
Abstract
Achondroplasia is the most common form of skeletal dysplasia, resulting in disproportionate short stature, and affects over 250,000 people worldwide. Individuals with achondroplasia demonstrate a number of well-recognized anatomical features that impact on growth and development, with a complex array of medical issues that are best managed through a multidisciplinary team approach. The complexity of this presentation, whereby individual impairments may impact upon multiple activity and participation areas, requires consideration and discussion under a broad framework to gain a more thorough understanding of the experience of this condition for individuals with achondroplasia. This paper examines the general literature and research evidence on the medical and health aspects of individuals with achondroplasia and presents a pictorial model of achondroplasia based on The International Classification of Functioning, Disability, and Health (ICF). An expanded model of the ICF will be used to review and present the current literature pertaining to the musculoskeletal, neurological, cardiorespiratory, and ear, nose, and throat impairments and complications across the lifespan, with discussion on the impact of these impairments upon activity and participation performance. Further research is required to fully identify factors influencing participation and to help develop strategies to address these factors.
Introduction
Achondroplasia is the most common form of nonlethal skeletal dysplasia, affecting more than 250,000 people worldwide.Citation1,Citation2 It is caused by a mutation in the gene that codes for fibroblast growth factor receptor 3 (FGFR3) and is transmitted as an autosomal dominant trait.Citation1,Citation3–Citation5 The estimated prevalence is currently 0.36 to 0.6 per 10,000 live births (1/27,780–1/16,670 live births).Citation6 The defining characteristics of achondroplasia are short stature with disproportionately shorter proximal limb bones, narrow trunk, and macrocephaly.Citation1,Citation7,Citation8 There is contraction at the base of the skull with a prominent forehead and flattened midface region and short, broad hands with a trident appearance of the fingers.Citation3,Citation8,Citation9
Disproportionate growth between endochondral bone and the underlying organs leads to a number of orthopedic, neurological, respiratory, ear, nose, and throat (ENT), and dental issues for individuals with achondroplasia.Citation8–Citation10 Whilst serious complications (such as sudden death due to severe compression of the spinal cord at the foramen magnum) impact on only 5%–10% of children,Citation8,Citation10 early monitoring and judicious medical and surgical interventions are important for reducing morbidity and mortality rates across the population.Citation1,Citation8,Citation10–Citation12 Knowledge regarding the type and timing of medical complications has led to international consensus for clinical management guidelines, documented originally in 1995 by the American Academy of Pediatrics, Committee on Genetics in the “Health supervision for children with achondroplasia” (HSCA) guidelinesCitation3 and revised by Trotter et alCitation8 in 2005. These guidelines provide recommendations for examination and anticipatory management by multidisciplinary teams across the lifespan, with the aim of reducing and promptly treating complications. While it is likely that appropriate and coordinated management in childhood could reduce or minimize medical complications for adults with achondroplasia, there remain considerable gaps in knowledge regarding medical and social experiences of adults with forms of skeletal dysplasia, including achondroplasia.Citation13,Citation14
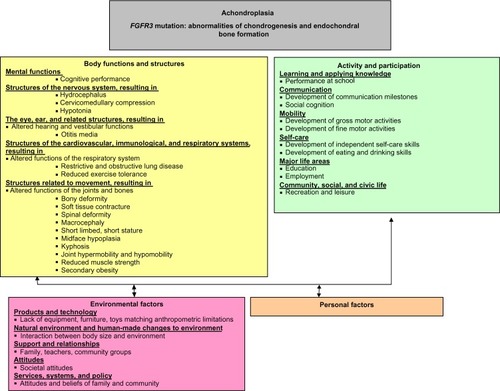
Expression of the defective FGFR3 gene in achondroplasia results in impairments of multiple body structures and functions. These impairments impact, both singularly and in combination, upon later development and performance. The complexity of this presentation, whereby individual impairments may impact upon multiple activity and participation areas, requires consideration under a broad framework to gain a thorough understanding of the complications experienced by individuals with achondroplasia. The International Classification of Functioning, Disability, and Health (ICF) published by the World Health Organization (WHO),Citation15 is currently considered the international gold standard for describing and measuring functioning, disability, and health. HagaCitation16 considered this framework when he developed the initial disablement model of achondroplasia. It is clear in HagaCitation16 that considering the interplay of individual factors across the ICF framework is beneficial for clinical reasoning, guidance of assessment, and in discussing prognostic factors with families. We propose an expanded model () that provides more detail regarding the dynamic linkages between body structures and functions, and related activity capacity/limitations and participation performance/restrictions. This expanded model will be used as the framework for the assessment and interpretation of the literature reported upon in this review.
Figure 1 ICF model of achondroplasia.
Musculoskeletal impairments and complications
As seen in , there are a number of changes related to body structures and functions in individuals with achondroplasia, including the musculoskeletal, neurological, cardiorespiratory, and ENT systems that impact upon overall participation. These will be discussed in more detail in each of the following sections. The head of the infant with achondroplasia is larger than in other infants,Citation1 potentially due to either a communicating hydrocephalus and/or dilated ventricles, which may be related to intracranial venous hypertension.Citation17 Close monitoring of head circumference (HC) using achondroplasia-specific growth charts, and periodic head ultrasound in the first year of life is essential, so that children who demonstrate a rapid increase in head size, or symptoms of increased pressure, such as irritability or a bulging fontanelle, can be referred to a pediatric neurologist or neurosurgeon for examination and consideration of ventricular shunting.Citation8 Macrocephaly has also been implicated in the development of a fixed, thoracolumbar kyphosis, which has led to the recommendation of restricted early sitting in this population.Citation18–Citation23
Children with achondroplasia demonstrate rhizomelic limb shortening with disproportionate intra-limb segmental ratios.Citation24 Rhizomelia also alters the limb-to-trunk growth ratio. Disproportionate shortening of the upper limbs creates a situation where children are unable to reach the top of their head, the middle of their back, or the intergluteal region.Citation25 The disproportionate limb-to-trunk ratio is greater during infancy and fingertip contact in an overhead reach is generally established by around 6 years of age. Individuals with achondroplasia also typically demonstrate a mixed pattern of joint mobility, including both joint contracture and/or joint hypermobility at characteristic joints. Infants and children consistently demonstrate limited elbow and hip extension ranges.Citation26 Both children and adults with achondroplasia uniformly display hip flexion contractures that have been postulated to contribute to the well-recognized lumbosacral lordosis and may be a contributing factor to the back pain and muscle fatigue reported by individuals with achondroplasia.Citation27 Hypermobility is typically observed in the knees and fingers of children with achondroplasia.Citation1,Citation16 This disproportionate limb shortening, joint contracture, and joint hypermobility were identified as possible factors contributing to the delayed development of independent self-care skills such as dressing and toileting identified by Ireland et al.Citation28,Citation29 These authors recommended that review by a physiotherapist or occupational therapist prior to school commencement could allow for targeted environmental modifications and equipment prescription to increase independence across self-care and mobility for the school-aged child with achondroplasia.
Another musculoskeletal change noted in the older child and adult is tibial bowing, and/or genu varum.Citation1,Citation7,Citation8,Citation30 KopitsCitation25 noted that tibial bowing was observed by parents in 40% of children with achondroplasia as they began to stand, with a more rapid progression of the deformity occurring at 3–4 years and 6–7 years. Hunter et alCitation10 reported that while approximately 10% of children demonstrate marked tibial bowing by 5 years, progression of this deformity through childhood leads to over 40% of adults being affected. Tibial bowing has been associated with recurrent periods of leg pain and discomfort. Chronic knee pain and changes in bony alignment can contribute to delays in weight-bearing, an altered gait pattern, and the potential for adult onset osteoarthritis associated with uneven weight distribution across the knee and ankle joints.Citation1,Citation9,Citation31 For those individuals demonstrating pain, and/or an altered gait pattern, corrective surgery such as tibial osteotomies, fibula epiphysiodesis, or continuous distraction epiphysiodesis may be utilized.Citation30,Citation32,Citation33 Hunter et alCitation10 reported that 22% of individuals in their multicenter review had had osteotomies, most commonly between 12 and 20 years of age.
Thoracolumbar kyphosis is a major secondary musculoskeletal impairment thought to arise from the combined impact of other common primary musculoskeletal impairments, such as macrocephaly, hypotonia, and joint hypermobility. Flexible kyphotic curves have been reported in over 90% of infants with achondroplasia, although the majority of these curves spontaneously improve once ambulation commences. Progression to a fixed kyphotic deformity occurs in 15%–30% of adults.Citation19,Citation34,Citation35 Progressive disruption of the vertebral epiphyseal ring that begins during childhood, combined with decreased growth in the anterior vertebral sections can create a progressive thoracolumbar kyphosis in adolescents, which is further exacerbated by age-related degenerative changes in the facet joints during adulthood.Citation36 This curve is then thought to contribute to adult onset spinal stenosis.Citation19,Citation36,Citation37 The kyphosis is thought to be exacerbated by early sitting where the effects of trunk hypotonia, increased head weight, and increased ligamentous laxity combine with the effect of gravity to force the child into a slumped sitting position, which can contribute to permanent spinal damage by increasing the anterior wedging of the vertebra and subsequent narrowing of the spinal canal.Citation4,Citation25,Citation27,Citation35,Citation36,Citation38,Citation39 This knowledge has led to the recommendation that sitting be restricted until the infant with achondroplasia is able to independently achieve this transition. Furthermore, parents of infants with achondroplasia should avoid pieces of equipment that reinforce this characteristic kyphosis such as baby slings or umbrella strollers.Citation35 When a kyphotic deformity is identified after commencement of independent ambulation, management may include education about positioning for nonfixed deformities, bracing,Citation18,Citation39,Citation40 and/or operative correction, usually for progressive curves or anterior vertebral wedging associated with a fixed angular kyphosis.Citation36,Citation41 Pauli et alCitation35 developed an algorithm for the monitoring and treatment of kyphosis in children, which they proposed could eliminate the neurological risks of angular kyphosis. However, the management of spinal kyphosis in achondroplasia is not consistent and requires further investigation to determine the optimal type and timing of management strategies.
Obesity is common in individuals with achondroplasia and is recognized as contributing to common medical problems for this group, including obstructive sleep apnea, genu varus, spinal stenosis, and hyperlordosis.Citation42–Citation44 Several authors have also identified a higher rate of cardiovascular disease-related death in adults with achondroplasia when compared with adults of average stature.Citation11,Citation45 While obesity is the most commonly recognized weight issue associated with this population, Hoover-Fong et alCitation42 stressed the importance of screening for and recognizing early failure to gain weight in infants and young children with achondroplasia, particularly if the infant presents with a number of more serious medical complications, including restrictive lung disease and obstructive sleep apnea. Nutritional counseling (such as smaller meal portion sizes), should be implemented early to help reduce the later effects of obesity in adult life. The inclusion of appropriately selected forms of exercise is also necessary for maintenance of a healthy weight range and increased social inclusion. Current recommendations are that children with achondroplasia stay within one standard deviation of the average height–weight curve on the achondroplasia-specific height–weight charts.Citation3,Citation8,Citation9,Citation42–Citation44,Citation46 Appropriate weight for height is also thought to reduce back and knee pain and reduce the chance of knee joint injury.
Neurological impairments and complications
Cervical cord compression at the cervicomedullary junction is frequently observed radiographically in children with achondroplasia, but symptomatic cord compression is less common. Significant compression at the foramen magnum can lead to severe neurological complications, including sleep apnea, disordered respiration, myelopathy, hydrocephalus, and sudden infant death.Citation21,Citation47,Citation48 There continues to be debate on the optimal assessment and type and timing of intervention for this problem. Some groups advocate for routine investigation of cervicomedullary compression by magnetic resonance imaging (MRI) or computer tomography (CT) studies in the infant with achondroplasia.Citation8,Citation49 These groups believe that the decision to intervene should not be based on traditional signs of neurological compression such as hypotonia, poor head control, and feeding issues, since these are common in children with achondroplasia.Citation50 In contrast, other clinical groups postulate that problems related to cervicomedullary compression will resolve spontaneously during childhood without specific intervention as the foramen magnum grows relative to the size of the spinal cord.Citation1,Citation22 They recommend undertaking investigation and intervention only if clear clinical evidence is present. The role of sleep studies and MRI cerebrospinal fluid flow studies remains unclear in the overall assessment of whether a child with achondroplasia might require decompressive surgery.
A proportion of children with achondroplasia will go on to require cervicomedullary decompression (CMD). Review of the literature identifies that 6.7%–13.3% of infants and children required CMD within the first 2 years,Citation12,Citation51 rising to 6.8%–28% by 4 years.Citation10,Citation52 The varying rates of CMD are likely to be a result of the different assessment and management approaches outlined in the previous paragraph.
Although the optimal methods of screening for cervicomedullary compression continue to be debated, there is consensus that education regarding safe early positioning and handling is beneficial in reducing the risks associated with cervicomedullary compression within this cohort. Careful handling around the head and neck area in the young infant with achondroplasia and the avoidance of baby equipment such as umbrella strollers and carrying slings, which may allow sudden, uncontrolled head movements that could create sudden compression at the brainstem level, is now considered best clinical practice in this population group.Citation8
Hydrocephalus, observed as ventriculomegaly and excessive extra-axial fluid, is another common complication resulting from disproportionate growth between the endochondral bone and surrounding structures. Restriction at the craniocervical junction can lead to increased venous pressure and altered cerebrospinal fluid dynamics, creating an increase in total head size.Citation1 Frequent monitoring of the occipital-frontal circumference (OFC) is recommended during the first 12 months using specialized head circumference growth charts for children with achondroplasia.Citation51,Citation53 Referral to a neurosurgeon or neurologist is recommended if the OFC is above the 95th percentile and/or there has been a rapid change in head size on the achondroplasia-specific head circumference charts associated with symptoms of increased pressure, and/or there have been other clinical signs or symptoms of symptomatic hydrocephalus.Citation1,Citation8,Citation9
Hypotonia is frequently observed in the infant and young child with achondroplasia. The precise cause remains unclear. Yang et alCitation54 found histological changes in the spinal cord of two infants with achondroplasia, and suggested that hyperextension type injuries with spinal cord damage might occur during delivery. A second hypothesis is that impairments in the craniocervical junction anatomy, in particular the narrow foramen magnum, constrict long tracts of the spinal cord, resulting in impaired signaling.Citation21–Citation23 Reynolds et alCitation20 found no correlation between the severity of hypotonia in infants with achondroplasia and the size of the foramen magnum. They hypothesized that the altered FGFR3 gene, expressed in the brain and nerve cells, caused a primary “brain-based” hypotonia. This hypotonia is thought to be a contributing factor to the delays reported in gross motor development for this group.Citation28,Citation55,Citation56
Neurological symptoms associated with lumbar spinal stenosis are present in a significant proportion of children and adults with achondroplasia. A number of factors are thought to contribute to spinal stenosis, including reduced size of the spinal canal, disc protrusions, spondyloarthritic spurs, kyphotic wedging, excessive lumbar lordosis related to hip flexion contractures, and vertebral malalignment or instability.Citation27,Citation37,Citation57,Citation58 Early reports of neurological symptoms associated with spinal stenosis suggested that this was predominantly an adult onset condition.Citation58 However, Hunter et alCitation10 noted that while issues related to spinal stenosis increased with age (with approximately 80% of individuals having clinical signs and symptoms by 60 years), nearly 10% of children had neurological signs, including claudication and hyperreflexia, by 10 years of age. They highlighted that these symptoms can lead to significant limitations in physical functioning and quality of life for these individuals. As early as 1978, Siebens et alCitation27 stressed the importance of reducing spinal canal disproportion through restriction of premature sitting, hip stretching whilst stabilizing the lumbar spine, and general education. As stated earlier, early best practice recommendations for this population now include caregiver education regarding avoidance of sitting to minimize potential complications and preserve function later in life. Surgery such as a decompressive laminectomy may be used to treat spinal canal stenosis in individuals with achondroplasia, although King et alCitation51 noted that evaluation of both spinal stenosis and instability is necessary prior to surgical intervention.
Cardiorespiratory impairments and complications
Respiratory signs and symptoms occur frequently in individuals with achondroplasia,Citation59 with a number of contributing mechanisms proposed: i) reduced chest circumference with altered mechanical function, ii) upper airway obstruction, and iii) cervicomedullary compression,Citation54,Citation59,Citation60 or iv) a significant combination of these factors. Upper airway obstruction is common in children with achondroplasia; with 10%–85% of patients requiring treatment for issues related to obstructive sleep apnea and chronic respiratory insufficiency.Citation1,Citation60,Citation61 In 1993, Waters et alCitation60 further stressed that airway obstruction should be considered a significant part of achondroplasia rather than an infrequent complication and that full polysomnography (overnight sleep studies) are required to clearly demonstrate and define the abnormalities. Tasker et alCitation62 observed a discrete group of children with persistent upper airway obstruction despite adenotonsillectomy, and reasoned that this was due to progressive hydrocephalus linked to foramen magnum stenosis. Management of respiratory and sleep disorders in this specific group required surgical management of the hydrocephalus combined with nocturnal positive airway pressure. More recently, Bagley et alCitation50 supported the finding that compression of the respiratory centers by musculoskeletal impairments at the craniocervical junction can reduce the central respiratory drive, and also that compression of the lower motor neurons innervating the respiratory muscles may result in weak respiratory efforts.Citation50
Tasker et alCitation62 identified a final group of children, who presented with progressive respiratory problems with chronic cardiorespiratory failure and a complex clinical presentation involving gastroesophageal reflux, pulmonary small airway pathology, and both obstructive and central sleep apneas. These children required several different forms of treatment, including foramen magnum decompression. Respiratory compromise can contribute to daytime respiratory problems, sleep disturbances and fatigue, and may influence development in this group. As such, the HSCA guidelines recommend regular examination of sleep apnea via polysomnography to identify potential central nervous system causes that may need immediate surgical management.Citation8
Exercise intolerance and exercise-induced fatigue is a common concern for children with achondroplasia. Takken et alCitation63 found that exercise capacity for children with achondroplasia was significantly reduced when compared with reference values for the general population and that children with achondroplasia demonstrated reduced muscle strength in almost all muscle groups. They hypothesized that these changes may have been caused by a decrease in muscle mass, reduced neuromuscular coordination, or altered biomechanics. Exercise-induced fatigue may influence a number of participation areas, including self-care performance and leisure pursuits.
ENT impairments and complications
Persistent or recurrent otitis media is common in children with achondroplasia and may cause hearing impairment.Citation8,Citation10,Citation64 Hunter et alCitation10 identified that over 25% of children reported chronic recurrent otitis media and Tunkel et alCitation65 observed that at least 25% also presented with hearing loss. Hunter et alCitation10 linked chronic recurrent otitis media to midface hypoplasia, shortened Eustachian tubes, small pharynx, and relative enlargement of the tonsils and adenoids. Other factors suggested include impaired nasal airflow and temporal bone abnormalities.Citation66 Consensus among clinicians is that recurrent otitis media in children with achondroplasia should be treated aggressively with adenotonsillectomy and insertion of ventilation tubes (grommets) to prevent conductive hearing loss.Citation1 A recent study by Ireland et alCitation67 found that insertion of grommets occurred frequently in children with achondroplasia <5 years of age, with over 50% of children undergoing this procedure over an 11-year period.
When poorly managed, the problem appears to persist into adulthood. McDonald et alCitation68 evaluated the peripheral auditory system in 18 adults with achondroplasia and found that 72% reported hearing loss at the time of assessment. This was supported by Tunkel et al,Citation65 who found that in a sample of 73 individuals with achondroplasia, 54% of the adults failed a hearing screening test. Both studies concluded that there is significant risk of long-term conductive hearing loss in this population and recommended that all patients with achondroplasia receive an early audiological evaluation to allow for the detection of hearing loss.
Hearing loss related to otitis media is thought to be a major contributor to the speech delays and articulation problems noted in approximately one in five children with achondroplasia.Citation10 This has significant impacts on communication development, and may influence learning and school performance.Citation28,Citation56 The high prevalence of otitis media and hearing loss in this population has led to the formal recommendation for routine early hearing tests and referral for speech and language review for infants and young children with achondroplasia as part of general surveillance.Citation3,Citation8,Citation9
Impact upon activity and participation
While much of the available literature evaluates the genetic basis of achondroplasia and the management of impairments in body structures and functions, there is comparatively less information regarding the influence that these factors have on activity and participation domains. As seen in , the complex interplay of the characteristic impairments of body structure can contribute directly and cyclically to activity limitations and participation restrictions for individuals with achondroplasia, including communication, mobility, and self-care.
The challenges posed by the combination of impairments in body structure and function can directly impact upon the major areas of participation for children, including mobility, self-care, education, and performance at school. Children with achondroplasia have a specific profile of developmental sequences, which differs from typical development, but is relatively consistent within the group. The developmental profile is influenced by both the musculoskeletal impairments characteristic of achondroplasia such as macrocephaly, short stature, and rhizomelic limb shortening, as well as positioning and handling restrictions necessary to reduce the risk of secondary injuries, eg, restricted sitting to avoid development of a fixed thoracolumbar kyphosis. Recognition that children with achondroplasia have a specific developmental profile has led to the development of milestone reference tables.Citation28,Citation55,Citation56,Citation69 Furthermore, a recent study by Ireland et alCitation29 noted a delay in the development of independence in functional self-care, mobility, and social cognition tasks for children with achondroplasia, with a need for caregiver assistance extending beyond 7 years. Delays in the development of gross motor, communication, and self-care skills may directly influence performance at school. Brinkmann et alCitation70 postulated that the altered body schema seen in short stature could lead to impaired social interaction with parents and other adults. This is supported by Ireland et alCitation29 who noted that many families reported an increased preference to remain in close proximity to their child during social situations because of the child’s short stature. The combination of short stature, physical mobility challenges, potential delays in language development and difficulty accessing appropriate equipment, may impact significantly on the child’s experiences within the educational setting, particularly during the formative school years. The knowledge of these challenges supports the need for children with achondroplasia to be reviewed by an occupational therapist and/or physiotherapist before school commencement to assist in school facility modification, equipment prescription, and problem solving. As there are currently no effective medical interventions to counteract the primary anatomical impairments seen in achondroplasia, improving overall participation will continue to be dependent on targeted assessment of limitations, and provision of environmental adaptations or equipment prescription.
Impact during adulthood
Thompson et alCitation14 reviewed the literature and research evidence on medical, health, and social aspects of life for adults with skeletal dysplasia including achondroplasia, and found substantial gaps in knowledge regarding medical and social aspects, recommending further robust research in this area. The medical and social complications associated with achondroplasia may impact on performance in areas such as employment. Roizen et alCitation71 compared education and occupation for 20 adults with achondroplasia with their same-sex siblings and found differences in occupation level despite comparable years of formal education for women, suggesting that other factors may be important. While Hunter et alCitation10 noted a trend towards the earlier diagnosis of achondroplasia, they went on to observe that a significant number of adults develop major physical limitations and pain, which impacts on their quality of life. It is possible that the onset of age-related medical issues (eg, spinal stenosis and leg pain), is exacerbated by physical access challenges related to short stature (eg, stairs) and is a contributing factor to differences in employment level. Further research is required to identify barriers to activity interactions for this population group, including more emphasis on those environmental factors that hinder or support participation performance.
New treatment options for achondroplasia
Recently, there have been large strides taken in terms of finding a medical (drug) treatment to alleviate some of the medical complications observed in achondroplasia. One medication that is currently undergoing early Phase II clinical trials is C-natriuretic peptide (CNP), which antagonizes the downstream effects of the aberrant FGFR3 signal, and has been shown to normalize bone growth in mouse models of achondroplasia.Citation72 In addition to this, other medications and antibodies are also being developed that may also aid in increasing bone growth and decreasing complications in this condition.
Conclusion
Children and adults with achondroplasia are impacted by a variety of medical issues created by the unique complexities associated with a form of disproportionate short stature. The pictorial presentation of achondroplasia based on the ICF that is presented in this paper highlights the need for ongoing commitment to coordinated multidisciplinary care to ensure that families receive timely service provision from medical subspecialists and therapists skilled in the management of this population. Further research on the changes in medical issues presenting across the lifespan for individuals with achondroplasia is needed to further drive health- and community-based services needs and assist with directing appropriate and timely service provision.
Disclosure
The authors report no conflicts of interest in this work. The authors alone are responsible for the content and writing of this paper.
References
- HortonWAHallJGHechtJTAchondroplasiaLancet2007370958216217217630040
- BaujatGLegeai-MalletLFinidoriGCormier-DaireVLe MerrerMAchondroplasiaBest Pract Res Clin Rheumatol200822131818328977
- American Academy of Pediatrics Committee on GeneticsHealth supervision for children with achondroplasiaPediatrics19959534434517862491
- ScottCIJrAchondroplastic and hypochondroplastic dwarfismClin Orthop Relat Res197611418301261109
- WeinsteinSLBuckwalterJATurek’s Orthopaedics: Principles and Their Application5th edPhiladelphia, PAJB Lippincott & Co1994
- WallerDKCorreaAVoTMThe population-based prevalence of achondroplasia and thanatophoric dysplasia in selected regions of the USAm J Med Genet A2008146A182385238918698630
- CarterEMDavisJGRaggioCLAdvances in understanding etiology of achondroplasia and review of managementCurr Opin Pediatr2007191323717224659
- TrotterTLHallJGAmerican Academy of Pediatrics Committee on GeneticsHealth supervision for children with achondroplasiaPediatrics2005116377178316140722
- WrightMJIrvingMDClinical management of achondroplasiaArch Dis Child201297212913421460402
- HunterAGBankierARogersJGSillenceDScottCIJrMedical complications of achondroplasia: a multicentre patient reviewJ Med Genet19983597057129733026
- HechtJTFrancomanoCAHortonWAAnnegersJFMortality in achondroplasiaAm J Hum Genet19874134544643631079
- PauliRMHortonVKGlinskiLPReiserCAProspective assessment of risks for cervicomedullary-junction compression in infants with achondroplasiaAm J Hum Genet19955637327447887429
- SavarirayanRRimoinDLThe skeletal dysplasiasBest Pract Res Clin Endocrinol Metab200216354756012464233
- ThompsonSShakespeareTWrightMJMedical and social aspects of the life course for adults with a skeletal dysplasia: a review of current knowledgeDisabil Rehabil200830111217852222
- World Health OrganizationInternational Classification of Functioning, Disability and Health: Children and Youth VersionGeneva, SwitzerlandWorld Health Organization Press2007
- HagaNManagement of disabilities associated with achondroplasiaJ Orthop Sci20049110310714767713
- SteinbokPHallJFlodmarkOHydrocephalus in achondroplasia: the possible role of intracranial venous hypertensionJ Neurosurg198971142482786928
- BorkhuuBNagarajuDKChanGHolmesLJrMackenzieWGFactors related to progression of thoracolumbar kyphosis in children with achondroplasia: a retrospective cohort study of forty-eight children treated in a comprehensive orthopaedic centerSpine (Phila Pa 1976)200934161699170519770611
- KopitsSEThoracolumbar kyphosis and lumbosacral hyperlordosis in achondroplastic childrenBasic Life Sci1988482412553240259
- ReynoldsKKModaffPPauliRMAbsence of correlation between infantile hypotonia and foramen magnum size in achondroplasiaAm J Med Genet20011011404511343336
- RimoinDLCervicomedullary junction compression in infants with achondroplasia: when to perform neurosurgical decompressionAm J Hum Genet19955648248277717392
- WassmanERJrRimoinDLCervicomedullary compression with achondroplasiaJ Pediatr198811324113397808
- YamadaHNakamuraSTajimaMKageyamaNNeurological manifestations of pediatric achondroplasiaJ Neurosurg198154149577463120
- NehmeAMRiseboroughEJTredwellSJSkeletal growth and development of the achondroplastic dwarfClin Orthop Relat Res19761168231277655
- KopitsSEOrthopedic aspects of achondroplasia in childrenBasic Life Sci1988481891973240253
- KitohHKitakojiTKuritaKKatohMTakamineYDeformities of the elbow in achondroplasiaJ Bone Joint Surg Br200284568068312188484
- SiebensAAHungerfordDSKirbyNACurves of the achondroplastic spine: a new hypothesisJohns Hopkins Med J19781426205210149212
- IrelandPJDonagheySMcGillJDevelopment in children with achondroplasia: a prospective clinical cohort studyDev Med Child Neurol201254653253722409389
- IrelandPJMcGillJZanklAFunctional performance in young Australian children with achondroplasiaDev Med Child Neurol2011531094495021838822
- StanleyGMcLoughlinSBealsRKObservations on the cause of bowlegs in achondroplasiaJ Pediatr Orthop200222111211611744865
- LeeSTSongHRMahajanRMakwanaVSuhSWLeeSHDevelopment of genu varum in achondroplasia: relation to fibular overgrowthJ Bone Joint Surg Br2007891576117259417
- BealsRKStanleyGSurgical correction of bowlegs in achondroplasiaJ Pediatr Orthop B200514424524915931026
- KaissiAAFarrSGangerRHofstaetterJGKlaushoferKGrillFTreatment of varus deformities of the lower limbs in patients with achondroplasia and hypochondroplasiaOpen Orthop J20137333923459260
- LonsteinJETreatment of kyphosis and lumbar stenosis in achondroplasiaBasic Life Sci1988482832923240263
- PauliRMBreedAHortonVKGlinskiLPReiserCAPrevention of fixed, angular kyphosis in achondroplasiaJ Pediatr Orthop19971767267339591973
- MisraSNMorganHWThoracolumbar spinal deformity in achondroplasiaNeurosurg Focus2003141e415766221
- BaileyJA2ndOrthopaedic aspects of achondroplasiaJ Bone Joint Surg Am1970527128513015472902
- HallJGThe natural history of achondroplasiaBasic Life Sci198848393071358
- SiebensAAHungerfordDSKirbyNAAchondroplasia: effectiveness of an orthosis in reducing deformity of the spineArch Phys Med Rehabil19876863843883592956
- HallJGKyphosis in achondroplasia: probably preventableJ Pediatr198811211661673335958
- SiebensAAKirbyNHungerfordDOrthotic correction of sitting abnormality in achondroplastic childrenBasic Life Sci1988483133173240267
- Hoover-FongJEMcGreadyJSchulzeKJBarnesHScottCIWeight for age charts for children with achondroplasiaAm J Med Genet A2007143A192227223517764078
- Hoover-FongJESchulzeKJMcGreadyJBarnesHScottCIAge-appropriate body mass index in children with achondroplasia: interpretation in relation to indexes of heightAm J Clin Nutr200888236437118689372
- HunterAGHechtJTScottCIJrStandard weight for height curves in achondroplasiaAm J Med Genet19966232552618882783
- WynnJKingTMGambelloMJWallerDKHechtJTMortality in achondroplasia study: a 42-year follow-upAm J Med Genet A2007143A212502251117879967
- HechtJTHoodOJSchwartzRJHennesseyJCBernhardtBAHortonWAObesity in achondroplasiaAm J Med Genet19883135976023228140
- PauliRMScottCIWassmanERJrApnea and sudden unexpected death in infants with achondroplasiaJ Pediatr198410433423486707788
- WangHRosenbaumAEReidCSZinreichSJPyeritzREPediatric patients with achondroplasia: CT evaluation of the craniocervical junctionRadiology198716425155193602395
- KeiperGLJrKochBCroneKRAchondroplasia and cervicomedullary compression: prospective evaluation and surgical treatmentPediatr Neurosurg1999312788310592476
- BagleyCAPindrikJABooklandMJCamara-QuintanaJQCarsonBSCervicomedullary decompression for foramen magnum stenosis in achondroplasiaJ Neurosurg2006104Suppl 316617216572633
- KingJAVachhrajaniSDrakeJMRutkaJTNeurosurgical implications of achondroplasiaJ Neurosurg Pediatr20094429730619795959
- HoNCGuarnieriMBrantLJLiving with achondroplasia: quality of life evaluation following cervico-medullary decompressionAm J Med Genet A2004131216316715487008
- HortonWARotterJIRimoinDLScottCIHallJGStandard growth curves for achondroplasiaJ Pediatr1978933435438690757
- YangSSCorbettDPBroughAJHeidelbergerKPBernsteinJUpper cervical myelopathy in achondroplasiaAm J Clin Pathol19776816872868806
- FowlerESGlinskiLPReiserCAHortonVKPauliRMBiophysical bases for delayed and aberrant motor development in young children with achondroplasiaJ Dev Behav Pediatr19971831431509213228
- IrelandPJJohnsonSDonagheySDevelopmental milestones in infants and young Australasian children with achondroplasiaJ Dev Behav Pediatr2010311414720081435
- LutterLDLangerLONeurological symptoms in achondroplastic dwarfs – surgical treatmentJ Bone Joint Surg Am19775918792833182
- LutterLDLongsteinJEWinterRBLangerLOAnatomy of the achondroplastic lumbar canalClin Orthop Relat Res1977126139142598103
- StokesDCPhillipsJALeonardCORespiratory complications of achondroplasiaJ Pediatr198310245345416834188
- WatersKAEverettFSillenceDFaganESullivanCEBreathing abnormalities in sleep in achondroplasiaArch Dis Child19936921911968215519
- AfsharpaimanSSillenceDOSheikhvatanMAultJEWatersKRespiratory events and obstructive sleep apnea in children with achondroplasia: investigation and treatment outcomesSleep Breath201115475576121225355
- TaskerRCDundasILavertyAFletcherMLaneRStocksJDistinct patterns of respiratory difficulty in young children with achondroplasia: a clinical, sleep, and lung function studyArch Dis Child1998792991089797588
- TakkenTvan BergenMWSakkersRJHeldersPJEngelbertRHCardiopulmonary exercise capacity, muscle strength, and physical activity in children and adolescents with achondroplasiaJ Pediatr20071501263017188608
- CollinsWOChoiSSOtolaryngologic manifestations of achondroplasiaArch Otolaryngol Head Neck Surg2007133323724417372080
- TunkelDKerbavazRSmithBAladeYHoover-FongJHearing loss in skeletal dysplasia patients10th Biennial Meeting of the International Skeletal Dysplasia SocietyJune 23–26, 2011Palm Cove, Australia
- GordonNThe neurological complications of achondroplasiaBrain Dev20002213710761826
- IrelandPJJohnsonSDonagheySMedical management of children with achondroplasia: evaluation of an Australasian cohort aged 0–5 yearsJ Paediatr Child Health201248544344922112170
- McDonaldJMSeippWSGordonEMHeroyJAudiologic findings in achondroplasiaBasic Life Sci1988481431473240243
- TodorovABScottCIJrWarrenAELeeperJDDevelopmental screening tests in achondroplastic childrenAm J Med Genet19819119237246617
- BrinkmannGSchlittHZorowkaPSprangerJCognitive skills in achondroplasiaAm J Med Genet19934758008048267016
- RoizenNEkwoEGosselinkCComparison of education and occupation of adults with achondroplasia with same-sex sibsAm J Med Genet19903522572602309765
- LorgetFKaciNPengJEvaluation of the therapeutic potential of a CNP analog in a Fgfr3 mouse model recapitulating achondroplasiaAm J Hum Genet20129161108111423200862