
Abstract
Reported cases of distal 15q interstitial duplications are uncommon and do not result in a recognizable pattern of abnormalities. Some studies report prenatal overgrowth, while others describe growth retardation. We present molecular cytogenetic characterization of a 14 Mb interstitial duplication, encompassing 81 Online Mendelian Inheritance in Man (OMIM) genes, in a fetus with single umbilical artery and short limbs. We propose that growth restriction, previously described and present in our patient, may be due to duplication of a gene or genes contained in the 15q24 region.
Introduction
Reported cases of distal 15q duplications are very uncommon; in fact, there are ~100 cases reported, and even less de novo duplications as in this case report. Previous authors have described a distal 15q trisomy syndrome characterized by prenatal and postnatal overgrowth, developmental delay, craniofacial and skeletal malformations, and genital abnormalities, particularly in affected males.Citation1 There are only few reported cases of de novo single duplication of 15q24-qter region.Citation2–Citation7 The type and severity of reported anomalies depend on the length and location of the duplicated region of chromosome 15q, but there is a common phenotype consisting of minor craniofacial anomalies (downslanting palpebral fissures and ptosis, large prominent nose, facial asymmetry, and micrognathia), arachnodactyly and camptodactyly, heart defects (septal communications, patent ductus arteriosus, pulmonary artery stenosis), hypogonadism and cryptorchidism, scoliosis, severe developmental delay, and anencephaly.Citation3
Reported patients with trisomy of 15q25/q26qter have presented prenatal and postnatal overgrowth.Citation1,Citation2,Citation4–Citation6 Overgrowth has been attributed to overexpression of the IGF1R gene, which is located on 15q26.3. On the contrary, patients with trisomy of 15q24qter region exhibit growth restriction/intrauterine growth restriction (IUGR) and developmental delay.Citation2,Citation7–Citation10
In this report, we present a prenatal diagnosis of a fetus with single umbilical artery, short limbs, and a de novo duplication of 15q24.3q26.1.
Clinical report
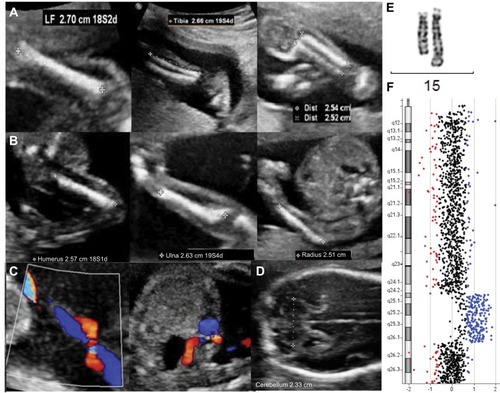
A 30-year-old patient had a routine anomaly scan at 21+1 weeks gestation. Although her first trimester combined screening risk was low, the ultrasound scan showed a male fetus with short long bones (−2.5 standard deviation [SD]), according to Chitty and AltmanCitation11 (femur length [FL]: 27–27 mm, tibia: 25–26 mm, fibula: 25–25 mm, humerus: 25-26 mm, ulna: 25–26 mm, radius: 25–25 mm) but with normal morphology and mineralization signs, corresponding to a 19+5 gestation week fetus, with an estimated weight of 289 g (according to Hadlock tables, biparietal diameter [BPD] 45 mm, head circumference [CC] 174 mm, abdominal circumference [AC] 147 mm) (). The remaining anatomy was normal except for a single umbilical artery (). At Week 24, the fetus still showed 2-week-younger measurements, and the transverse cerebellar diameter was 23 mm, below the 5th centile, according to Snijders and NicolaidesCitation12 (). After ruling out an error in pregnancy dating, an amniocentesis was performed to find out the origin of the growth delay. The fetus karyotype showed a 15q duplication, visible by conventional G-banding (). The duplication was considered de novo because the parents displayed normal karyotypes on testing. Comparative genomic hybridization (CGH) array (KaryoNIM® Prenatal 60K; NIMGenetics, Madrid, Spain) was carried out to determine the size and extent of the duplication (). It was an interstitial duplication of 14 Mb: 46,XY,dup(15)(q24.3q26.1).arr15q 24.3q26.1(76223116-90340143)×3. The duplicated region contains 257 genes in the Genes on Sequences National Center for Biotechnology Information (NCBI) map, of which 81 are in the Online Mendelian Inheritance in Man (OMIM) database. The patients underwent genetic counseling and opted for a termination of pregnancy. They declined postmortem examination.
Figure 1 Morphologic ultrasonogram of a 21+1-week male fetus with 19+5-week-ultrasound parameters.
Abbreviation: CGH, comparative genomic hybridization.
Written informed consent has been provided by the patient to have the case details and any accompanying images published.
Discussion
The fetus described in this report exhibited single umbilical artery, had short limbs, and had a de novo duplication of 15q24.3q26.1. Based on the cases reported to date, it is not clear whether the duplication of 15q24-qter results in a recognizable pattern of abnormalities.
Zollino et alCitation1 reported a total of 32 patients with 15q duplications and divided them in two groups: one group had trisomy for 15q21-24qter, showing microcephaly and normal prenatal growth; and the other group showed trisomy 15q25-26qter, characterized by prenatal overgrowth, macrocephaly, and craniosynostosis. The cause of overgrowth has been thought to be related to a dosage excess of the IGF1R gene, located in 15q26.3.Citation1,Citation2,Citation4–Citation6 This gene is not contained in the region duplicated in the fetus we report herein.
Roggenbuck et alCitation7 reported two unrelated cases with single 15q24q26.3 duplication showing small size. O’Connor et alCitation6 reported a patient with a single 15q24qter trisomy and normal sizes/measures at birth. Genesio et alCitation8 described the case of a multiple-malformed newborn with IUGR and a de novo inverted duplication of 15q21q26.3, with three copies of the IGF1R gene. The authors hypothesized that the IUGR depends on global transcription dysregulation more than the impairment of a single gene specifically correlated to the malformation.Citation8 El-Hattab et alCitation13 reported a case with short stature and developmental delay and a 15q24 microduplication that contained the OMIM genes SCAPER, ISL2, EFTA, NRG4, FBXO22, and UBE2Q2. All these genes, except UBE2Q2, are duplicated in the fetus reported here. It is tempting to speculate that dosage excess of genes located in 15q24 leads to short limbs/IUGR instead of tall stature.
In the case of a fetal ultrasonogram displaying short long bones (<5th percentile), it is advisable to analyze their morphology and mineralization, as well as rule out a possible error in gestational dating and femur–humerus confusions. Then, differential diagnoses should include constitutional short stature, IUGR, skeletal dysplasia such as achondroplasia, and chromosomal abnormalities such as deletion of 15q24, similar to this case report.
This study underscores the utility of the CGH array in the characterization of the size and nature of rearrangements, as well as in predicting the severity of phenotypes, which depends on the length and location of the duplicated region. Associations between phenotypes and copy number variations of small chromosome regions provide valuable information about clinically important genes or regulatory elements and allow the investigation of their role in the phenotypes. Systematic characterization of newly reported patients provides useful information for clinicians and patients.
Acknowledgments
The authors wish to thank Miss Jéssica Calvo for technical support. This work was supported by Citolab and Cátedra de Biomedicina Reproductiva Vistahermosa. The abstract of this work was presented at the 10th European Cytogenetics Conference, Strasbourg, France, July 2015.
Disclosure
The authors report no conflicts of interest in this work.
References
- ZollinoMTizianoFDi StefanoCNeriGPartial duplication of the long arm of chromosome 15: confirmation of a causative role in craniosynostosis and definition of a 15q25-qter trisomy syndromeAm J Med Genet199987539139410594876
- CannarellaRMattinaTCondorelliRAChromosome 15 structural abnormalities: effect on IGF1R gene expression and functionEndocr Connect20176752853928899882
- ChenCPChenCYChernSRMolecular cytogenetic characterization of a duplication of 15q24.2-q26.2 associated with anencephaly and neural tube defectTaiwan J Obstet Gynecol201756455055328805617
- Gutiérrez-Franco MdeLMadariaga-Campos MdeLVásquez-VelásquezAIMatuteEGuevara-YáñezRRiveraHA girl with 15q overgrowth syndrome and dup(15)(q24q26.3) that included telomeric sequencesKorean J Lab Med201030331832420603595
- KimEYKimYKKimMKA case of de novo duplication of 15q24-q26.3Korean J Pediatr201154626727121949522
- O’ConnorRAl-MurraniAAftimosSPure duplication of the distal long arm of chromosome 15 with ebstein anomaly and clavicular anomalyCase Rep Genet201120115
- RoggenbuckJAMendelsohnNJTenenholzBLaddaRLFinkJMDuplication of the distal long arm of chromosome 15: report of three new patients and review of the literatureAm J Med Genet2004126A439840215098238
- GenesioRDe BrasiDContiAInverted duplication of 15q with terminal deletion in a multiple malformed newborn with intrauterine growth failure and lethal phenotypeAm J Med Genet A2004128A442242815264291
- MillerMSRaoPNDudovitzRNFalkREEbstein anomaly and duplication of the distal arm of chromosome 15: report of two patientsAm J Med Genet2005139A214114516278886
- RoetzerKMSchwarzbraunTObenaufACHauserESpeicherMRFurther evidence for the pathogenicity of 15q24 microduplications distal to the minimal critical regionsAm J Med Genet A2010152A123173317821108404
- ChittyLSAltmanDGCharts of fetal size: limb bonesBJOG2002109891992912197373
- SnijdersRJNicolaidesKHFetal biometry at 14-40 weeks’ gestationUltrasound Obstet Gynecol19944344812797224
- El-HattabAWSmolarekTAWalkerMERedefined genomic architecture in 15q24 directed by patient deletion/duplication breakpoint mappingHum Genet2009126458960219557438