
Abstract
Medical therapy for hereditary hepatorenal tyrosinemia (hereditary tyrosinemia type 1, HT-1) with nitisinone was discovered incidentally, and is a by-product of agrochemistry. It blocks the catabolic pathway of tyrosine, thereby leading to a reduction in the accumulation of toxic metabolites in HT-1. It has to be combined with a low-protein diet supplemented with amino acid mixtures devoid of tyrosine and phenylalanine. This treatment option has completely changed the clinical course of patients suffering from HT-1 who used to die in the first few months to years of life from liver failure, renal dysfunction, and/or hepatocellular carcinoma (HCC). It is essential to start nitisinone therapy early in life to avoid sequelae; beginning treatment in the newborn period is ideal. As initial clinical symptoms of HT-1 are often atypical and because there is a clinically latent phase during the first few months of life in many patients, newborn screening is required to secure early diagnosis. Succinylacetone in blood is a reliable screening parameter whereas tyrosine is neither specific nor sensitive. Especially HCC, but also liver and kidney dysfunction, rickets, and neurological crises can be prevented in most patients if nitisinone therapy is started in the newborn period. It is essential to adhere to a low-protein diet to avoid tyrosine toxicity. Reversible eye symptoms may occur as a side-effect of nitisinone, but other side effects are rare. Neurocognitive development is impaired in some patients, and the reason for this is unclear. Metabolic monitoring includes measurement of tyrosine, succinylacetone, and nitisinone concentrations in blood.
Introduction to the pathophysiology, clinical symptoms, and treatment of hereditary tyrosinemia type-1
Hereditary tyrosinemia type-1 (hepatorenal tyrosinemia, HT-1) is a rare inborn error of metabolism in the catabolism of the amino acid tyrosine (). In Central Europe, the prevalence is 1:125,000, although much higher incidence rates are observed in other regions such as Turkey, Quebec, and India. HT-1 is inherited as an autosomal-recessive trait and is, thus, more common in populations with a high degree of consanguinity.
Figure 1 Degradative pathway of tyrosine. HT-1 is due to fumarylacetoacetase deficiency. NTBC (nitisinone) leads to proximal inhibition in the tyrosine pathway with reduction of toxic metabolites (surrogate parameter succinylacetone).
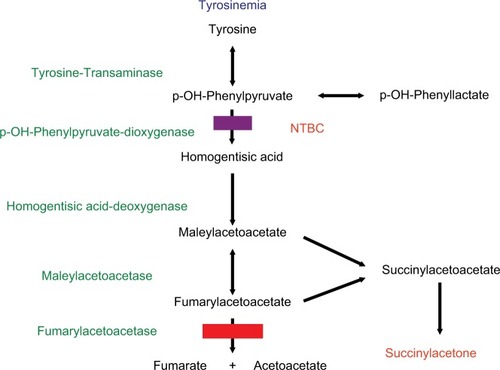
Biochemically, a deficiency of fumarylacetoacetase leads to the accumulation of not only tyrosine but also different metabolites such as maleylacetoacetate, fumarylacetoacetate, and succinylacetone (SA) – the latter is commonly used as a surrogate parameter of toxicity in blood and/or urine ().
Diagnosis is based on elevated SA levels in blood and/or urine, as tyrosine elevation is an unreliable marker. There are many false-positive and false-negative results when tyrosine is used as the only diagnostic parameter.Citation1
Clinical symptoms comprise liver dysfunction (sometimes culminating in liver failure), tubular dysfunction, rickets, and, sometimes, neurological symptoms. A long-term complication is hepatocellular carcinoma (HCC); neurocognitive deficits can be observed in some patients.Citation2–Citation5
Therapy consists of nitisinone (Orfadin®, 2-(2-nitro-4-trifluoromethylbenzoyl)cyclohexane 1-,3-dione, NTBC) in order to decrease levels of toxic compounds (). Nitisinone blocks the degradation of tyrosine. A low-protein diet supplemented with special amino acid mixtures devoid of tyrosine and its precursor phenylalanine is required to prevent excessive tyrosine levels. In patients in whom nitisinone therapy fails to prevent acute liver failure or in those who develop HCC, liver transplantation (LTx) is the therapy of choice.Citation4,Citation5
Nitisinone was approved by the European Medicine Agency (EMA) under exceptional circumstances in 2005. The first clinical use of nitisinone in HT-1 dates back to 1991. Originally, nitisinone was developed as a weed-killer by Zeneca Agrochemicals.Citation6 It was epidemiologically observed that the growth of plants and weeds was inhibited under the bottlebrush plant (Callistemon citrinus).Citation7 It became clear that neither the shade nor the litterfall of these plants were responsible for suppression of plant and weed growth. Rather, a substance – which was identified as leptospermone – in the soil under the bottlebrush plant was shown to have bleaching activity on the emerging plants.Citation8 The allelochemical leptospermone was extracted from the bottlebrush plant and chemically characterized. Leptospermone belongs to the triketone family and inhibits chloroplast development due to a lack of plastoquinone secondary to hepatic 4-hydroxyphenylpyruvate dioxygenase (HPPD) inhibition; thus, it served as a blueprint for the synthesis of nitisinone.Citation9
Toxicology testing of nitisinone revealed that it was not acutely toxic, but eye lesions (keratopathy) could be observed in animals after prolonged treatment. Lesions were reversible upon cessation of exposure to the compound. Elevated tyrosine levels were found in the blood and urine after nitisinone exposure. Nitisinone was established as a potent inhibitor of rat hepatic HPPD at the Zeneca Central Toxicity Laboratories (). Inhibition of human HPPD was demonstrated in human liver by Sven Lindstedt and his group at Gothenburg University (Sweden). The research was already ongoing for an inhibitor of HPPD to treat patients with the lethal disease HT-1. Zeneca Pharmaceuticals acquired the compound as a potential drug candidate, although with some reluctance, as only a limited number of patients with this rare disease would possibly benefit from this drug. The Swedish Medical Agency approved a clinical trial with nitisinone in HT-1 patients and, in February 1991, a critically ill 2-month-old baby became the first HT-1 patient to be treated with nitisinone in Gothenburg. SA quickly disappeared from the urine and the clinical state gradually improved. Subsequently, several HT-1 patients were successfully treated with nitisinone on a compassionate-use basis. In the following years, many patients were successfully treated with nitisinone, culminating in the approval of nitisinone by the US Food and Drug Administration in 2002 and the European Medicines Agency (EMA) in 2005 under “exceptional circumstances” as large-scale field trials and real-world data in HT-1 patients were unavailable. The first sublicense-holder Swedish Orphan International was obliged to conduct postmarketing studies, which are now carried out by the present sublicense-holder Swedish Orphan Biovitrum (SoBi) in the framework of the “OPAL” study.
Review of pharmacology, mode of action, and pharmacokinetics of nitisinone
In HT-1, organ damage and dysfunction is mediated by toxic compounds like maleylacetoacetate, fumarylacetoacetate, and SA (). The main organs affected are the liver and kidneys; rickets and neurological crises may occur; and HCC may be a long-term complication.Citation3 Nitisinone blocks the catabolic pathway of tyrosine proximal to the deficient enzyme fumarylacetoacetase at the level of 4-OH-phenylpyruvate-dioxygenase (HPPD), which catabolizes p-OH phenylpyruvate to homogentisic acid, thereby reducing the levels of toxic compounds (). SA is used as a surrogate parameter for toxic compounds. As the block in tyrosine catabolism results in tyrosine accumulation, a protein-reduced diet supplemented with a special amino acid mixture devoid in phenylalanine (precursor of tyrosine) and tyrosine is required to prevent tyrosine toxicity. Calculation of tyrosine and phenylalanine intake is not required in most patients with HT-1.
In rat liver, enzyme kinetic studies revealed inhibition of HPPD by nitisinone in a dose- and time-dependent manner with a rate constant of 9.9 × 10−5 s−1 (nmol L−1)−1.Citation10 Nitisinone does not bind irreversibly to HPPD; the enzyme–inhibitor complex dissociates with a half-life of 63 hours in rats at 25°C. Tests in human adult volunteers revealed nitisinone had a half-life of 54 hours.Citation11 It is recommended that nitisinone be administered in a twice-daily dosage. However, based on the long half-life of nitisinone, once-daily dosing was advocated,Citation12 which seems to be adequate to maintain metabolic control. Moreover, once-daily dosing may improve adherence to pharmacological therapy.
The recommended dose of nitisinone is 1–2 mg/kg per day, in two divided doses. In a recent survey,Citation13 we found several HT-1 patients in whom nitisinone was titrated down without hampering metabolic control, as judged by the absence of SA, with doses as low as 0.3 mg/kg per day shown to be sufficient.
Efficacy studies
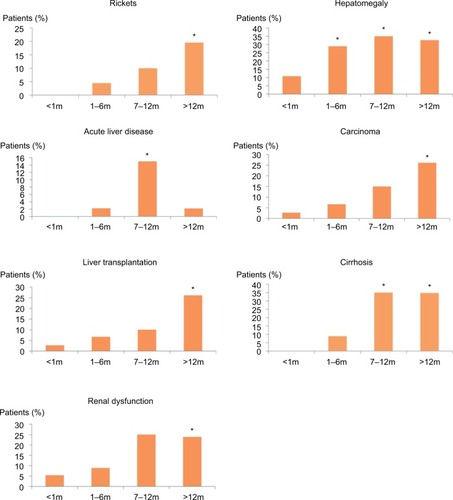
Although it is clear that nitisinone can reduce the levels of toxic compounds, as judged by the surrogate parameter SA, and secure survival, the impact on long-term clinical outcome is less clear. This is mainly due to the rarity of the disease. In the literature, a few regional studies can be found,Citation14–Citation20 recommendations by a group of experienced clinicians were published,Citation21 and there is only one multinational cross-sectional study that included 168 patients from 21 centers.Citation13 This study showed a clear benefit of nitisinone treatment in combination with a low-protein diet supplemented by amino acid mixtures devoid of tyrosine and phenylalanine. If present, liver dysfunction/failure, renal dysfunction, tubulopathy, and rickets could be reversed by nitisinone treatment. Furthermore, HCC prevalence could be reduced by nitisinone treatment. Long-term complications, especially development of HCC, critically depend on early initiation of treatment, and, therefore, on early diagnosis. If treatment is started beyond the first year of life, the risk of HCC is 13 times higher as compared to patients for whom treatment is initiated in the neonatal period; furthermore, risk of liver cirrhosis, rickets, and tubular dysfunction is increased 40-, 19-, 4.3-fold, respectively ().Citation13 Thus, early diagnosis in the newborn period is essential to secure a good long-term outcome.Citation15,Citation18,Citation22 Initial clinical symptoms (hepatomegaly, renal tubular dysfunction, rickets, etc.) are atypical, and often occur after a clinically latent phase. Therefore, it is difficult to make an early diagnosis based on clinical symptoms alone.Citation13 Neonatal mass screening is crucial to secure early diagnosis (and treatment) in the newborn period. Tyrosine as a screening parameter is not appropriate due to the high rate of false positives and false negatives; SA is the screening parameter of choice.Citation1,Citation13,Citation23,Citation24
Figure 2 Effect of age at treatment initiation with nitisinone and low-protein diet on development of clinical symptoms.
It recently became evident that many patients with HT-1 suffer from neurocognitive deficits.Citation25–Citation28 The etiology of these sequelae is unclear, although it may be attributed to tyrosine toxicity, phenylalanine deficiency, drug toxicity, or natural disease progression in long-term survivors with HT-1. Prospective clinical studies are necessary to solve this issue.
Nitisinone leads to the accumulation of tyrosine as it blocks tyrosine catabolism. Protein restriction is necessary to avoid tyrosine toxicity, and target values for plasma tyrosine levels have been tentatively set by consensus to below 400 µM.Citation13
The incidence of acute or chronic liver failure and HCC has dropped enormously since nitisinone was approved for clinical use. However, a few patients may develop therapy-refractory liver failure. HCC is mostly due to late initiation of treatment in the absence of neonatal screening.
No alternative treatments for HT-1 are currently known. After the marketing exclusivity for Orfadin® expired, alternative nitisinone-containing medication was produced in Turkey and the United Kingdom at lower prices.
Safety and tolerability
Side effects in nitisinone-treated patients are rare and mostly reversible. Eye pain, eye itching/conjunctivitis, corneal crystals, and thrombocytopenia are the most common side effects reported;Citation13 these are mostly related to high tyrosine levels and are reversible when tyrosine levels are lowered by strict dietary compliance.Citation30
Neurocognitive deficits are a problem in long-term managementCitation25–Citation29; it is not clear whether these are direct side effects of nitisinone treatment, a result of high tyrosine or low phenylalanine levels, or part of natural disease progression. It seems reasonable to reduce nitisinone levels without compromising metabolic control (based on SA levels in urine and/or blood). Therefore, nitisinone levels should be regularly determined in dried blood spots, together with SA.Citation31 In most cases, it is possible to titrate down the daily dose of nitisinone initially from 1 mg/kg per day without hampering metabolic control. The tentative therapeutic range of nitisinone concentration in dried blood is 20–40 µM.Citation13
Patient-focused perspectives
Adherence to drug therapy with nitisinone is obviously not easy but, based on nitisinone levels in dried blood, most patients manage to take nitisinone regularly. Once-daily dosing may enhance adherence. Life-long adherence to a low-protein diet supplemented with an amino acid mixture is a challenge. Calculation of protein, phenylalanine, or tyrosine intake is not required in most cases and this facilitates adherence. Dietary noncompliance often leads to eye problems, which are reversible with reduced protein intake. Moreover, adherence to therapy depends on financial reimbursement at least in some patients. In most centers participating in our cross-sectional survey, costs for nitisinone treatment and special low-tyrosine amino acid mixtures are covered by health insurance or the government whereas patients were reimbursed for protein-restricted diet in only half of the centers.Citation13
Regular outpatient visits are required for monitoring of diet and disease and are time-consuming as well as a financial burden. Sending dried blood for monitoring of SA, nitisinone, and tyrosine from home facilitates control of therapy.Citation31
As female patients with HT-1 reach adulthood, “maternal” HT-1 becomes an issue. A few successful pregnancies of mothers with HT-1 have been reported where the use of nitisinone was not interrupted during pregnancy and lactation.Citation32,Citation33
After liver transplantation, SA is still excreted in urine by many patients as the enzyme defect is also expressed outside the liver. It is not clear whether nitisinone should be continued in these cases to avoid toxicity. The use of nitisinone implies introducing a low-protein diet supplemented with an amino acid mixture.
Conclusion
Nitisinone as a therapeutic option in HT-1 was discovered by chance and is a by-product of agrochemistry. Its use has substantially changed the outcome in HT-1 patients. Nitisinone treatment has to be combined with a low-protein diet supplemented with an amino acid mixture devoid of tyrosine and phenylalanine to avoid tyrosine toxicity. Based on the long half-life of nitisinone, once-daily dosing should be possible.
There are a few side effects, mostly related to the eye, which are reversible upon stricter protein restriction. In most HT-1 patients, there is an initial latent phase; early diagnosis based on clinical symptoms is not possible in most HT-1 patients, and newborn screening with SA as the screening parameter is essential. Early diagnosis and treatment leads to a much better outcome; especially, HCC incidence is low when treatment is started in the newborn period. In some patients, neurocognitive deficits occur.
Treatment monitoring includes tyrosine levels (therapeutic target, <400 µM), SA-(therapeutic target, negative), and nitisinone concentration.
Disclosure
The author reports no conflict of interest in this work.
References
- SanderJJanzenNPeterMNewborn Screening or hepatorenal tyrosinemia: tandem mass spectrometric quantification of succinylacetoneClin Chem200652348248716439608
- LindbladBLindstedtSSteenGOn the enzymatic defects in hereditary tyrosinemiaProc Natl Acad Sci U S A1977741046414645270706
- ChakrapaniAHolmeEDisorders of tyrosine metabolismFernandezSvan den BergheWInborn Metabolic Diseases4th edHeidelbergSpringer2006233243
- van SpronsenFJBijleveldCMvan MaldegemBTWijburgFAHepatocellular carcinoma in hereditary tyrosinemia type I despite 2-(2 nitro-4-3-trifluoro-methylbenzoyl)-1,3-cyclohexanedione treatmentJ Pediatr Gastroenterol Nutr2005401909315625434
- WeinbergAGMizeCEWorthenHGThe occurrence of hepatoma in the chronic form of hereditary tyrosinemiaJ Pediatr1976883434438173827
- LockERanganathLRTimmisOThe role of nitisinone in tyrosine pathway disordersCurr Rheumatol Rep2014161145746425266991
- KnudsenCGLeeDLMichaelyWJDiscovery of the triketone class of HPPD inhibiting herbicides and their relationship to naturally occurring beta-triketonesNarwalSSHoaglandREDildayRHReigosaMAllelopathy in Ecological Agriculture and ForestryDordrechtKluwer Academic Publishers2000101111
- SantucciABernardiniGBraconiDPetricciEManettiF4-hydroxyphenylpyruvate dioxygenase and its inhibition in plants and animals: small molecules as herbicides and agents for the treatment of human inherited diseasesJ Med Chem201760104101412528128559
- PallettKCan we expect new herbicides with novel modes of action in the foreseeable future?Outlooks Pest Manag20162713943
- EllisMKWhitfieldACGowansLAInhibition of 4-hydroxyphenylpyruvate dioxygenase by 2-(2-nitro-4-trifluoro - methylbenzoyl)-cyclohexane-1,3-dione and 2-(2-chloro-4-methanesulphonylbenzoyl)-cyclohexane-1,3-dioneToxicol Appl Pharmacol1995133112197597701
- HallMGWilksMFMcLean ProvanWEksborgSLumholtzBPharmacokinetics and pharmacodynamics of NTBC (2-(2-nitro-4-fluoromethylbenzoyl)-1,3-cyclohexanedione) and mesotrione, inhibitors of 4-hydroxyphenyl pyruvate dioxygenase (HPPD) following a single dose to healthy male volunteersBr J Clin Pharmacol200152216917711488774
- SchluneAThimmEHerebianDSpiekerkoetterUSingle dose NTBC-treatment of hereditary tyrosinemia type IJ Inherit Metab Dis201235583183622307209
- MayorandanSMeyerUGokcayGCross sectional study of 168 patients with hepatorenal tyrosinaemia and implications for clinical practiceOrphanet J Rare Dis2014910725081276
- Masurel-PauletAPoggi-BachJRollandMONTBC-treatment in tyrosinaemia type I: long-term outcome in French patientsJ Inherit Metab Dis2008311818718214711
- VondrákováATesarováMMagnerMClinical, biochemical and molecular characteristics in 11 Czech children with tyrosinemia type ICas Lek Cesk20101499411416 Czech21117323
- CouceMLDalmauJdel ToroMPintos-MorellGAldámiz-Echevarría LSpanish Working Group on Tyrosinemia type 1Tyrosinemia type I in Spain: mutational analysis, treatment and long-term outcomePediatr Int201153698598921752152
- CouceMLAldámiz-EchevarríaLBaldellouARecomendaciones y manejo de la tirosinemia hereditaria Tipo I o Tirosinemia hepatorrenal [Recommendations and management of type I hereditary or hepatorenal tyrosinemia]An Pediatr (Barc)2010735279.e1e4 Spanish20813594
- LarochelleJAlvarezFBussièresJFEffect of nitisinone (NTBC) treatment on the clinical course of hepatorenal tyrosinemia in QuébecMol Genet Metab20121071–2495422885033
- SchiffMBrouePChabrolBFrench-Belgian study group for HT-1Heterogeneity of follow-up procedures in French and Belgian patients with treated hereditary tyrosinemia type I: results of a questionnaire and proposed guidelinesJ Inherit Metab Dis201235582382922167277
- CoşkunTOzalpIKoçakNYüceACaglarMBergerRType I hereditary tyrosinaemia: presentation of 11 casesJ Inherit Metab Dis19911457657701664010
- de LaetCDionisi-ViciCLeonardJVRecommendations for the management of tyrosinaemia type 1Orphanet J Rare Dis20138823311542
- HolmeELindstedtSTyrosinaemia type I and NTBC (2-(2-nitro-4-trifluoromethylbenzoyl)-1,3-cyclohexanedioneJ Inherit Metab Dis19982155075179728331
- la MarcaGMalvagiaSMaterazziSLC-MS/MS method for simultaneous determination on a dried blood spots of multiple analytes relevant for treatment monitoring in patients with tyrosinemia type IAnal Chem20128421184118822148291
- AllardPGrenierAKorsonMSZytkoviczTHNewborn screening for hepatorenal tyrosinemia by tandem mass spectrometry: analysis of succinylacetone extracted from dried blood spotsClin Biochem200437111010101515498530
- ThimmERichter-WerkleRKampGNeurocognitive outcome in patients with hypertyrosinemia type I after a long-term treatment with NTBCJ Inherit Metab Dis201235226326822069142
- De LaetCMunozVTJaekenJNeuropsychological outcome of NTBC-treated patients with tyrosinaemia type 1Dev Med Child Neurol2011531096296421745202
- PohoreckaMBiernackaMJakubowska-WineckaABehavioral and intellectual functioning in patients with tyrosinemia type IPediatr Endocrinol Diabetes Metab20121839610023146787
- BendadiFde KoningTJVisserGImpaired cognitive functioning in patients with tyrosinemia type I receiving nitisinoneJ Pediatr2014164239840124238861
- GarcíaMIde la ParraAAriasCArredondoMCabelloJFLong-term cognitive functioning in individuals with tyrosinemia type 1 treated with nitisinone and protein-restricted dietMol Genet Metab Rep201711121628377889
- GissenPPreeceMAWillshawHAMcKiernanPJOphthalmic follow-up of patients with tyrosinaemia type I on NTBCJ Inherit Metab Dis2003261131612872835
- SanderJJanzenNTerhardtMMonitoring tyrosinaemia type I: blood spot test for nitisinone (NTBC)Clin Chim Acta20114121–213413820883679
- VancloosterADevliegerRMeerssemanWPregnancy during nitisinone treatment for tyrosinaemia type I: first human experienceJIMD Rep20125273323430914
- KasselRSprietsmaLRudnickDAPregnancy in an NTBC-treated patient with hereditary tyrosinemia type IJ Pediatr Gastroenterol Nutr2015601e5e723838819