
Abstract
Introduction
Exome sequencing is recognized as a powerful tool for identifying the genetic cause of intellectual disability (ID). It is uncertain, however, whether only the exome of the proband should be sequenced or if the sequencing of parental genomes is also required, and the resulting increase in diagnostic yield justifies the increase in costs.
Patients and methods
We sequenced the exomes of eight individuals with sporadic syndromic ID and their parents.
Results and discussion
Likely pathogenic variants were detected in eight candidate genes, namely homozygous or compound heterozygous variants in three autosomal genes (ADAMTSL2, NALCN, VPS13B), one in an X-linked gene (MID1), and de novo heterozygous variants in four autosomal genes (RYR2, GABBR2, CDK13, DDX3X). Two patients harbored rare variants in two or more candidate genes, while in three other patients no candidate was identified. In five probands (62%), the detected variants explained their clinical findings. The causative recessive variants would have led to diagnosis even without parental exome sequencing, but for the heterozygous dominant ones, the exome trio-based approach was fundamental in the identification of the de novo likely pathogenic variants.
Introduction
Intellectual disability (ID) is a complex and heterogeneous clinical condition that affects 1%–2% of the general population, and can result from genetic or environmental factors, or a combination of both. However, most severe forms of ID have a single genetic basis, ranging from chromosomal alterations to point mutations.Citation1–Citation3
About 700 genes have already been associated with ID;Citation4 however, a clear genetic explanation for the phenotype of many patients remains unknown. The implementation of whole exome sequencing (WES) in the last decade increased the identification yield of new mutations and genes associated with various diseases, and led to the demonstration that de novo mutations are a frequent cause of ID.Citation5 WES has also successfully identified autosomal recessiveCitation6,Citation7 and X-linkedCitation8,Citation9 causative mutations in ID cohorts.
In non-familial cases, the situation is complicated by the lack of information on the type of inheritance underlying the phenotype. To date, studies of sporadic cases that have been performed using WES to elucidate the causes of ID have led to the diagnosis of 15%–30% of the patients.Citation10–Citation12
Through the exome sequencing of probands and their unaffected parents (trio analysis), this work aimed at identifying variants, which could explain ID in sporadic cases, and evaluating the utility of trio-based exome sequencing in the identification of pathogenic variants.
Patients and methods
The patients were referred to the Genetic Counseling Service of the Department of Genetics and Evolutionary Biology, Institute of Biosciences, University of São Paulo. The study was approved by the Ethics Committee of the institution. Written informed consent was obtained from the parents of all patients.
The patients had ID ranging from moderate to severe and other associated clinical signs. summarizes the main clinical findings of the patients in the cohort.
Table 1 Main clinical findings of the patients in the cohort
Genomic DNA from peripheral blood samples was extracted, according to standard procedures. Fragile-X syndrome (AmplideX® FMR1; Asuragen, Austin, TX, USA) and genomic imbalances (180K platform; Agilent Technologies, Santa Clara, CA, USA, or 850K platform; Illumina, San Diego, CA, USA) had previously been excluded in these families.
Genomic libraries were constructed using the SureSelect XT or SureSelect QXT kit V6 (Agilent SureSelect Whole Exome Enrichment kit), according to the manufacturer’s instructions, with 100× coverage and 90% of the targets covered at 20×; sequencing was performed on the Hiseq 2500 sequencer from Illumina. The quality of the sequencing was verified through the FastQC program (Babraham Institute). The raw reads were aligned to the reference genome (GRCh37/hg19), using the Burrows–Wheeler Aligner,Citation13 and pre-processed according to GATK toolkit,Citation14 which involves indel realignment, base quality score recalibration, base alignment quality scoring, and variant calling. Filtering and prioritization were conducted using VarSeq® software (Golden Helix, Bozeman, MT, USA) and variant effect predictor. After coding, non-synonymous variants fitting the models of dominant de novo or recessive homozygote/compound heterozygote/hemizygote were filtered per frequency (1%) against the databases: NHLBI ESP6500SI-V2 exomes variant frequencies, ClinVar,Citation15 dbSNP138, 1000 Genome Project,Citation16 ExAC Browser,Citation17 and ABRAOM.Citation18
After variant filtering, in silico prediction of pathogenicity of variants was performed using five prediction algorithms, namely SIFT,Citation19 PolyPhen-2,Citation20 Mutation Taster,Citation21 Mutation Assessor, and FATHMM.Citation22 The VarElect online tool was used to prioritize variants according to the phenotype. The OMIM database and scientific literature were used to compare the expected phenotypes with the clinical features of the patients.
Potentially pathogenic variants in the proband were validated by Sanger sequencing also performed to analyze the presence or absence of the same variants in their parents. Variants were classified according to the ACMG guideline.Citation23
Results and discussion
We sequenced the exomes (WES) of eight patients with idiopathic syndromic ID and their parents (trios). Rare variants in eight genes were detected in five patients: a homozygous variant in ADAMTSL2; compound heterozygous variants in NALCN and VPS13B; a variant in the X-linked gene MID1; and four heterozygous de novo variants in the autosomal genes RYR2, GABBR2, DDX3X, and CDK13. summarizes the WES findings; the variants in bold were considered as causative of the clinical phenotypes. The likely pathogenic variants found in this study were missense, except for those in VPS13B (stop gain), and the clinical impact could only be estimated, even with the help of prediction algorithms. illustrates the results, showing the de novo variant detected in GABBR2 and the maternally inherited variant in MID1.
Figure 1 Example of pathogenic mutations identified in the cohort.
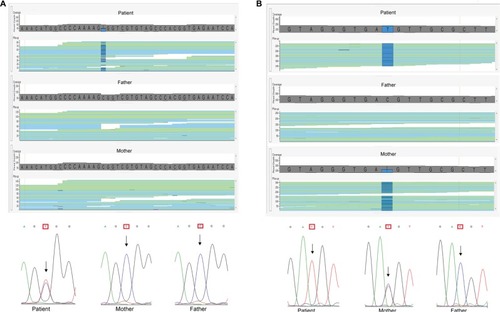
Table 2 The candidate mutations identified in five of the patients of the cohort
As shown in , Patient 1 had rare variants of uncertain significance (VUS) in three different genes:a missense variant in RYR2, a gene associated with dominant arrhythmogenic right ventricular dysplasia or ventricular tachycardia, neither of the conditions documented in the patient; a homozygous missense variant in ADAMTSL2, whose mutations are known to cause recessive Ehlers–Danlos syndrome, not compatible with the patient’s phenotype; and a maternally inherited missense variant in the MID1 gene, associated with Opitz G/BBB syndrome, which could explain the cognitive impairment, cardiac defects, and cryptorchidism exhibited by the patient. The variant in MID1 was predicted as damaging (SIFT – http://sift.jcvi.org/) or probably damaging (PolyPhen-2 – http://genetics.bwh.harvard.edu/pph2/), but the RYR2 variant was also considered probably damaging, and diagnosis of Opitz G/BBB syndrome mostly relied on the fact that the MID1 variant could explain the phenotype.
Patients 4, 6, and 8 carried de novo variants. The variants in GABBR2 and in CDK13 had not been described in the searched databases (GnomAD, dbSNP, and ClinVar) and are therefore novel, while the variant in DDX3X had already been described in ClinVar and classified as probably pathogenic.
Patient 4 harbored VUS in GABBR2. Variants in this gene have been described recently, and the associated phenotype has not been consolidated in OMIM, but they emerge as important contributors for epileptic encephalopathies,Citation24–Citation27 in accordance with our patient clinical phenotype.
Patient 6 carried a known pathogenic variant in DDX3X; the disorder associated with this gene, x-linked mental retardation, is clinically variable and includes other symptoms in addition to cognitive impairment, such as hearing loss, which is present in this patient. On the other hand, polycystic kidney disease, exhibited by the patient, has not been reported in DDX3X mutation carriers. Although mutations in DDX3X have only recently been reported, it is estimated that they are responsible for 1%–3% of idiopathic ID in females.Citation28
Patient 8, carrier of a likely pathogenic variant in CDK13, exhibited ID and dysmorphic features commonly associated with CDK13 mutations, including hypertelorism, telecanthus, inverse epicanthal folds, broad nasal bridge, and low-set, posteriorly rotated ears. She did not present heart defects and seizures, which are frequently found among patients carrying CDK13 mutations. A recent paper by Hamilton et al shows that mutation in CDK13 results in syndromic ID, with or without congenital heart disease and seizures.Citation28
In Patient 5, we identified potential pathogenic variants in more than one candidate gene. She was a compound heterozygote for variants in NALCN, a gene associated with recessive syndromic hypotonia and psychomotor retardation. This would have been considered as the probable cause of the phenotype if she was not a compound heterozygote for loss of function variants in VPS13B, associated with Cohen syndrome. The patient presented many clinical signs of Cohen syndrome in addition to ID, including low birth weight (2300 g), short stature (<5 centile), microcephaly (<<2 centile), palpebral ptosis, myopia, decreased visual acuity, optic atrophy, and neutropenia, but loss of function of both VPS13B alleles would have led to Cohen syndrome diagnosis even if phenotypic data were not available. It is disturbing to realize that the NALCN variants, which were predicted to be damaging/likely damaging by SIFT and PolyPhen-2, respectively, would likely be considered responsible for the phenotype in the absence of the VPS13B variants. However, we cannot exclude the possibility that the NALCN variants contribute to the patient’s phenotype.
In the last few years, exome sequencing has become an important clinical tool in genetic diagnosis, at least in developed countries. An issue on the procedure is whether only the exome of the proband should be sequenced or sequencing the trio (probands plus parents) would be more cost-effective. Obviously, the latter approach costs three times more, and the magnitude of the increase in diagnostic yield is not clear, depending on the criteria of patient referral. Using the trio analyses of exome sequencing, we identified the probable genetic cause of the clinical phenotype in five out of eight patients with sporadic syndromic ID, which resulted in a diagnostic rate of 62%. It is important to note that some rare variants that were considered as candidate for the phenotypes were later excluded with the release of a database of variants in the Brazilian Population (http://abraom.ib.usp.br/), being relatively common variants among Brazilians.Citation18
In the two patients with the diagnosis of recessive disorders, the causative mutations would have been identified even if only the proband exomes had been sequenced. However, in the three patients with dominant disorders, parental exome sequencing was instrumental to reach the conclusion that the de novo variants were likely pathogenic. A recent publication from the Deciphering Developmental Disorders Study on the exomes of 4,293 families reported damaging de novo mutations in 42% of the cohort.Citation29 These results clearly show that parental exome sequencing is fundamental for efficient diagnosis in isolated cases.
Acknowledgments
This work was supported by scholarships from the Brazilian National Council for Scientific and Technological Development (CNPq—306879/2014-0; CR) and grants from the São Paulo Research Foundation (FAPESP—2012/50981-5 and 2013/08028-1). We thank our colleagues from the University of São Paulo who contributed with ideas and expertise for the research and, of course, our collaborators from other department of the University of São Paulo and AC Camargo Cancer center for all the help during this work. We would like to especially thank those who took time to read and improve this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
- TopperSOberCDasSExome sequencing and the genetics of intellectual disabilityClin Genet201180211712621627642
- MoeschlerJBShevellMAmerican Academy of Pediatrics Committee on GeneticsClinical genetic evaluation of the child with mental retardation or developmental delaysPediatrics200611762304231616740881
- RopersHHGenetics of early onset cognitive impairmentAnnu Rev Genomics Hum Genet20101116118720822471
- VissersLEGilissenCVeltmanJAGenetic studies in intellectual disability and related disordersNat Rev Genet201617191826503795
- VissersLEde LigtJGilissenCA de novo paradigm for mental retardationNat Genet201042121109111221076407
- ÇalışkanMChongJXUricchioLExome sequencing reveals a novel mutation for autosomal recessive non-syndromic mental retardation in the TECR gene on chromosome 19p13Hum Mol Genet20112071285128921212097
- NajmabadiHHuHGarshasbiMDeep sequencing reveals 50 novel genes for recessive cognitive disordersNature20114787367576321937992
- PhilipsAKSirénAAvelaKX-exome sequencing in Finnish families with intellectual disability – four novel mutations and two novel syndromic phenotypesOrphanet J Rare Dis201494924721225
- Bissar-TadmouriNDonahueWLAl-GazaliLNelsonSFBayrak-ToydemirPKantarciSX chromosome exome sequencing reveals a novel ALG13 mutation in a nonsyndromic intellectual disability family with multiple affected male siblingsAm J Med Genet A2014164A116416924501762
- VolkAConboyEWicalBPattersonMKirmaniSWhole-exome sequencing in the clinic: lessons from six consecutive cases from the clinician’s perspectiveMol Syndromol201561233125852444
- MonroeGRFrederixGWSavelbergSMEffectiveness of whole-exome sequencing and costs of the traditional diagnostic trajectory in children with intellectual disabilityGenet Med201618994995626845106
- ChérotEKerenBDubourgCUsing medical exome sequencing to identify the causes of neurodevelopmental disorders: experience of 2 clinical units and 216 patientsClin Genet201893356757628708303
- LiHDurbinRFast and accurate short read alignment with Burrows-Wheeler transformBioinformatics200925141754176019451168
- DePristoMABanksEPoplinRA framework for variation discovery and genotyping using next-generation DNA sequencing dataNat Genet201143549149821478889
- LandrumMJLeeJMBensonMClinVar: public archive of interpretations of clinically relevant variantsNucleic Acids Res201644D1D862D86826582918
- AutonAAbecasisGRAltshulerDMA global reference for human genetic variationNature2015526687426432245
- LekMKarczewskiKJMinikelEVExome Aggregation ConsortiumAnalysis of protein-coding genetic variation in 60,706 humansNature2016536761628529127535533
- NaslavskyMSYamamotoGLde AlmeidaTFExomic variants of an elderly cohort of Brazilians in the ABraOM databaseHum Mutat201738775176328332257
- KumarPHenikoffSNgPCPredicting the effects of coding non-synonymous variants on protein function using the SIFT algorithmNat Protoc2009471073108119561590
- AdzhubeiIASchmidtSPeshkinLA method and server for predicting damaging missense mutationsNat Methods20107424824920354512
- SchwarzJMCooperDNSchuelkeMSeelowDMutationTaster2: mutation prediction for the deep-sequencing ageNat Methods201411436136224681721
- ShihabHAGoughJMortMCooperDNDayINGauntTRRanking non-synonymous single nucleotide polymorphisms based on disease conceptsHum Genomics201481124980617
- RichardsSAzizNBaleSACMG Laboratory Quality Assurance Committee Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular PathologyGenet Med201517540542425741868
- AppenzellerSBallingRBarisicNEuroEPINOMICS-RES Consortium; Epilepsy Phenome/Genome Project; Epi4K ConsortiumDe novo mutations in synaptic transmission genes including DNM1 cause epileptic encephalopathiesAm J Hum Genet201495436037025262651
- HamdanFFMyersCTCossettePHigh rate of recurrent de novo mutations in developmental and epileptic encephalopathiesAm J Hum Genet2017101566468529100083
- YooYJungJLeeYNGABBR2 mutations determine phenotype in Rett syndrome and epileptic encephalopathyAnn Neurol201782346647828856709
- Snijders BlokLMadsenEJuusolaJMutations in DDX3X are a common cause of unexplained intellectual disability with gender-specific effects on Wnt signalingAm J Hum Genet201597234335226235985
- HamiltonMJCaswellRCCanhamNHeterozygous mutations affecting the protein kinase domain of CDK13 cause a syndromic form of developmental delay and intellectual disabilityJ Med Genet2018551283829021403
- Deciphering Developmental Disorders StudyPrevalence and architecture of de novo mutations in developmental disordersNature2017542764243343828135719