
Abstract
Background
Bladder recurrence after nephroureterectomy (NU) is common. However, there is no acceptable policy of adjuvant intravesical treatment after NU.
Objective
To assess the rate of bladder recurrence following NU and to identify the high-risk subgroups that may become candidates for adjuvant intravesical therapy after NU.
Patients and methods
Ninety-one patients (mean age 66.4 years) underwent NU. High-grade (HG) tumors were found in 63 patients and low-grade (LG) tumors in 28. Median follow-up was 72 months. The risk of bladder recurrence was assessed by uni- and multivariate analyses of patient and tumor characteristics.
Results
Bladder recurrence developed in 38 patients (41.8%) after a median period of 11 months. Among these, 25 patients with HG upper tract urothelial carcinoma (39.7%) and 13 patients with LG upper tract urothelial carcinoma (46.4%) developed recurrence. HG bladder recurrence developed in 24 patients (63.2%) and LG recurrence developed in 14 patients (36.8%). Stages pTa, pT1, pT2, or higher bladder recurrence developed in 26 (68.4%), 7 (18.4%), and 4 patients (10.5%), respectively, and pure pTis developed in 1 patient. On uni- and multivariate analyses, the risk of bladder recurrence was independent of any clinicopathologic characteristics.
Conclusion
High rate and short time interval of bladder recurrence after NU were found, with no specific subgroup of patients with increased risk. These findings support prescribing adjuvant intravesical therapy to all patients after NU.
Introduction
Urothelial carcinoma (UC) is the fourth most common solid malignancy and the eighth most fatal malignancy in men.Citation1 Most UCs arise in the bladder, but 5%–10% arise in the upper urinary tract.Citation1,Citation2 Upper tract urothelial carcinoma (UTUC) poses diagnostic and therapeutic challenges: tissue-based diagnosis and follow-up are difficult compared to bladder cancer. The standard care in UTUC is nephroureterectomy (NU).Citation3,Citation4 Kidney preserving treatments are reserved for selected low-risk patients.Citation5
UCs are notorious for their high recurrence rate. After excision of a bladder cancer, up to 55% of the patients develop recurrence.Citation6 Following extirpative surgery for UTUC, 22%–47% of patients develop bladder recurrence.Citation1,Citation3,Citation5,Citation7–Citation9 Two main theories hypothesize to explain this high recurrence rate. The field cancerization theory suggests that multiplicity is due to carcinogenic exposure of the entire urothelium.Citation10,Citation11 The seeding theory claims for intraluminal seeding of a single progenitor cancerous cell.Citation1,Citation11–Citation13 With the emergence of a new molecular-based studies, the intraluminal seeding theory gained the spotlight, though both mechanisms probably coexist.Citation14
Following transurethral resection of bladder tumor, intravesical instillations of chemotherapy or immunotherapy are recommended according to the patient’s risk group: for low- or intermediate-risk patients, a single postoperative intravesical instillation of chemotherapy is advisable; in the intermediate-risk patients, chemotherapy or immunotherapy is recommended with maintenance therapy up to 1 year; and in high-risk patients, a 3-year maintenance protocol is recommended.Citation1,Citation15,Citation16 Currently, there are no established recommendations for adjuvant treatments after NU.
In this study, we estimated the rate of bladder recurrence following NU in an attempt to identify subgroups that are at a higher risk for this type of recurrence.
Patients and methods
Surgery and follow-up protocols
Surgery was done either openly or laparoscopically. In either way, a bladder cuff was removed. Tumors were staged according to the tumor node metastasis (TNM) classificationCitation17 and graded according to the World Health Organization classification.Citation18 Adjuvant intravesical treatment was not given to any patient. Follow-up was based on tumor grade. In patients with high-grade tumors, cystoscopy and urinary cytologic examination were done at 3-month intervals in the first year, at 6-month intervals for another 2 years, and annually for an additional 2 years. Annual ultrasonic examination of the urinary system was then done indefinitely. Computed tomography scan was performed at 6-month intervals for the first 3 years. For low-grade tumor, the same protocol was applied without computed tomography or cytology. Additional investigations were performed if clinically indicated. Patients included in the study were followed for at least 6 months or until disease recurrence or death. Median follow-up was 72 months (range 6–240 months). Data for all patients were available and none were lost to follow-up.
Data analysis
Disease-free and overall survival rates were calculated from the day of NU. The effect of the following parameters on recurrence and survival was assessed: age, gender, UTUC grade, stage, previous bladder UC, location in the urinary system, type of surgery (laparoscopic vs. open), and if diagnostic ureteroscopy was done prior to NU. A two-tailed p<0.05 was considered statistically significant. Vesical and extravesical tumor recurrences were analyzed separately. Statistical analysis was performed using SPSS v23.0 statistical software (IBM Corporation, Armonk, NY, USA) and Microsoft Excel 2016 (Microsoft Inc., Redmond, WA, USA).
The official institutional review committee which approved our study is the Ethics (Helsinki) Committee at Hadassah University Hospital for the conduct of clinical studies. The committee is in due compliance with the Public Health Regulations (Medical Experiments In Human Subjects) – 1980, the Governing Regulations of the Ministry of Health and the provisions of the current harmonized international guidelines for good clinical practice, namely, ICH-GCP. All data were kept secured with the relevant precautions. Committee approval number: HMO-16-0026. Patient consent was not required.
Results
Patients
Between January 1996 and December 2015, 91 patients (67 men and 24 women) underwent NU as the treatment of UTUC (). Mean patients’ age was 66.4 years (SD 11.24, range 40–86 years, median age 67). UTUC was located in the renal pelvis in 52 patients (57.1%) and in the ureter in 39 (42.9%) patients. Tumor stages were pTa and pT1 in 22 (24.2%) and 27 patients (29.7%), respectively, pT2 in 19 patients (20.9%), and pT3 in 23 patients (25.3%). Sixty-three patients (69.2%) had high-grade tumors and 28 (30.8%) had low-grade tumors. Twelve patients (12.8%) had prior bladder UC. Thirty-seven patients (39.4%) underwent diagnostic ureteroscopy before NU. Surgery was laparoscopic in 43 patients (47.3%) and open in 48 patients (52.7%). Ureteral margins were negative in all patients.
Table 1 Patients’ characteristics
Recurrence and survival
During follow-up, 51 patients (56.0%) were diagnosed with cancer recurrence. Among them, 38 (74.5%) had bladder recurrence, 23 (25.5%) had extravesical recurrence without bladder recurrence, and 10 (19.6%) had both extra- and intravesical recurrences.
A total of 30 patients (33%) died during follow-up, after a median period of 43 months after surgery. In 20 patients (66.7%), death was disease specific (after a median period of 36.5 months) and in 10 patients (33.3%), death was non-disease specific (after a median period of 70 months). Overall survival rate at 5 years was 72.5% and was associated with tumor grade (p<0.001) and patients’ age (p<0.05). High-grade tumor and advanced age were associated with lower survival rates with an odds ratio of 0.941 for every year, and having high-grade tumor had an odds ratio of 0.101. However, stage, previous ureteroscopy, gender, location, history of previous bladder cancer, and surgical approach showed no significant effect on overall survival.
Disease-specific survival rate was 79.9% and was not associated with age, gender, tumor location, and laparoscopic surgery, as opposed to open, location or previous bladder UC. Disease-specific survival rate was significantly lower among patients with high UTUC grade (p<0.001), advanced stage (p<0.001), and in the absence of previous ureteroscopy (p<0.05).
Bladder recurrence
Bladder recurrence occurred in 38 patients (41.8%) after a median period of 11 months (). Three-quarters of the recurrences occurred during the first year after NU and 91.67% occurred within 2 years. pTa bladder recurrence developed in 26 patients (68.4%), pT1 tumor in 7 patients (18.4%), pT2 tumor in 4 patients (10.5%), and 1 patient developed pure pTis. High-grade bladder recurrence developed in 24 patients (63.2%) and low-grade recurrence developed in 14 patients (36.8%). Twenty-five patients with high-grade UTUC (39.7%) developed bladder recurrence. Of these, 20 (80%) were high grade and 5 (20%) were low grade. Thirteen patients with low-grade UTUC (46.4%) developed bladder recurrence, including 9 patients (69.2%) with low-grade recurrence and 4 (30.8%) with high-grade recurrence. Bladder recurrence was fatal in nine patients (disease-specific rate 23.7%).
Figure 1 Bladder recurrence-free survival according to recurrence grade.
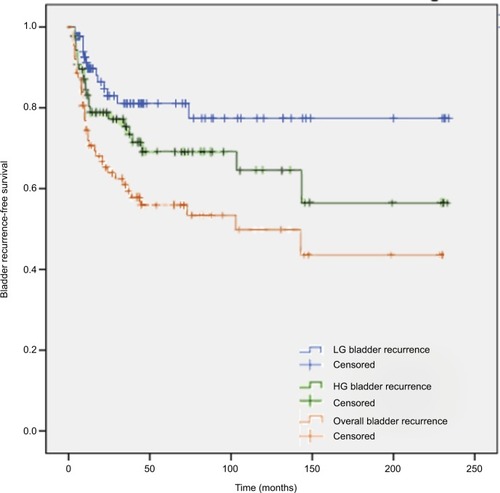
The risk of bladder recurrence after UTUC was independent of patients’ age, gender, UTUC grade, stage, location in the urinary system, surgery method, or the use of diagnostic ureteroscopy prior to NU in univariate analysis (). Bladder recurrence timing is depicted in . The treatment of bladder recurrence was as for primary bladder tumors and included transurethral resection and further therapy and follow-up according to the pathologic findings. Two patients underwent radical cystectomy with ileal conduit and two had non-operable disease upon diagnosis.
Table 2 Bladder recurrence univariate model
A binary logistic regression analysis was conducted to predict bladder recurrence using gender, age, grade, stage, location of tumor, surgical method, previous bladder cancer, and previous ureteroscopy. The full model was not found to be statistically significant in comparison to the model using constant only, indicating that the predictors as a set did not reliably distinguish patients with and without bladder recurrence (chi-square=11.011, p=0.201 with degrees of freedom=8).
Discussion
This work demonstrates the high frequency of bladder recurrence after NU, which developed in 41.8% of the patients after a median period of 11 months and was fatal in nine patients (disease-specific rate 23.7%). In the current study, none of the patients received adjuvant intravesical therapy. This may explain the high rate of bladder recurrence after NU. Bladder recurrence rate was independent of patients’ age, gender, UTUC grade, stage, location in the urinary system, and surgery type. Previous studies showed bladder recurrence rate of 22%–47% after NU. Various risk factors of bladder recurrence after NU that were reported in the past included gender, previous bladder cancer, preoperative chronic kidney disease, urinary cytology, location, multifocality, T stage, necrosis, laparoscopic approach, extravesical bladder cuff removal method, and surgical margins.Citation19,Citation20 None of these factors were found to be a risk factor in consensus.Citation19
This frequency of bladder recurrence after NU is similar to the frequency of recurrence after transurethral resection of bladder cancer (31%–78%).Citation8,Citation9,Citation21 Despite this similarity and its potential aggressive behavior, a well-established bladder adjuvant therapy protocol following NU has not been established. Several clinical trials have examined the efficacy of different protocols. Three large trials examined the effect of adjuvant intravesical therapy after NU.
The ODMIT-C trial was the first large-scale prospective, multicenter, randomized clinical trial addressing the efficacy of immediate adjuvant intravesical therapy after NU. A single postoperative intravesical dose of mitomycin C (MMC; 40 mg in 40 mL of saline; Kyowa, Hakko, Slough, UK) demonstrated an absolute risk reduction of 11% of bladder recurrence. Number needed to treat to prevent one bladder tumor was nine.Citation22 In another study including 196 patients, a significant vesical recurrence-free survival was demonstrated, but not in cancer-specific survival.Citation23 THP Monotherapy Study Group trial, which included 72 patients, demonstrated that intravesical instillation of pirarubicin within 48 hours after NU was associated with lower bladder tumor recurrence rates of 16.9% at 2 years vs. 42.2% at 2 years, with a hazard rate of 0.26.Citation24
Several systematic reviews and meta-analyses demonstrated the efficacy of prophylactic intravesical instillation chemotherapy for preventing bladder tumor recurrence after NU. These studies suggest a preventive effect with an odds ratio of 0.45–0.48 and a progression-free interval prolongation of 38%. Furthermore, the first instillation that begins within 24 hours after surgery was more effective compared to instillation at 48 hours or 2 weeks, and a single instillation had similar effect to multiple instillations.Citation25 Despite these findings that were reported in the years 2010–2013, immediate intravesical instillation of chemotherapy has not become a common practice. This is probably due to the fear from perivesical chemotherapy leak and its potential disastrous consequences.
In this study, we emphasize the high risk, the short time interval, and the absence of reliable predictive factors for bladder recurrence after NU. Thus, it seems reasonable to prescribe adjuvant intravesical therapy for most, if not all, patients after NU. This should be administered as if they had a resection of bladder tumor.
The main limitation of the study is its retrospective design. Despite the wide time range of follow-up, the follow-up and the treatment protocol were consistent and stable. Additionally, the effectiveness of adjuvant intravesical treatment recommended here is extrapolated from bladder cancer. There is no high-quality evidence in the literature to support it.
Conclusion
This study demonstrates the high frequency (41.8%), short time interval (median of 11 months), and substantial aggressive nature of bladder recurrence after NU. No specific subgroup of patients with higher risk of bladder recurrence was identified. Therefore, we suggest that adjuvant intravesical therapy be administered to all patients after NU, as is done after trans-urethral resection of bladder tumor.
Disclosure
The authors report no conflicts of interest in this work.
References
- Non-Muscle Invasive Bladder Cancer: American Urological Association Available from: http://www.auanet.org/education/guidelines/non-muscle-invasive-bladder-cancer.cfmAccessed June 15, 20164
- MunozJJEllisonLMUpper tract urothelial neoplasms: incidence and survival during the last 2 decadesJ Urol200016451523152511025695
- FangDLiX-SXiongG-YYaoLHeZ-SZhouL-QProphylactic intravesical chemotherapy to prevent bladder tumors after nephroureterectomy for primary upper urinary tract urothelial carcinomas: a systematic review and meta-analysisUrol Int201391329129623948770
- MargulisVShariatSFMatinSFUpper Tract Urothelial Carcinoma CollaborationThe Upper Tract Urothelial Carcinoma CollaborationOutcomes of radical nephroureterectomy: a series from the upper tract urothelial carcinoma collaborationCancer200911561224123319156917
- RouprêtMBabjukMCompératEEuropean association of urology guidelines on upper urinary tract urothelial carcinoma: 2017 updateEur Urol201873111112228867446
- LeblancBDuclosAJBénardFLong-term followup of initial Ta grade 1 transitional cell carcinoma of the bladderJ Urol199916261946195010569544
- ZigeunerREHuttererGChromeckiTRehakPLangnerCBladder tumour development after urothelial carcinoma of the upper urinary tract is related to primary tumour locationBJU Int20069861181118617125475
- NovaraGDe MarcoVDalpiazOIndependent predictors of metachronous bladder transitional cell carcinoma (TCC) after nephroureterectomy for TCC of the upper urinary tractBJU Int2008101111368137418241252
- XylinasERinkMMargulisVKarakiewiczPNovaraGShariatSFMultifocal carcinoma In situ of the upper tract is associated with high risk of bladder cancer recurrenceEur Urol20126151069107022402109
- MilláN-RodríGuezFChéChile-TonioloGSalvador-BayarriJHuguet-PéRezJVicente-RodríGuezJUpper urinary tract tumors after primary superficial bladder tumors: prognostic factors and risk groupsJ Urol200016441183118710992362
- HabuchiTMetachronous multifocal development of urothelial cancers by intraluminal seedingLancet19933428879108710888105314
- CattoJWFHartmannAStoehrRMultifocal urothelial cancers with the mutator phenotype are of monoclonal origin and require panurothelial treatment for tumor clearanceJ Urol200617562323233016697867
- HafnerCKnuechelRZanardoLEvidence for oligoclonality and tumor spread by intraluminal seeding in multifocal urothelial carcinomas of the upper and lower urinary tractOncogene2001203549104915 Available from: http://search.ebscohost.com/login.aspx?direct=true&profile=ehost&scope=site&authtype=crawler&jrnl=09509232&AN=8911021&h=ILJ1sWCVqqV3Sw9NbreemxkktylKW8OoniW5BwJrYkI35JgFThDZWj9lfXwnGF92ye%2FpdtM1QGUYG35RAfk94w%3D%3D&crl=cAccessed November 4, 201611521204
- TakahashiTKakehiYMitsumoriKDistinct microsatellite alterations in upper urinary tract tumors and subsequent bladder tumorsJ Urol2001165267267711176456
- BadalamentRAHerrHWWongGYA prospective randomized trial of maintenance versus nonmaintenance intravesical bacillus Calmette-Guérin therapy of superficial bladder cancerJ Clin Oncol1987534414493546618
- SylvesterRJOosterlinckWWitjesJAThe schedule and duration of intravesical chemotherapy in patients with non–muscle-invasive bladder cancer: a systematic review of the published results of randomized clinical trialsEur Urol200853470971918207317
- SobinLHGospodarowiczMKWittekindCTNM Classification of Malignant Tumours7th revised edHoboken, USAJohn Wiley & Sons2009
- Lopez-BeltranAGasserTHartmannATumours of the urinary systemEbleJNSauterGEpsteinJISesterhennIAWorld Health OrganisationClassification of Tumors Pathology and Genetics of Tumours of the Urinary System and Male Genital OrgansLyon, FranceIARC Press200488157
- Professionals S-OUpper Urinary Tract Urothelial Cell CarcinomaUroweb Available from: https://uroweb.org/guideline/upper-urinary-tract-urothelial-cell-carcinoma/?type=summary-of-changesAccessed June 15, 2016
- SeisenTGrangerBColinPA systematic review and meta-analysis of clinicopathologic factors linked to intravesical recurrence after radical nephroureterectomy to treat upper tract urothelial carcinomaEur Urol20156761122113325488681
- SylvesterRJvan der MeijdenAPMOosterlinckWPredicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trialsEur Urol200649346647716442208
- O’BrienTRayESinghRCokerBBeardRBritish Association of Urological Surgeons Section of OncologyPrevention of bladder tumours after nephroureterectomy for primary upper urinary tract urothelial carcinoma: a prospective, multicentre, randomised clinical trial of a single postoperative intravesical dose of mitomycin C (the ODMIT-C Trial)Eur Urol201160703–10 Eur Urol2012613e1421684068
- WuW-JKeH-LYangY-HLiC-CChouY-HHuangC-HShould patients with primary upper urinary tract cancer receive prophylactic intravesical chemotherapy after nephroureterectomy?J Urol20101831566119913833
- ItoAShintakuISatohMProspective randomized Phase II trial of a single early intravesical instillation of pirarubicin (THP) in the prevention of bladder recurrence after nephroureterectomy for upper urinary tract urothelial carcinoma: the THP monotherapy study group trialJ Clin Oncol201331111422142723460707
- WuPZhuGWeiDProphylactic intravesical chemotherapy decreases bladder tumor recurrence after nephroureterectomy for primary upper tract urothelial carcinoma: a systematic review and meta-analysisJ BUON20152051229123826537069