
Abstract
Background
Germline mutations BRCA1 and BRCA2 contribute almost equally in the causation of breast cancer (BC). The type of mutations in the Indian population that cause this condition is largely unknown.
Purpose
In this cohort, 79 randomized BC patients were screened for various types of BRCA1 and BRCA2 mutations including frameshift, nonsense, missense, in-frame and splice site types.
Materials and methods
The purified extracted DNA of each referral patient was subjected to Sanger gene sequencing using Codon Code Analyzer and Mutation Surveyor and next-generation sequencing (NGS) methods with Ion torrent software, after appropriate care.
Results
The data revealed that 35 cases were positive for BRCA1 or BRCA2 (35/79: 44.3%). BRCA2 mutations were higher (52.4%) than BRCA1 mutations (47.6%). Five novel mutations detected in this study were p.pro163 frameshift, p.asn997 frameshift, p.ser148 frameshift and two splice site single-nucleotide polymorphisms (SNPs). Additionally, four nonsense and one in-frame deletion were identified, which all seemed to be pathogenic. Polymorphic SNPs contributed the highest percentage of mutations (72/82: 87.8%) and contributed to pathogenic, likely pathogenic, likely benign, benign and variant of unknown significance (VUS). Young age groups (20–60 years) had a high frequency of germline mutations (62/82;75.6%) in the Indian population.
Conclusion
This study suggested that polymorphic SNPs contributed a high percentage of mutations along with five novel types. Younger age groups are prone to having BC with a higher mutational rate. Furthermore, the SNPs detected in exons 10, 11 and 16 of BRCA1 and BRCA2 were higher than those in other exons 2, 3 and 9 polymorphic sites in two germline genes. These may be contributory for BC although missense types are known to be susceptible for cancer depending on the type of amino acid replaced in the protein and associated with pathologic events. Accordingly, appropriate counseling and treatment may be suggested.
Introduction
The continuing global demographic and epidemiologic transitions signal an ever-increasing cancer burden over the next decades, particularly in low- and middle-income countries (LIMC), with over 20 million new cancer cases expected annually as early as 2025. Breast cancer (BC) is one of the most common and dreadful diseases affecting Indian women.Citation1,Citation2 It is actually considered the main type of cancer among new cases in India.Citation3 It has been divided into two subtypes, early-onset and late-onset, based on age-specific cancers. Mutation in BRCA1 is thought to account for about 45% of families, whose locus is to chromosome 17p. The second one is mapped to chromosome 13q and responsible for the early onset of BC.Citation4 About 200 mutations in both genes have been reported and are widely scattered across them.Citation5–Citation7 Most mutations of these genes affect the structure and function of the gene, altering protein synthesis and function (34% BRCA1 and 38% BRCA2 mutations), and others are missense types that alter amino acids but do not truncate the protein.Citation8,Citation9 Hence, the mutation of BRCA1/2 results in the gene’s function silencing or over-activation.
According to the GLOBOCAN project set up by the International Agency for Research on Cancer (IARC),Citation10 145,000 new cases were diagnosed and 70,000 deaths occurred in India in 2012. Considering the size of the population, the incidence of BC in India appears to be lower, when compared to developed countries such as the USA (233,000 cases) and the European union (362,000 cases). But the ratio of death in India was much higher (48.3%) in comparison with the USA (18.9%) and the European union (25.4%).Citation11,Citation12 Thus, the frequency of BC patients seems to be lower than in the developing countries, but mortality is higher in our country attributable to lifestyle changes, delay in introduction of cancer screening centers and limited medical awareness including treatment.Citation12–Citation14
The relatively high death rate from BC in the Indian health care system thus demonstrates a need for a cost-effective method of early detection, screening and treatment.Citation12 However, early detection of hereditary BC is essential to reduce this type of cancer in a developing country like India. Hence, this study was undertaken to detect the germline mutations using molecular diagnostic methods and their correlation with pathogenic events for its better treatment in addition to other factors, such as age, in our cohort. Emphasis is also paid to the involvement of missense mutations occurring in BRCA1 and BRCA2 genes of BC patients in the Indian population.
Materials and methods
Patient selection
A total of 79 referral, diagnosed, pre- and post-menopausal BC cases from India were selected. EDTA blood samples and a request for biological specimens were collected from the respondents after completion of consent forms and counseling. The patients provided test reports which were used for our current research. This work was approved by Gujarat University (Ahmedabad, India) Human Ethical Committee (GUHEC/001/2015) for investigation.
DNA extraction
Genomic DNA was extracted from 3–4 mL of peripheral EDTA blood using automated DNA extraction method (PerkinElmer Inc., Waltham, MA, USA). The concentration of DNA was determined using the Qubit 2.0 Fluorometer (Thermo Fisher Scientific, Waltham, MA, USA).
Targeted next-generation sequencing (NGS) (amplification)
For targeted NGS analysis, the Ion AmpliSeq™ BRCA1 and BRCA2 Panel (Thermo Fisher Scientific) containing 167 primer pairs in three pools (Pool 1 is 56 pairs, 2 is 56 pairs and 3 is 55 pairs) was used. Multiplex PCR was performed using 10–30 ng genomic DNA with a premixed primer pool and Ion AmpliSeq™ HiFi master mix; Ion AmpliSeq™ Library Kit 2.0; Cat. no. 4480441) for 2 min at 99°C, followed by 19 cycles of denaturation at 99°C for 15 s and annealing and elongation at 60°C for 4 min, ending with a holding period at 10°C. The PCR amplicons were treated with 2 µL FuPa reagent to partially digest primer sequences and phosphorylate the amplicons at 50°C for 10 min, followed by 55°C for 10 min, then 60°C for 20 min. The amplicons were ligated to adapters with the diluted barcodes of the Ion Xpress™ Barcode Adapters kit (Thermo Fisher Scientific) for 30 min at 22°C, then 72°C for 10 min. Adaptor-ligated amplicon libraries were purified using Agencourt AMPure XP (Cat no. A63881) reagents (Beckman Coulter, CA, USA). The library concentration was determined using an Ion Library Quantitation Kit (Cat no. 4468802) (Thermo Fisher Scientific), then each library was diluted to 4–8 pmol/L and the same amount of libraries was pooled for one sequence reaction. Next, emulsion PCR was carried out using the Ion OneTouch™ 2.0 System and Ion PGM™ Hi-Q™ OT2 (Cat no. A27743) reagents, or Ion 540™ OT2 (Cat no. A27752) reagents (Thermo Fisher Scientific), according to the manufacturer’s instructions. Template-positive Ion Sphere™ particles were then enriched with Dynabeads MyOne™ Streptavidin C1 Beads (Cat no. 65001) (Thermo Fisher Scientific) using an Ion OneTouch™ ES system (Thermo Fisher Scientific). Purified Ion Sphere particles were loaded on any of chip types 314, 316, or 318 (Compatible with Ion PGM) or 520, 530, or 540 (Compatible with Ion S5 System) Chip. Massively parallel sequencing was carried out on a Personal Genome Machine (PGM) sequencer (Ion Torrent™) using the Ion PGM™ Hi-Q™ Sequencing Kit or Ion S5 sequencer (Thermo Fisher Scientific) using Ion S5 Sequencing kit according to the manufacturer’s instructions. Sequencing was performed using 500 flow runs that generated ~200 bp reads.
Sanger DNA sequencing
Possible high confidence variants were confirmed by Sanger sequencing. PCR primers were designed using the OligoCalc (http://biotools.nubic.northwestern.edu/OligoCalc.html) to determine the properties of designed primers and Primer Blast (https://www.ncbi.nlm.nih.gov/tools/primer-blast/) was also used to check whether our region of interest was covered. Primers were synthesized at 100 nM scale and cartridge purified (Eurofins, Bengaluru, India). PCR amplification was carried out using Takara Taq™ Hot Start Version 2.0 PCR mix with each primer at 10 pM concentration under standard conditions. These PCR amplifications were all carried out in duplicate along with a known normal control cell line sample. Successful PCR products were purified prior to sequencing using ExoSAP-IT (Cat no. 78201) reagent (Thermo Fisher Scientific) according to the manufacturer’s protocol. Purified PCR products were subjected to Sanger sequencing technique in both forward and reverse orientations with the same primer sequences used for PCR at 10 pM final concentration using BigDye® v3.1(Cat no. 4336917) according to the manufacturer’s cycling conditions. BigDye® v3.1 sequencing reactions were then purified using EDTA (Cat no. 194822) and sodium acetate (Cat no. 567418) according to the manufacturer’s protocol and analyzed on 3500 Genetic Analyzer (Thermo Fisher Scientific). Sanger sequencing data were analyzed using Codon Code Aligner v5.0.2, (CodonCode Corporation, Centerville, MA, USA) and Mutation Surveyor v5.0, (SoftGenetics, State College, PA, USA).
Data analysis
The sequence data were processed using standard Ion Torrent Suite™ Software running on the Torrent Server (Thermo Fisher Scientific). Raw signal data were analyzed using Torrent Suite™ version 4.4, 4.6 or 5.0. The pipeline included signaling processing, base calling, quality score assignment, adapter trimming, PCR duplicate removal, read alignment to human genome 19 reference (hg19), quality control of mapping quality, coverage analysis, and variant calling. Coverage analysis and variant calling used Torrent Variant Caller plugin software (Version 4.4, 4.6 or 5.0) in the Torrent Server. The variant caller parameter setting was germline PGM high stringency. Following data analysis, annotation of single-nucleotide variants, insertions, deletions, and splice site alterations were performed by the Ion Reporter™ Server System (Thermo Fisher Scientific), which identified nonsynonymous mutations. Splice site alteration were analyzed 2 bp upstream or downstream of exon–intron boundaries. Sequence data were visually confirmed with the Integrative Genomics Viewer (IGV) and any sequence, alignment, or variant call error artifacts were discarded. Nonsynonymous mutations were annotated using the Breast Cancer Information Core (BIC) database (https://research.nhgri.nih.gov/projects/bic/index.shtml) and ClinVar (http://www.ncbi.nlm.nih.gov/clinvar/).Citation14 Minor allele frequency was determined from the 1000 Genomes Project database.Citation15 The 5000 Exome project (http://evs.gs.washington.edu/EVS/) and The Human Genetic Variation Database (http://www.genome.med.kyoto-u.ac.jp/SnpDB) were used to identify the pathogenic conditions of the BRCA1/2 gene mutations.
Statistics
Percentage was calculated wherever necessary.
Results
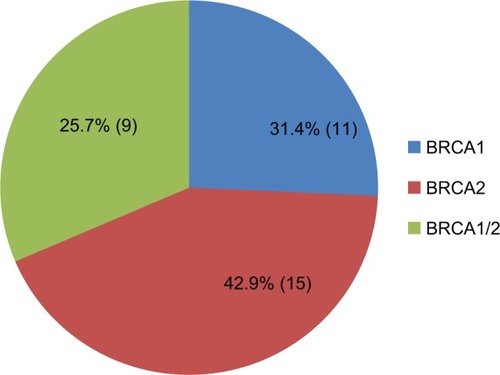
After analyzing 79 referral cases of women ranging in age between 23 and 72 years, 35 BC-positive (44.30%) cases were detected with germline gene mutations. Among them, 11 cases were with BRCA1 gene mutations (31.4%) followed by 15 with BRCA2 gene mutations (42.9%), and both BRCA1 and BRCA2 mutations were found in nine cases (25.7%) ().
Figure 1 Patients (n=35) with BRCA1 and BRCA2 mutations.
Mutation types in BRCA1 and BRCA2
A total of 82 mutations, 39 with BRCA1 (39/82; 47.6%) and 43 with BRCA2 (43/82; 52.4%), were identified in 35 cancer patients. A total of 72 (72/82) missense mutations (87.8%) with amino acid replacement (BRCA1, 36/82, 43.9%; BRCA2, 36/82, 43.9%) were detected with two novel mutations (BRCA1; two splice sites). Among other types, five frameshift mutations (5/82:6.1%) were detected in five cases (exon 1, exon 14 in BRCA1; exon 6, exon 10, exon 11 in BRCA2), where three were novel types. Others were four nonsense mutations of BRCA2 (4/82:4.9%) and one in-frame deletion of BRCA1 (1/82:1.2%). A total of five novel mutations were present with three frameshift and two missense (splice site) mutations in our study (; ). Moreover, familial (20) and sporadic (15) cases were not significantly different ().
Figure 2 Mutation types in BRCA1 and BRCA2 mutations.
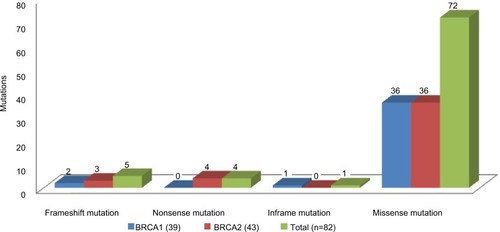
Table 1 Patients with BRCA1 and BRCA2 mutations
Frequency of SNPs in BRCA1 and BRCA2 and pathologic variants
The single-nucleotide polymorphism (SNP) frequency was higher in exons 10, 11 and 16 of BRCA1 and BRCA2 followed by exons 9, 2 and 3. In BRCA1, exon 9 had two splice site SNPs which were pathogenic and one SNP likely benign (total of three). Exon 10 had seven SNPs benign, two each with likely pathogenic and variant of unknown significance (VUS) (total of four). Exon 11 contributed 12 SNPs, each with two amino acid changes showing likely benign and two with VUS having two amino acid changes. The exon 16 possessed six benign and two with VUS. In BRCA2, exon 10 showed nine SNPs likely benign/benign/likely pathogenic, four SNPs likely benign/likely pathogenic and one with VUS, respectively. Exon 11 exhibited seven SNPs likely benign/benign/likely pathogenic and three likely benign/benign. It also had three VUS with two amino acid changes followed by one likely benign. Exon 16 showed six SNPs likely benign, whereas exon 3 and exon 2 had one each of VUS and benign SNPs (two), respectively (). The SNPs of each exon percent of two germline genes, i.e., BRCA1 (36) and BRCA2 (36), are shown in and .
Figure 3 BRCA1 SNP mutations.
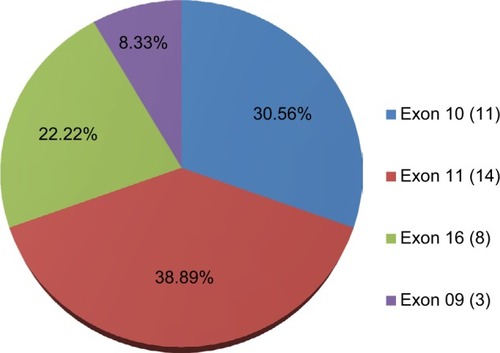
Figure 4 BRCA2 SNP mutations.
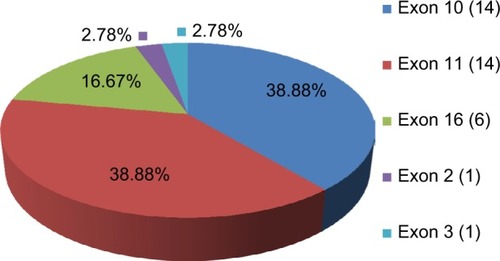
Table 2 Types of polymorphic SNPs in BRCA1 and BRCA2
Age at diagnosis and mutation frequency
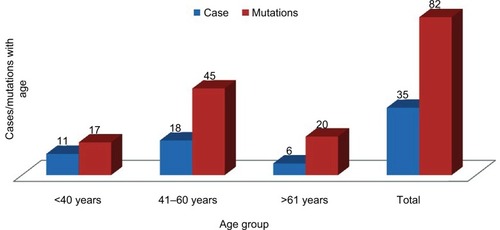
The average age was 47.3 ± 3.2 ranging from 23 to 72 years. The age group 41–60 years (18 patients) had a high frequency of mutations (45/82: 54.9%) followed by >61 years (six) with 20 (20/82: 24.4%) and <40 years (11) with 17 (17/82: 20.7%). However, the 23–60 years group had 62 mutations (62/82: 75.6%) ().
Figure 5 Cases and mutations in age groups of our study.
Discussion
BC can be caused by germline mutations in BRCA1 and BRCA2, or by several other genes. In our cohort, we analyzed 79 referral cases using NGS and gene sequencing of Sanger with other reports of clinicians for phenotypic variations. Only 35 cases (44.30%) detected positive for BRCA1 or BRCA2. The mutations in BRCA2 (52.4%) were marginally higher than those in BRCA1 (47.6%) in our study. Similar results were observed in a North Indian population where BRCA2 had maintained equal distribution of BRCA1/2.Citation2 BRCA2 mutations contribute more than BRCA1 mutations in Philippine women in support of our data.Citation17 Jang et alCitation18 in Korean cases found no variations between BRCA1 and BRCA2 mutations. But in a South Indian population, BRCA1 mutations were more than BRCA2 germline mutations.Citation19
Others included five frameshift mutations, where protein was truncated altering its structure and function. In these, three were novel types – BRCA2 (exon 6) of c.484-484delG, BRCA2 (exon 10) of c.2169_2170InsA and BRCA1 (exon 14) of c.4442_4442delG) – and the other two were referenced in BIC and the SNP database. All were pathogenic and familial in our study. Four nonsense mutations were found in our cancer patients, with two each of familial and sporadic in BRCA2 mutations, and these could lead to premature termination of protein due to change in specific amino acid proving lethal, and referenced in database. Furthermore, only one in-frame deletion in exon 10 of BRCA1(c.3328_3330delAAG) was detected in our cohort which was familial and deleterious. Finally, in our study, five novel mutations were detected, i.e., splice-site missense (two) and frameshift (three) types. Similar mutations are well reported globally in BC and ovarian cancer women except novel mutations in our report.Citation12,Citation18,Citation19
High frequency of missense polymorphism (72) in women with BC is seen in our study, which was equal in both genes. Exons 10, 11 and 16 were more than exons 2, 3 and 9 of both genes, and all these may be responsible for BC in these patients depending upon amino acid substitution and its subsequent effect on protein structure and function.Citation2 Few missense polymorphic SNPs detected in Algerian populations were tested negative for both gene mutations, but could have a role as a susceptibility BC marker in BRCA1/2.Citation20 In both familial (20) and sporadic (15) cases, few expressed multiples of polymorphic sites as found by others.Citation20 In these mutations, two were found to be novel (two splice sites) in BRCA1 only, i.e., c.5137+1G>A in two cases in which G was replaced by A, and others were registered. In our cohort, as per database of ClinVar (National Center for Biotechnology Information [NCBI]), dbSNP and BIC revealed most of them were benign in BRCA1 except two splice site types (c.5137+1G>A) which were pathogenic (No. 8, 11 of ) and one with VUS (p.A841T). In BRCA2, five SNPs, p.Cys315Ser, p.Gly1593Asp(2), p.Lys2077Asn and p.Asn2106Ser were with VUS and others in both genes, and were benign only. However, these can be confirmed further by other predictive programs such as POLYPHEN 2, SIFT and PROVENCitation20 as in silico analysis may not provide the pathogenicity of them. However, controversial reports exist about the role of SNPs in these BRCA1/2 genes for the induction of human breast and ovarian cancer (HBOC).Citation2,Citation18,Citation21,Citation22,Citation23 Dombernowsky et alCitation22 reported that missense mutations cannot explain the risk of HBOC in women with familial history. Contrarily, Dodova et alCitation21 in their study implicated the role of missense variants which may be deleterious. In an Iranian population, Neamatzadeh et alCitation23 detected these polymorphic SNPs at higher frequency in BRCA1 and BRCA2 genes compared to control subjects supporting our data. Valarmathi et alCitation7 in their study indicated that many of these variants are proposed to be deleterious in the Indian population. We further propose that polymorphic sites in BRCA1 and BRAC2 genes to cause cancer are dependent on the frequency and nature of amino acid replaced in the protein in regard to their lethality. These SNPs of BRCA1/2 could be related to the pathological condition of BC patients which differ from pathogenic, likely pathogenic, benign and likely benign, VUS or mixed types. It requires further elucidation by analyzing BRCA1/2 haplotypes in relation to gene mutations.Citation24
In our study, young age groups (23–60 years) had more frequency of mutations 62/82 (75.6%). This indicated that age is also one of the factors to be noted including other lifestyles, ethnicity and geographic distribution for these differences in their frequency as reported earlier.Citation25,Citation26,Citation27 Mannan et alCitation12 found in their cohort, that the mutation rate was proportionally higher in patients aged <50 years. Wong et alCitation26 reported that early age is to be considered for higher rate of BRCA gene variants in HBOC patients in support of our observations. In the Indian population, the proportion of patients with early onset of mutations to BC is also much higher than in Caucasians. In North India,Citation2 lower BRCA mutations in early age were reported in comparison with other ethnic populations. Vaidyanathan et alCitation8 detected a high rate of germline mutations with early age, like that of Mannan et alCitation12 and our report. This discrepancy in these cohorts is related to the latest technologies including the gene panel used for monitoring gene mutations profiles in Indian patients.
In conclusion, BRCA2 gene mutations were marginally more than BRCA1 mutations. Young age groups had high frequency mutations which were also positively comparable. Polymorphic SNPs were higher than others, with five novel mutations, i.e., three frameshift and two spice site types, where synthesis of premature or truncating proteins occurs by amino acid replacement for their termination, respectively. Nonsense, in-frame and frameshift with splice site were pathogenic, and other polymorphic SNPs were benign, pathogenic and variant of unknown significance. The association of these mutations with haplotypes of BRCA1/2 needs to be evaluated in our future work in addition to age. This may help understand the role of SNPs in the causation of BC for better treatment and genetic testing highlighting sporadic and familial types in the Indian population.
Author contributions
Drs Nidhi D Shah and Parth S Shah contributed to writing the results and discussion during manuscript preparation when they visited India. Hari Shankar P Ray and Yash Y Panchal were involved in the collection of blood from the patients after duly completed consent forms, blood analysis, DNA extraction, DNA sequencing, and data analysis of 79 patients. Dr Sandip C Shah, Dr Bhavini S Shah and Dr Mandava V Rao contributed to the preparation of reports after finalization of the results and the final preparation of the manuscript for submission to the journal. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors are thankful to all the staff including the clinicians of Supratech Micropath Laboratory, Ahmedabad, India, for their continuous assistance in this work. Parth S Shah, Nidhi D Shah, Sandip C Shah and Bhavini S Shah are son, daughter-in-law, and father and mother, respectively, and run this research institute.
Disclosure
The authors report no conflicts of interest in this work.
References
- RajkumarTSoumittraNNancyKNShantaVBRCA 1, BRCA 2 and CHEK2 (1100 del C) germline mutations in hereditary and ovarian cancer families in South IndiaAsian Pac J Can Prev20034203208
- SaxenaSChakrabortyAKaushalMContributions of germline BRCA1 and BRCA2 sequence alterations to breast cancer in Northern IndiaBMC Med Gen2006775
- Indian Council of Medical Research (ICMR) NewsOver 17 lakh new cancer cases in India by 20202016 Available from: http://www.mid-day.com/articles
- MikiYSwensenJShattuck-EidensDA strong candidate for the breast and ovarian cancer susceptibility gene BRCA1Science199426666717545954
- Shattuck-EidensDMcClureMSimardJA collaborative survey of 80 mutations in BRCA, breast and ovarian cancer susceptibility gene. Implications for presymptomatic testing and screeningJAMA19952735355417837387
- Shattuck-EidensDOliphantAMcClureMBRCA1 sequence analysis in woman at high risk for susceptibility mutationsJAMA1997278124212509333265
- ValarmathiMTSawhneyMDeoSSShuklaNKDasSNNovel germline mutations in the BRCA1 and BRCA2 genes in Indian breast and ovarian cancer familiesHum Mutat200423205215
- VaidyanathanKLakhotiaSRavishankarHMTabassumUMukherjeeGSomasundaramKBRCA1 and BRCA2 germline mutation analysis among Indian woman from south India: identification of four novel mutations and high frequency occurrence of 185 del.AG mutationsJ Biosci20093441542219805903
- KaramiFMehdipourPA comprehensive focus on global spectrum of BRCA1 and BRCA2 mutations in breast cancerBiomed Res Int2013201392856224312913
- FerlayJSoerjomataramIDixshitRCancer incidence and mortility worldwide: sources methods and major patterns in GLOBOCAN 2012Int J Cancer2015136E35938625220842
- AlteriRBertautTBrintonLAon behalf of the American Cancer SocietyBreast cancer facts and figures 2015–2016Atlanta, GAAmerican Cancer Society2015138
- MannanAUSinghJLakshmikeshavaRDetection of high frequency mutations in a breast and ovarian cancer cohort: implications of embracing a multigene panel in molecular diagnosis in IndiaJ Hum Genet20166151552226911350
- TorreLABrayFSiegelRLFerlayJLortet-TieulentJJemalAGlobal cancer statistics, 2012CA Cancer J Clin2015658710825651787
- JemalACenterMMDeSantisCWardEMGlobal patterns of cancer incidence and mortality rates and trendsCancer Epidemiol Biomarkers Prev20101981893190720647400
- LandrumMJLeeJMRileyGRClinVar: public archive of relationships among sequence variation and human phenotypeNucleic Acids Res201442980985
- AbecasisGRAutonABrooksLDon behalf of the 1000 Genomes Project ConsortiumAn integrated map of genetic variation from 1,092 human genomesNature2012491566523128226
- De Leon MatsudaMLLiedeAKwanEBRCA1 and BRCA2 mutations among breast cancer patients from the PhilippinesInt J Cancer20029859660311920621
- JangJHLeeJEKwonMJSpectra of BRCA1 and BRCA2 mutations in Korean patients with breast cancer: the importance of whole gene sequencingJ Hum Genet20125721221522217648
- SoumittraNMeenakumariBParijaTMolecular genetics analysis of hereditary breast and ovarian cancer patients in IndiaHeredi Clin Pract2009713
- CherbalFSalhiNBakourRAdaneSBoualgaKMailletPBRCA1 and BRCA2 unclassified variants and missense polymorphisms in Algerian breast/ovarian cancer familiesDis Markers20123234335322684231
- DodovaRIMitkovaAVDachevaDRSpectrum and frequencies of BRCA1/2 mutations in Bulgarian high risk breast cancer patientsBMC Cancer20151552326183948
- DombernowskySLWeischerMFreibergJJBojesenSETybjaerg-HansenANordestgaardBGMissense polymorphisms in BRCA1 and BRCA2 and risk of breast and ovarian cancerCancer Epidemiol Biomarkers Prev2009823392342
- NeamatzadehHShiryazdiSMKalantarSMBRCA1 and BRCA2 mutations in Iranian breast cancer patients: A systematic reviewJ Res Med Sci20152028429326109977
- JudkinsTHendricksonBCDeffenbaughAMApplication of embryonic lethal or other obvious phenotypes to characterize the clinical significances of genetic variants found in trans with known deleterious mutationsCancer Res200565100961010316267036
- GholipoorfeshkechehRArjunanSGenotyping frequent BRCA1 SNPs in familiar breast cancer in Indian population by restriction fragment length polymorphism and sequencingAdv Appl Sci Res20145262267
- WongYEYhenkavSChanTHCPredictive factors for BRCA1 and BRCA2 genetic testing in an Asian based populationPLoS One201510112
- SharmaSRajaramSSharmaTRole of BRCA1 and BRCA2 gene mutations in epithelial ovarian cancer in Indian population: a pilot studyInt J Biochem Mol Biol20145111024955283