
Abstract
Secondary hyperparathyroidism (SHPT), a very frequent, severe, and worsening complication of chronic kidney disease, is characterized by high serum parathyroid hormone (PTH), parathyroid gland hyperplasia, and disturbances in mineral metabolism. Clinically, SHPT shows renal osteodystrophy, vascular calcification, cardiovascular damage, and fatal outcome. Calcium-sensing receptor (CaSR) is the main physiological regulator of PTH secretion; its activation by calcium rapidly inhibits PTH. Another important player in regulating mineral metabolism is vitamin D receptor (VDR), which is under the influence of vitamin D and influences the intestinal absorption of calcium and phosphate, PTH gene expression, and bone calcium mobilization. Serum phosphate levels influence fibroblast growth factor 23 (FGF-23) production, a phosphatonin that modulates serum phosphate reabsorption, PTH synthesis, and vitamin D production. Current therapeutic approaches consist of 1) phosphate intake control by diet or phosphate binders, 2) vitamin D by VDR activation, and 3) calcimimetic agents that activate CaSR. Recently, a new long-acting peptide (etelcalcetide) belonging to the calcimimetics class was approved for intravenous use in hemodialysis patients with SHPT. Etelcalcetide binds directly to CaSR, by a sulfide bond, inhibiting the production and secretion of PTH by parathyroid glands. After intravenous administration in rats, etelcalcetide is quickly distributed to the tissues and eliminated by kidneys, while in uremic animals the nonrenal excretion is only 1.2%. In hemodialysis patients, the treatment itself is the main route of elimination. Etelcalcetide in hemodialysis patients with SHPT was more effective than placebo and cinacalcet, with a PTH reduction of >30% in 76% of patients with etelcalcetide versus 10% with placebo. Particular attention was paid to the safety of the drug; the most common adverse event was asymptomatic blood calcium reduction, similar to cinacalcet, while gastrointestinal symptoms were less frequent. This promising new drug available for better control of SHPT will, together with drugs already in use, optimize the treatment to normalize the biochemical parameters.
Pathogenesis of secondary hyperparathyroidism in chronic kidney disease
Parathyroid hormone (PTH) is a key regulator of calcium metabolism; it stimulates bone reabsorption, increases serum calcium and phosphorus levels, and promotes vitamin D synthesis.Citation1 Secondary hyperparathyroidism (SHPT), a common, serious, and progressive complication of chronic kidney disease (CKD), is characterized by high serum PTH, parathyroid gland hyperplasia, and disturbances in mineral metabolism, mainly hypocalcemia and hyperphosphatemia.Citation1 These mineral disturbances mainly cause renal osteodystrophy, progressive vascular calcification, and in turn, cardiovascular disease and death, especially in patients receiving hemodialysis.Citation2–Citation5 Together, this constellation of comorbidities is known as CKD–mineral and bone disorder (CKD-MBD).Citation6 In the US, the estimated prevalence of SHPT in patients with CKD ranges from 2 to nearly 5 million individuals, with 30%–50% of end-stage renal disease (ESRD) patients affected by SHPT.Citation3
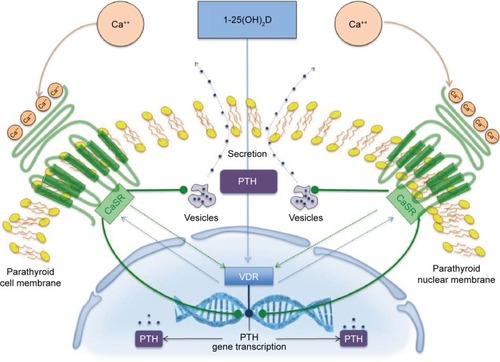
Under normal physiological conditions (), the principal regulator of PTH secretion and parathyroid gland function is the calcium-sensing receptor (CaSR).Citation4–Citation7 Activation of the CaSR by serum calcium rapidly inhibits PTH synthesis and secretion and parathyroid gland growth. Furthermore, the CaSR influences PTH gene expression and may also upregulate the vitamin D receptor (VDR). Parathyroid glands express high levels of the VDR, which when activated by vitamin D binding decreases PTH gene transcription; on the contrary, decreasing levels of vitamin D or vitamin D deficiency stimulate PTH synthesis.Citation8 VDRs are expressed in several tissues, such as the intestines (where calcium and phosphate absorption is regulated), the kidneys (where calcium reabsorption is regulated), and in bone (where calcium mobilization is regulated).Citation9 VDR activation by the active form of vitamin D, calcitriol, also elevates parathyroid expression of the CaSR.Citation4–Citation7 Moreover, VDR activation in the gastrointestinal tract increases calcium absorption, thus elevating serum calcium levels and controlling parathyroid gland activity through CaSR activation.Citation8,Citation10 Serum phosphorus and phosphorus intake also affect calcitriol levels, primarily through modulation of the activity of 25-hydroxyvitamin D3-1α-hydroxylase and PTH expression by the parathyroid. Phosphate also stimulates production of the phosphatonin and fibroblast growth factor 23 (FGF-23) in osteocytes and osteoblasts.Citation11 FGF-23 binds to a receptor complex consisting of FGFR1 and the transmembrane protein Klotho and modulates phosphate reabsorption, PTH synthesis, and vitamin D production. In turn, both PTH and FGF-23 regulate phosphate reabsorption by affecting the local density of the type 2 sodium-dependent phosphate cotransporter in the renal proximal tubules.Citation11,Citation12
Figure 1 Regulation of PTH synthesis and secretion by CaSR and VDR in parathyroid glands.
Hyperphosphatemia, hypocalcemia, and low calcitriol levels that occur as kidney function declines are major players in the pathogenesis of SHPT in patients with CKD.Citation11,Citation13 Low calcium levels can downregulate the cellular expression of CaSR after the parathyroid cell proliferation. Compensatory downregulation of the CaSR and the VDR in the parathyroid may play a central role in the development of mineral disturbances in SHPT.Citation11,Citation13 Hyperphosphatemia directly causes increased PTH synthesis and secretion, and parathyroid hyperplasia, with downregulation of both CaSR and VDR expression in SHPT.Citation14 Additionally, high serum phosphate levels inhibit the activity of 25-hydroxyvitamin D3-1α-hydroxylase, the enzyme that converts vitamin D to its active form, calcitriol, thus disrupting the feedback loop acting through the CaSR and VDR that suppresses PTH.Citation5,Citation11 Persistent alterations in the signaling of the CaSR and VDR, including the reduced expression of both, can eventually result in refractory SHPT, in which the parathyroid gland becomes insensitive to calcium- or calcitriol-mediated inhibition of PTH synthesis.Citation4,Citation10 As kidney function declines in CKD, levels of FGF-23 are also increased.Citation11 This has been attributed, at least in part, to reduced levels of Klotho in the kidney and parathyroid gland that occur as kidney function declines.Citation15,Citation16 Two additional factors that have been associated with disease progression and cardiovascular disease in CKD are indoxyl sulfate and p-cresyl sulfate, products of colonic bacterial fermentation of dietary proteins.Citation17
Continuous stimulation of the parathyroid glands by these derangements in mineral homeostasis promotes PTH synthesis and eventually parathyroid hyperplasia.Citation11 Because of their integral roles in the pathogenesis of SHPT, the CaSR, the VDR, and FGF-23 are biologically plausible targets for emerging therapies in the treatment of this disorder.
Current treatment options
SHPT is a common, serious, and costly manifestation of CKD, with negative effects on patient outcomes, especially on HD. With current treatment approaches, a considerable proportion of patients have inadequately controlled PTH, phosphorus, and/or calcium levels, and the ranges of these often fall outside of recommended ranges.Citation18 Data from the Dialysis Outcomes and Practice Patterns Study (DOPPS) of patients receiving hemodialysis for >180 days support a greater risk of cardiovascular and all-cause mortality in patients with calcium levels >10 mg/dL, phosphorus levels >7 mg/dL, and PTH levels >600 pg/mL; risks are likewise increased in patients with combinations of these high-risk categories.Citation19,Citation20
Current treatment for SHPT should follow three steps: reduction of phosphorus uptake by dietary restriction or the use of phosphate binders; control of PTH with the use of vitamin D metabolites; and the use of calcimimetics, currently agents that allosterically modify the CaSR to enhance activation in the presence of circulating levels of calcium, thus reducing PTH ().Citation21 Parathyroidectomy is usually a treatment strategy of last resort, after pharmacotherapy has failed.Citation11 The goal of treatment is to maintain serum calcium, serum phosphorus, and PTH within accepted targeted ranges.Citation22 Because of the limitations associated with the standard-of-care treatment for SHPT, PTH targets are not met for many patients.Citation23
Table 1 Treatment options for secondary hyperparathyroidism
Low-phosphorus diet and phosphate binders
Current guidelines suggest maintaining serum calcium and phosphorous with the normal range via balanced diet and/or phosphate binders administration.Citation22 The use of vegetarian products as well as protein restriction is commonly suggested to limit phosphate intake.Citation22 Cooking methods such as boiling are also proposed to limit (20%–70%) the amount of phosphate contained in different foods.Citation23 A recent meta-analysis suggested a significant reduction of phosphate levels of about 0.8 mg/dL (95% confidence interval [CI]: −1.43 to −0.18).Citation24
In spite of these data, phosphate binders have long been perceived as a cornerstone in the treatment of SHPT.Citation1 Indeed, due to poor treatment adherence, diet is often insufficient to reach a desirable control of serum phosphate levels, and a wide range of phosphate binders are now available.Citation25 Although effective, aluminum-based phosphate binders have been replaced by calcium and iron-based and polymer-based phosphate binders due to their toxicity.Citation25 Current guidelines suggest to limit aluminum-based phosphate binders in case of severe hyperphosphatemia and for a short period of time.Citation22 When compared to placebo, all available compounds have been shown to lower serum phosphate to similar extent.Citation23 However, differences among drugs may exist. Calcium-free phosphate binders are associated with lower serum calcium, and differences in PTH control with various drugs have been reported.Citation24 Preliminary data also suggest that phosphate restriction and calcium-free phosphate binders may reduce FGF-23.Citation25 Although the clinical relevance of different biochemical profiles still needs to be elucidated, some lines of evidence suggest that calcium-based phosphate binders may accelerate vascular calcification deposition and progression when compared to calcium-free phosphate binders.Citation26 Calcium supplements can represent a substantial portion of an individual’s daily calcium intake and contribute to deposition of calcium crystals in soft tissuesCitation26 in individuals with normal renal functionCitation27 as well as renal function impairment.Citation26 Also, evidence supports the notion that calcium-free phosphate binders are associated with a better survival when compared to calcium-based phosphate binders,Citation28 although future efforts are still required to shed light on this vexing question. Similarly, future studies should investigate the impact of combination therapies for CKD-MBD on calcium and phosphate balance and their effect on outcome in CKD patients.Citation29
Calcimimetics
Calcimimetics are a newer class of agents for the treatment of SHPT in patients receiving renal replacement therapy.Citation30 This class of agents allosterically bind and activate the CaSR, increasing the response of the receptor to serum calcium (orthosteric agonist).Citation22 To date, cinacalcet is the only commercially available drug of this class, although other molecules are under clinical development or about to hit the market.Citation25,Citation30 Although effective in PTH lowering, calcimimetics do not increase intestinal calcium or phosphate absorption.Citation22,Citation31 In the pivotal phase 3 clinical study, treatment of uncontrolled SHPT with cinacalcet or placebo for 26 weeks resulted in a greater proportion of patients in the calcimimetic arm achieving intact PTH levels ≤250 pg/mL (43% versus 5% in the cinacalcet and placebo-treated study arms, respectively).Citation30 Of interest, besides a greater overall PTH suppression, a better control of serum calcium and phosphorous was also noted.Citation30 Additional studies further corroborate the PTH suppression efficacy of cinacalcet in combination with vitamin D or vitamin D analogs when compared with calcitriol as monotherapy.Citation21 Sixty five (65%) versus 36% of patients receiving cinacalcet or active vitamin D open-label monotherapy experienced a reduction in PTH from baseline of at least 30% in the ACHIEVE study.Citation32 In another open-label study of 16 weeks, 71% of patients receiving cinacalcet plus low-dose, active vitamin D treatment achieved PTH ≤300 pg/mL versus 22% of patients receiving vitamin D alone.Citation33 Notably, in all these studies, mild-to-moderate hypocalcemia was a common, albeit easily managed, side effect attributed to CaSR modulation and likely a reduction in calcium mobilization from bone due to a tighter PTH control.Citation11 Finally, the EVOLVE study, the largest placebo-controlled, double-blind clinical trial conducted in dialysis patients with SHPT also confirmed a greater achievement of biochemical parameters of CKD-MBD among patients treated with cinacalcet compared to placebo.Citation34,Citation35 Although the primary end point of the study (ie, time until death, myocardial infarction, hospitalization for unstable angina, heart failure, or peripheral vascular event) was unmet, serum levels of intact PTH, calcium, phosphate, and FGF-23 were better controlled among patients allocated to cinacalcet.Citation16,Citation35 Notably, when compared to placebo, the most common complaints associated with treatment with calcimimetic were nausea, vomiting, and hypocalcemia (12% versus 2% of cinacalcet as opposed to placebo-treated patients experiencing hypocalcemia)Citation16,Citation34 that contributed to the slightly higher discontinuation rate due to adverse events (AEs) reported in the cinacalcet group (16% versus 12%). CaSR modulation may exert beneficial effects beyond serum biochemical parameters control.Citation36,Citation37 Although inconclusive, the ADVANCE study (a phase 4 randomized clinical trial) showed a trend toward vascular calcification progression attenuation among subjects receiving low doses of active vitamin D and cinacalcet versus flexible doses of vitamin D to control SHPT.Citation38 Overall, a small but not significant reduction in coronary artery calcification (CAC) progression was noted. However, patients adherentCitation39 to the assigned therapy or with higher burden of CAC or cardiac valve calcification at study inception seem to benefit more from this combination theraphy.Citation37,Citation40 In a post hoc analysis, subjects with aortic valve calcification treated with CasR modulators experienced a 74% risk reduction (adjusted odds ratio: 0.26; 95% CI: 0.10–0.64) of CAC progression.Citation40 As in a previous study, the most common side effects reported by subjects assigned to cinacalcet treatment were gastrointestinal discomfort and hypocalcemia, affecting 21% and 7% of patients, respectively.Citation37
Although CaSR modulation is an effective strategy to control SHPT, future efforts are needed to elucidate the effect interactions of different drugs to control CKD-MBD. In a recently published post hoc analysisCitation38 of the INDEPENDENT study, a potentially deleterious effect of the combination of cinacalcet with calcium containing phosphate binders was shown. Indeed, among the 466 incident to dialysis patients recruited in the study, sevelamer but not calcium carbonate administration was associated with survival benefit.Citation38 However, the concomitant administration of cinacalcet significantly modulated the impact of these phosphate binders on mortality (interaction test P=0.006). Coadministration of cinacalcet and calcium-free phosphate binders (hazard ratio: 0.34, 95% CI: 0.14–0.81, P=0.01 for subjects treated with sevelamer and receiving cinacalcet or not) but not cinacalcet and calcium-containing phosphate binders (hazard ratio: 1.28, 95% CI: 0.82–2.00; P=0.26 for subjects treated with calcium cinacalcet and receiving cinacalcet or not) was associated with improved survival.Citation38 Although the hypothesis generating this piece of evidence suggests that calcium balance modulation may impact survival in CKD, future efforts are needed to explore the effects of different combination therapies.
Vitamin D and vitamin D derivatives
In patients with CKD stages 3–5 (), both nutritional (cholecalciferol, ergocalciferol, calcifediol) and VDR activators (VDRAs) such as calcitriol and its analogs can improve abnormal mineral homeostasis.Citation22 Although the optimal target of 25(OH)D remains uncertain, serum levels >30 ng/mL are accepted as a normal threshold.Citation41 Clinical data support a mild effect of nutritional vitamin D against nonsevere SHPT in CKD stages 3–5.Citation42 International guidelines suggest the correction of nutritional vitamin D deficiency as a first-line therapy to counteract the onset and progression of CKD-MBD in predialysis patients.Citation41,Citation43,Citation44 However, due to the inconsistency of current evidence on the best approach to correct 25(OH)D deficiency, the KDIGO, NICE, and ERBP guidelines are unable to provide any therapeutic suggestion on how to replenish low 25(OH) D levels.Citation22,Citation41,Citation43 Doses originally recommended by KDOQI guidelines were often insufficient to achieve the expected 25(OH)D levels.Citation45 Higher doses of cholecalciferol and ergocalciferol were thus suggested in 2012,Citation46 showing the superiority of cholecalciferol compared to ergocalciferol in replenishing 25(OH)D deficiency.Citation47 Wetmore et alCitation48 have recently randomized 44 nondialysis CKD patients to receive cholecalciferol 50,000 IU/wk versus ergocalciferol 50,000 IU/wk for 12 weeks, without suspending concomitant active therapy. Although cholecalciferol was more effective than ergocalciferol at raising serum 25(OH)D levels (45±16.5 ng/mL and 30.7 versus 15.3 ng/mL, P<0.01), changes in serum PTH or active vitamin D were similar between the groups, and a similar decline of 25(OH)D levels between the groups was observed after cessation of therapy.Citation48 Recent data support an innovative efficacy of a modified-release formulation of calcifediol,Citation49 probably favored by its capability to raise 25(OH)D levels slowly enough for limiting an abrupt activation of vitamin D catabolism.Citation50 This novel compound was effective in reducing iPTH levels in 44 predialysis CKD patients in a dose-dependent manner compared to placebo.Citation49 Independently from the type and dose of nutritional vitamin D adopted, 25(OH)D levels should not exceed 100 ng/mL, and particular caution should be paid while supplementing patients at high risk of 1-α-hydroxylase activity, as kidney transplant patients and those affected by sarcoidosis or B-cell lymphoma.Citation42 VDRA was shown to be effective in counteracting SHPT in nondialysis CKD patients.Citation51 Selective VDRAs such as paricalcitol and doxercalciferol were developed to provide VDR activation with a lower risk of positive Ca and P balance.Citation52 In a 12-week, placebo-controlled, randomized study in patients receiving dialysis, paricalcitol effectively reduced PTH levels, with 6.7% of assessments indicative of hypercalcemia (serum calcium >10.5 mg/dL) versus 3.3% with placebo.Citation53 Doxercalciferol has also been shown to be effective in reducing PTH in hemodialysis patients, with a modest but clinically notable incidence of hypercalcemia in 15% of assessments during treatment,Citation54 while more recently a minimal increase in Ca and P levels was reported among patients receiving paricalcitolCitation55 VDRAs are largely used to treat SHPT in dialysis patients. Improved survival among ESRD patients receiving VDRA was inconsistently reported in observational studies.Citation56–Citation58 Similarly, observational data showed heterogeneous results about the superiority of paricalcitol against nonselective VDRA in improving survival.Citation59 Although selective VDRAs have been purported to limit calcitriol administration in CKD patients at higher cardiovascular risk,Citation60 it must be noted that the impact of different VDRA on hard end points has never been tested in head-to-head RCTs. Due to the widespread genomic effect elicited by VDR activation, vitamin D is receiving growing interest for other targets than SHPT such as proteinuria,Citation61,Citation62 left ventricular hypertrophy (LVH),Citation16,Citation63 and anemia.Citation64,Citation65 Thus, vitamin D represents a culprit of medical therapy for CKD-MBD. However, further studies are advocated to shed light on the many unresolved issues of this multifaceted therapy.Citation66
Table 2 Stages of chronic kidney disease
Parathyroidectomy
Advances in the pharmacological treatment of SHPT often obviate parathyroidectomy; however, some researchers have reported that parathyroidectomy may be more cost-effective than cinacalcet in some patients with ESRD and uncontrolled SHPT.Citation67 Successful parathyroidectomy can yield a dramatic reduction in PTH level and clinical symptoms.Citation68 Dialysis patients undergoing parathyroidectomy have an increased risk of cardiopulmonary complications and mortality compared to patients not on dialysis. The risks of parathyroidectomy in dialysis patients are likely similar to other commonly performed procedures for dialysis patients. However, a retrospective review of dialysis patients with severe and unresponsive SHPT indicated that parathyroidectomy did not improve cardiovascular outcomes compared with standard medical treatment.Citation69 In some instances, SHPT may continue after parathyroidectomy because of incomplete resection or because of ongoing PTH secretion from autotransplanted parathyroid tissue.Citation11
Current research goals
As of November 30, 2016, 207 studies evaluating sSHPT were reported on ClinicalTrials.gov; 137, 26, and 34 studies are completed, open, or active but not recruiting patients, respectively. Of these 32 are observational and 175 interventional (14 on phase 1, 32 on phase 2, 40 on phase 3, and 55 on phase 4; 34 not defined).Citation70,Citation71 The largest proportion of these trials were for agents that modulate the activity of the CaSR (65 trials related to cinacalcet and 15 trials related to the new peptide CaSR agonist etelcalcetide [AMG 416]) or activate the VDR (paricalcitol, 94 trials). These findings reflect current interest in therapies that target pathways known to be involved in the development and progression of SHPT74. Etelcalcetide (AMG 416) is a new long-acting peptide calcimimetic agent composed of a linear chain of seven amino acids.Citation72 It binds directly to CaSRs, inhibiting the production and the secretion of PTH by the parathyroid.Citation73 This activity is due to the formation of a disulfide bridge between D-cysteine of etelcalcetide molecule and L-cysteine of the CaSRs, resulting in a rapid activation of the receptors.Citation74
Several papers have been published in the last 2 years about pharmacological properties of etelcalcetide focusing on pharmacokinetics, biotransformation, and excretion of the drug in animal modelsCitation2 and in CKD patients on hemodialysis treatment.Citation75–Citation77
In rats model with intact kidneys after intravenous dose, the drug is rapidly distributed to the tissues, and the renal elimination is the major removal pathway, while in binephrectomized rats the nonrenal elimination is only 1.2%.Citation74 Etelcalcetide in whole blood is biotransformed by disulfide exchange to mainly form a covalent serum albumin peptide conjugate (SAPC). The biotransformation process in the human blood is reversible, but the rate of SAPC formation from etelcalcetide is faster than the inverse process. The preformation of SAPC also decreases the clearance rate during hemodialysis.Citation75 When etelcalcetide was administered intravenously to CKD patients on hemodialysis, the treatment itself was the predominant clearance and elimination route, with a 60% of the administered dose recovered in the dialysate.Citation72,Citation75 As a result of these observations, it was stated that etelcalcetide should be administered after the hemodialysis session to avoid elimination of a substantial fraction of the delivered dose.Citation78 The efficacy of etelcalcetide was tested in several studies comparing the new molecule with placebo or cinacalcet in CKD patients suffering from SHPT on dialysis. In 340 patients receiving etelcalcetide versus 343 treated with oral cinacalcet, etelcalcetide reduced PTH value 50% more than cinacalcet.Citation9,Citation79,Citation80 In another study, etelcalcetide administered thrice a week for as long as 26 weeks in 509 patients with moderate-to-severe SHPT, compared to 514 treated with placebo, resulted in a significantly greater reduction in PTH and FGF-23 values (70% versus 30% in placebo group), as well as an improvement in other markers of mineral metabolism.Citation81,Citation82 In a randomized double-blind placebo-controlled trial, patients, dived into three cohorts, received etelcalcetide 5 mg or placebo for 2 weeks (cohort 1), or etelcalcetide 5 mg or 10 mg or placebo for 4 weeks (cohorts 2 and 3). The mean percentage change from baseline PTH levels was −49% with etelcalcetide versus +29% with placebo in cohort 2 (etelcalcetide 10 mg), while in cohort 3 (etelcalcetide 5 mg) the percentage change was −33% versus +2%. Percentage of patients reaching a PTH value reduction of ≥30% was 76% in etelcalcetide 10 mg cohort versus 10% in placebo (P<0.0001). In the cohort with etelcalcetide 5 mg, the percentage was smaller (54% versus 15%). The number of patients achieving at the end of the study protocol a PTH value of ≤300 pg/mL were 67% and 46% in etelcalcetide arm 10 and 5 mg, respectively.Citation77,Citation83 According to findings from this trial, there was a dose-dependent reduction in PTH values and a corresponding effect on the bone formation (bone-specific alkaline phosphatase) and bone resorption (tartrate-resistant acid phosphatase 5b) markers.Citation84 The safety profile of etelcalcetide has been studied relative to a specific patient population (CKD patients on hemodialysis therapy) for whom the drug is intended. During phase 2 and phase 3 clinical studies, a total of 1,655 subjects received at least 1 dose of etelcalcetide, and 499 of them received etelcalcetide for over 1 year. The most common AE within the placebo-controlled studies was asymptomatic blood calcium reduction (63.8% etelcalcetide; 10.1% placebo).Citation76,Citation85,Citation86 A similar pattern was observed in the active-controlled study and consistent with the placebo-controlled studies. For the most frequently reported AEs, asymptomatic blood calcium reduction (68.9% etelcalcetide; 59.8% cinacalcet) was the most important adverse effect, while gastrointestinal symptoms were prevalent in cinacalcet-treated patients compared to etelcalcetide (). Based on the Kaplan–Meier estimate, the median of the first occurrence of hypocalcemic event was 9.6 weeks in the placebo-controlled study and 9.6 weeks in active controlled study in the arm of etelcalcetide.Citation87,Citation88
With regard to the incidence of serious AEs, these were less frequent (21.4%) in patients with a PTH value of >1,000 pg/mL at the screening compared with subjects with PTH >600 ≤1,000 pg/mL (26.2%) or <600 pg/mL (28.2%). A similar behavior has been observed with respect to age, with a lower incidence of events related to serum calcium reduction (56.5%) in subjects aged ≥65 years compared to <65 years (67.8%).Citation88 In the pooled placebo-controlled trials, a QT prolongation (500 ms) secondary to hypocalcemia was observed in 4.8% of etelcalcetide and 1.9% of placebo subjects. For this reason, close monitoring of calcium levels is necessary in patients with a previous risk factor such as congenital long QT syndrome, previous history of QT prolongation, family history of long QT syndrome, or sudden cardiac death and other conditions that predispose to QT prolongation.Citation88
Considering the overall safety profile of using etelcalcetide, we can see that the reported AEs are related to the mechanism of action of calcimimetic drugs and are somewhat similar to cinacalcet. The most important risk for etelcalcetide is hypocalcemia and other events that can occur secondary to reductions in serum calcium (ie, QTc prolongation, ventricular arrhythmia, convulsions, and worsening heart failure). These adverse effects, specially hypocalcemia and reduced calcium levels, occurred slightly more than with cinacalcet, possibly due to a more potent effect of etelcalcetide. However in dialysis patients, attending a dialysis unit thrice a week, regular monitoring of these parameters will be enough to prevent serious AEs. Despite bypassing the gastrointestinal tract, owing to intravenous administration, etelcalcetide only partially reduced gastrointestinal adverse effects (nausea and diarrhea) () seen with cinacalcet use, supporting evidence that these effects are possibly related to a systemic action rather than a local one, mediated by CaSRs activation.Citation89 Etelcalcetide intravenous administration at the end of the dialysis session, on the contrary, would ameliorate substantially the adherence to the SHPT treatment by the patients, also reducing the burden of pills of drug therapy. On the other hand, the superiority of etelcalcetide versus cinacalcet in reducing the levels of sPTH can offer a viable chance to demonstrate the role of PTH on the cardiovascular risk of patients on dialysis.Citation89,Citation90 The possibility of normalizing, with the new available drugs, mineral metabolism in uremic patients on dialysis may reduce bias related to the problem of therapeutic compliance in RCTs and help to clarify the effect of biochemical normalization on patients’ survival, even if it will be necessary to clearly identify the patients to whom this therapy should be offered, and this is also related to the economic capacity of health systems in the various countries.Citation91,Citation92 The EMA Assessment Report (Procedure No EMEA/H/C/003995/0000) related to “Parsabiv” (Amgen Inc, Thousand Oaks, CA, USA) (etelcalcetide), after careful benefit–risk assessment, argues that overall, the benefits of etelcalcetide in the treatment of secondary HPT in CKD patients are considered to outweigh the risks, recommending accurate controls of safety in the postmarketing period.Citation87
Table 3 Incidence (%) of most frequent adverse drug reactions
Scientific rationale
Vitamin D analogs, such as paricalcitol, selectively target the VDR, lowering PTH levels.Citation2 However, clinical data reveal that paricalcitol treatment can be associated with elevation in serum calcium and phosphorus, and a significant minority of patients treated with paricalcitol experience hypercalcemia.Citation16 Calcimimetics, such as cinacalcet, lower PTH levels and reduce serum calcium and phosphorus.Citation15,Citation21,Citation22,Citation30 However, cinacalcet is administered orally and has been associated with gastrointestinal AEs in approximately 30% of patients and with hypocalcemia in 7%.Citation21 In addition, poor adherence has been observed among dialysis patients self-administering oral cinacalcet.Citation93 Consequently, there has been interest in the development of novel CaSR agonists with improved tolerability and vitamin D derivatives with reduced calcemic actions to further advance the treatment of SHPT.
Conclusion
The pharmacological management of SHPT has progressed in recent years. The introduction of targeted therapies, such as selective VDR and CaSR modulators, offers an increased opportunity to adequately control elevated PTH, especially in patients with CKD receiving dialysis. Emerging therapies for SHPT, such as etelcalcetide (AMG 416) administered intravenously, may promote patient adherence, simplify treatment, and, in turn, improve the likelihood of achieving treatment goals. However, an open question remains as to whether emerging treatments for SHPT will reduce the risk of clinical end points such as cardiovascular morbidity and mortality. If emerging therapies for SHPT can reduce PTH, restore mineral homeostasis, promote adherence, and reduce the risk of troublesome side effects, they may provide the prerequisite features for improving long-term outcomes in patients with SHPT receiving dialysis.
Disclosure
Antonio Bellasi has received speaking honoraria or consultancy fees from Amgen, Sanofi, and Sanifit. The authors report no other conflicts of interest in this work.
References
- SalibaWEl-HaddadBSecondary hyperparathyroidism: pathophysiology and treatmentJ Am Board Fam Med20092257458119734404
- BrownAJSlatopolskyEDrug insight: vitamin D analogs in the treatment of secondary hyperparathyroidism in patients with chronic kidney diseaseNat Clin Pract Endocrinol Metab2007313414417237840
- JoyMSKaragiannisPCPeyerlFWOutcomes of secondary hyperparathyroidism in chronic kidney disease and the direct costs of treatmentJ Manag Care Pharm20071339741117605511
- McCannLMBetoJRoles of calcium-sensing receptor and vitamin D receptor in the pathophysiology of secondary hyperparathyroidismJ Ren Nutr20102014115020303786
- MoeSMDruekeTBManagement of secondary hyperparathyroidism: the importance and the challenge of controlling parathyroid hormone levels without elevating calcium, phosphorus, and calcium-phosphorus productAm J Nephrol20032336937914551461
- CozzolinoMUrena-TorresPVervloetMGIs chronic kidney disease-mineral bone disorder (CKD-MBD) really a syndrome?Nephrol Dial Transplant201429101815182024516228
- RiccardiDBrownEMPhysiology and pathophysiology of the calcium-sensing receptor in the kidneyAm J Physiol Renal Physiol2010298F485F49919923405
- GallieniMCozzolinoMFallabrinoGVitamin D: physiology and pathophysiologyInt J Artif Organs200932879419363780
- EvenepoelPRodriguezMKettelerMLaboratory abnormalities in CKD-MBD: markers, predictors, or mediators of disease?Semin Nephrol20143415116324780470
- WetmoreJBQuarlesLDTreatment of secondary hyperparathyroidism in kidney disease: what we know and do not know about use of calcimimetics and vitamin D analogsInt J Nephrol Renovasc Dis2008151721694914
- CunninghamJLocatelliFRodriguezMSecondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic optionsClin J Am Soc Nephrol2011691392121454719
- GoodmanWGQuarlesLDDevelopment and progression of secondary hyperparathyroidism in chronic kidney disease: lessons from molecular geneticsKidney Int20087427628817568787
- CozzolinoMCiceriPVolpiEMPathophysiology of calcium and phosphate metabolism impairment in chronic kidney diseaseBlood Purif20092733834419295196
- NakajimaKUminoKAzumaYStimulating parathyroid cell proliferation and PTH release with phosphate in organ cultures obtained from patients with primary and secondary hyperparathyroidism for a prolonged periodJ Bone Miner Metab20092722423319194773
- DruekeTBMassyZACirculating Klotho levels: clinical relevance and relationship with tissue Klotho expressionKidney Int201383131523271484
- MoeSMThadhaniRWhat have we learned about chronic kidney disease-mineral bone disorder from the EVOLVE and PRIMO trials?Curr Opin Nephrol Hypertens20132265165524100218
- RossiMCampbellKLJohnsonDWIndoxyl sulphate and p-cresyl sulphate: therapeutically modifiable nephrovascular toxinsOA Nephrology2013113
- YoungEWAlbertJMSatayathumSPredictors and consequences of altered mineral metabolism: the Dialysis Outcomes and Practice Patterns StudyKidney Int2005671179118715698460
- TentoriFBlayneyMJAlbertJMMortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: the Dialysis Outcomes and Practice Patterns Study (DOPPS)Am J Kidney Dis20085251953018514987
- FukagawaMKidoRKomabaHAbnormal mineral metabolism and mortality in hemodialysis patients with secondary hyperparathyroidism: evidence from marginal structural models used to adjust for time-dependent confoundingAm J Kidney Dis20146397998724119541
- StubbsJRWetmoreJBDoes it matter how parathyroid hormone levels are suppressed in secondary hyperparathyroidism?Semin Dial20112429830621682772
- KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD)Kidney Int Suppl2009113S1S130
- GalassiACupistiASantoroACozzolinoMPhosphate balance in ESRD: diet, dialysis and binders against the low evident masked poolJ Nephrol20152841542925245472
- SekerciogluNAngeliki VeronikiAThabaneLEffects of different phosphate lowering strategies in patients with CKD on laboratory outcomes: a systematic review and NMAPLoS One2017123e017102828248961
- CozzolinoMTomlinsonJWalshLBellasiAEmerging drugs for secondary hyperparathyroidismExpert Opin Emerg Drugs201520219720825702624
- CozzolinoMMazzaferroSBrandenburgVThe treatment of hyperphosphataemia in CKD: calcium-based or calcium-free phosphate binders?Nephrol Dial Transplant20112640240721079194
- AndersonJJKruszkaBDelaneyJACalcium intake from diet and supplements and the risk of coronary artery calcification and its progression among older adults: 10-year follow-up of the Multi-Ethnic Study of Atherosclerosis (MESA)J Am Heart Assoc20165e00381527729333
- PalmerSCGardnerSTonelliMPhosphate-binding agents in adults with CKD: a network meta-analysis of randomized trialsAm J Kidney Dis201668569170227461851
- di FilippoSCarfagnaFla MiliaVAssessment of intradialysis calcium mass balance by single pool variable-volume calcium kinetic modelHemodial Int Epub201725
- BlockGAMartinKJde FranciscoALCinacalcet for secondary hyperparathyroidism in patients receiving hemodialysisN Engl J Med20043501516152515071126
- BellasiACozzolinoMCinacalcet: the chemical parathyroidectomy?Clin Kidney J20136325325626064483
- FishbaneSShapiroWBCorryDBCinacalcet HCl and concurrent low-dose vitamin D improves treatment of secondary hyperparathyroidism in dialysis patients compared with vitamin D alone: the ACHIEVE study resultsClin J Am Soc Nephrol200831718172518945995
- MessaPMacarioFYaqoobMThe OPTIMA study: assessing a new cinacalcet (Sensipar/Mimpara) treatment algorithm for secondary hyperparathyroidismClin J Am Soc Nephrol20083364518178780
- Evolve Trial InvestigatorsEffect of cinacalcet on cardiovascular disease in patients undergoing dialysisN Engl J Med20123672482249423121374
- ParfreyPSChertowGMBlockGAThe clinical course of treated hyperparathyroidism among patients receiving hemodialysis and the effect of cinacalcet: the EVOLVE trialJ Clin Endocrinol Metab2013984834484424108314
- BellasiACozzolinoMAdragaoTPhosphate binders in moderate chronic kidney disease: where do we stand?J Nephrol201326993100023543481
- RaggiPChertowGMTorresPUThe ADVANCE study: a randomized study to evaluate the effects of cinacalcet plus low-dose vitamin D on vascular calcification in patients on hemodialysisNephrol Dial Transplant2011261327133921148030
- BellasiAReinerMPétavyFGoodmanWFloegeJRaggiPPresence of valvular calcification predicts the response to cinacalcet: data from the ADVANCE studyJ Heart Valve Dis201322339139924151766
- Ureña-TorresPAFloegeJHawleyCMProtocol adherence and the progression of cardiovascular calcification in the ADVANCE studyNephrol Dial Transplant201328114615223028103
- BellasiACozzolinoMRussoDMolonyDDi IorioBCinacalcet but not vitamin D use modulates the survival benefit associated with sevelamer in the INDEPENDENT studyClin Nephrol201686911312427443567
- GoldsmithDJCovicAFouqueDEndorsement of the Kidney Disease Improving Global Outcomes (KDIGO) Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guidelines: a European Renal Best Practice (ERBP) commentary statementNephrol Dial Transplant201025123823383120829401
- MorroneLFBolascoPCameriniCVitamin D in patients with chronic kidney disease: a position statement of the Working Group “Trace Elements and Mineral Metabolism” of the Italian Society of NephrologyJ Nephrol20162930532827062486
- NICEChronic kidney disease in adults: assessment and management clinical guideline Pub Available from: https://nice.org.uk/guidance/cg182Accessed July 23, 2014
- KDIGO 2012 Clinical practice guideline for the evaluation and management of chronic kidney diseaseKidney Int Suppl2013311150
- KandulaPDobreMScholdJDSchreiberMJJrMehrotraRNavaneethanSDVitamin D supplementation in chronic kidney disease: a systematic review and meta-analysis of observational studies and randomized controlled trialsClin J Am Soc Nephrol20116506220876671
- NigwekarSUBhanIThadhaniRErgocalciferol and cholecalciferol in CKDAm J Kidney Dis201260113915622560832
- TripkovicLLambertHHartKComparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysisAm J Clin Nutr20129561357136422552031
- WetmoreJBKimberCMahnkenJDStubbsJRCholecalciferolVErgocalciferol for 25-hydroxyvitamin D (25(OH)D) repletion in chronic kidney disease: a randomised clinical trialBr J Nutr2016116122074208128065190
- SpragueSMCrawfordPWMelnickJZUse of extended-release calcifediol to treat secondary hyperparathyroidism in stages 3 and 4 chronic kidney diseaseAm J Nephrol201644431632527676085
- PetkovichMMelnickJWhiteJTabashSStrugnellSBishopCWModified-release oral calcifediol corrects vitamin D insufficiency with minimal CYP24A1 upregulationJ Steroid Biochem Mol Biol201514828328925446887
- HamdyNAKanisJABenetonMNEffect of alfacalcidol on natural course of renal bone disease in mild to moderate renal failureBMJ199531069763583637677827
- BrownAJVitamin D analogs for secondary hyperparathyroidism: what does the future hold?J Steroid Biochem Mol Biol20071033–557858317368185
- MartinKJGonzálezEAGellensMHammLLAbboudHLindbergJ19-Nor-1-alpha-25-dihydroxyvitamin D2 (Paricalcitol) safely and effectively reduces the levels of intact parathyroid hormone in patients on hemodialysisJ Am Soc Nephrol199898142714329697664
- FrazaoJMChesneyRWCoburnJWIntermittent oral 1alpha-hydroxyvitamin D2 is effective and safe for the suppression of secondary hyperparathyroidism in haemodialysis patients. 1alphaD2 Study GroupNephrol Dial Transplant199813Suppl 368729568825
- CoyneDWGoldbergSFaberMGhosseinCSpragueSMA randomized multicenter trial of paricalcitol versus calcitriol for secondary hyperparathyroidism in stages 3–4 CKDClin J Am Soc Nephrol2014991620162624970869
- MessaPCozzolinoMBrancaccioDFARO Study GroupEffect of VDRA on survival in incident hemodialysis patients: results of the FARO-2 observational studyBMC Nephrol2015161125886515
- KovesdyCPKalantar-ZadehKVitamin D receptor activation and survival in chronic kidney diseaseKidney Int200873121355136318288097
- TentoriFAlbertJMYoungEWThe survival advantage for haemodialysis patients taking vitamin D is questioned: findings from the Dialysis Outcomes and Practice Patterns StudyNephrol Dial Transplant200924396397219028748
- TentoriFHuntWCStidleyCAMedical Directors of Dialysis Clinic IncMortality risk among hemodialysis patients receiving different vitamin D analogsKidney Int200670101858186517021609
- MazzaferroSGoldsmithDLarssonTEMassyZACozzolinoMVitamin D metabolites and/or analogs: which D for which patient?Curr Vasc Pharmacol201412233934923713876
- KimMJFrankelAHDonaldsonMOral cholecalciferol decreases albuminuria and urinary TGF-β1 in patients with type 2 diabetic nephropathy on established renin-angiotensin-aldosterone system inhibitionKidney Int201180885186021832985
- de BorstMHHajhosseinyRTamezHWengerJThadhaniRGoldsmithDJActive vitamin D treatment for reduction of residual proteinuria: a systematic reviewJ Am Soc Nephrol201324111863187123929770
- ThadhaniRAppelbaumEPritchettYVitamin D therapy and cardiac structure and function in patients with chronic kidney disease: the PRIMO randomized controlled trialJAMA2012307767468422337679
- BrancaccioDCozzolinoMGallieniMHyperparathyroidism and anemia in uremic subjects: a combined therapeutic approachJ Am Soc Nephrol200415Suppl 1S21S2414684666
- RiccioESabbatiniMBruzzeseDEffect of paricalcitol vs calcitriol on hemoglobin levels in chronic kidney disease patients: a randomized trialPLoS One2015103e011817425781618
- GalassiABellasiAAuricchioSPapagniSCozzolinoMWhich vitamin D in CKD-MBD? The time of burning questionsBiomed Res Int2013201386401223991423
- NarayanRPerkinsRMBerbanoEPParathyroidectomy versus cinacalcet hydrochloride-based medical therapy in the management of hyperparathyroidism in ESRD: a cost utility analysisAm J Kidney Dis20074980181317533023
- ConzoGPernaAFSavicaVImpact of parathyroidectomy on cardiovascular outcomes and survival in chronic hemodialysis patients with secondary hyperparathyroidism. A retrospective study of 50 cases prior to the calcimimetics eraBMC Surg201313Suppl 2S424268127
- Di IorioBMolonyDBellCINDEPENDENT Study InvestigatorsSevelamer versus calcium carbonate in incident hemodialysis patients: results of an open-label 24-month randomized clinical trialAm J Kidney Dis201362477177823684755
- ClinicalTrials.gov [homepage on the Internet]Secondary Hyperparathyroidism Available from: https://clinicaltrials.govAccessed November 30, 2016
- BoverJUreña-TorresPLloretMJIntegral pharmacological management of bone mineral disorders in chronic kidney disease (part II): from treatment of phosphate imbalance to control of PTH and prevention of progression of cardiovascular calcificationExpert Opin Pharmacother201617101363137327156578
- BlairHAEtelcalcetide: first global approvalDrugs201676181787179227900648
- MartinKJBellGPickthornKVelcalcetide (AMG 416), a novel peptide agonist of the calcium-sensing receptor, reduces serum parathyroid hormone and FGF23 levels in healthy male subjectsNephrol Dial Transplant20142938539224235081
- SubramanianRZhuXKerrSJNonclinical pharmacokinetics disposition, and drug-drug interaction potential of a novel d-amino acid peptide agonist of the calcium sensing receptor AMG 416 (Etelcalcetide)Drug Metab Dispos20164481319133126895981
- SubramanianRZhuXHockMBPharmacokinetics, biotransformation, and excretion of [14C]Etelcalcetide (AMG 416) following a single microtracer intravenous dose in patients with chronic kidney disease on hemodialysisClin Pharmacokinetics2017562179192
- MartinKJBlockGAChengSComparison of the Efficacy and Safety of Intravenous (IV) Etelcalcetide (AMG 416) and Oral Cinacalcet (CIN) in Patients on Hemodialysis (HD) with Secondary Hyperparathyroidism (sHPT)Abstract Poster presented at: Kidney WeekNovember 7; 2015San Diego, CA
- ChenPOlsson GisleskogPPerez-RuixoJJPopulation pharmacokinetics and pharmacodynamics of the calcimimetic Etelcalcetide in chronic kidney disease and secondary hyperparathyroidism receivingCPT Pharmacometrics Syst Pharmacol2016548449427639083
- EdsonKZWuBMIyerAGoodmanWSkilesGLSubramanianRDetermination of Etelcalcetide biotransformation and hemodialysis kinetics to guide the timing of its dosingKidney Int Rep201612433
- BlockGABushinskyDAChengSEffect of Etelcalcetide vs cinacalcet on serum parathyroid hormone in patients receiving hemodialysis with secondary hyperparathyroidism a randomized clinical trialJAMA2017317215616428097356
- FukagawaMYokoyamaKShigematsuTONO-5163 Study Group Efficacy and Safety of a Novel Intravenous CalcimimeticONO-5163 (ETELCALCETIDE) in Japanese hemodialysis patients with secondary hyperparathyroidism: results of a placebo controlled phase III studyNephrol Dial Transplant201631Suppl 1i454i471
- CunninghamJA long acting intravenous calcimimetic (AMG416) for secondary hyperparathyroidism (SHPT) in haemodialysed patientsPoster presented at: 52 nd ERA-EDTA Congress2015London, UK
- StollenwerkBBriggsADehmelBModelling Etelcalcetide effectiveness on health outcomes: relating biochemical outcomes to mortality, cardiovascular events, fractures and parathyroidectomyAbstract Poster presented at: 16th Biennial European Conference SMDMJune 12–24; 2016London, UK
- BellGHuangSOaksTMartinKJBlockGAA randomized, double-blind, phase 2 study evaluating the safety and efficacy of AMG 416 for the treatment of secondary hyperparathyroidism in hemodialysis patientsCurr Med Res Opin201531594395225786369
- YokoyamaKFukagawaMShigematsuTONO-5163 Study Group A novel Intravenous CalcimimeticsONO-5163 (ETELCALCETIDE): a multicenter single and multiple dose study in Japanese hemodialysis patients with secondary hyperparathyroidismNephrol Dial Transplant201631Suppl 1i454i471
- BlockGABushinskyDACunninghamJEffect of Etelcalcetide vs placebo on serum parathyroid hormone in patients receiving hemodialysis with secondary hyperparathyroidism two randomized clinical trialsJAMA2017317214615528097355
- BushinskyDABlockGAMartinKJTreatment of secondary hyperparathyroidism: results of a phase 2 trial evaluating an intravenous peptide agonist of the calcium-sensing receptorAm J Nephrol201542537938826684933
- BushinskyDABlockGAChengSOne year efficacy and safety of intravenous (IV) ETELCALCETIDE (AMG 416) in patients on hemodialysis (HD) with secondary hyperparathyroidism (SHPT)Abstract Poster presented at: 53rd ERA-EDTA CongressMay 21–24; 2016Vienna, Austria
- European Medicines Agency [homepage on the Internet]Parsabiv: summary of product characteristics Available from: http://www.ema.europa.euAccessed November 30, 2016
- MiddletonJPWolfMSecond chances to improve ESRD outcomes with a second-generation calcimimeticJAMA2017317213914128097342
- HaradaKETELCALCETIDE(ONO-5163, AMG 416), an intravenously available allosteric modulator of the calcium sensing receptor, effectively controls parathyroid hormone levels in a rat chronic renal insufficiency model with secondary hyperparathyroidismNephrol Dial Transplant201631Suppl 1i246i258
- StollenwerkBIannazzoSAkehurstRAssessing the cost-utility of Etelcalcetide: a Markov modelAbstract presented at: ISPOR 19th Annual European CongressOctober 31, 2016Vienna, Austria
- StollenwerkBIannazzoSCooperKBelozeroffVExploring the potential value of improved care for secondary hyperparathyroidism (SHPT) with a novel investigational calcimimetics therapyAbstract presented at: ISPOR 19th Annual European CongressOctober 31, 2016Vienna, Austria
- GinchermanYMoloneyKMcKeeCCoyneDWAssessment of adherence to cinacalcet by prescription refill rates in hemodialysis patientsHemodial Int201014687219732171