Mycobact Dis19946245685737868955
- GelberRHFukudaKByrdSA clinical trial of minocycline in lepromatous leprosyBMJ1992304681991921737148
- GrossetJHJiBHGuelpa-LaurasCCPeraniEGN’DeliLNClinical trial of pefloxacin and ofloxacin in the treatment of lepromatous leprosyInt J Lepr Other Mycobact Dis19905822812952198315
- BalagonMFCellonaRVAbalosRMGelberRHSaundersonPRThe efficacy of a four-week, ofloxacin-containing regimen compared with standard WHO-MDT in PB leprosyLepr Rev2010811273320496567
- GelberRHChemotherapy of lepromatous leprosy: recent developments and prospects for the futureEur J Clin Microbiol Infect Dis199413119429527698121
- GelberRHSiuPTsangMRichardVChehlSKMurrayLPActivity of combinations of dapsone, rifampin, minocycline, clarithromycin, and sparfloxacin against M. leprae-infected miceInt J Lepr Other Mycobact Dis19956322592647602221
- JiBGrossetJOfloxacin for the treatment of leprosyActa Leprol1991743213261950440
- JiBPeraniEGPetinomCN’DeliLGrossetJHClinical trial of ofloxacin alone and in combination with dapsone plus clofazimine for treatment of lepromatous leprosyAntimicrob Agents Chemother19943846626678031029
- ConsignySBentouchaABonnafousPGrossetJJiBBactericidal activities of HMR 3647, moxifloxacin, and rifapentine against Mycobacterium leprae in miceAntimicrob Agents Chemother200044102919292110991891
- JiBChauffourAAndriesKJarlierVBactericidal activities of R207910 and other newer antimicrobial agents against Mycobacterium leprae in miceAntimicrob Agents Chemother20065041558156016569884
- BurgosJde la CruzEParedesRAndayaCRGelberRHThe activity of several newer antimicrobials against logarithmically multiplying M. leprae in miceLepr Rev201182325325822125933
- KatochKKatochVMNatrajanM10–12 years follow-up of highly bacillated BL/LL leprosy patients on combined chemotherapy and immunotherapyVaccine20042227–283649365715315844
- NarangTKaurIKumarBRadotraBDDograSComparative evaluation of immunotherapeutic efficacy of BCG and mw vaccines in patients of borderline lepromatous and lepromatous leprosyInt J Lepr Other Mycobact Dis200573210511416830653
- BrowneSGSelf-healing leprosy: report on 2749 patientsLepr Rev19744521041114417433
- EkambaramVSithambaramMSelf-healing in non-lepromatous leprosy in the area of the ELEP Leprosy Control Project Dharmapuri (Tamil Nadu)Lepr India1977493387392592741
- BakkerMIHattaMKwenangAPrevention of leprosy using rifampicin as chemoprophylaxisAm J Trop Med Hyg200572444344815827283
- SmithWCChemoprophylaxis in the prevention of leprosyBMJ2008336764773073118390497
- MoetFJOskamLFaberRPahanDRichardusJHA study on transmission and a trial of chemoprophylaxis in contacts of leprosy patients: design, methodology and recruitment findings of COLEPLepr Rev200475437638815682975
- VijayakumaranPKrishnamurthyPRaoPDeclerqEChemoprophylaxis against leprosy: expectations and methodology of a trialLepr Rev2000Suppl 71S37S40 discussion S–111201885
- NguyenLNCartelJLGrossetJHChemoprophylaxis of leprosy in the southern Marquesas with a single 25 mg/kg dose of rifampicin. Results after 10 yearsLepr Rev2000Suppl 71S33S35 discussion S5–S611201884
- DilettoCBlancLLevyLLeprosy chemoprophylaxis in MicronesiaLepr Rev2000Suppl 71S21S33 discussion S4–S511201881
- SmithCMSmithWCChemoprophylaxis is effective in the prevention of leprosy in endemic countries: a systematic review and meta-analysis. MILEP2 Study Group. Mucosal immunology of leprosyJ Infect200041213714211023757
- TinKPopulation screening and chemoprophylaxis for household contacts of leprosy patients in the Republic of the Marshall IslandsInt J Lepr Other Mycobact Dis199967Suppl 4S26S2910700934
- DaulakoECPopulation screening and mass chemoprophylaxis in KiribatiInt J Lepr Other Mycobact Dis1999674 SupplS23S2510700933
- MoetFJSchuringRPPahanDOskamLRichardusJHThe prevalence of previously undiagnosed leprosy in the general population of northwest BangladeshPLoS Negl Trop Dis200822e19818301731
- MoetFJPahanDOskamLRichardusJHCOLEP Study GroupEffectiveness of single dose rifampicin in preventing leprosy in close contacts of patients with newly diagnosed leprosy: cluster randomised controlled trialBMJ2008336764776176418332051
- SetiaMSSteinmausCHoCSRutherfordGWThe role of BCG in prevention of leprosy: a meta-analysisLancet Infect Dis20066316217016500597
- MerleCSCunhaSSRodriguesLCBCG vaccination and leprosy protection: review of current evidence and status of BCG in leprosy controlExpert Rev Vaccines20109220922220109030
- BehrMAWilsonMAGillWPComparative genomics of BCG vaccines by whole-genome DNA microarrayScience199928454191520152310348738
- ZodpeySPBansodBSShrikhandeSNMaldhureBRKulkarniSWProtective effect of Bacillus Calmette Guerin (BCG) against leprosy: a population-based case-control study in Nagpur, IndiaLepr Rev199970328729410603718
- ZodpeySPAmbadekarNNThakurAEffectiveness of Bacillus Calmette Guerin (BCG) vaccination in the prevention of leprosy: a population-based case-control study in Yavatmal District, IndiaPublic Health2005119320921615661132
- RodriguesLCKerr-PontesLRFrietasMVBarretoMLLong lasting BCG protection against leprosyVaccine20072539–406842684417728023
- FischerEAde VlasSJHabbemaJDRichardusJHThe long-term effect of current and new interventions on the new case detection of leprosy: a modeling studyPLoS Negl Trop Dis201159e133021949895
- ConvitJSampsonCZúñigaMImmunoprophylactic trial with combined Mycobacterium leprae/BCG vaccine against leprosy: preliminary resultsLancet199233987914464501346818
- KarongaPreventionTrialGroupRandomised controlled trial of single BCG, repeated BCG, or combined BCG and killed Mycobacterium leprae vaccine for prevention of leprosy and tuberculosis in MalawiLancet1996348901917248691924
- WHOGlobal tuberculosis programme and global programme on vaccines. Statement on BCG revaccination for the prevention of tuberculosisWkly Epidemiol Rec199570322292317669527
- RodriguesLCPereiraSMCunhaSSEffect of BCG revaccination on incidence of tuberculosis in school-aged children in Brazil: the BCG-REVAC cluster-randomised trialLancet200536694931290129516214599
- BarretoMLPereiraSMFerreiraAABCG vaccine: efficacy and indications for vaccination and revaccinationJ Pediatr (Rio J)2006823 SupplS45S5416826312
- DüppreNCCamachoLAda CunhaSSEffectiveness of BCG vaccination among leprosy contacts: a cohort studyTrans R Soc Trop Med Hyg2008102763163818514242
- CunhaSSAlexanderNBarretoMLBCG revaccination does not protect against leprosy in the Brazilian Amazon: a cluster randomised trialPLoS Negl Trop Dis200822e16718270542
- van BrakelWCrossHDeclercqEReview of leprosy research evidence (2002–2009) and implications for current policy and practiceLepr Rev201081322827521067065
- OharaNMatsuokaMNomaguchiHNaitoMYamadaTInhibition of multiplication of Mycobacterium leprae in mouse foot pads by recombinant Bacillus Catmette-Guérin (BCG)Vaccine200018141294129710618524
- OharaNMatsuokaMNomaguchiHNaitoMYamadaTProtective responses against experimental Mycobacterium leprae infection in mice induced by recombinant Bacillus Calmette-Guerin overproducing three putative protective antigen candidatesVaccine20011915–161906191011228360
- MakinoMMaedaYIshiiNImmunostimulatory activity of major membrane protein-II from Mycobacterium lepraeCell Immunol20052331536015885677
- MakinoMMaedaYInagakiKImmunostimulatory activity of recombinant Mycobacterium bovis BCG that secretes major membrane protein II of Mycobacterium lepraeInfect Immun200674116264627117057093
- GillisTPTulliusMVHorwitzMArBCG30-induced immunity and cross-protection against Mycobacterium leprae challenge are enhanced by boosting with the Mycobacterium tuberculosis 30-kilodalton antigen 85BInfect Immun20148293900390925001602
- GupteMDVallishayeeRSAnantharamanDSComparative leprosy vaccine trial in south IndiaIndian J Lepr199870436938810189587
- SreevatsaDesikanKVEvaluation of the efficacy of candidate vaccines against M. leprae infection in miceIndian J Lepr19886022522593192974
- BhideMBPradhanKSBapatCVA vaccine from ICRC bacilli against M. leprae infection in mouse foot-padLepr India1978503334344359922
- SharmaPMukherjeeRTalwarGPImmunoprophylactic effects of the anti-leprosy Mw vaccine in household contacts of leprosy patients: clinical field trials with a follow up of 8–10 yearsLepr Rev200576212714316038246
- RichardusRAAlamKPahanDFeenstraSGGelukARichardusJHThe combined effect of chemoprophylaxis with single dose rifampicin and immunoprophylaxis with BCG to prevent leprosy in contacts of newly diagnosed leprosy cases: a cluster randomized controlled trial (MALTALEP study)BMC Infect Dis20131345624088534
- GelberRHBrennanPJHunterSWEffective vaccination of mice against leprosy bacilli with subunits of Mycobacterium lepraeInfect Immun19905837117182407654
- NgamyingMSawanpanyalertPButrapornREffect of vaccination with refined components of the organism on infection of mice with Mycobacterium lepraeInfect Immun20037131596159812595485
- BrittonWJMartinEKamathATNeupaneKDRochePWImmunoprophylaxis against Mycobacterium leprae infection with subunit vaccinesLepr Rev2000Suppl 71S176S18111201878
- RochePWNeupaneKDFailbusSSKamathABrittonWJVaccination with DNA of the Mycobacterium tuberculosis 85B antigen protects mouse foot pad against infection with M. lepraeInt J Lepr Other Mycobact Dis2001692939811757171
- NomaguchiHMukaiTTakeshitaFEffect of hsp65 DNA vaccination carrying immunostimulatory DNA sequences (CpG motifs) against Mycobacterium leprae multiplication in miceInt J Lepr Other Mycobact Dis200270318219012483966
- GelberRHMehraVBloomBVaccination with pure Mycobacterium leprae proteins inhibits M. leprae multiplication in mouse footpadsInfect Immun19946210425042557927681
- NaitoMMatsuokaMOharaNNomaguchiHYamadaTThe antigen 85 complex vaccine against experimental Mycobacterium leprae infection in miceVaccine1999189–1079579810580191
- NgamyingMVarachitPPhaknilratPLevyLBrennanPJChoSNEffects of vaccination with several mycobacterial proteins and lipoproteins on Mycobacterium leprae infection of the mouseInt J Lepr Other Mycobact Dis2001691434511480318
- ColeSTEiglmeierKParkhillJMassive gene decay in the leprosy bacillusNature200140968231007101111234002
- DuthieMSSampaioLHOliveiraRMDevelopment and pre-clinical assessment of a 73 kD chimeric fusion protein as a defined sub-unit vaccine for leprosyVaccine201331581381923228811
- DuthieMSColerRNLauranceJDProtection against Mycobacterium leprae infection by the ID83/GLA-SE and ID93/GLA-SE vaccines developed for tuberculosisInfect Immun20148293979398525024362
- SchreuderPALibenDSWahjuniSVan Den BroekJDe SoldenhoffRA comparison of Rapid Village Survey and Leprosy Elimination Campaign, detection methods in two districts of East Java, Indonesia, 1997/1998 and 1999/2000Lepr Rev200273436637512549844
- OskamLSlimEBührer-SékulaSSerology: recent developments, strengths, limitations and prospects: a state of the art overviewLepr Rev200374319620514577464
- ReeceSTIretonGMohamathRML0405 and ML2331 are antigens of Mycobacterium leprae with potential for diagnosis of leprosyClin Vaccine Immunol200613333334016522774
- DuthieMSGotoWIretonGCUse of protein antigens for early serological diagnosis of leprosyClin Vaccine Immunol200714111400140817898185
- SampaioLHStefaniMMOliveiraRMImmunologically reactive M. leprae antigens with relevance to diagnosis and vaccine developmentBMC Infect Dis2011112621269435
- HungriaEMde OliveiraRMde SouzaALSeroreactivity to new Mycobacterium leprae protein antigens in different leprosy-endemic regions in BrazilMem Inst Oswaldo Cruz2012107Suppl 110411123283461
- GelukADuthieMSSpencerJSPostgenomic Mycobacterium leprae antigens for cellular and serological diagnosis of M. leprae exposure, infection and leprosy diseaseLepr Rev201182440242122439280
- MillerRAGorderDHarnischJPAntibodies to phenolic glycolipid-I during long-term therapy: serial measurements in individual patientsInt J Lepr Other Mycobact Dis19875546336363323367
- ChanteauSCartelJLCelerierPPlichartRDesforgesSRouxJPGL-I antigen and antibody detection in leprosy patients: evolution under chemotherapyInt J Lepr Other Mycobact Dis19895747357432681456
- MeekerHCSchuller-LevisGFuscoFGiardina-BecketMASersenELevisWRSequential monitoring of leprosy patients with serum antibody levels to phenolic glycolipid-I, a synthetic analog of phenolic glycolipid-I, and mycobacterial lipoarabinomannanInt J Lepr Other Mycobact Dis19905835035112205685
- PrakashKSehgalVNAggarwalREvaluation of phenolic glycolipid-I (PGL-I) antibody as a multidrug therapy (MDT) monitorJ Dermatol199320116208482747
- RadaEUlrichMAranzazuNA follow-up study of multibacillary Hansen’s disease patients treated with multidrug therapy (MDT) or MDT + immunotherapy (IMT)Int J Lepr Other Mycobact Dis19976533203279401484
- ChoSNCellonaRVVillahermosaLGDetection of phenolic glycolipid I of Mycobacterium leprae in sera from leprosy patients before and after start of multidrug therapyClin Diagn Lab Immunol20018113814211139208
- RochePWBrittonWJFailbusSSNeupaneKDTheuvenetWJSerological monitoring of the response to chemotherapy in leprosy patientsInt J Lepr Other Mycobact Dis199361135438326179
- DrowartAChanteauSHuygenKEffects of chemotherapy on antibody levels directed against PGL-I and 85A and 85B protein antigens in lepromatous patientsInt J Lepr Other Mycobact Dis199361129348326178
- DuthieMSHayMNRadaEMSpecific IgG antibody responses may be used to monitor leprosy treatment efficacy and as recurrence prognostic markersEur J Clin Microbiol Infect Dis201130101257126521544695
- DuthieMSOrculloFMAbbelanaJMaghanoyABalagonMFComparative evaluation of antibody detection tests to facilitate the diagnosis of multibacillary leprosyAppl Microbiol Biotechnol201610073267327526820649
- DuthieMSRaychaudhuriRTutterrowYLA rapid ELISA for the diagnosis of MB leprosy based on complementary detection of antibodies against a novel protein-glycolipid conjugateDiagn Microbiol Infect Dis201479223323924666703
- DuthieMSBalagonMFMaghanoyARapid quantitative serological test for detection of infection with Mycobacterium leprae, the causative agent of leprosyJ Clin Microbiol201452261361924478496
- CardosoLPDiasRFFreitasAADevelopment of a quantitative rapid diagnostic test for multibacillary leprosy using smart phone technologyBMC Infect Dis201313149724152601
- FreitasAAOliveiraRMHungriaEMAlterations to antigen-specific immune responses before and after multidrug therapy of leprosyDiagn Microbiol Infect Dis201583215416126233487
- RadaEDuthieMSReedSGAranzazuNConvitJSerologic follow-up of IgG responses against recombinant mycobacterial proteins ML0405, ML2331 and LID-1 in a leprosy hyperendemic area of VenezuelaMem Inst Oswaldo Cruz2012107Suppl 1909423283459
- StefaniMMGuerraJGSousaALPotential plasma markers of type 1 and type 2 leprosy reactions: a preliminary reportBMC Infect Dis2009917519473542
- DuthieMSGotoWIretonGCAntigen-specific T-cell responses of leprosy patientsClin Vaccine Immunol200815111659166518784342
- SampaioLHSousaALBarcelosMCReedSGStefaniMMDuthieMSEvaluation of various cytokines elicited during antigen-specific recall as potential risk indicators for the differential development of leprosyEur J Clin Microbiol Infect Dis20123171443145122076550
- OliveiraRMHungriaEMde Araújo FreitasASynergistic antigen combinations for the development of interferon gamma release assays for paucibacillary leprosyEur J Clin Microbiol Infect Dis20143381415142424619112
- GelukABiomarkers for leprosy: would you prefer T (cells)?Lepr Rev201384131223741878
- BoboshaKTangSTvan der Ploeg-van SchipJJMycobacterium leprae virulence-associated peptides are indicators of exposure to M. leprae in Brazil, Ethiopia and NepalMem Inst Oswaldo Cruz2012107Suppl 111212323283462