Abstract
Endemic to over 70 countries and resulting in 200 million infected individuals and 500,000 deaths each year, the Schistosoma trematode worm can result in multisystem morbidity. Bowel obstruction secondary to this parasite has previously been described, but we report the first case of schistosomiasis affecting the sigmoid colon and resulting in perforation in a male positive for human immunodeficiency virus.
Introduction
Schistosomiasis is a relatively common finding in patients in South Africa, and the intestinal, hepatic, and urinary sequelae of parasitic invasion are well documented.Citation1 Bowel obstruction has previously been reported in this patient population but, with the exception of a case from Kuwait of jejunal perforation,Citation2 a French case of rectal perforation,Citation3 and a case of sigmoid colonic obstruction resulting in perforation,Citation4 there are no recorded cases of large bowel perforation in an individual positive for human immunodeficiency virus (HIV) in the literature. We report an unusual cause of large bowel obstruction with associated perforation and discuss the etiology.
Case report
A 44-year-old HIV-positive South African male presented with a short history of symptoms consistent with large bowel obstruction. Initial imaging including a plain abdominal radiograph (), and a single contrast enema identified large bowel obstruction secondary to a stricturing lesion in the descending colon (). A tentative diagnosis of colonic malignancy was made. Due to the patient’s poor physical condition, a transverse colostomy was fashioned as a temporizing measure before optimizing the patient for definitive surgery.
Figure 1 Abdominal X-ray on presentation demonstrating dilated large bowel loops.

Figure 2 Single contrast enema identifying a stricturing lesion in the left colon.

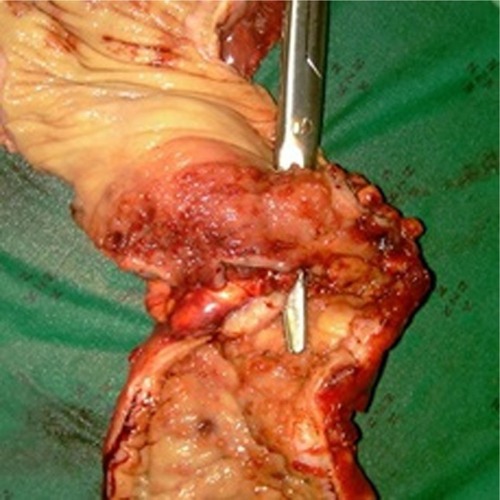
Computed tomography confirmed the presence of a left-sided colonic stricture, and bladder calcification was noted retrospectively (). Six weeks on from the original surgery, the patient returned in an improved physical state for an extended left hemicolectomy. Intraoperative findings were that of an inflammatory lesion involving the descending colon, with multiple vascular adhesions and a small localized perforation (). The lesion was resected, the colostomy left in situ, and the distal bowel stapled.
Figure 3 Computed tomography of pelvis.

Figure 4 Left colonic specimen with instrument outlining site of perforation.
Subsequent histopathology identified Schistosomiasis haematobium, with ova identified within the submucosa, evidence of fibrosis, and granulomatous colitis with a small localized perforation. Treatment with praziquantel was therefore implemented and the patient made an uneventful recovery.
Discussion
Predominantly affecting tropical and subtropical regions, schistosomiasis is transmitted by larvae-producing snails, with penetration of these larvae through the host’s skin. Pathogenic subclassification (S. mansoni, S. japonicum, S. haematobium) differs between geographical regions and will govern the clinical presentation.
Intestinal schistosomiasis can present in a number of ways, eg, acutely with bloody diarrhea, tenesmus, and/or abdominal pain, while chronic infection leads to granulomatous polyp formation,Citation5 bilharziomas, larger lesions, and stricture formation. Diagnosis is made by microscopic visualization of ova in stool or rectal mucosa, and can be treated with praziquantel or oxamniquine.Citation6
Stoever et alCitation7 suggested that the presence of S. haematobium, particularly in women, led to lesions affecting the external genitalia and therefore was a lasting entry point for HIV. They suggest that treatment of schistosomiasis can subsequently reduce the risk of contracting HIV. Speculation still exists regarding the exact role of coexisting HIV and schistosomiasis infection, and Secor and SundstromCitation8 suggest schistosomal infections create an immune environment that may accelerate HIV disease progression. However, further work is necessary to establish the effect on antiretroviral therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
- SchaferTHaleBGastrointestinal complications of schistosomiasisCurr Gastroenterol Rep2001329330311469998
- SinghNMannanAKahvicMJejunal perforation caused by schistosomiasisTrop Doct20104019119220555055
- ArgemiXCamusetGAbou-BakerARectal perforation caused by Schistosoma haematobiumAm J Trop Med Hyg20098017918119190208
- AtikFLopes FilhoGLinharesMLarge intestine obstruction complicated by perforation: A rare manifestation of Schistosoma mansoni infectionSao Paulo Med J1998116178117839951750
- SmithJSaidMKeladaAStudies on schistosomal rectal and colonic polyposisAm J Trop Med Hyg1977268084842787
- SaconatoHAttalahAInterventions for treating Schistosoma mansoniCochrane Database Syst Rev19993CD000528
- StoeverKMolyneuxDHotezPHIV/AIDs, schistosomiasis and girlsLancet200937320252026
- SecorWSundstromJBelow the belt: New insights into potential complications of HIV-1/schistosome coinfectionsCurr Opin Infect Dis20072051952317762787