
Abstract
GreenLight laser™ photovaporization of the prostate (GLL-PVP) has become a valid alternative to traditional transurethral resection of the prostate (TURP) in men requiring surgery for benign prostatic hyperplasia. We aimed to review systematically the safety and efficacy of studies comparing GLL PVP and TURP in the medium-term. A comprehensive literature search was performed. Twelve studies were identified for meta-analysis. Meta-analyses showed a longer postoperative catheterization time (risk ratio (RR): 1.12, 95% CI:1.09–1.14, p<0.00001) and length of stay (RR: 1.16, 95% CI:1.12–1.19, p<0.00001) in the TURP group; higher risk of transfusion in the TURP group (RR: 6.51, 95% CI: 2,90–14,64 p<0.00001); no difference in the risk of urinary tract infections (RR: 0.83, 95% CI: 0.58–1.18, p=0.30) and transient re-catheterization (RR: 1.11, 95% CI: 0.76–1.60, p=0.60). Regarding reoperation rate, no difference was found in term of postoperative urethral stricture (RR: 1.13, 95% CI: 0.73–1.75, p=0.59) and bladder neck contracture (RR: 0.66, 95% CI: 0.31–1.40, p=0.28). A significantly higher incidence in reoperation for persistent/regrowth adenoma was present in the GLLL-PVP (RR: 0.64, 95% CI: 0.41–0.99, p=0.05). Data at 2-year follow-up showed significant better post-voiding residual (PVR) (MD: -1.42, 95% CI: -2.01, -0.82, p<0.00001) and International Prostate Symptom Score (IPSS) (MD: -0.35, 95% CI: -0.50, -0.20, p<0.00001) after TURP. No difference was found in the mean PVR at 2 years after TURP, in the mean maximum flow rate (Qmax) (MD: 0.30, 95% CI: -0.02–0.61, p=0.06) and quality of life QoL score (MD: 0.05, 95% CI: -0.02–0.42, p=0.13). At 5-year follow-up, data showed better IPSS (MD: -1.70, 95% CI: -2.45,-0.95, p<0.00001), QoL scores (MD: -0.35, 95% CI: -0.69, -0.02, p=0.04) and Qmax (MD: 3.29, 95% CI: 0.19–6.38, p=0.04) after TURP. Data of PVR showed no significant difference (MD: -11.54, 95% CI: -29.55–6.46, p=0.21). In conclusion, our analysis shows that GLL-PVP is a safer and more efficacious procedure than standard TURP in the early and medium-term. However, in the long term period GLL-PVP showed a higher incidence of reoperation rate due to incomplete vaporization/regrowth of prostatic adenoma.
Introduction
Lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) are among the most common complaints reported by adult males to their general practitioners. It is estimated that up to 50% of men over the age of 50 and 80% of men over the age of 80 experience LUTS from BPH.Citation1
Despite medical therapy represents the first line of treatment, many men progress and need surgical therapy. For its well‐documented favorable long‐term outcomes, transurethral resection of the prostate (TURP) is still considered the reference treatment for clinical BPH.Citation2 However, TURP has its issues of postoperative morbidity, especially in patients on antiplatelet/anticoagulant medications and with a large prostate volume, wherein an increased rate of bleeding requiring transfusions, TUR-syndrome, and long catheterization time have been reported.Citation3,Citation4
New energy sources/modalities, mainly bipolar and laser energies, have been introduced in the last three decades to decrease the early morbidity of monopolar TURP. Among them, one of the most practiced techniques is the photoselective vaporization of the prostate (PVP) with the GreenLight laser™ (GLL) (American Medical Systems, Minnetonka, USA). The first generation machines (60 W and 80 W) used a potassium-titanyl-phosphate crystal to double the frequency of a Nd:YAG laser, emitting a 532-nm wavelength, delivered to tissues by a side-firing fiber and producing a vaporization effect due to a very high absorption coefficient at this wavelength by its target chromophore that is hemoglobin molecule.Citation5 This high energy density delivered to the prostatic tissue leads to rapid vaporization of the superficial tissue with a small rim of coagulated tissue.Citation6 The new generation machines use a lithium-triborate crystal that allowed an increase in the maximum power output of the GLL from 80 W to 180 W. Moreover, new fibers have been introduced, resulting in even higher energy application and faster tissue vaporization via a larger laser beam area.Citation7 Therefore, GLL has become the reference surgical technique to manage patients who cannot stop anticoagulation/antiplatelet therapy.Citation8 Regarding efficacy in the functional outcomes, GLL PVP showed early comparable results compared to standard TURP.Citation9
However, GLL PVP has been criticized for lower reduction of prostate volume compared with TURP that could translate into a major reoperation rate for residual/regrowth adenoma in the long term. High-power potassium-titanyl-phosphate laser PVP was first described by Hai and Malek in 2003 and long-term results of comparative studies with TURP are still lacking.Citation10 Therefore, we aimed to review the safety and efficacy of studies comparing GLL PVP and TURP in the medium-term (at least 2-year follow-up).
Materials and Methods
Aim of the Review and Literature Search
The present systematic review aimed to assess the differences in the incidence of postoperative complications and functional outcomes in men with LUTS due to BPH after PVP versus TURP. The primary outcome was to assess whether outcomes were different in the 2 groups. This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. A comprehensive literature search was performed on October 10, 2020, in MEDLINE via PubMed, Web of Science, Scopus, and Embase. Medical Subject Heading (MeSH) terms and keywords such as “Benign prostatic hyperplasia”, “Transurethral Resection of Prostate”, “Prostate resection”, and “Prostate vaporization” were used with no date limits imposed.
Selection Criteria
The PICOS (Patient Intervention Comparison Outcome Study type) model was used to frame and answer the clinical question. P: patients undergoing BPH surgery; Intervention: patients undergoing Green-Light PVP; Comparison: patients undergoing TURP; Outcome: complications and functional outcomes in studies with at least 2-year follow-up; Study type: randomized clinical trials (RCTs), prospective and retrospective studies. Patients were allocated in two groups regardless of the surgical approach. We gathered the following complications: blood transfusion; postoperative dysuria/urgency rate; postoperative lower urinary tract infection; re-intervention rate for urethral stricture, bladder neck contracture, and residual/regrowth adenoma. We sought the following outcomes: postoperative catheterization time; hospital stay after operation; IPSS and QoL score, PVR, Qmax at 2, 3, and 5 years after surgery.
Study Screening and Selection
Two independent authors screened all retrieved studies. A third author solved discrepancies. Studies were included based on PICOS eligibility criteria. Prospective, retrospective, and RCTs were accepted. Meeting abstracts were excluded. Case reports, non-English, animal, and pediatric studies were also excluded. The full text of the screened papers was selected if found relevant to the topic of this review. The research was further implemented by the manual search based on the references of the full-text relevant papers.
Data Synthesis and Statistical Analysis
We aimed to perform a meta-analysis comparing the medium-term outcomes after Green-Light PVP for clinical BPH compared to TURP. Meta-analyses were performed when studies were reporting the same outcomes. The incidences of complications were pooled using the Cochran-Mantel-Haenszel Method with the random effect model and expressed as Risk Ratios (RR), 95% Confidence Intervals, and p-values. Risk ratios of more than one (1) indicate an increased risk of complications after TURP. Functional outcomes were pooled using the inverse variance of the mean difference with a fixed effect, 95% Confidence Intervals, and p-values. Analyses were two-tailed, with a significance set at p ≤0.05 and a 95% confidence interval. Study heterogeneity was assessed utilizing the I2 value. Substantial heterogeneity was defined as an I2 value >50% or a Chi2 p-value <0.10. Meta-analysis and risk of bias assessment were performed using Review Manager (RevMan) 5.4 software by Cochrane Collaboration. The quality assessment of the included studies was performed using the Cochrane Risk of Bias tool.Citation11 RoB 2 was applied for randomized studies and ROBINS-I for retrospective and prospective non-randomized ones.
Results
The literature search retrieved 1088 papers. 79 duplicates were removed. 1009 papers were screened against title and abstract. The full texts of the remaining 175 studies were assessed for eligibility and 163 papers were excluded because the content was irrelevant to this review. The remaining 12 papers were further assessed to include papers from the same study reporting data of early complications. Finally, 14 papers were identified for meta-analysis.Citation12–Citation25 Supplementary Figure 1 shows the PRISMA flow diagram of the study.
Study Characteristics
There were 2181 patients involved in 12 studies: 1136 and 1045 patients underwent Green Light PVP and TURP, respectively. Supplementary Table 1 shows the characteristics of the 12 studies included in this meta-analysis, including 1 retrospective study, 3 prospective studies, and 8 RCTs. Twelve studies reached 2 years, 4 studies 3 years, and 2 studies 5 years follow-up.
Quality Assessment
Supplementary Figure 2 demonstrates the details of quality assessment for RCTs. One RCT showed a serious attrition bias. The most common risk factors for quality assessment were performance and detection bias. Supplementary Figure 3 shows the quality assessment for retrospective and prospective non-randomized studies. Overall, one study showed serious and two moderate risks of bias due to missing data.
Postoperative Course and Complications Within 30 Postoperative Days
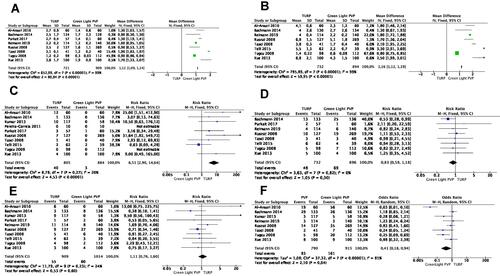
shows perioperative outcomes. Data from 8 available studies showed a longer postoperative catheterization time and length of stay in the TURP group (Risk Ratio (RR): 1.12, 95% CI:1.09–1.14, p<0.00001 and RR: 1.16, 95% CI: 1.12–1.19, p<0.00001, respectively). Data from ten studies of 1689 patients (884 in the Green Light PVP group) compared the need for blood transfusion and showed a higher risk of transfusion in the TURP group (RR: 6.51, 95% CI: 2.90–14.64 p<0.00001). Data from ten studies including 1628 patients (896 in the Green Light PVP group) showed no difference in the risk of urinary tract infections between the two groups (RR: 0.83, 95% CI: 0.58–1.18, p=0.30). Data from eight studies including 1923 patients (1014 in the Green Light PVP group) showed a non-significant higher risk of transient re-catheterization in the TURP group (RR: 1.11, 95% CI: 0.76–1.60, p=0.60). Data from eight study including 1705 patients (915 in the Green Light PVP group) showed a significant risk of higher dysuria/urgency in the Green Light PVP group (RR: 0.41 95% CI 0.18–0.94, p=0.04)
Figure 1 Postoperative course. (A) Postoperative catheterization; (B) Length of stay; (C) Blood transfusion; (D) Urinary tract infection rate; (E) Re-catheterization; (F) Dysuria/urgency incidence.
Reoperation Rate After 30 Postoperative Days
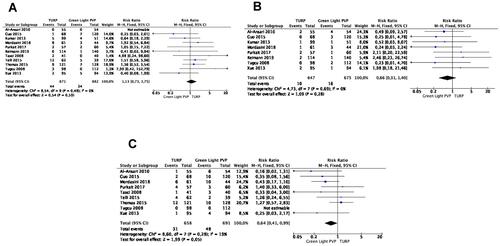
The reoperation rate is reflected in . Data from eleven studies of 1753 patients (882 in the Green Light PVP group) reporting postoperative urethral stricture showed no significant difference between the two groups (RR: 1.13, 95% CI: 0.73–1.75, p=0.59). Data from eight studies of 1322 patients (675 in the Green Light PVP group) describing bladder neck contracture demonstrated no significant difference between the two groups (RR: 0.66, 95% CI: 0.31–1.40, p=0.28). Data from nine studies of 1349 patients (691 in the Green Light PVP group) demonstrated a significantly higher incidence in reoperation for persistent/regrowth adenoma in the Green Light PVP group (RR: 0.64, 95% CI: 0.41–0.99, p=0.05).
Figure 2 Reoperation rate (A) For urethral stricture; (B) For bladder neck contracture; (C) For adenoma regrowth.
Functional Outcomes
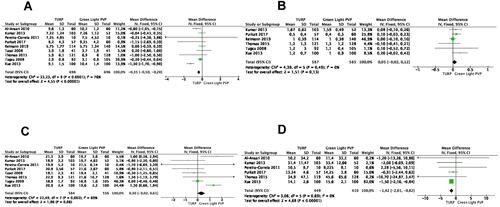
shows functional outcomes 2 years after surgery. Data from nine available studies of 1394 patients (696 in the Green Light PVP group) describing postoperative LUTS score at 2 years showed better IPSS in the TURP group (MD: −0.35, 95% CI: −0.50,-0.20, p<0.00001). Data from six available studies of 1166 patients (585 in the Green Light PVP group) showed no difference in QoL scores at 2 years between the two groups (MD: 0.05, 95% CI: −0.02–0.42, p=0.13). Data from eight studies of 1140 patients (556 in the Green Light PVP group) showed no difference in the mean Qmax at 2 years between the two groups (MD: 0.30, 95% CI: −0.02–0.61, p=0.06). Data from six available studies of 859 patients (410 in the Green Light PVP group) showed better PVR at 2 years in the TURP group (MD: −1.42, 95% CI: −2.01,-0.82, p<0.00001).
Figure 3 Functional outcomes at 2 years (A) International Prostate Symptoms Score; (B) quality of life score; (C) Maximum flow rate; (D) Post voiding residual.
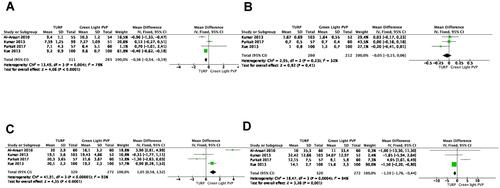
shows functional outcomes 3 years after surgery. Data from four available studies of 576 patients (265 in the Green Light PVP group) describing postoperative LUTS score at 3 years showed better IPSS in the TURP group (MD: −0.36, 95% CI: −0.54,-0.19, p<0.00001). Data from three available studies of 472 patients (212 in the Green Light PVP group) showed no difference in QoL scores at 3 years between the two groups (MD: −0.05, 95% CI: −0.15–0.06, p=0.41). Data from four studies of 592 patients (272 in the Green Light PVP group) showed better Qmax at 3 years in the Green Light PVP group (MD: 1.05, 95% CI: 0.58–1.52, p<0.00001). Data from four available studies of 592 patients (272 in the Green Light PVP group) showed better PVR at 2 years in the TURP group (MD: −1.10, 95% CI: −1.76,-0.44, p=0.001).
Figure 4 Functional outcomes at 3 years (A) International Prostate Symptoms Score; (B) quality of life score; (C) Maximum flow rate; (D) Post voiding residual.
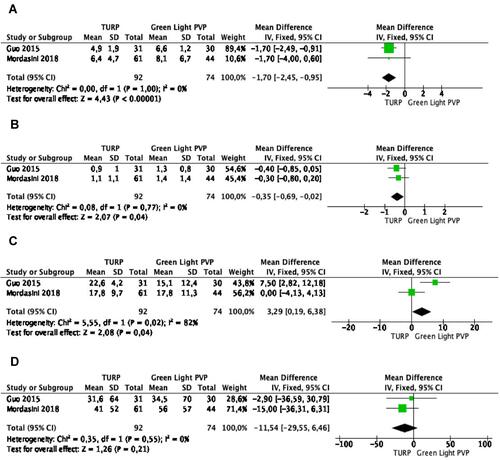
shows functional outcomes 5 years after surgery. Data from two studies of 166 patients (74 in the Green Light PVP group) are available at 5 years. Meta-analysis of LUTS scores showed better IPSS (MD: −1.70, 95% CI: −2.45,-0.95, p<0.00001) and QoL scores (MD: −0.35, 95% CI: −0.69,-0.02, p=0.04) in the TURP group. Meta-analysis of Qmax showed better results in the TURP Group (MD: 3.29, 95% CI: 0.19–6.38, p=0.04). Meta-analysis of PVR showed no significant difference between the two groups (MD: −11.54, 95% CI: −29.55–6.46, p=0.21)
Figure 5 Functional outcomes at 5 years (A) International Prostate Symptoms Score; (B) quality of life score; (C) Maximum flow rate; (D) Post voiding residual.
Discussion
TURP has stood the test of time and is still advocated as the reference surgical procedure in men with symptomatic BPH with a prostate volume up to 80 mL.Citation2 Despite advancements in surgical and anesthesiologic techniques, a recent large real-life study in more than ten thousand patients showed that TURP still has a mortality rate of 0.1% with a cumulative short-term morbidity rate of 11.1%, including 2.9% of blood transfusion.Citation26 Due to its property, the energy produced by GLL is mainly absorbed by hemoglobin in the prostatic tissue with reduced dispersion in the irrigating fluid (saline solution). This effect allows rapid tissue vaporization and refined coagulation, obviating the need for patients to stop their antiplatelet/anticoagulant drugs during PVP.Citation6 According to our results, the need for blood transfusion was significantly higher by sixfold in the TURP group compared to the PVP group (RR: 6.51, 95% CI: 2.90–14,64 p<0.00001). Indeed, only 3 out of 884 patients required transfusions in the PVP group compared to 40 out of 805 patients in the TURP. Unfortunately, subgroup analysis in men taking antiplatelet/anticoagulant drugs was not possible due to missing data.
The advantage of GLL PVP over TURP in bleeding also translated into a shorter postoperative course. Indeed, our study pointed out that the length of catheterization and postoperative stay were again in favor of GLL PVP. This better postoperative course makes GLL PVP an appealing technique that can be carried out as a day procedure in most patients. This is also supported by our finding of no difference in the risk of transient re-catheterization (RR: 1.11, 95% CI: 0.76–1.60, p=0.60) and postoperative urinary tract infections (RR: 0.83, 95% CI: 0.58–1.18, p=0.30) between the two procedures. Emara et al demonstrated in 131 men treated with the new generation 180 W High-Performance System that no perioperative transfusion was required and all men were discharged home the same day. Interestingly, more than 25% of patients in their series had a prostate volume larger than 80 mL.Citation27
GLL PVP is an expensive technique due to the machine and single-use fibers costs. However, the safer profile and shorter postoperative course make PVP more cost-effective compared to TURP. Thomas et al confirmed in a recent meta-analysis that GLL PVP becomes cost-effective compared to TURP if more than 32% of the patients can be discharged the same day.Citation28
The result of functional outcomes after surgery is another important point in evaluating comparative techniques. In this systematic review, the evaluation of functional outcomes was based on four pivotal findings: IPSS with QoL item, Qmax, and PVR. Most of the data showed greater improvement in urinary symptoms after TURP, both early and in the medium-term follow-up. This finding might also be explained by a higher incidence of early postoperative dysuria/urgency after GLL PVP. Indeed, a recent systematic review confirmed that the incidence of postoperative dysuria/urgency after transurethral BPH surgery was significantly higher after ablation procedures as compared to enucleation techniques and TURP.Citation29
QoL results revealed a different trend than urinary symptoms change. Indeed, early outcomes of QoL (2 and 3-year follow-up) were similar between the two groups, although early IPSS were lower in patients treated with GLL PVP. Furthermore, the early results of Qmax and PVR were not superior after GLL PVP compared to TURP. Indeed, it is controversial that early QoL improvement was not correlated to higher flow and greater bladder emptying. QoL changed at 5-year follow-up, showing a greater improvement after TURP. These latter outcomes may be related to the better Qmax results at 5-year follow-up after TURP compared to GLL PVP (MD: 3.29, 95% CI: 0.19–6.38, p=0.04), although PVR volumes did not differ significantly. Nevertheless, data on GLL PVP showed initial results not inferior in terms of Qmax, and better mean Qmax at 3-year follow-up. A greater improvement in uroflow results was achieved by TURP compared to GLL PVP after 5 years. These data confirmed that GLL PVP was very effective in the first period, but that its efficiency was not long-lasting. The lower reduction of prostatic adenoma by GLL PVP might be an explanation of its decreased efficacy in micturition over time. As proof of this, GLL PVP appeared to be associated with a higher incidence of reoperation due to persistence or regrowth of the prostatic adenoma (RR: 0.64, 95% CI: 0.41–0.99, p=0.05). This could be related to both inadequate energy delivery during the procedure, leading to incomplete tissue removal, or ineffective tissue ablation due to the surgeon’s inexperience, at the beginning of their procedural learning curve.Citation18
Regarding PVR, TURP showed a greater benefit in emptying the bladder at early follow-up, while 5 years after surgery the two surgical techniques demonstrated the same results (MD: −11.54, 95% CI: −29.55–6.46, p=0.21). Therefore, PVR was positively influenced by TURP only in the first period after surgery. However, PVR is a controversial parameter, lacking standardized pathological thresholds, and affected by several factors.Citation2 Therefore, other criteria may better reveal bladder emptying efficiencies, such as bladder voiding efficiency and post-void residual ratio, and could be probably be used in future comparative studies.Citation30,Citation31 Another limit to the evaluation of all the functional outcomes may be since not all studies reported these parameters, and had the same follow-up. Therefore, we were able to compare partially different samples during the various follow-up periods.
Concerning the reoperation rate for postoperative urethral stricture and bladder neck contracture, we found no significant difference between the two groups. This result showed that energy source was probably not the cause for stricture/contracture and different reasons, such as prostate volume, length of surgery, size of instruments, should be considered. Unfortunately, a subgroup analysis was not possible due to missing data in most studies.
Conclusion
Our meta-analysis shows that GLL PVP has better perioperative (catheterization time, length of hospitalization, blood transfusions) and early functional outcomes that have definitely to be balanced cautiously against an overall higher rate of reoperation, due to incomplete vaporization or regrowth of prostatic adenoma.
Our review suggests that GLL PVP is a safer and more efficacious procedure than standard TURP in the early and medium-term. However, long-term definitive conclusions favoring one technique over the other cannot be claimed. Further, multicentric prospective investigations comparing the long-term results of these two surgical procedures are recommended.
Ethics Approval
The present study did not involve humans or animals and it did not require formal ethics approval.
Disclosure
The authors report no conflicts of interest in this work.
References
- Egan KB. The epidemiology of benign prostatic hyperplasia associated with lower urinary tract symptoms: prevalence and incident rates. Urol Clin North Am. 2016;43(3):289–297. doi:10.1016/j.ucl.2016.04.001
- Gravas S, Cornu J, Gacci M, et al. EAU guidelines on non-neurogenic male LUTS incl. BPO 2020. EAU guidelines; 2020. Available from: https://uroweb.org/wp-content/uploads/EAU-Guidelines-on-Non-Neurogenic-Male-LUTS-incl.-BPO-2020.pdf. Accessed May 3, 2021.
- Cornu JN, Ahyai S, Bachmann A, et al. A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: an update. Eur Urol. 2015;67(6):1066–1096. doi:10.1016/j.eururo.2014.06.017
- Mebust WK, Holtgrewe HL, Cockett ATK, et al. Transurethral prostatectomy: immediate and postoperative complications. Cooperative study of 13 participating institutions evaluating 3885 patients. J Urol. 1989;141:243–247. doi:10.1016/S0022-5347(17)40731-2
- Bach T, Muschter R, Sroka R, et al. Laser treatment of benign prostatic obstruction: basics and physical differences. Eur Urol. 2012;61(2):317–325. doi:10.1016/j.eururo.2011.10.009
- Rieken M, Bachmann A. Laser treatment of benign prostate enlargement-which laser for which prostate. Nat Rev Urol. 2014;11(3):142–152. doi:10.1038/nrurol.2014.23
- Rieken M, Bonkat G, Müller G, et al. The effect of increased maximum power output on perioperative and early postoperative outcome in photoselective vaporization of the prostate. Lasers Surg Med. 2013;45(1):28–33. doi:10.1002/lsm.22108
- Oelke M, Bachmann A, Descazeaud A, et al. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2013;64(1):118–140. doi:10.1016/j.eururo.2013.03.004
- Teng J, Zhang D, Li Y, et al. Photoselective vaporization with the green light laser vs transurethral resection of the prostate for treating benign prostate hyperplasia: a systematic review and meta-analysis. BJU Int. 2013;111(2):312–323. doi:10.1111/j.1464-410X.2012.11395.x
- Hai MA, Malek RS. Photoselective vaporization of the prostate: initial experience with a new 80 W KTP laser for the treatment of benign prostatic hyperplasia. J Endourol. 2003;17(2):93–96. doi:10.1089/08927790360587414
- Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
- Bachmann A, Tubaro A, Barber N, et al. 180-W XPS greenlight laser vaporisation versus transurethral resection of the prostate for the treatment of benign prostatic obstruction: 6-month safety and efficacy results of a European multicentre randomised trial - The GOLIATH study. Eur Urol. 2014;65(5):931–942. doi:10.1016/j.eururo.2013.10.040
- Pereira-Correia JA, De Moraes Sousa KD, Santos JBP, et al. GreenLight HPSTM 120-W laser vaporization vs transurethral resection of the prostate (<60 mL): a 2-year randomized double-blind prospective urodynamic investigation. BJU Int. 2012;110(8):1184–1189. doi:10.1111/j.1464-410X.2011.10878.x
- Purkait B, Sinha RJ, Srinivas KSA, Bansal A, Sokhal AK, Singh V. Outcome analysis of transurethral resection versus potassium titanyl phosphate-photo selective vaporization of the prostate for the treatment of benign prostatic hyperplasia; a randomized controlled trial with 4 years follow up. Turk J Urol. 2017;43(2):176–182. doi:10.5152/tud.2017.20586
- Guo S, Müller G, Lehmann K, et al. The 80-W KTP GreenLight laser vaporization of the prostate versus transurethral resection of the prostate (TURP): adjusted analysis of 5-year results of a prospective non-randomized bi-center study. Lasers Med Sci. 2015;30(3):1147–1151. doi:10.1007/s10103-015-1721-x
- Ruszat R, Wyler SF, Seitz M, et al. Comparison of potassium-titanyl-phosphate laser vaporization of the prostate and transurethral resection of the prostate: update of a prospective non-randomized two-centre study. BJU Int. 2008;102(10):1432–1439. doi:10.1111/j.1464-410X.2008.07905.x
- Mordasini L, Di Bona C, Klein J, Mattei A, Wirth GJ, Iselin CE. 80-W GreenLight laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic obstruction: 5-year outcomes of a single-center Prospective Randomized Trial. Urology. 2018;116:144–149. doi:10.1016/j.urology.2018.01.037
- Thomas JA, Tubaro A, Barber N, et al. A multicenter randomized noninferiority trial comparing GreenLight-XPS laser vaporization of the prostate and transurethral resection of the prostate for the treatment of benign prostatic obstruction: two-yr Outcomes of the GOLIATH Study. Eur Urol. 2016;69(1):94–102. doi:10.1016/j.eururo.2015.07.054
- Tugcu V, Tasci AI, Sahin S, Zorluoglu F. Comparison of photoselective vaporization of the prostate and transurethral resection of the prostate: a prospective nonrandomized bicenter trial with 2-year follow-up. J Endourol. 2008;22(7):1519–1525. doi:10.1089/end.2007.0321
- Tasci AI, Tugcu V, Sahin S, Zorluoglu F. Rapid communication photoselective vaporization of the prostate versus transurethral resection of the prostate for the large prostate: a prospective nonrandomized bicenter trial with 2-year follow-up. J Endourol. 2008;22(2):347–353. doi:10.1089/end.2007.0137
- Reimann M, Fishman N, Lichy I, et al. Outcome of photoselective vaporization of the prostate with the GreenLight-XPS 180 Watt system compared to transurethral resection of the prostate. J Clin Med. 2019;8(7):1004. doi:10.3390/jcm8071004
- Xue B, Zang Y, Zhang Y, et al. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic hyperplasia: a prospective randomized trial. J Xray Sci Technol. 2013;21(1):125–132. doi:10.3233/XST-130359
- Al-Ansari A, Younes N, Sampige VP, et al. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic hyperplasia: a randomized clinical trial with midterm follow-up. Eur Urol. 2010;58(3):349–355. doi:10.1016/j.eururo.2010.05.026
- Kumar N, Vasudeva P, Kumar A, Singh H. Prospective randomized comparison of monopolar TURP, bipolar TURP and photoselective vaporization of the prostate in patients with benign prostatic obstruction: 36 months outcome. Low Urin Tract Symptoms. 2018;10(1):17–20. doi:10.1111/luts.12135
- Telli O, Okutucu TM, Suer E, et al. A prospective, randomized comparative study of monopolar transurethral resection of the prostate versus photoselective vaporization of the prostate with GreenLight 120-W laser, in prostates less than 80 cc. Ther Adv Urol. 2015;7(1):3–8. doi:10.1177/1756287214556643
- Reich O, Gratzke C, Bachmann A, et al. Morbidity, mortality and early outcome of transurethral resection of the prostate: a prospective multicenter evaluation of 10,654 patients. J Urol. 2008;180(1):246–249. doi:10.1016/j.juro.2008.03.058
- Emara AM, Barber NJ. The continuous evolution of the Greenlight laser; the XPS generator and the MoXy laser fiber, expanding the indications for photoselective vaporization of the prostate. J Endourol. 2014;28(1):73–78. doi:10.1089/end.2013.0356
- Thomas JA, Tubaro A, Barber N, et al. The continuing story of the cost-effectiveness of photoselective vaporization of the prostate versus transuretheral resection of the prostate for the treatment of symptomatic benign prostatic obstruction. Value Health. 2015;18(4):376–386. doi:10.1016/j.jval.2015.04.002
- Wroclawski ML, Castellani D, Heldwein FL, et al. Shedding light on polypragmasy of pain after transurethral prostate surgery procedures: a systematic review and meta-analysis. World J Urol. 2021. doi:10.1007/s00345-021-03678-6
- Rubilotta E, Balzarro M, Trabacchin N, et al. Post-void residual urine ratio: a novel clinical approach to the post-void residual urine in the assessment of men with lower urinary tract symptoms. Investig Clin Urol. 2021;62. doi:10.4111/icu.2021.62.e45
- Abrams P. Bladder outlet obstruction index, bladder contractility index and bladder voiding efficiency: three simple indices to define bladder voiding function. BJU Int. 1999;84(1):14–15. doi:10.1046/j.1464-410x.1999.00121.x