
Abstract
With the universal adoption of antibiotic prophylaxis prior to prostate biopsy, the current risk of post-biopsy infection (including sepsis) is <2%. Preoperative prophylactic antibiotic regimens can vary, and although fluoroquinolones have emerged as the standard of care, there is no universally agreed upon preoperative antibiotic regimen. Recently, an increase in the proportion of postoperative infections caused by fluoroquinolone-resistant Escherichia coli (as well as other Enterobacteriaceae) has led to the exploration of simple, practical, and cost-effective methods to minimize this postoperative infection risk. We performed a prospective, nonrandomized, controlled study of preoperative rectal cultures to screen for rectal colonization with fluoroquinolone-resistant bacteria using ciprofloxacin-supplemented MacConkey agar culture media. To evaluate the feasibility and practicality of this test, one provider used the results of rectal swab cultures collected during the preoperative outpatient evaluation to adjust each patient’s preoperative antibiotic prophylaxis when fluoroquinolone-resistant enteric bacteria were detected, whereas two other providers continued usual preoperative care and empiric antimicrobial prophylaxis. Rectal colonization with fluoroquinolone-resistant bacteria was detected in 19/152 (12.5%) of patients. In our intention-to-treat analysis (N=268), the rate of post-biopsy sepsis was 3.6% lower in the group that was screened for rectal colonization with fluoroquinolone-resistant bacteria prior to transrectal prostate biopsy. The observed risk reduction in the rectal screening group trended toward, but did not achieve, statistical significance. We suggest that preoperative screening for rectal colonization with fluoroquinolone-resistant enteric bacteria may be a useful step toward mitigating post-prostate biopsy sepsis.
Introduction
Preoperative antimicrobial treatment has been demonstrated to decrease the incidence of postoperative infection following transrectal ultrasound-guided prostate biopsy, but definitive data regarding the length, number, and selection of antibiotics are lacking.Citation1 With the emergence of community-acquired infection and enteric colonization with multidrug-resistant gram-negative bacterial pathogens in the US, and in particular extended-spectrum β-lactamase-positive strains of Enterobacteriaceae and extremely drug resistant strains of carbapenemase-positive Klebsiella pneumonia (which spread from Israel to New York City over a decade ago and are now endemic throughout the US), concern has arisen about the adequacy of single antibiotic prophylaxis prior to prostate biopsy.Citation2-Citation4 Two recent studies (a single-center trial and a meta-analysis) argue for adding an extra empiric antibiotic agent to the standard fluoroquinolone prophylaxis to minimize the risk of severe infection associated with fluoroquinolone-resistant organisms following transrectal prostate biopsy.Citation5,Citation6 However, most fluoroquinolone-resistant Enterobacteriaceae (FQRE) are resistant to other drug classes in addition to fluoroquinolones, so selecting antibiotics that have reliable activity for empiric preoperative prophylaxis would need to be based on local antibiogram data as opposed to national guidelines or recommendations. Furthermore, in this current era of severe NAP1 Clostridium difficile infections, routine administration of two empiric preoperative antibiotics may be viewed as an unacceptable risk.Citation7
To examine the feasibility and practicality of focused, targeted (ie, non-empirical) preoperative antibiotic prophylaxis for men with documented rectal colonization with fluoroquinolone-resistant bacteria, we validated a pre-biopsy culture-based screening assay of rectal swabs for detection of FQRE using MacConkey agar plates supplemented with 1 μg/mL of ciprofloxacin. MacConkey agar with ciprofloxacin is US Food and Drug Administration-approved screening medium for the selective isolation of ciprofloxacin-resistant E. coli from clinical samples. Once the test was validated in the microbiology laboratory, we met with the urology group based at our academic teaching institution to inform them of the availability of this screening assay and its potential applications. Following this meeting, one of the three urologists in the group elected to begin routine screening of his/her patients prior to transrectal ultrasound-guided prostate biopsy (TRUPB) by collecting rectal swabs and submitting them to the laboratory for culture on the ciprofloxacin-supplemented MacConkey agar plates. The two other urologists in the group continued their previous practice of empiric ciprofloxacin 500 mg oral dosing twice daily starting 1 day prior to biopsy and continuing for 6 days after biopsy (7 days total). We aimed to determine if the pre-biopsy rectal swab influenced the therapy and decreased the post-biopsy infection rate above the standard, control group.
Methods
Approval was obtained from the University of Illinois College of Medicine and the OSF/Saint Francis Medical Center Institutional Review Boards (IRBs) to allow the protocol for tracking the results of the cultures of rectal swab specimens submitted to the microbiology laboratory from outpatients undergoing evaluation and treatment at the Order of Saint Francis Medical Center Medical Group (OSFMG) urology practice for prostate cancer screening. All men with rectal swab specimens collected between October 1, 2013, and October 31, 2014, were eligible for inclusion in the study in accordance with the study period proposed in the Institutional Review Board (IRB) protocol. The University of Illinois College of Medicine and Saint Francis Medical Center Institutional Review Boards waived the requirement to obtain informed consent from patients because all specimens were collected as part of the routine care of the patient and submitted to the microbiology laboratory by the treating physicians for screening cultures. Consequently, the patients seen by the other two physicians in the group constituted our IRB-approved control group.
All patients scheduled for transrectal ultrasound-guided prostate biopsy in the OSFMG urology office during the 13-month enrollment period were eligible for inclusion in this study. Patient age, gender, antibiotics received, prostate-specific antigen result, and pathologic findings on prostate biopsy were recorded. Patients already receiving antibiotic treatment (eg, patients with suspected prostatitis or patients with urinary tract infections); immunocompromised patients, patients on chemotherapy for treatment of malignancy, patients with HIV infection, and patients with a history of allergic or adverse reactions to fluoroquinolone antibiotics were excluded from this study.
OSFMG urology patients scheduled for TRUPB either consented to screening for colonization with FQRE or proceeded directly to TRUPB. All patients received oral ciprofloxacin pre-TRUPB antibiotic prophylaxis unless a FQRE was detected in culture from the screening rectal sample, in which case prophylaxis was guided by susceptibility test results for the isolate. All rectal swabs were submitted to the OSF system microbiology laboratory (Peoria, IL, USA) for screening for FQRE. The resistance screening assay used to detect rectal colonization with fluoroquinolone-resistant bacteria employed in this study targets all bacteria that are capable of growth on MacConkey agar media supplemented with 1 μM ciprofloxacin (Hardy Diagnostics, Santa Monica, CA, USA) and incubated in 5% CO2 at 37°C for 2 days. Rectal swabs collected from patients included in the study were plated directly onto the ciprofloxacin-supplemented MacConkey agar immediately following receipt in the laboratory. Following incubation of the agar plates in a 5% CO2 environment at 37°C for 48 hours, negative cultures were declared negative for growth (ie, “no growth”) for those samples with no evidence of bacterial growth on the media. Standard laboratory techniques also included automated identification of organisms recovered in culture which was performed with the aid of the VITEK 2 instrument (bioMérieux, Durham, NC, USA).
The study period encompassed 13 months from October 1, 2013, to October 31, 2014. All patients in both study cohorts were followed for at least six weeks from pre-operative evaluation. Sepsis was defined as inpatient hospitalization with evidence of infection within 30 days of TRUPB based on a positive blood culture or fever (T>38°C/100.4°F) plus one of the following: tachycardia (heart rate > 90 bpm), abnormal white blood cell (WBC) count (WBC<4,000 or >12,000 cells/mm3), or a positive urine culture. Vital signs, WBC count, and urine and blood culture results were recorded and included in the analysis for all study patients diagnosed with post-TRUBP sepsis.
We compared the risk of sepsis following TRUPB between the patients of the provider who employed rectal screening for colonization with FQRE to adjust preoperative antimicrobial prophylaxis (when necessary) prior to TRUPB versus the patients of the two providers who employed standard empiric antibiotic prophylaxis prior to TRUPB. Epi Info™, a public domain suite of interoperable software tools maintained by Centers for Disease Control, was employed for the statistical analysis.
Results
Between October 1, 2013, and October 31, 2014, 268 patients were seen in the OSFMG urology offices for preoperative evaluation prior to TRUPB. A preoperative rectal culture to screen for rectal colonization with FQRE was recommended to 152 patients by one provider. Only one patient refused to consent to rectal screening (). Rectal swabs were thus collected from 151 patients, and swabs were submitted to the microbiology laboratory for culture-based screens for resistance to fluoroquinolones (study group). Enterobacteriaceae grew on the selective MacConkey agar plates enriched with 1% ciprofloxacin (Hardy Diagnostics) from rectal swabs collected from 19 of the 151 patients. According to the intention-to-treat design, the prevalence of rectal colonization with FQRE in our study population was 12.5% (19/152). All 19 ciprofloxacin-resistant Enterobacteriaceae were identified in our laboratory as E. coli. Complete susceptibilities were performed on each isolate: 12/19 (63%) of the ciprofloxacin-resistant E. coli were susceptible to trimethoprim/sulfamethoxazole (TMP/SMX) and 7 were TMP/SMX resistant, but were cefuroxime susceptible.
Figure 1 Study design and patient allocation.
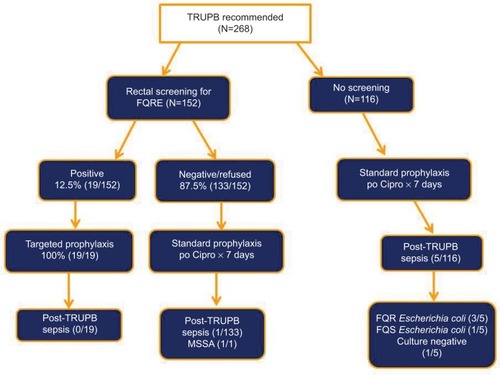
The 116 control patients from the two providers who did not screen patients for rectal colonization with FQRE all received ciprofloxacin 500 mg by mouth twice daily beginning 1 day prior to TRUPB and then for 6 days following TRUPB.
Ciprofloxacin was also the antimicrobial prophylaxis taken by the lone patient who refused preoperative rectal screening and the 132 patients who screened negative for rectal colonization with FQRE. Perioperative prophylactic antimicrobial treatment for the 19 men who tested positive for rectal colonization with FQRE was guided by the results of antimicrobial susceptibility testing performed in the OSF system microbiology laboratory.
For patients with FQRE rectal colonization and a TMP/SMX-susceptible E. coli isolate, the preferred prophylactic treatment regimen was TMP/SMX 160/800mg by mouth twice a day for 1 week beginning 1 day prior to TRUPB. Fifty-eight percent (11/19) of patients colonized with ciprofloxacin-resistant, TMP/SMX-susceptible E. coli satisfactorily completed the preferred prophylaxis. The preferred prophylactic treatment regimen for patients colonized by a TMP/SMX-resistant E. coli isolate was cefuroxime: 500 mg orally twice a day for 7 days beginning 1 day prior to TRUPB; 31.5% (6/19) of patients (the lone sulfa-allergic patient and 5/7 patients with cefuroxime-susceptible isolates) received cefuroxime for prophylaxis. Finally, 10.5% (2/19) of the patients received cephalexin 500 mg tabs orally 4 times a day for 7 days beginning 1 day prior to TRUPB and then for 6 days following TRUPB.
The study was designed as an intention-to-treat analysis. Patient age and prostate biopsy results for the two study groups are shown in , stratified by whether rectal screening for FQRE (152) versus usual care (116) was offered. There were no significant differences between the two groups in age or the prevalence of adenocarcinoma, carcinoma in situ, or benign tissue ().
Table 1 Comparison of mean age and carcinoma prevalence by patient group
Among the group that was not offered rectal screening (N=116), five patients (4.3%) developed signs and symptoms of postoperative infection that met our a priori criteria for post-biopsy sepsis. Three of five patients (60%) had growth of fluoroquinolone-resistant E. coli, one had infection with a fluoroquinolone-resistant species of Micrococcus, and one had growth of multiple organisms in urine culture (including E. coli) that were not fluoroquinolone resistant. None of the patients had positive blood cultures ().
Table 2 Risk of post-TRUPB sepsis by screening for rectal colonization with FQRE prior to TRUPB
One patient from the cohort patients who were offered screening but had no evidence of rectal colonization with FQRE (132/152) met the study criteria for post-biopsy sepsis. This patient grew a methicillin-susceptible Staphylococcus aureus (MSSA) in the culture of his urine that was resistant to ciprofloxacin, but no Enterobacteriaceae were isolated from his urine. MacConkey agar, a medium that is specifically designed to suppress the growth of gram-positive organisms, cannot detect rectal colonization with a fluoroquinolone-resistant MSSA because S. aureus does not grow on this media.
The risk of post-TRUPB sepsis was 0.0066 in the patient cohort that was offered pre-TRUPB rectal screening for FQRE, compared with 0.043 in the cohort that was not offered rectal screening for FQRE prior to TRUPB ().
Discussion
The risk of post-TRUPB sepsis was noticeably lower for the patient cohort that was offered pre-TRUPB screening for rectal colonization with FQRE (0.66% vs 4.3%), but the confidence intervals are large and the risk reduction (RR) did not achieve significance (p=0.08). Nonetheless, this was an intention-to-treat analysis of a study performed in a busy clinical practice, which suggests that the RR of 3.65% is achievable outside a controlled setting. Furthermore, the laboratory cost of the rectal culture to screen each patient was only US$13.52 (including laboratory manpower costs). The total laboratory cost of FQRE rectal screening for our study was US$2041.52 (one patient did not consent to screening). This translates to a cost of US$370.45 for every case of post-TRUPB sepsis that is prevented (number needed to screen = 27.4).
These data must be interpreted with caution. One might argue that the “real-world” practice setting of this study would suggest that our findings should translate well into daily clinical practice, but our patients were not randomized to pre-TRUPB rectal screening versus usual care. Although the two groups appear similar in , there may be inherent bias in patient selection that was not identified in this study. Also, our study is only suggestive of a potential benefit associated with rectal screening and adjustment of preoperative antimicrobial prophylaxis, as the difference in outcomes did not achieve statistical significance. It is also important to acknowledge a limitation to this screening methodology that was demonstrated by the lone case of post-TRUPB sepsis from the patient cohort that was offered screening for rectal colonization with FQRE. Rectal colonization with fluoroquinolone-resistant gram-positive organisms would not be expected to be detected with this screening methodology because gram-positive bacteria such as the S. aureus that caused our patient’s infection would not be recovered in culture on MacConkey agar, a medium that is specifically designed to suppress the growth of gram-positive organisms.
We have observed wider adoption of rectal screening for FQRE prior to TRUPB in our community, but ultimately several factors must be taken into consideration when weighing the pros and cons of adopting preoperative screening for rectal colonization with FQRE as a routine practice. These factors include the expense of the screening assays offered by the local microbiology laboratory, the regional prevalence of FQRE (prevalence varies by organism and region from 2% to 62%),Citation8 and the lack of randomized, controlled trial evidence of beneficial outcomes. In our community, where the cost of screening is reasonable, even with a low-to-moderate prevalence of FQRE in the region (12%), the risk–reward metrics do appear to favor preoperative collection of rectal swabs to screen for colonization with FQRE prior to TRUPB, to ensure that patients undergoing TRUPB receive effective perioperative antimicrobial prophylaxis.
Acknowledgments
We acknowledge the dedicated staff of the OSF system microbiology laboratory for their extraordinary commitment and, in particular, Lindsay O’Rourke for her assistance with validation of the rectal culture screening assay for detection of FQRE.
Disclosure
The authors report no conflicts of interest in this work.
References
- ZaniELClarkOARodrigues NettoNAntibiotic prophylaxis for transrectal prostate biopsyCochrane Database Syst Rev2011115CD006576
- YigitHQueenanAMAndersonGJNovel carbapenem-hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniaeAntimicrob Agents Chemother20014541151116111257029
- Centers for Disease Control and Prevention [webpage on the Internet]Antibiotic resistance threats in the United States, 2013 Available from: http://www.cdc.gov/drugresistance/threat-report-2013/Accessed December 7, 2017
- TumbarelloMVialePViscoliCPredictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapyClin Infect Dis20125594395022752516
- LuongBDanforthTVisnjevacOSurafMDuffMChevliKKReduction in hospital admissions with the addition of prophylactic intramuscular ceftriaxone before transrectal ultrasonography-guided prostate biopsiesUrology201585351151625596154
- YangLGaoLChenYProphylactic antibiotics in prostate biopsy: a meta-analysis based on randomized controlled trialsSurg Infect2015166733747
- WaltzPZuckerbraunBNovel therapies for severe Clostridium difficile colitisCurr Opin Crit Care201622216717326771898
- DalhoffAGlobal fluoroquinolone resistance epidemiology and implications for clinical useInterdiscip Perspect Infect Dis2012201297627323097666