Abstract
Hereditary angioedema (HAE) is a potentially fatal genetic disorder typified by a deficiency (type I) or dysfunction (type II) of the C1-inhibitor (C1-INH) and characterized by swelling of the extremities, face, trunk, abdominal viscera, and upper airway. Type III is normal estrogen-sensitive C1-INH HAE. Bradykinin, the main mediator of HAE, binds to endothelial B2 receptors, increasing vascular permeability and resulting in edema. HAE management includes short- and long-term prophylaxis. For treating acute episodes, C1-INH concentrate is recommended with regression of symptoms achieved in 30–90 min. Infusions of 500–1000 U have been used in Europe for years. Two plasma-derived C1-INH concentrates have been licensed recently in the United States: Berinert® for treating acute attacks and Cinryze® for prophylaxis in adolescent/adult patients. A recombinant C1-INH that is being considered for approval (conestat alfa) exhibited significant superiority versus placebo. Ecallantide (Kalbitor®) is a selective kallikrein inhibitor recently licensed in the United States for treating acute attacks in patients aged >16 years. It is administered in three 10-mg subcutaneous injections with the risk of anaphylactic reactions. Icatibant (Firazyr®) is a bradykinin B2 receptor competitor. It is administered subcutaneously as a 30-mg injection and approved in Europe but not in the United States.
Introduction
Angioedema is a localized, transient swelling of the deeper layers of the skin or mucous membranes of the upper respiratory or gastrointestinal tract. The swelling has a predilection for the areas of more loosely attached skin (lips, face, tongue, genitals, extremities, or larynx). A burning sensation or pain may be present, but pruritus or erythema is absent. This is in contrast to urticaria with angioedema, which is characterized by itching and wheals.Citation1
There are two distinct pathophysiological pathways leading to angioedema: histamine-mediated angioedema and kinin-mediated angioedema ().Citation2
Table 1 Classification of angioedema
In histamine-mediated angioedema, degranulation of mast cells can be by cross-linking of immunoglobulin E (IgE) bound by autoantibodies against the mast cell IgE receptor or by direct response to different agents such as opiates or contrast medium. Histamine released by mast cells increases local blood flow and endothelium permeability. Clinically, it produces urticaria, angioedema, and, in severe cases, anaphylaxis. However, in kinin-mediated angioedema, bradykinin binds to receptors on the vascular endothelium and increases vascular permeability and leakage of plasma into the interstitial space. This angioedema is not associated with urticaria. Angiotensin-converting enzyme (ACE) inhibitor-induced angioedema and hereditary angioedema (HAE) occur as a result of kinin effects.Citation1
Hereditary angioedema
Epidemiology and types
HAE is a potentially fatal genetic disorder typified by a deficiency or dysfunction of the plasma protein C1-INH, and characterized clinically by swelling of the extremities, face, trunk, abdominal viscera, and upper airway.Citation3 HAE has an incidence of <1/50,000 persons.
The disease is inherited in an autosomal dominant manner. About 85% of patients have low levels of C1-INH (type I) and in 15% of patients the protein is nonfunctional (type II).
HAE is a result of C1-inhibitor (C1-INH) deficiency. This serine protease inhibitor plays an important role in the regulation of the complement, contact, and fibrinolytic systems. Those affected are heterozygous for C1-INH mutations, which result in low levels of circulating C1-INH (type I HAE) or normal levels of a nonfunctional C1-INH (type II HAE). Both types are indistinguishable clinically.Citation4
HAE type III is an autosomal dominant inherited angioedema without abnormalities of complement or C1-INH.Citation5 It is estrogen-sensitive, often appearing during pregnancy or estrogen administration, and it is usually symptomatic only in women.
Although patients with acquired angioedema (AAE) have symptoms similar to HAE, there is a lack of a family history. It starts commonly in middle age and is associated with lymphoproliferative disease, autoimmune disease, vasculitis, or infection. C1-INH deficiency occurs as a result of increased consumption by paraprotein or immune complexes (type I AAE), or direct cleavage by C1-INH autoantibodies (type II AAE).Citation3
Immunology and genetics
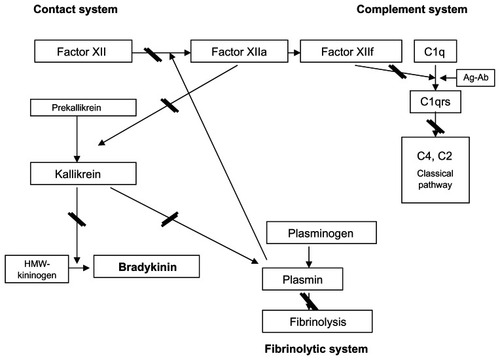
C1-INH is mainly produced in the liver. It is the main regulator of the early activation steps of the classical complement pathway and the plasma pathways for bradykinin formation. In the absence of C1-INH, the classical complement pathway is excessively activated. Immune complexes trigger the activation of the first component C1q to C1qrs. C1 esterase then acts with C4 and C2 to form the complex C4b2a. Formation of this new complex in association with a C3 activation leads to the production of anaphylactic, chemotactic, and vasoactive peptides.
Although activation of the complement system in HAE may contribute to the initiation, duration, and severity of attacks by consuming C1-INH, the primary mediators of vascular permeability leading to angioedema are products of the contact system or kallikrein-kinin pathway.Citation6 A summary of the C1 regulation points in these pathways is shown in . C1-INH deficiency results in an increase in kallikrein, which, in turn, increases bradykinin production. Inhibitory effects of C1 on factor XIIa and plasmin have also been described. Estrogen therapy may raise blood levels of factor XII.Citation7
Figure 1 C1-INH regulates the contact and classical complement pathways and the fibrinolytic system by inhibition at a variety of points marked with arrows (
More than 180 different mutations in the C1-INH gene (SERPING1/C1-INH) on chromosome band 11q12–q13.1 have been described, 25% being spontaneous mutations. There is no correlation between symptoms and type of genetic defect.
Mutations in the C1-INH gene may be seen along the entire protein sequence. Type I mutations are those in which the gene product is not translated into a viable protein product. These mutations are likely to be insertions, deletions, transversions, formation of stop codons, or altered carbohydrate linkages needed for secretion.Citation8,Citation9 Type II disease is typified by mutations that involve single amino acid substitutions, which are more likely to lead to synthesis of a dysfunctional protein. Genetic tests are not currently indicated routinely; however, under certain circumstances a genetic test may be of use.Citation10
Patients with HAE have a higher incidence of autoimmune diseases, although they are usually mild.Citation11
Laboratory tests
Serum C4 level is a good screening test for HAE as it is low in untreated HAE. If the C4 level is low, then C1-INH level and function should be assessed. If HAE is highly suspected in spite of normal C4 levels, C1-INH function should be measured.Citation4 The diagnosis of type I HAE is by demonstrating low amounts of C1-INH.Citation12 An absence of function suggests a type II defect. In , the laboratory findings in different types of angioedema are detailed. Interpretation in very young children is difficult due to paucity of data regarding reference ranges in children.
Table 2 Laboratory results for HAE
Clinical characteristics
Angioedema attack begins with trauma, infection, febrile illness, and other unknown factors that lead to activation of the complement, contact, and/or fibrinolytic systems. This leads to consumption of C1-INH, which results in complete deregulation of the complement and contact systems with decreasing levels of C4 and C2, and the generation of bradykinin. Bradykinin is the main mediator of HAE.Citation13 Bradykinin binds to B2 bradykinin receptors on the endothelial cells and causes an increase in vascular permeability, which results in edema.
Most HAE episodes only involve the skin and subcutaneous tissue. However, the upper respiratory tract and the majority of visceral organs may also be affected.Citation14,Citation15
Cutaneous and subcutaneous lesions
Clinically, skin lesions of HAE consist of recurrent episodes of subcutaneous edema. The lesions are typically nonpruritic and nonpitting and usually involve the arms, legs, hands, feet, trunk, face, tongue, or larynx.Citation15,Citation16 Upper extremities are involved more often than the lower ones.Citation15 Facial areas more frequently involved are the lips, eyelids, and tongue.Citation17,Citation18 Although a few patients develop symptoms during their first decade, the disease typically manifests during the second decade of life,Citation14,Citation15 with the episodes worsening around puberty and persisting through life.Citation15,Citation16 Most attacks are triggered by trauma, medical procedures, emotional stress, menstruation, infections, or the use of medications such as ACE inhibitors or oral contraceptives.Citation18–Citation21 Dental interventions are of particular risk because they may induce angioedema of oral mucosa that expands to the upper airway with the risk of asphyxia.
In most cases, the episodes are preceded by a tingling, burning, or pain sensation in the involved area.Citation22 Over the first 24 h, the swelling worsens slowly and then gradually subsides. Typical attacks of angioedema persist for 2–5 days before resolving spontaneously.Citation14,Citation16 This is one of the classical signs that distinguish HAE from allergic angioedema, which resolves in <24 h. Another feature that aids in differential diagnosis is that the swelling of HAE is painful while allergic angioedema is usually pruriginous and may be accompanied by the typical erythematous-edematous lesions of urticaria. However, before and during acute attacks of HAE, patients may develop macular cutaneous lesions, usually described as slight redness of the cutaneous region, lines of redness, or red rings.Citation22 It may be distinguished from urticaria because the dermal lesions associated with HAE are erythematous macules but not warm and pruritic erythema-edematous plaques.Citation14,Citation22 In summary, the diagnosis should be suspected in any patient who presents with recurrent angioedema lasting for more than 24 h in the absence of associated urticaria. Although most patients report a family history of angioedema, up to 25% have a de novo C1-INH mutation.Citation23
Abdominal attacks
Abdominal episodes occur in most patients.Citation15 They are caused by edema of the intestinal wall, resulting in varying degrees of intestinal obstruction. The resulting symptoms are painful abdominal cramps that can be severe, with nausea and vomiting. Diarrhea can also occur, particularly as the acute episode resolves.Citation14 At clinical exploration, the abdomen is tender to palpation, usually without guarding. Gastrointestinal episodes may, however, be unaccompanied by cutaneous lesions, and because rebound tenderness may be present, the symptoms can be mistaken for an acute abdomen. Unnecessary abdominal surgery has been performed.Citation14,Citation16
Fortunately, fever and leukocytosis are unusual in episodes of HAE. For this reason, their presence during an attack in a patient diagnosed with HAE suggests that another process, such as infection or intra-abdominal disorder, may be the cause of the acute exacerbation.Citation14 The abdominal attacks are less persistent than cutaneous lesions and usually subside within 12–24 h.Citation14 In women, discrete abdominal episodes may also be confounded with dysmenorrhoea, mostly in those patients in which the attacks are triggered by menstruation.
Severe complications of HAE
The most severe complication of HAE is laryngeal edema. It is a frequent complication because more than half of patients have had at least one episode of laryngeal edema during their lifetime.Citation15 Moreover, before the development of effective treatments that are currently available, <30% of patients died of asphyxiation.Citation5,Citation18 Tracheostomy can be lifesaving because the edema involving the upper airway typically occurs at or above the larynx. Asphyxiation has been documented in individuals as young as 4 weeks and as old as 78 years.Citation5 Another potentially life-threatening complication of HAE is hypovolemic shock caused by a shift of fluids into the interstitium or peritoneal cavity during abdominal attacks.Citation14,Citation18,Citation24 Cerebral edema caused by the acute HAE episode may produce migraine-like symptoms, transient ischemic attack,Citation25,Citation26 seizures, and hemiparesia.Citation18,Citation27,Citation28
Treatment of HAE
First, patients with HAE must avoid the previously mentioned factors that may precipitate attacks. The aims in HAE acute attacks management consist of aborting an episode when a patient presents signs of an attack (on-demand treatment), avoiding an attack before triggers act (short-term prophylaxis), and, lastly, in a long-term manner applying treatment periodically to prevent symptoms (long-term prophylaxis) and even at the onset of the early signs of an attack (individual replacement therapy). Antihistamines, corticosteroids, and epinephrine are ineffective in the treatment of HAE.Citation14
Long-term prophylaxis
Long-term prophylaxis is considered in patients who have more than one acute attack monthly.Citation12,Citation29,Citation30 However, some authors consider that the risk of upper airway edema is high regardless of which organ system was involved in previous attacks or the number of previous episodes, and that long-term prophylaxis should also be considered in any patient with a previous history of acute lesions affecting any organ system.Citation5,Citation14
There are two types of drugs that significantly reduce the frequency of episodes of HAE. These include attenuated androgens (the 17α-alkylated androgens danazol and stanozolol) and antifibrinolytic agents (tranexamic acid and ɛ-aminocaproic acid). Although the two groups of agents have not been compared in randomized studies, attenuated androgens appear to be more effective.Citation12,Citation31–Citation34
The usual starting dose of danazol is 200–600 mg daily.Citation12,Citation16,Citation35 As soon as symptomatic control is achieved, the dosage is reduced to the minimum dose that suppresses the attacks. Doses as low as 200 mg every 2 or 3 days can be successful.Citation36 Stanozolol is administered at a dosage of 4 mg 3 times daily. As soon as symptomatic control is achieved, the dose is reduced to 1–2 mg daily. In some patients, alternate-day administration of stanozolol is also effective.Citation14 Attenuated androgens stimulate the production of C1-INH and increase serum levels of C1-INH, C4, and C2.Citation32,Citation37 However, the dose of attenuated androgens is best assessed based on the clinical response rather than in laboratory tests, as improvement may occur even when the C1-INH levels remain low.Citation35
Side effects include increased seborrhea, acne, hair growth, deepening of the voice, decreased breast size, menstrual irregularities, decreased libido, weight gain, lipid abnormalities, and hypertension.Citation12,Citation14,Citation30 Major adverse effects are hepatic necrosis, cholestasis, and hepatocellular adenomas.Citation14,Citation30,Citation38–Citation41 Several cases of danazol-associated hepatocellular carcinoma have also been reported.Citation42–Citation45 Stanozolol therapy seems to have fewer adverse effects than danazol therapy.Citation14
In patients taking attenuated androgens, liver enzyme levels and serum lipid profiles should be monitored every 6–12 months. Because of the risk of liver adenoma or carcinoma, periodic abdominal ultrasonography is recommended.Citation12,Citation38,Citation45 Attenuated androgens are contraindicated in pregnancy, lactation, prostate cancer, and childhood.Citation12,Citation14
Antifibrinolytic agents are considered less effective than attenuated androgens.Citation14 However, because of the potential side effects of attenuated androgens (masculinization of the fetus, premature puberty, and premature closure of epiphyseal plates), antifibrinolytic drugs are considered as the first choice in pregnant women and children who require long-term prophylaxis.Citation46,Citation47 The usual dosage is 1 g twice daily (0.25 g twice daily to 1.5 g thrice daily) for tranexamic acid and 2 g thrice daily (1 g twice daily to 4 g thrice daily) for ɛ-aminocaproic acid.Citation12,Citation16 Tranexamic acid is more effective than ɛ-aminocaproic acid.Citation12 Muscle cramps, myalgia, and increased serum creatine phosphokinase or aldolase levels secondary to rhabdomyolysis are potential side effects.Citation14,Citation16,Citation36 Another possible adverse effect of antifibrinolytic agents is a potential risk of thrombosis.Citation16 Liver and renal function and creatine phosphokinase levels should be monitored every 6 months, and eye pressure should be checked annually for the risk of glaucoma.Citation12
Short-term prophylaxis
When a patient with HAE is expected to be exposed to a situation likely to trigger an attack, such as substantial dental intervention or surgical procedures, short-term prophylactic treatment is indicated. There are several options, including the administration of C1-INH 1 h before the provoking event (500–1500 U), 2 units of fresh-frozen plasma (FFP) administered 1–12 h before, or danazol at a dose of 200 mg orally 3 times a day for the 10 days prior to the provoking factor and 2–5 days after.Citation12,Citation48,Citation49 For minor manipulation such as mild dental work, danazol is the most widely used. For intubation or major procedures, C1-INH concentrate is the first option.Citation12
Short-term prophylaxis should also be considered before administration of intravenous radiologic contrast, streptokinase, or tissue plasminogen activators, because previous studies have suggested that these agents may decrease levels of CI-INH in these patients.Citation14,Citation50–Citation52
Management of acute attacks
As has been discussed before, attacks in HAE patients produce swelling involving subcutaneous tissues in different locations. As upper respiratory swelling can be life-threatening and attacks can manifest in 20 min, an efficient treatment is needed.Citation18
Under the pathophysiological point of view, there are two approaches to treat acute angioedema, including emergent therapies: to replace C1-INH and to inhibit bradykinin generation either by blocking the enzyme kallikrein or preventing the interaction of bradykinin with its receptor.Citation53
Replacement therapy: FFP and C1-INH concentrates (viral transmission concerns)
C1-INH inactivates several different proteases such as factor XII and kallikrein in the contact system. Indeed, the lack of kallikrein-inhibitory activity in HAE patients was observed by Landerman and Donaldson in the early 1960s.Citation54,Citation55
With the fundamental observation that HAE patients were deficient in the plasma protein C1-INH, it seemed obvious to treat them by replacing the missing plasma protein. For such reason, FFP has been used in therapy of acute attacks in HAE and AAE patients. Jaffe et al reported the use of FFP 2 U (200 mL) 1–12 h before the triggering agent.Citation48 Because the dose of 10 mL/kg of solvent or detergent-treated FFP has been usually used for coagulopathies, it was thought that it might work in C1-INH deficiency.Citation49 Moreover, no other effective way of treatment was available in many countries, including the United States and Australia.Citation56,Citation57
Even though FFP is proven to be effective in short-term prophylaxis, its use in acute attacks may be dangerous, worsening swelling because FFP contains substrates other than C1-INH. Bradykinin, the main responsible agent for swelling, is released by cleavage of the high-molecular-weight kininogen, which is present in normal plasma. With the infusion of FFP, high-molecular-weight kininogen is provided along with C1-INH, potentially worsening the swelling. On the other hand, concerns regarding viral safety questions discourage their use when safer products are available.Citation58,Citation59
The lack of sufficient data to demonstrate FFP benefits prompted Prematta et al to perform a literature search from 1996, as well as a review of their own practice. The evidence found could not confirm the theory that FFP could exacerbate symptoms or precipitate an attack of HAE. On the contrary, it seemed safe and effective in surgical prophylaxis and treatment of acute attacks.Citation57
C1-INH is a 104-kDa protein, which inhibits complement components, contact, and fibrinolytic.Citation5 C1-INH concentrate is recommended as first-line therapy for the treatment of acute attacks of HAE and for short-term (and eventually long-term) prophylaxis in several consensus statements.Citation5,Citation7,Citation49
The C1-INH concentrate is a more advantageous alternative compared with FFP. Although it is derived from human plasma with risk of infectious disease, beginning in the 1970s, efforts started in Europe to manufacture a more purified preparation of missing protein.Citation60 The blood-borne contagious risk has been reduced by multiple viral inactivation and removal steps including cryoprecipitation, chromatography, and pasteurization; nanofiltration is added to a recently US Food and Drug Administration (FDA)-approved C1-INH concentrate.
Another advantage of C1-INH is the faster way to replace the missing inhibitor due to a high concentration of the manufactured product: 1 unit of C1-INH preparation is equal to the amount of C1-INH in 1 mL of normal human plasma, which is equivalent to 270 mg or 2.5 μM/L of plasma.Citation61 Finally, we can benefit from C1-INH concentrate because it can be kept at home by patients to be self-administered intravenously when needed, as has been done in some countries for years (after a rigorous training), or can be taken to the emergency room, avoiding unnecessary delays before treatment is started.Citation62–Citation64
Emphasizing viral safety, the use of human plasma-derived products is an ongoing concern of infectious transmission. More than 80% of patients treated with the partially purified C1-INH produced by Immuno Pharmaceuticals, Viena, in 1980 (brand name C1 Inactivator) were infected with hepatitis C virus (HCV), even though no patient was reported to be infected by human immunodeficiency virus (HIV). In 1986, pasteurization was introduced in the preparation of the product, but viral transmission could not be excluded, because one case of HCV was detected.Citation65 Immuno Pharmaceuticals was sold to Baxter Pharmaceuticals, which in 2003 discontinued manufacturing C1 Inactivator.Citation66
The plasma-derived C1-INH concentrate Berinert® P (CSL Behring, Marburg, Germany) has been used in Europe and Canada for more than 20 years, and a lot of postmarketing safety and tolerability experience is available. It was first licensed in Germany in 1985, and a similar nonpasteurized product had been previously approved also in Germany in 1979.Citation61 It is obtained from human plasma and is subjected to rigorous pathogen safety measures, such as donor selection, testing of each single donation with sensitive and specific nucleic acid testing/polymerase chain reaction assay for hepatitis A virus, hepatitis B virus, HCV, HIV1, and human parvovirus B19, and pasteurization. Afterward, the product is purified by precipitation and chromatography, sterile filtrated, and lyophilized without preservatives. Since 2004, a new Berinert® P formulation has been developed, and the product can be stored without refrigeration at room temperature below 25°C.Citation67 It is recommended to not shake it during the reconstitution process, as this will denature the protein. Administration should be via peripheral vein (usually over 10 min).
There have been no reports of viral transmission with the use of this plasma-derived product since its introduction in January 1985, and few adverse effects have been published. In fact, fewer than 30 events were reported from 1985 to 2003, of which only 10 were thought to be directly related to treatment by 100 million units dispensed. Associated adverse effects include anaphylactoid reactions (most probably related to too rapid or too low temperature administration), the formation of inhibitory antibodies, localized redness at the injection site, and general reactions such as fever, chills, and headaches.Citation61
De Serres et al in a Berinert® P efficacy and safety review quotes a number of studies, some of which are commented on below.Citation61 A series of 30 HAE patients under long-term prophylaxis receiving C1-INH concentrate twice or three times a week were checked in regard to viral transmission hepatitis A, B, C, G, and HIV, and no seroconversion was found.Citation68
Bork and Barnstedt published 193 laryngeal edema cases treated with Berinert® P, and viral transmission was not reported.Citation69
Agostoni and Cicardi, in a retrospective study on 235 HAE and AAE patients, reported 67 laryngeal and 15 abdominal attacks treated with infusions of 500–1500 U of different C1-INH concentrates, achieving regression of symptoms in 30–90 min, and found effects in only one case.Citation29
The C1-INH Berinert® P was finally approved in September 2009 by the FDA for the treatment of acute abdominal and facial angioedema attacks in adolescents and adults with HAE.Citation70
A nanofiltered C1-INH concentrate (Cinryze®) has been recently developed. Along with pasteurization, it is double-nanofiltered with the use of 15-nm filters, increasing safety by size exclusion, particularly regarding nonenveloped viruses and prions.
Pharmacokinetics of C1-INH concentrates
Martinez-Saguer et al investigated the pharmacokinetics of pasteurized human plasma-derived C1-INH concentrate (Berinert® P) in children and adults receiving on-demand treatment (in acute attacks) as well as in adults receiving individual replacement therapy (administered at the onset of the early signs of an attack) as a home therapy.
The mean time to achieve maximum plasma activity after administration was 0.5 h in adults receiving individual replacement therapy, 1 h in adults receiving on-demand therapy, and 0.6 h in children. Clearance was 1.1 and 1 mL/kg/h for children and adults, respectively. The volume of distribution at steady state was 50 and 56.7 mL/kg for children and adults, respectively. Although the mean doses applied were similar between groups, the reported mean half-lives of plasma C1-INH were 31.5 h in children, 33.3 h in adults receiving replacement therapy, and 47.8 h in adults under on-demand therapy. The difference in half-life of adults receiving on-demand treatment compared with adults receiving individual replacement therapy reached significance. The authors argue that patients with a high frequency of severe attacks (as were patients receiving individual replacement therapy) presented a higher turnover of plasmatic C1-INH concentrate, with increased catabolic rate and shorter half-life.Citation71 The investigation was during an attack-free interval over 72 h, whereas the Kunschak et al study (performed with a different plasma-derived concentrate) of patients having an acute attack over 24 h reported a similar mean half-life (37.9 h).Citation72
Besides multiple descriptions of the use of Berinert® P in surgical prophylaxis at 500–1000 U before the procedure, Lehmann et al reported a successful administration of 1000 U before and 500 U every 6 h in a patient receiving coronary artery bypass graft surgery.Citation73
Alvarez published the use of a different concentrate (C1-INH TIM3, Baxter Healthcare, Deerfield, IL, USA) in an HAE patient requiring coronary bypass surgery. The patient received 1000 U 1 h before surgery and 1000 U 1 h before extubation (7 h after operation), and the uncontrolled complement activation was avoided.Citation74
Martinez-Saguer et al reported an uneventful continuous infusion of Berinert® P during surgery in three cases, receiving 1000 U each, followed by 0.5–1 U/kg body weight.Citation75
In a recently completed study with Berinert® P, I.M.P.A.C.T.1, pharmacokinetic results in the treatment of acute attacks have been 32.7 h for half-life, 0.43 dL/kg for volume of distribution, and 0.92 mL/kg/h for clearance. Results were obtained from samples extracted after acute abdominal and facial attacks,Citation76 in contrast to the Martinez-Saguer et al investigation, with samples obtained during the attack-free intervals.Citation71
In studies done in a recombinant human C1-INH (rC1-INH) concentrate, the half-life was dose dependent, and at 100 U/kg body weight it was estimated to be 3 h. Although it is very similar to plasma-derived C1-INH, rC1-INH is heavily glycosylated, which affects the half-life of this agent while not affecting its functional activity.Citation77
Efficacy of C1-INH concentrates
In 1980, two pilot experiences with C1-INH concentrate (other than Berinert® P) in 13 and 8 HAE patients, respectively, were published with very good results.Citation78,Citation79 However, it was not until 16 years later when the first double-blind clinical trial came out. Meanwhile, multiple experiences with C1-INH concentrate were described by De Serres et al.Citation61
First double-blind study of plasma-derived C1-INH
In 1996, the first double-blind study of C1-INH (Immuno Pharmaceuticals, Vienna, Austria) purified from plasma (vapor heated) was reported, with patients with severe attacks receiving treatment every 3 days. The results showed a fast increase in blood C1-INH (mean 85% of normal values) and a slower increase in C4 levels after the infusion of concentrate. In placebo-treated patients, neither the level of circulating C1-INH nor the C4 level changed. The mean levels of C1-INH 24 h after the infusion were <70% of normal, which fell to 48% after 72 h.
The HAE symptoms decreased in the treatment group (60% less in the scores for extremities, larynx, abdomen, and genitourinary tract edema). In the study group, a clinical response was noted within 30 min after most infusions of C1-INH (75%), when compared with many hours after the infusions of placebo. In the treatment group, the larynx and abdomen swelling responded better than did the subcutaneous swelling of the extremities, as has been reported previously.Citation80
The product tested was prepared by Immuno Pharmaceuticals, which was later sold to Baxter Pharmaceuticals. A phase III trial of the Immuno C1-INH concentrate (Baxter Healthcare) was performed several years ago for acute HAE attacks. However, it failed to show any improvement in C1-INH-treated patients compared with placebo-treated subjects. This result was likely due to the experimental design, which involved a 1-h crossover between C1-INH and placebo.Citation53
Berinert® P studies
Bork reported 517 episodes of laryngeal edema in 42 patients, of which 18 patients received 500 or 1000 U of Berinert® P in 193 episodes. The therapy was effective in all laryngeal edemas.Citation69
Recently, a double-blind, placebo-controlled, international, multicenter, prospective angioedema C1-INH trial (I.M.P.A.C.T.1) has been completed, which compared the efficacy (shortening onset of relief of symptoms) of Berinert® P at intravenous doses of 10 or 20 U/kg body weight with placebo in 125 patients with type I or II HAE with moderate to severe abdominal or facial attacks. Only single attacks were evaluated. After the start of the treatment, patients were observed for a minimum of 4 h. If no improvement was observed, they received a rescue medication, then the onset of symptom relief was set to 24 h.
Subjects receiving 20 U/kg body weight presented a significant reduction in the median time to onset of relief of symptoms compared with the placebo group (0.5 versus 1.5 h, P = 0.0025). Median time to complete resolution of all HAE symptoms was also significantly shorter in the 20 U/kg group compared with the control group (4.92 versus 7.79 h, P = 0.0237). At a dose of 10 U/kg, the median time to onset of relief was 1.2 h, which was not significantly different from the placebo group.
Most patients (87.1%) had type I HAE. Overall, 79% suffered abdominal attacks and 20.2% suffered facial attacks. There was no statistical difference between facial and abdominal attack treatment effect, although the median time to onset of symptom relief was shorter for abdominal attacks. In the same way, the efficacy was higher for severe than for moderate attacks, but any difference could not be demonstrated statistically (). In patients treated with C1-INH 20 U/kg, no new attacks were suffered before the complete resolution of the previous attack; therefore, rebound angioedema seems not to exist.
Table 3 Efficacy of Berinert® P at intravenous doses of 10 or 20 U/kg body weight versus placebo in 125 patients with type I or II HAE with moderate to severe abdominal to facial attacks. I.M.P.A.C.T.1 study
Viral safety and adverse events were monitored up to 12 weeks after treatment. No seroconversions were observed for HIV, hepatitis virus, or human B19 virus. No serious adverse events were reported within 4 h after study treatment. Later, four patients had nine episodes of HAE exacerbation.Citation81
The lack of statistical significance for C1-INH 10 U/kg versus placebo related to onset of relief is surprising after 25 years of experience using the same or lower doses with good results.
A prospective, open-label trial, I.M.P.A.C.T.2, showed a median time to onset of symptom relief of 15 min for laryngeal attacks, 20 min for abdominal attacks, 28 min for facial attacks, and 31 min for peripheral attacks. These results were based on treatment with 20 U/kg of C1-INH in 975 episodes of HAE attacks at any body location in 57 patients. No serious adverse events were reported.Citation82
Nanofiltered C1-INH concentrate: Cinryze® formerly Cetor®
The Red Cross in Amsterdam (currently Sanquin Plasma Product) developed in 1974 the first large-scale method to prepare C1-INH. A viral inactivation step was added to the manufacturing process in 1986. The product, brand name Cetor®, has been in the Netherlands market since 1997, and it has been recently acquired by Lev Pharmaceuticals to be commercialized in the United States, adding to Cetor® a double-nanofiltration to enhance viral safety. The nanofiltered version of Cetor® is marketed in the United States under the brand name Cinryze®. It is manufactured by Sanquin in the Netherlands using US plasma.
Recently, Lev Pharmaceuticals has been acquired by ViroPharma Incorporated, a company specialized in commercializing products to treat inflammatory diseases. The company received FDA approval for Cinryze® in October 2008 for routine prophylaxis against attacks in adolescent and adult patients with HAE. It is not licensed for use in acute attacks of HAE in the United States. In June 2009, the FDA approved the patient labeling to include self-administration for routine prophylaxis, once patients are properly trained by their health care provider.
In March 2010, ViroPharma Incorporated announced the European approval request for both prevention and treatment of acute attacks of HAE as well as the initiation of two open-label, phase II studies: one to evaluate the safety, pharmacokinetics, and pharmacodynamics of subcutaneous versus intravenous administration; the other with the aim to evaluate doses in children below 12 years of age with acute attacks.Citation83
The results of two randomized trials of nanofiltered C1-INH concentrate for the management of HAE are reported. One study evaluates its use in acute attacks, and the other reports its use as prophylaxis. A total of 68 patients with severe attacks were randomly assigned to receive either C1-INH 1000 U intravenously (36 subjects) or placebo (35 subjects). If significant relief was not reported within 60 min, subjects were then given a second dose of the same study drug they received initially. The median time to beginning of unequivocal relief of symptoms was significantly shorter in the C1-INH group (median time 2 h) than in the placebo group (median time > 4 h) (P = 0.026). C1-INH-treated patients’ group also showed a statistically significant improvement in median time to complete resolution of symptoms (P = 0.004). The efficacy of the product did not vary by attack location.
The second study assessed the efficacy and safety of nanofiltered C1-INH concentrate as long-term prophylaxis to prevent attacks of angioedema. A total of 22 patients suffering from frequent attacks were treated with 1000 U of C1-INH or placebo twice a week during 12 weeks, then crossed over and received the opposite treatment for the same period. During the treatment periods, the frequency of attacks decreased in a significant manner (6.26 versus 12.73; P < 0.0001). It is stable at room temperature.Citation84
Recombinant C1-INH: efficacy
Recombinant C1-INH (rC1-INH) conestat alfa (Rhucin®, Pharming Technologies BV, Leiden, the Netherlands) is a concentrate for intravenous infusion, produced in transgenic rabbits’ milk. It is identical to human plasma-derived C1-INH at the amino acid level and demonstrates the same inhibitory profile as plasma-derived C1-INH. Reports from van Doorn et al estimated that infusion of rC1-INH at doses of 100 U/kg resulted in a half-life of about 3 h.Citation85
Choi et al in an open-label, phase II study of rC1-INH, demonstrated beginning of relief on average within 1 h (median time 30 min), with time to minimal symptoms between 6 and 12 h after infusion. No late angioedema relapses were found.Citation86
Two phase III studies have been performed for rC1-INH in the treatment of acute attacks of angioedema in HAE patients. A European randomized, placebo-controlled, double-blind clinical study in 32 HAE patients treated with rC1-INH (100 U/kg) was conducted. It was stopped before completion for ethical reasons because there was a strong and highly significant positive difference for rC1-INH versus placebo in median time to beginning of relief (62 versus 508 min, P = 0.0009) as well as time to minimal symptoms (480 versus 1480 min, P = 0.0038).
The second phase III study was performed in the United States and Canada in 39 HAE subjects receiving rC1-INH (100 and 50 U/kg). The results exhibited a significant superiority for rC1-INH versus placebo in median time to beginning of relief (68 min for rC1-INH 100 U/kg, 122 min for 50 U/kg, and 258 min for placebo). Time to minimal symptoms was also significantly shortened after treatment with rC1-INH (245 min at 100 U/kg and 247 min at 50 U/kg, and 1101 min for placebo) ().
Table 4 Efficacy of recombinant C1-INH concentrate
There were no serious allergic or clinically relevant immune responses reported in either of the two studies, although there is a risk of anaphylactic reactions based on either contaminating rabbit proteins or the glycosylation differences.Citation87
The nature of recombinant products eliminates concerns about potential viral infection transmission from plasma derivatives; another great advantage is that supply can be increased on demand.
The short half-life of the rC1-INH can make this product less convenient for prophylactic use, especially long-term prophylaxis.Citation88
Conestat alfa concentrate is currently under review by the European Medicines Agency, as well as by the FDA. The product will be marketed in the European Union under the name Ruconest®.Citation89
Treatment of acute attacks: inhibition of bradykinin generation blocking the enzyme kallikrein
Ecallantide (Kalbitor®, Dyax, Cambridge, MA, USA), a selective plasma kallikrein inhibitor, is a 60-amino acid peptide produced in the Pichia pastoris strain of yeast. It is available in the United States for the treatment of acute attacks of HAE in patients 16 years of age and older. The recommended dose of ecallantide to treat an angioedema attack is 30 mg, administered in three 10-mg subcutaneous injections. Maximum ecallantide levels are reached 2–3 h following administration, and the half-life is <2 h.Citation90
Ecallantide was studied in two double-blind, randomized clinical trials that enrolled 143 individuals. Both studies were performed in the United States and involved subjects randomized 1:1 to receive ecallantide 30 mg or placebo during a moderate or acute attack at any location.
The first trial (EDEMA3) measured response to therapy in 72 patients using a categorical scale, treatment outcome score (TOS) at 4 h. Ecallantide-treated patients reported a mean TOS score of 49.5 ± 59.4 compared with 18.5 ± 67.8 in placebo-treated patients (P = 0.037). The improvement in TOS score was maintained at 24 h (44.3 ± 70.4 versus –0.5 ± 87.9, P = 0.044).
The second trial (EDEMA4) measured improvement of symptoms in 96 patients with the primary endpoint being mean symptom complex severity (MSCS) at 4 h. Ecallantide-treated subjects reported a mean decrease in symptom score at 4 h of 0.81 compared with a decrease of 0.37 in placebo-treated subjects (P = 0.01). At 24 h, mean symptom scores fell by 1.5 in the ecallantide-treated subjects compared with 1.1 in the placebo-treated subjects (P = 0.039).Citation91
No differences were observed in the response to ecallantide based on the location of swelling; however, subjects who presented relatively late in the attack (6–8 h) showed less benefit than those who presented earlier.Citation92
The overall safety profile of ecallantide observed in EDEMA4 was similar to that of the placebo. The most common treatment-emergent adverse events (nausea, headache, and dizziness) were mild or moderate and occurred at a similar proportion in both the ecallantide and placebo groups. No symptoms suggestive of hypersensitivity were reported in the treatment group. However, as anaphylactic-like reactions have been reported in some patients receiving the product, there is a black box warning of anaphylactic potential, requiring that the drug be administered by a health care provider. Out of refrigeration, it is stable for 14 days.Citation91
Treatment of acute attacks: inhibition of bradykinin generation preventing its interaction with the receptor
Icatibant (Firazyr®, Jerini, Berlin, Germany) is a synthetic selective decapeptide bradykinin B2 receptor competitive antagonist that contains five nonnatural amino acids to enhance resistance to peptidases. Icatibant is administered subcutaneously as a single 30-mg injection, achieving peak concentration within 30 min, and has a half-life of 1–2 h.Citation94 Icatibant (bradykinin B2 receptor inhibitor) is approved in Europe for acute treatment of HAE.
Icatibant was studied in two double-blind, randomized, placebo-controlled, phase III clinical trials,Citation94 during moderate to severe abdominal or cutaneous angioedema attack, in subjects randomized 1:1. One study, FAST-1 compared icatibant with placebo in 56 subjects in different American countries; the second study, FAST-2, compared icatibant with tranexamic acid in 72 subjects in Europe and Israel. Primary endpoint was time to onset of symptom relief. In the FAST-2 study, time to onset of relief was significantly faster in the icatibant-treated group (2 versus 12 h, P < 0.0001). On the basis of this, the drug was approved for use for acute attacks in the European Union. In contrast, the FAST-1 study failed to show a significant benefit for icatibant (2.5 versus 4.6 h, P = 0.13). The drug was not approved by the FDA, and a new phase III trial is ongoing. The investigators of the FAST-1 suggest that this study did not reach statistical significance due to the stringent definition of the primary endpoint as well as the early use of rescue medication. Icatibant was generally well tolerated, although most patients had an injection-site reaction that was transient. Icatibant is stable at room temperature.
Subanalyses of these trials suggest that icatibant may be as effective for laryngeal swelling as for abdominal and cutaneous symptoms, with the time required for first symptom improvement being ≤1 h.Citation95
The drug was also used in three acute abdominal attacks of HAE type III with rapid resolution of symptoms.Citation96
A recent report suggested that the permeability enhancement in HAE attacks may be transduced by the combination of bradykinin B2 receptors and bradykinin B1 receptors. Bradykinin antagonists that block both bradykinin receptors may therefore have important advantages over those that only block the bradykinin B2 receptor.Citation97
Summary of current therapeutic options in HAE acute attacks treatment
Replacement therapy
It was initially administered using FFP, but concerns arose with regard to the infectious risk and the controversial capacity to worsen attacks.Citation57–Citation59 The administration of C1-INH concentrates is a faster way to replace the missing protein. In plasma-derived concentrates, the risk of viral contamination has been greatly reduced by applying different viral inactivation and removal techniques. In Europe, plasma-derived C1-INH concentrates are being used to treat HAE attacks at a dose of 500–1500 U. The improvement is seen within 30–90 min.Citation29,Citation61,Citation80,Citation83 Their long half-life, mean 31.5–47.8 h, makes the product convenient also for prophylactic use.Citation71,Citation72,Citation76
All C1-INH concentrates (plasma-derived and recombinant) are administered intravenously.
Two plasma-derived C1-INH concentrates have been licensed recently in the United States: Berinert® and Cinryze®.
Berinert® (CSL Behring) is a pasteurized C1-INH concentrate widely used in Europe and recently licensed by the FDA to treat acute abdominal and facial attacks in adolescent and adult HAE patients.Citation70 Associated adverse effects (scarce despite its widespread use) include anaphylactoid reactions (most probably related to too rapid or too low temperature administration).Citation61 The I.M.P.A.C.T.1 trial has shown Berinert® to be effective to treat acute angioedema attacks at a dose of 20 U/kg.Citation81 In the I.M.P.A.C.T.2 trial, 20 U/kg showed a median time to onset of improvement of 15 min for laryngeal attacks, 20 min for abdominal attacks, 28 min for facial attacks, and 31 min for peripheral attacks.Citation82 No serious adverse events were reported.Citation81,Citation82 The product can be stored at room temperature below 25°C.Citation67
Cinryze® (ViroPharma Incorporated, Exton, PA, USA) is manufactured by the same process as the existing Cetor® from Sanquin but is double nanofiltered. It has recently been approved by the FDA for long-term prophylactic use only for adolescent and adults at a dose of 1000 U every 3 or 4 days. Although the product causes significant reductions in both the severity and the duration of HAE attacks, the approval for this indication is still pending. Subcutaneous administration is under trial. The tolerability of the product is goodCitation83 and is stable at room temperature.Citation84
Rhucin® (Pharming Technologies BV), conestat alfa, is a recombinant C1-INH concentrate produced in transgenic rabbits’ milk. Its half-life is dose dependent, and at 100 U/kg body weight it is about 3 h.Citation77 The product is currently under review by the FDA as well as by the European Medicines Agency (brand name Ruconest).Citation89
The inhibition of bradykinin generation
Plasma kallikrein inhibitor, ecallantide (Kalbitor®, Dyax), is a 60-amino acid peptide recently approved in the United States for treatment of HAE in patients 16 years of age and older at a recommended dose of 30 mg, administered as three 10-mg subcutaneous injections. About 72.5% of patients treated with ecallantide reported significant improvement in symptoms within 4 h of administration. The half-life is about 2 h.Citation90
It is not recommended for self-infusion because of anaphylactic-like reaction risk, and there is a black box warning regarding this potential. Ecallantide needs to be refrigerated for periods exceeding 14 days.Citation91
Icatibant (Firazyr®, Jerini) is a small peptide bradykinin receptor blocker licensed in Europe for use in treatment of HAE attacks. Dose is 30 mg administered subcutaneously in adults. The time to first symptom improvement is ≤1 h.Citation95 Its half-life is 1–2 h.Citation94 Mild injection-site reactions are common. The product is stable at room temperature.Citation95
Acknowledgment
We thank Dr Jonathan Rogerson for his assistance in drafting the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- PowellRJDu ToitGLSiddiqueNBSACI guidelines for the management of chronic urticaria and angio-oedemaClin Exp Allergy200737563165017456211
- GrigoriadouSLonghurstHJClinical immunology review series: an approach to the patient with angio-oedemaClin Exp Immunol2009155336737719220828
- FrankMM8. Hereditary angioedemaJ Allergy Clin Immunol2008121 Suppl 2S398S40118241690
- GompelsMMLockRJAbinunMC1 inhibitor deficiency: consensus documentClin Exp Immunol2005139337939415730382
- BorkKBarnstedtSEKochPTraupeHHereditary angioedema with normal C1-inhibitor activity in womenLancet2000356922521321710963200
- KaplanAPGhebrehiwetBThe plasma bradykinin-forming pathways and its interrelationships with complementMol Immunol201047132161216920580091
- BinkleyKEFactor XII mutations, estrogen-dependent inherited angioedema, and related conditionsAllergy Asthma Clin Immunol2010611620667119
- TosiMMolecular genetics of C1 inhibitorImmunobiology199811923583659777419
- RocheOBlanchACaballeroTSastreNCallejoDLópez-TrascasaMHereditary angioedema due to C1 inhibitor deficiency: patient registry and approach to the prevalence in SpainAnn Allergy Asthma Immunol200594449850315875532
- WeilerCRvan DellenRGGenetic test indications and interpretations in patients with hereditary angioedemaMayo Clin Proc200681795897216835976
- BrickmanCMTsokosGCBalowJEImmunoregulatory disorders associated with hereditary angioedema. I. Clinical manifestations of autoimmune diseaseJ Allergy Clin Immunol19867757497573084606
- BowenTCicardiMFarkasH2010 International consensus algorithm for the diagnosis, therapy and management of hereditary angioedemaAllergy Asthma Clin Immunol2010612420667127
- BasMAdamsVSuvoravaTNiehuesTHoffmannTKKojdaGNonallergic angioedema: role of bradykininAllergy200762884285617620062
- NzeakoUCFrigasETremaineWJHereditary angioedema: a broad review for cliniciansArch Intern Med20011612417242911700154
- BorkKMengGStaubachPHardtJHereditary angioedema: new findings concerning symptoms, affected organs, and courseAm J Med2006119326727416490473
- ZurawBLClinical practice. Hereditary angioedemaN Engl J Med2008359101027103618768946
- CunninghamDSJensenJTHereditary angioneurotic edema in the puerperium. A case reportJ Reprod Med19913643123132072364
- FrankMMGelfandJAAtkinsonJPHereditary angioedema: the clinical syndrome and its managementAnn Intern Med19768455805931275365
- FrankMMEffect of sex hormones on the complement-related clinical disorder of hereditary angioedemaArthritis Rheum1979221112951299508378
- BorumMLHowardDEHereditary angioedema. Complex symptoms can make diagnosis difficultPostgrad Med199810342512552569553599
- ByrdJBAdamABrownNJAngiotensin-converting enzyme inhibitor-associated angioedemaImmunol Allergy Clin North Am200626472573717085287
- KempJGCraigTJVariability of prodromal signs and symptoms associated with hereditary angioedema attacks: a literature reviewAllergy Asthma Proc200930549349919843403
- PappalardoECicardiMDuponchelCFrequent de novo mutations and exon deletions in the C1 inhibitor gene of patients with angioedemaJ Allergy Clin Immunol200010661147115411112899
- BorkKHypovolemic shock caused by ascites in hereditary angioedemaMed Klin (Munich)19989395549792023
- KrauseKHRentropUMehreganUCerebral manifestations in angioneurotic edemaJ Neurol Sci1979423429435512675
- BrettleRPDunmowREMilneLAYapPLAngioneurotic oedema in the elderlyScott Med J19822743093117146879
- ThorvaldssonSESedlackREGleichGJRuddySJAngioneurotic edema and deficiency of C’1 esterase inhibitor in a 61-year-old womanAnn Intern Med19697123533575800297
- LandermanNSHereditary angioneurotic edema. I. Case reports and review of the literatureJ Allergy19623331632914461961
- AgostoniACicardiMHereditary and acquired C1-inhibitor deficiency: biological and clinical characteristics in 235 patientsMedicine (Baltimore)19927142062151518394
- CicardiMCastelliRZingaleLCAgostoniASide effects of long-term prophylaxis with attenuated androgens in hereditary angioedema: comparison of treated and untreated patientsJ Allergy Clin Immunol19979921941969042044
- FrankMMSergentJSKaneMAAllingDWEpsilon aminocaproic acid therapy of hereditary angioneurotic edema. A double-blind studyN Engl J Med1972286158088124551861
- GelfandJASherinsRJAllingDWFrankMMTreatment of hereditary angioedema with danazol. Reversal of clinical and biochemical abnormalitiesN Engl J Med19762952614441448792688
- FrankMMHereditary angioedema: the clinical syndrome and its management in the United StatesImmunol Allergy Clin North Am200626465366817085283
- ShefferALAustenKFRosenFSTranexamic acid therapy in hereditary angioneurotic edemaN Engl J Med197228794524544558045
- GrattanCEHBlackAKUrticaria and mastocytosisBurnsTBreathnachSCoxNGriffithsGRook’s Textbook of Dermatology8th edOxfordWiley-Blackwell201022.2122.22
- LaurentJGuinnepainMTAngioedema associated with C1 inhibitor deficiencyClin Rev Allergy Immunol199917451352310829818
- ShefferALFearonDTAustenKFClinical and biochemical effects of stanozolol therapy for hereditary angioedemaJ Allergy Clin Immunol19816831811876790595
- BorkKPittonMHartenPKochPHepatocellular adenomas in patients taking danazol for hereditary angio-oedemaLancet199935391581066106710199359
- SzéplakiGVargaLValentinSAdverse effects of danazol prophylaxis on the lipid profiles of patients with hereditary angioedemaJ Allergy Clin Immunol2005115486486915806011
- SloaneDELeeCWShefferALHereditary angioedema: safety of long-term stanozolol therapyJ Allergy Clin Immunol2007120365465817765757
- BorkKBygumAHardtJBenefits and risks of danazol in hereditary angioedema: a long-term survey of 118 patientsAnn Allergy Asthma Immunol2008100215316118320917
- BuamahPKAn apparent danazol-induced primary hepatocellular carcinoma: case reportJ Surg Oncol19852821141162578590
- WeillBJMenkèsCJCormierCLouvelADougadosMHoussinDHepatocellular carcinoma after danazol therapyJ Rheumatol1988159144714492848945
- CramponDBarnoudRDurandMDanazol therapy: an unusual aetiology of hepatocellular carcinomaJ Hepatol1998296103510369875659
- ConfavreuxCSèvePBroussolleCRenaudierPDucerfCDanazol-induced hepatocellular carcinomaQJM200396431731812651980
- FarkasHVargaLSzéplakiGVisyBHarmatGBowenTManagement of hereditary angioedema in pediatric patientsPediatrics20071203e713e72217724112
- BouilletLHereditary angioedema in womenAllergy Asthma Clin Immunol2010611720667120
- JaffeCJAtkinsonJPGelfandJAFrankMMHereditary angioedema: the use of fresh frozen plasma for prophylaxis in patients undergoing oral surgeryJ Allergy Clin Immunol19755563863931138015
- BowenTCicardiMBorkKHereditary angioedema: a current state-of-the-art review. VII. Canadian Hungarian 2007 International Consensus Algorithm for the Diagnosis, Therapy, and Management of Hereditary AngioedemaAnn Allergy Asthma Immunol2008100 1 Suppl 2S30S4018220150
- EwaldGAEisenbergPRPlasmin-mediated activation of contact system in response to pharmacological thrombolysisCirculation199591128367805216
- LynchMPentecostBLLittlerWAStockleyRAWhy do patients develop reactions to streptokinase?1993942279285
- FrancisCWBrennerBLeddyJPMarderVJAngioedema during therapy with recombinant tissue plasminogen activatorBr J Haematol19917745625631902745
- ZurawBLChristiansenSCNew promise and hope for treating hereditary angioedemaExpert Opin Investig Drugs2008175697706
- DonaldsonVHEvansRRA biochemical abnormality in hereditary angioneurotic edema: absence of serum inhibitor of C’1-esteraseAm J Med196335374414046003
- LandermanNSWebsterMEBeckerELRatcliffeHEHereditary angioneurotic edema. II. Deficiency of inhibitor for serum globulin permeability factor and/or plasma kallikreinJ Allergy19623333034114461960
- PickeringRJGoodRAKellyJRGewurzHReplacement therapy in hereditary angioedema. Successful treatment of two patients with fresh frozen plasmaLancet1969175903263304179348
- PremattaMGibbsJGPrattELStoughtonTRCraigTJFresh frozen plasma for the treatment of hereditary angioedemaAnn Allergy Asthma Immunol200798438338817458436
- ZurawBLDiagnosis and management of hereditary angioedema: an American approachTransfus Apher Sci200329323924514572816
- ZurawBLCurrent and future therapy for hereditary angioedemaClin Immunol20051141101615596404
- VogelaarEFBrummelhuisHGKrijnenHWContributions to the optimal use of human blood. 3. Large-scale preparation of human C1 esterase inhibitor concentrate for clinical useVox Sang19742621181274207849
- de SerresJGronerALindnerJSafety and efficacy of pasteurized C1 inhibitor concentrate (Berinert P) in hereditary angioedema: a reviewTransfus Apher Sci200329324725414572817
- LeviMChoiGPicavetCHackCESelf-administration of C1-inhibitor concentrate in patients with hereditary or acquired angioedema caused by C1-inhibitor deficiencyJ Allergy Clin Immunol2006117490490816630950
- Pastó-CardonaLBordas-OrpinellJMercadal-OrfilaGPérez de la VaraAJódar-MassanésRProfilaxis y tratamiento del angioedema hereditario y adquirido en el HUB; utilización del inhibidor de la C1-esterasaFarm Hosp (Madrid)2003276346352
- Aygoren-PursunEMartinez-SaguerIRusickeEKlingebielTKreuzWOn demand treatment and home therapy of hereditary angioedema in Germany – the Frankfurt experienceAllergy Asthma Clin Immunol2010612120667124
- CicardiMZingaleLHow do we treat patients with hereditary angioedemaTransfus Apher Sci200329322122714572813
- CicardiMZingaleLCZanichelliADeliliersDLCacciaSThe use of plasma-derived C1 inhibitor in the treatment of hereditary angioedemaExpert Opin Pharmacother20078183173318118035961
- SchulteUHofmannPStability of a New Formulation of C1-esterase-inhibitor Concentrate at Room TemperatureInternational Clinical Practice SeriesTunbridge Wells (Kent)Wells Medical, Ltd2004
- Martinez-SaguerIHellerCFischerDEttingshausenCEKreuzWProphylactic treatment with pasteurized C1 inhibitor in hereditary angioedema (HAE) – a prospective 32 months follow upBlood199994 Suppl 12339
- BorkKBarnstedtSETreatment of 193 episodes of laryngeal edema with C1 inhibitor concentrate in patients with hereditary angioedemaArch Intern Med2001161571471811231704
- US Food and Drug Administration (FDA)FDA Approves Berinert to Treat Abdominal Attacks, Facial Swelling Associated with Hereditary Angioedema Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm186257.htmAccessed 2010 Oct 21.
- Martinez-SaguerIRusickeEAygören-PürsünEvon HentigNKlingebielTKreuzWPharmacokinetic analysis of human plasma-derived pasteurized C1-inhibitor concentrate in adults and children with hereditary angioedema: a prospective studyTransfusion201050235436019788511
- KunschakMEnglWMaritschFA randomized, controlled trial to study the efficacy and safety of C1 inhibitor concentrate in treating hereditary angioedemaTransfusion19983865405499661687
- LehmannALangJBoldtJSaggauWSuccessful off-pump coronary artery bypass graft surgery in a patient with hereditary angioedemaJ Cardiothorac Vasc Anesth200216447347612154430
- AlvarezJMSuccessful use of C1 esterase inhibitor protein in a patient with hereditary angioneurotic edema requiring coronary artery bypass surgeryJ Thorac Cardiovasc Surg2000119116817110612778
- Martinez-SaguerIHellerCKreuzWContinuous infusion of a pasteurized C1 inhibitor concentrate in patients with severe hereditary angioedema (HAE)Eur J Pediatr1999158 Suppl 3S211S220
- BernsteinJARitchieBLevyRJPopulation pharmacokinetics of plasma-derived C1 esterase inhibitor concentrate used to treat acute hereditary angioedema attacksAnn Allergy Asthma Immunol2010105214915420674826
- BernsteinJAHereditary angioedema: a current state-of-the-art review, VIII: current status of emerging therapiesAnn Allergy Asthma Immunol20081001 Suppl 2S41S4618220151
- AgostoniABergamaschiniLMartignoniGCicardiMMarasiniBTreatment of acute attacks of hereditary angioedema with C1-inhibitor concentrateAnn Allergy19804452993016155097
- GadekJEHoseaSWGelfandJAReplacement therapy in hereditary angioedema: successful treatment of acute episodes of angioedema with partly purified C1 inhibitorN Engl J Med1980302105425467351888
- WaytesATRosenFSFrankMMTreatment of hereditary angioedema with a vapor-heated C1 inhibitor concentrateN Engl J Med199633425163016348628358
- CraigTJLevyRJWassermanRLEfficacy of human C1 esterase inhibitor concentrate compared with placebo in acute hereditary angioedema attacksJ Allergy Clin Immunol2009124480180819767078
- GoodmanSLevyRWassermanRC1 esterase inhibitor (C1-INH) concentrate in the treatment of acute attacks in hereditary angioedema: interim results of the treatment of 975 attacks in an ongoing, prospective, open-label study in North America (I.M.P.A.C.T.2)J Allergy Clin Immunol20101252 Suppl 1AB166
- ViroPharma Incorporated (VPHM.OQ) Key Developments Reuters.comAccessed 2010 Aug 30
- ZurawBLBussePJWhiteMNanofiltered C1 inhibitor concentrate for treatment of hereditary angioedemaN Engl J Med2010363651352220818886
- van DoornMBBurggraafJvan DamTA phase I study of recombinant human C1 inhibitor in asymptomatic patients with hereditary angioedemaJ Allergy Clin Immunol2005116487688316210064
- ChoiGSoetersMRFarkasHRecombinant human C1-inhibitor in the treatment of acute angioedema attacksTransfusion20074761028103217524093
- ZurawBLHAE therapies: past present and futureAllergy Asthma Clin Immunol2010612320667126
- EidelmanFJHereditary angioedema: new therapeutic options for a potentially deadly disorderBMC Blood Disord201010320470390
- http://www.biospace.com/news_story.aspx?NewsEntityId=185307Accessed 2010 Sep 3.
- ZurawBLChristiansenSCNew promise and hope for treating hereditary angioedemaExpert Opin Investig Drugs200817697706
- LevyRMcNeilDLiHHsuFIHornPRobertsJResults of a 2-stage, phase 3 pivotal trial, EDEMA3: a study of subcutaneous DX-88 (Ecallantide), a plasma kallikrein inhibitor, in patients with hereditary angioedema (HAE)J Allergy Clin Immunol20081212 Suppl 1S231
- BantaECraigTHornPTPullmanWETime of intervention with ecallantide for the treatment of acute attacks of hereditary angioedema: results from the edema development programAnn Allergy2009103A131A132
- DeeksEDIcatibantDrugs2010701738120030426
- CHMP assessment report for Firazyr http://www.ema.europa.eu/ema/index.jsp?curl=pages/home/Home_Page.jspAccessed 2010 Oct 26.
- CicardiMBanerjiABrachoFIcatibant, a new bradykinin-receptor antagonist, in hereditary angioedemaN Engl J Med2010363653254120818888
- BouilletLBocon-GibodIPonardDBradykinin receptor 2 antagonist (icatibant) for hereditary angioedema type III attacksAnn Allergy Asthma Immunol2009103544819927548
- BossiFFischettiFRegoliDNovel pathogenic mechanism and therapeutic approaches to angioedema associated with C1 inhibitor deficiencyJ Allergy Clin Immunol2009124613031310e419796797