
Abstract
Typhoid vaccines have been available as a means of disease control and prevention since 1896; however, their use as a routine tool for disease prevention in endemic settings has been hampered because of: 1) insufficient data on disease burden particularly regarding the lack of health care access in the poorest communities affected by typhoid; 2) limitations of the typhoid vaccine, such as shorter duration of protection, moderate efficacy in young children, and no efficacy for infants; 3) inadequate evidence on potential economic benefits when used for a larger population; 4) neglect in favor of alternative interventions that require massive infrastructure; 5) no financial support or commitment regarding vaccine delivery cost; 6) ambivalence about whether to invest in water and sanitation hygiene versus the vaccine; and 7) clarity on global policy for country adoption. If current typhoid-protein conjugate vaccines live up to their promise of higher efficacy, longer duration of protection, and efficacy in young children, typhoid vaccine use will be a critical component of short- and medium-term disease control strategies. Typhoid control could be accelerated if the global framework includes plans for accelerated introduction of the conjugate typhoid vaccine in developing countries.
Introduction
Three-fourths of the world’s population remains at risk of contracting enteric fever.Citation1 Salmonella enterica serovar typhi (S. typhi) and S. enterica serovar paratyphi (S. paratyphi) A and B cause enteric fever, a febrile illness specific to humans.Citation2 The genus Salmonella belongs to the family of Enterobacteriaceae and are Gram-negative, nonspore-forming, facultative anaerobic bacilli.Citation3 Of the paratyphoid group, S. paratyphi A is the most common serovar in Asia, with a few instances when S. paratyphi B strain rates were higher for paratyphoid fever.Citation4,Citation5 The other serotype of the Salmonella genus is nontyphoidal Salmonellae, which infect a variety of hosts and are frequently zoonotic.Citation6
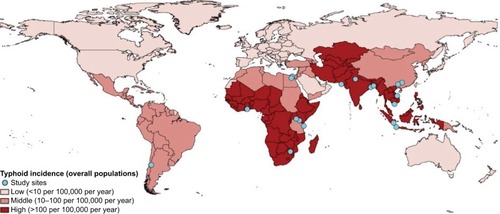
Typhoid fever, the major contributor to global enteric fever burden, is a systemic infection contracted through the ingestion of contaminated water or food.Citation7,Citation8 Prior to the discovery of antibiotics and scaling up of water treatment methods, typhoid fever was a major cause of mortality worldwide. Currently, it remains a significant cause of illness and death in developing countries where access to safe water and basic sanitation is significantly compromised.Citation9–Citation11 Asian and African countries report the largest share of global typhoid cases.Citation1,Citation12,Citation13 The burden of disease in Asia is well documented, and a recent multinational African study found a significant burden in Africa as well.Citation14 Children, those between the ages of two and four being the most vulnerable, are at far greater risk in typhoid-endemic countries such as Bangladesh, India, Nepal, and Pakistan.Citation15–Citation17 Typhoid and paratyphoid fever incidence rates vary between and within countries from 6/100,000 to 1173/100,000 persons per year ().Citation18–Citation20 These variations can be explained primarily by differences in access to clean water and sanitation, as well as population prevalence of chronic carriers, baseline immune status, and cultural norms (such as dietary habits).Citation11
Figure 1 Burden of typhoid fever in low-income and middle-income countries.
Typhoid fever can be treated with antibiotics. However, treatment as an alternative to prevention has proven ineffective. Antibiotic resistance has negated the efficacy of many frontline antibiotics.Citation21,Citation22 Treatment may not prevent chronic carriage, which, in turn, perpetuates disease transmission. Many people in resource-poor settings do not have ready access to health care services. Finally, delayed treatment can result in fatal disease outcomes, which include intestinal bleeding, intestinal perforation, and neurological complications, such as delirium and hallucination.Citation2,Citation23 For these reasons, prevention primarily with vaccines remains preferable to focusing on treatment.
Disease prevention and the role of typhoid vaccines
The countries where economic development resulted in improved supply of clean drinking water and sanitation facilities have been able to control typhoid fever transmission substantially.Citation24 The development of sewage and supplies of piped water in many urban settings decreased the incidence of typhoid fever in the early twentieth century in North America and Europe. In many countries in Asia and Africa, typhoid is still highly endemic. As witnessed in the past, the control of typhoid fever in endemic countries will continue to be challenged by lack of water and sanitation infrastructural improvements primarily because of the costs involved.Citation25 Like all developing countries, lack of financial resources and low prioritization of water and sanitation in typhoid-endemic countries constrain the water, sanitation, and hygiene (WASH) maintenance and expansion.Citation26 Lack of accountability, corruption, and inefficient management has hampered the expansion of services, if any, in these countries. Among all the regions that are typhoid endemic, the millennium development goal for safe drinking water and hygiene was not met, an indication of the challenges that these countries face in improving access to WASH.Citation10
History of vaccine use
Vaccination is an effective prevention tool for typhoid fever, especially when coupled with hand washing and household water treatment.Citation27 Inactivated phenol-preserved whole-cell typhoid vaccine was developed during the 1890s. Although production was poorly standardized, the vaccine was associated with reduction in typhoid fever incidence in British and US soldiers.Citation28–Citation30 Subsequently, the vaccine was used in public health programs in many countries; however, a high level of reactogenicity occurred including fever (up to 30% of the vaccinees), headache (up to 10%), and severe local pain (up to 35%), which led to its removal from routine vaccination programs.Citation31–Citation33 However, the adverse effects associated with the vaccine and availability of antimicrobial treatment (chloramphenicol) in 1949 affected widespread use of the vaccine.Citation34,Citation35 In the early 1960s, when S. typhi strains resistant to chloramphenicol were isolated, typhoid vaccine development again garnered interest.Citation36 Over time, improved vaccine formulations have become available, including an oral live-attenuated formulation, injectable polysaccharide vaccine, and more recently, injectable typhoid conjugate vaccines with improved safety and efficacy profile.Citation37,Citation38
Currently licensed vaccines
Adverse effects associated with the whole-cell killed vaccine, directed vaccine development efforts at improving the vaccine safety profile. The injectable Vi polysaccharide and oral live-attenuated Ty21a vaccines developed during the 1990s are safe with minimal side effects. The overall protective efficacy for a three-dose regimen of the oral typhoid vaccine ranged between 67% and 80% in large-scale efficacy trials, conducted during the 1980s in Chile.Citation39–Citation41 Two different formulations were tested in typhoid-endemic regions of Indonesia in a randomized, double-blind trial design.Citation42 The protective efficacies of the liquid and enteric-coated formulations were 53% and 42%, respectively. The most common adverse events reported with Ty21a were mild and transient gastrointestinal disturbances, followed by general symptoms such as fever.Citation33 Only a limited and transient level of shedding in the stools of volunteers was seen with Ty21a and no person-to-person transmission was observed.Citation39
The injectable Vi polysaccharide vaccine is given in a single dose and was found to be well tolerated and to confer 64%–72% protection for 17–21 months and 55% over 3 years. The protection conferred and immunological response to the vaccine were consistent both in populations of endemic and nonendemic areas.Citation43–Citation47 The most common side effects are pain, redness and induration at injection site, and fever. In very rare cases, allergic reactions and rashes have been observed.Citation48
The current World Health Organization (WHO) position paper recommends the programmatic use of typhoid vaccines in endemic areas and for outbreak control.Citation27 Despite this, the injectable Vi polysaccharide vaccine has been used in routine immunization programs only in China, Vietnam, and India.Citation49 A properly designed randomized trial has not been conducted in these settings. Available government data from China and Vietnam suggest a significant reduction in the burden of typhoid fever in these settings.Citation49 While burden reductions could have occurred because of factors other than the vaccine, the concurrent rise in disease caused by S. paratyphi, which has the same transmission routes as typhoid, suggests that this was not the case.
Two primary reasons exist for the limited scale of vaccine use including: 1) reduced or no immunogenicity in younger children and infants; and 2) duration of protection only up to 3 years for polysaccharide vaccine and 7 years for oral live vaccine, which, in turn, requires repeat doses and alternative platforms for vaccine delivery. To address these challenges, typhoid conjugate vaccine development was initiated at the US National Institutes of Health (NIH) in the 1980s based on a recombinant vaccine that used exoprotein A from Pseudomonas aeruginosa. The expectation from typhoid conjugate vaccines is that the vaccination of infants and young children will result in protection that endures through the high-risk preschool and school-age years and that it addresses other challenges faced with the improving use of oral and polysaccharide vaccines.Citation50 The safety and efficacy data of US NIH typhoid conjugate vaccine were published in 1999.Citation51,Citation52 The vaccine is highly immunogenic in young infants, provides long-term protection, and is safe.Citation53 Following on the footsteps of US NIH, there are currently 11 manufacturers working on the development of a toxoid conjugate vaccine (TCV) globally (), including a model of technology transfer to developing country vaccine manufacturers, so that low-cost vaccines are accessible to the populations that would benefit most from their production (GlaxoSmithKline and International Vaccine Institute programs). Two vaccine manufacturers in India have acquired a marketing license for a TCV. Both vaccines are sold in the Indian private market. Despite this notable progress, development of a better vaccine will not necessarily result in widespread use and resultant large impact on typhoid burden. For this to occur, many barriers must be overcome as described subsequently.
Table 1 Pipeline of the development of enteric fever vaccines
Scaling up typhoid vaccine use: barriers or facilitators?
The fundamental knowledge needed to support vaccine introduction or scale-up of any intervention relates to burden of disease, vaccine safety, effectiveness of vaccination, financial implications, value for money invested compared to alternative choices, capacity of immunization systems, and operationalization of a comprehensive communication and advocacy strategy to garner a political will at national and global levels.Citation54
Disease burden
Accurate assessment of typhoid disease burden remains a challenge.Citation13,Citation20 In resource-poor areas, health care access may be limited because of lack of referral, transportation, or the ability to pay for services. Once a person arrives at a health care facility, the outcome may not be suspected (e.g., in malaria-endemic areas where all fever is initially considered malaria), staff may not be available to collect a specimen, or blood culture supplies may not be available. In the laboratory, staff may be improperly trained, insufficient blood may be collected, blood culture has imperfect sensitivity and specificity, and patients may already have received antibiotics. Surveillance systems may be limited in scope – for example, focusing on urban areas – and thus not representative, a serious concern for a disease with wide variability in incidence and risk factors over time and place. Surveillance systems may also have imperfect criteria for triggering collection of a blood culture. While fever may be a relatively easy outcome to assess, complications of typhoid, such as intestinal perforation and out-of-hospital death, pose a substantial challenge for surveillance systems.
Advances have been made that address some of the above concerns. Novel diagnostic techniques that are currently being tested (e.g., sero-surveys based on polymerase chain reaction and antibody titers), once in routine practice, may allow for point-of-care documentation of typhoid, allow accurate testing even after antibiotic pretreatment, and improve on blood culture sensitivity. Insurance schemes in some countries have increased health care access. Risk factor-based modeling that extrapolates from one epidemiological setting to another has been used, but it does not present a compelling case for vaccine introduction in a country because of poor availability and representativeness of local data.
Limited and inaccurate disease burden estimates seriously hamper national and international decision-making regarding typhoid vaccine. Ministry of Health and immunization personnel require multisite/multiregion data from within a country to trigger an introduction decision and convince other ministries (i.e., ministry of finance) to finance such endeavors. The distribution of disease within the country and regions is necessary to target groups for vaccination and to choose the optimal vaccination schedule. Documentation of severe disease, complications, and death is necessary for typhoid vaccine to compete with other health care priorities.
Typhoid vaccine safety, efficacy, and effectiveness
For oral and injectable typhoid vaccines, safety, efficacy, and effectiveness are well documented. These vaccines cannot be given to children below 2 years and revaccination every 3 years (for polysaccharide vaccine) or 5–7 years (for Ty21a vaccine) is necessary. Ineffectiveness in young children and requirement for booster doses limit the public health utility of these vaccines, issues that should be solved by TCV. However, unlike earlier vaccines, a WHO expert consultation in 2014 identified many knowledge gaps for TCV, including lack of clinical efficacy data, especially in <2 years of age; immune duration; availability of adequate postlicensure safety data; and lack of demonstration studies to guide public health use. This information is critical for the large-scale use of the vaccine, and its absence has further delayed vaccine introduction.
These issues could be addressed by a multicenter effectiveness study that includes nested immunogenicity assessments and separate trial arms to evaluate effectiveness in young children. The Bill & Melinda Gates Foundation has recently received requested proposals to conduct just such evaluations. It will take several years for the results to be available and used for decision making.
Economic analyses and vaccine financing
A major criterion for policy makers in adopting new vaccination is its value for money. Health economic evaluations such as rigorous cost-effectiveness analysis need to be conducted for typhoid conjugate vaccines. The primary reason for the lack of studies is absent data that would inform these evaluations, including: 1) unknown duration of protection and level of effectiveness of TCV; 2) ill-defined vaccination strategies; 3) poorly defined incidence for all, severe, and fatal typhoid, as well as the impact of antibiotic resistance on these outcomes; 4) poorly defined impact of typhoid on non-illness outcomes such as school absenteeism and lost work; 5) incomplete cost information such as that for illness, treatment, vaccines, and immunization delivery; and 6) poor understanding of the role of chronic carriers and their impact on disease transmission risk, despite public vaccination. For example, while it is known that the cost of illness per episode of typhoid fever in some settings is the highest for 2–5-year-old children and both hospitalization and antimicrobial resistance increase the cost of illness, data for other settings are lacking.Citation55
Financing of typhoid vaccines has been a major bottleneck in country adoption. Many typhoid-endemic countries are low-income ones and eligible for support from Gavi, the vaccine alliance. Gavi, however, has withheld a decision to support the existing typhoid vaccines while waiting for WHO prequalification.Citation56 This support window will continue until Gavi determines its next vaccine investment strategy in 2018 where the financing decision will be reevaluated based on other competing uses for funding, including other new vaccines. In most of the new vaccine introductions, financial support from Gavi and strong recommendations from WHO on the need and benefits of vaccine have resulted in public sector vaccine introduction. It is, thus, encouraging that during 2016, WHO started a process of updating its policy recommendations by establishing a working group on typhoid vaccine.Citation57 Even if Gavi provides support for vaccination, this will not address all concerns because such funding is restricted to the period during which a country is below a poverty threshold, after which it enters a transition to full country funding of vaccines. As few countries to date have completed full transition, it is uncertain whether this process will lead to countries eliminating some vaccines from public programs. In addition, typhoid may occur in relatively poor areas of non-Gavi-eligible countries, that is not in current global debate for TCV roll out.
Vaccine and programmatic costs
Vaccine price is a major concern for all vaccines. A low-income country is unlikely to be able to afford the purchase of new vaccine unless provided with external support, such as through Gavi, despite many of these countries experiencing endemic typhoid. Similarly, Gavi-graduating and middle-income countries may have severely constrained immunization program budgets. It is possible that bulk purchase and pooled procurement mechanisms could lead manufacturers to offer a lower sales price. However, data on this hypothesis are lacking because national and subnational purchase prices are not generally made public. Furthermore, vaccine prices in the past have remained relatively high until multiple manufacturers have entered the market. Even if these mechanisms could lead to lower prices, they require substantial organizational capacity such as that provided by the Pan American Health Organization in Latin America, which has to date been lacking for typhoid vaccine.
With expectation of WHO prequalification, the TCV is on the Gavi priority list for funding considerations until 2018. Once a WHO-prequalified typhoid conjugate vaccine is available, Gavi will likely invite country application for supporting typhoid vaccination. The next Gavi funding window for country support of new vaccines will be the 2019–2023 cycle and TCV will be reevaluated in 2018 for continuation of financing. If Gavi elects to include typhoid vaccine in its investment portfolio, it will still need to come to an agreement with the manufacturers on price.
Beyond vaccines, countries and donors will need to consider the programmatic costs of incorporating typhoid vaccine into public immunization programs. For example, the immunization supply chain and national immunization program staff, space, and infrastructure in many instances are at capacity because of other new vaccine introductions, so adding new vaccines may require new investments.
Vaccine prioritization
Persons living in developing countries face high infectious disease risk throughout their lifespan, and many of these infectious diseases have become vaccine preventable. Consequently, governments must prioritize which vaccines to introduce and in which order. Numerous factors enter into this decision, including disease burden, outbreak or epidemic potential, impact on health care utilization and disruption, availability of other interventions for disease control, economic implications, availability of external funding (e.g., through Gavi), recommendations from national immunization technical advisory groups, and political considerations.
Preference to incorporate new vaccine into routine Expanded Program on Immunization
Governments usually have a preference for introducing new vaccines through existing Expanded Program on Immunization (EPI) systems because this minimizes the programmatic costs associated with vaccine introduction. Regardless of the typhoid vaccine used, public health programs will likely target persons other than mothers and infants, the traditional target groups for EPI vaccines. For example, in many countries, the peak incidence occurs among persons aged 9–12 years. This reality requires alternative approaches, which, in turn, can increase costs and programmatic challenges.
Despite this, successful examples exist already of vaccine introductions outside of traditional age ranges. If typhoid vaccine were to be delivered during adolescence, immunization program leads could learn from the example of human papillomavirus (HPV) vaccine, which has been delivered through school-based programs and community outreach. If vaccine was delivered in mass campaigns (followed by, e.g., routine infant immunization), lessons could be learned from the successful introduction of yellow fever and serogroup A meningococcal conjugate vaccines in West Africa.
The typhoid fever vaccines have similar challenges to yellow fever, meningitis, and HPV vaccines when it comes to vaccine delivery strategy. The vaccine efficacy below 5 years of age for Vi vaccines is not clear, and the disease distribution is geographic. The introduction in EPI is much easier when a vaccine schedule could be the same as the existing vaccines (pentavalent vaccine introduction). This has not been the case for typhoid so far. The expectation for the conjugate vaccine is that this may be given with the measles vaccines, overcoming the barriers for an alternative plan.
Policy factors: what generates political will?
Global: strong and clear recommendations, donor commitment
There are no current policy recommendations to use conjugate vaccines in the control of typhoid fever. Although other available vaccines are recommended for typhoid control in the WHO position paper,Citation23 global policies often do not percolate downwards to regions or countries, to provide clear guidance on a policy framework for vaccine use. Such clarity would support not only country decision-making but also provide donors the information needed to deliver efficient, evidence-based support.
Competing priorities/focus on broader context (e.g., child survival)
Vaccines have to compete with other health priorities for financing within health ministries, which themselves have to compete with other ministries for financing. Choosing from multiple competing alternative financing choices is complex and often politically charged rather than strictly evidence based. Where an evidence-based approach is used, vaccines usually demonstrate a high return on investment. This is particularly true when the full public health value of a vaccine is tallied. In the case of typhoid vaccines this would include not only direct reduction in morbidity and mortality but indirect protection of unvaccinated persons, reduction in antibiotic use and antibiotic resistant organisms, reduction or elimination of outbreaks and the health care delivery distortions these entail, economic consequences from loss of business or tourism when an outbreak occurs, reduced risk of household impoverishment because of the cost of health care for typhoid, and reduction in health inequities and the moral capital this provides.
Conclusion
Typhoid fever is a preventable disease. However, it continues to affect many populations across the globe. The highest burden of disease occurs in settings with prevailing low socioeconomic development and insufficient clean water, sewage and water management systems, and sanitary practices as well as other social risk factors, including population displacement, civil strife, and natural catastrophes.
A global strategy to reduce typhoid disease burden needs to consider the introduction of currently available typhoid vaccines, particularly conjugate vaccines. For typhoid conjugate vaccines to have an impact in the short term on disease incidence, vaccination coverage levels will need to reach high levels in at-risk populations – including young children – which, in turn, will require a public program delivered through national immunization programs.
Disclosure
The authors report no conflicts of interest in this work.
References
- MogasaleVMaskeryBOchiaiRLBurden of typhoid fever in low-income and middle-income countries: a systematic, literature-based update with risk-factor adjustmentLancet Glob Health2014210e570e58025304633
- ParryCMHienTTDouganGWhiteNJFarrarJJTyphoid feverN Engl J Med2002347221770178212456854
- MurrayPRosenthalKKobayashiGPfallerMMedical Microbiology5th edSt Louis, MIMosby Elsevier Science2005
- MeltzerEStienlaufSLeshemESidiYSchwartzEA large outbreak of Salmonella paratyphi A infection among Israeli travelers to NepalClin Infect Dis201458335936424198224
- KarkeyAThompsonCNThieuNTVDifferential epidemiology of Salmonella typhi and paratyphi A in Kathmandu, Nepal: a matched case control investigation in a highly endemic enteric fever settingPLoS Negl Trop Dis201378e239123991240
- GordonMAInvasive nontyphoidal Salmonella disease: epidemiology, pathogenesis and diagnosisCurr Opin Infect Dis201124548448921844803
- KhanMIOchiaiRLSoofiSBRisk factors associated with typhoid fever in children aged 2–16 years in Karachi, PakistanEpidemiol Infect2012140466567221676350
- KarkeyAJombartTWalkerAWThe ecological dynamics of fecal contamination and Salmonella typhi and Salmonella paratyphi a in municipal Kathmandu drinking waterPLoS Negl Trop Dis2016101e000434626735696
- WHO/UNICEF Joint Water Supply, Sanitation Monitoring Programme, World Health OrganizationProgress on Drinking Water and Sanitation: 2014 UpdateGeneva, SwitzerlandWorld Health Organization2014
- SatterthwaiteDMissing the millennium development goal targets for water and sanitation in urban areasEnviron Urban201628199118
- WrightJGundrySConroyRHousehold drinking water in developing countries: a systematic review of microbiological contamination between source and point-of-useTrop Med Int Health20049110611714728614
- CrumpJAUpdating and refining estimates of typhoid fever burden for public health actionLancet Glob Health2014210e551e55325304622
- CrumpJARamPKGuptaSKMillerMAMintzEDPart I. Analysis of data gaps pertaining to Salmonella enterica serotype Typhi infections in low and medium human development index countries, 1984–2005Epidemiol Infect2008136443644817686194
- von KalckreuthVKoningsFAabyPThe Typhoid Fever Surveillance in Africa Program (TSAP): clinical, diagnostic, and epidemiological methodologiesClin Infect Dis201662Suppl 1S9S1626933028
- SinhaASazawalSKumarRTyphoid fever in children aged less than 5 yearsLancet1999354918073473710475185
- BrooksWAHossainAGoswamiDBacteremic typhoid fever in children in an urban slum, BangladeshEmerg Infect Dis200511232632915752457
- KhanMISoofiSBOchiaiRLEpidemiology, clinical presentation, and patterns of drug resistance of Salmonella typhi in Karachi, PakistanJ Infect Dev Ctries201261070471423103892
- BreimanRFCosmasLNjugunaHPopulation-based incidence of typhoid fever in an urban informal settlement and a rural area in Kenya: implications for typhoid vaccine use in AfricaPloS One201271e2911922276105
- SrikantiahPGirgisFYLubySPPopulation-based surveillance of typhoid fever in EgyptAm J Trop Med Hyg200674111411916407354
- MogasaleVMogasaleVVRamaniERevisiting typhoid fever surveillance in low and middle income countries: lessons from systematic literature review of population-based longitudinal studiesBMC Infect Dis2016163526822522
- ZakiSAKarandeSMultidrug-resistant typhoid fever: a reviewJ Infect Dev Ctries20115532433721628808
- NeilKPSodhaSVLukwagoLA large outbreak of typhoid fever associated with a high rate of intestinal perforation in Kasese district, Uganda, 2008–2009Clin Infect Dis20125481091109922357703
- World Health OrganizationBackground Document: The Diagnosis, Treatment and Prevention of Typhoid Fever Vol WHO/V&B/03.07Geneva, SwitzerlandWorld Health Organization2003
- CutlerDMillerGThe role of public health improvements in health advances: the twentieth-century United StatesDemography200542112215782893
- HuttonGBartramJGlobal costs of attaining the millennium development goal for water supply and sanitationBull World Health Organ2008861131918235885
- MontgomeryMAElimelechMWater and sanitation in developing countries: including health in the equationEnviron Sci Technol2007411172417265923
- World Health OrganizationTyphoid vaccines: WHO position paperWkly Epidemiol Rec2008836495918260212
- HawleyPRSimmonsJSThe effectiveness of vaccines used for the prevention of typhoid fever in the United States army and navyAm J Public Health Nations Health193424768970918014010
- SilerJFDunhamGCDuration of immunity conferred by typhoid vaccine: results of re-vaccination by intracutaneous injection of typhoid vaccineAm J Public Health Nations Health19392929510318014993
- WrightAEVaccine therapy-its administration, value, and limitationsProc R Soc Med19103Gen Rep138
- WahdanMHSippelJEMikhailIAControlled field trial of a typhoid vaccine prepared with a nonmotile mutant of Salmonella typhi Ty2Bull World Health Organ197552169731082383
- IvanoffBLevineMMLambertPHVaccination against typhoid fever: present statusBull World Health Organ19947269579717867143
- EngelsEABennishMLFalagasMELauJTyphoid fever vaccinesVaccine200018151433143410733438
- MurtiBRRajyalakshmiKBhaskaranCSResistance of Salmonella typhi to chloramphenicol. I. A preliminary reportJ Clin Pathol19621554455113936803
- WoodwardTESmadelJEPreliminary report on the beneficial effect of chloromycetin in the treatment of typhoid feverAnn Intern Med194829113113418869867
- HejfecLBLevinaLASalminLBControlled field trials of killed oral typhoid and paratyphoid B vaccines and cell-free, chemical aerosol typhoid vaccineDev Biol Stand1976339397821803
- MartinLBVaccines for typhoid fever and other salmonellosesCurr Opin Infect Dis201225548949922825288
- FraserAPaulMGoldbergEAcostaCJLeiboviciLTyphoid fever vaccines: systematic review and meta-analysis of randomised controlled trialsVaccine200725457848785717928109
- WahdanMHSerieCCerisierYSallamSGermanierRA controlled field trial of live Salmonella typhi strain Ty 21a oral vaccine against typhoid: three-year resultsJ Infect Dis198214532922957037982
- LevineMMFerreccioCBlackRELagosRSan MartinOBlack-welderWCTy21a live oral typhoid vaccine and prevention of paratyphoid fever caused by Salmonella enterica serovar Paratyphi BClin Infect Dis200745Suppl 1S24S2817582564
- LevineMMFerreccioCCryzSOrtizEComparison of enteric-coated capsules and liquid formulation of Ty21a typhoid vaccine in randomised controlled field trialLancet199033687208918941976928
- SimanjuntakCHPaleologoFPPunjabiNHOral immunisation against typhoid fever in Indonesia with Ty21a vaccineLancet19913388774105510591681365
- KlugmanKPGilbertsonITKoornhofHJProtective activity of Vi capsular polysaccharide vaccine against typhoid feverLancet198728569116511692890805
- KlugmanKPKoornhofHJRobbinsJBLe CamNNImmunogenicity, efficacy and serological correlate of protection of Salmonella typhi Vi capsular polysaccharide vaccine three years after immunizationVaccine19961454354388735556
- MirzaNBWamolaIAEstambaleBAMbithiEPoilletMTyphim Vi vaccine against typhoid fever: a clinical trial in KenyaEast Afr Med J19957231621647796767
- SurDOchiaiRLBhattacharyaSKA cluster-randomized effectiveness trial of Vi typhoid vaccine in IndiaN Engl J Med2009361433534419625715
- KhanMISoofiSBOchiaiRLEffectiveness of Vi capsular polysaccharide typhoid vaccine among children: a cluster randomized trial in Karachi, PakistanVaccine201230365389539522721899
- HesselLDeboisHFletcherMDumasRExperience with Salmonella typhi Vi capsular polysaccharide vaccineEur J Clin Microbiol Infect Dis199918960962010534182
- DateKABentsi-EnchillADFoxKKTyphoid Fever surveillance and vaccine use – South-East Asia and Western Pacific regions, 2009–2013MMWR Morb Mortal Wkly Rep2014633985586025275329
- PoddaASaulAJAroraRConjugate vaccines for enteric fever: proceedings of a meeting organized in New Delhi, India in 2009J Infect Dev Ctries20104640441120601795
- LinFYCHoVAKhiemHBThe efficacy of a Salmonella typhi Vi conjugate vaccine in two-to-five-year-old childrenN Engl J Med2001344171263126911320385
- KossaczkaZLinFYHoVASafety and immunogenicity of Vi conjugate vaccines for typhoid fever in adults, teenagers, and 2- to 4-year-old children in VietnamInfect Immun199967115806581010531232
- MaiNLPhanVBVoAHPersistent efficacy of Vi conjugate vaccine against typhoid fever in young childrenN Engl J Med2003349141390139114523155
- LevineOSHajjehRWeckerJA policy framework for accelerating adoption of new vaccinesHum Vaccin20106121021102421150269
- BahlRSinhaAPoulosCCosts of illness due to typhoid fever in an Indian urban slum community: implications for vaccination policyJ Health Popul Nutr200422330431015609783
- GAVI AllianceGAVI Alliance Board Meeting: final minutes2011 Available from: http://www.gavi.org/about/governance/gavi-board/minutes/2011/16-november/Accessed January 6, 2017
- World Health OrganizationImmunization, Vaccines and Biologicals: SAGE Working Group on Typhois Vaccines2016 Available from: http://www.who.int/immunization/policy/sage/sage_wg_typhoid_mar2016/en/Accessed January 6, 2017