
Abstract
This study was conducted in a tertiary medical center in Kuala Lumpur, Malaysia. A total of 200 erectile dysfunction (ED) patients with 499 cases who had received pharmacological treatments for their ED participated in this study. Types, causes and factors associated with drug-related problems (DRPs) in ED patients with multiple comorbidities were assessed. A total of 244 DRPs with an average of 1.2±2.1 DRPs per patient were identified. Drug interaction contributed the most to DRPs occurrence. There was a significant higher risk of DRPs in patients with benign prostatic hyperplasia, lower urinary tract infection and elderly and end-stage renal disease. Early identification of types of DRPs and factors associated may enhance their prevention and management.
Background
Erectile dysfunction (ED), formerly known as impotence, is defined as “persistent inability to attain and maintain an erection sufficient to permit satisfactory sexual performance”.Citation1 It is a benign disorder that affects men, but the incidence increases with age as reported from 59 studies.Citation2 By 2025, 322 million men are predicted to have ED problems worldwide.Citation3 The high prevalence of ED has drawn much concern due to its profound impact on physical and psychosocial health and quality of life of sufferers and their partners.Citation4
Normal penile erection requires coordination between psychological, endocrine, vascular and neurological systems, and impairment or abnormalities of any of these can lead to ED. ED is classified into organic, psychogenic or mixed organic and psychogenic.Citation5 Organic ED is caused by vascular, neurological and hormonal disorders, whereas psychogenic ED is due to any psychological factors that can affect normal erectile function. Approximately 80% of ED cases are of organic origin with vascular disease among the most common causes of ED.Citation6
Treatments are available for certain types of ED, though only ED secondary to psychogenic causes, posttraumatic arteriogenic lesions and hormonal deficiency has shown evidence of being curable.Citation7 The first-line therapy that is widely used is oral phosphodiesterase-5 (PDE5) inhibitors. Second-line treatment includes intracavernous or transurethral prostaglandin E1 injection and vacuum erection device, whereas penile prosthesis and revascularization surgery are third-line therapies.Citation8 In addition to pharmacotherapy, lifestyle, risk factor modification, proper education and counseling to both patients and their partners play a crucial role in ED treatment.Citation9
Certain drug-related problems (DRPs), defined as events or circumstances involving drug therapy, may actually or potentially interfere with desired health outcomes.Citation10 Careful assessment of DRPs such as drug–drug interactions, dosing problems, drug choice or drug use problems and adverse reactions is essential to optimize treatment in ED patients with multiple comorbidities. This could also be significantly important in elderly with multiple comorbidities who are susceptible to polypharmacy.Citation11,Citation12
This study investigated the types, causes and factors associated with ED DRPs in ED patients with multiple comorbidities. The aim of our study was to provide baseline data regarding DRPs to allow implementation of more efficient management and to reduce the mortality and morbidity associated with DRPs.
Methodology
Study design and setting
This was an observational, retrospective study conducted in the University of Malaya Medical Centre (UMMC), a tertiary hospital in Malaysia with 1,200 beds.
Study population and sampling frame
Patients with ED who fulfilled the International Classification of Disease Tenth Revision (ICD 10) code F52.2 and Pharmacy Information System with a keyword sildenafil were included. The minimum sample size required was calculated using Epi Info Program version 7.0 (Centers for Disease Control and Prevention, Atlanta, GA, USA). The level of significance, α, was set as 0.05, and the desired power of the study (1−β) was 80%. The expected proportion of ED patients was based on the prevalence of 69.5% with a 5% confidence limit.Citation13 The minimum sample size calculated was 148 patients.
Study procedures
The study was performed in accordance with the Declaration of Helsinki, and the medical ethics committee of the UMMC (reference number: 201410-705) approved the study. The committee waived the need for written informed consent from participants. Patient records and information were anonymized and de-identified prior to analysis. A total of 266 registration numbers of patients from January 2000 to December 2014 with an ICD code of F52.2 were selected, and 232 patients’ medical folders were successfully retrieved from the Patient Medical Record office. Of these, 200 patients (499 cases) fulfilled the inclusion criteria (). We counted each prescription/admission/clinic visit as a single case.
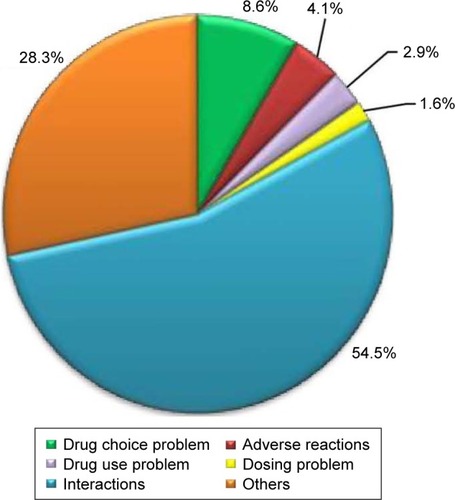
Figure 1 Drug-related problems (N=244).
Inclusion criteria
Diagnosed with any type of ED (organic, psychogenic or a combination of both) and had one or more comorbidities.
Aged 18 years and above (pharmacological treatments for ED are indicated for patients with a minimum age of 18).
Received pharmacological treatments, for instance, oral PDE-5 inhibitors (sildenafil, vardenafil, tadalafil), intracavernosal injection (aprostadil) or hormone replacement therapy (testosterone undecanoate and enanthate).
Exclusion criteria
Received non-pharmacological treatments, for instance, psychosexual therapy and physiotherapy, vacuum erection device, penile prosthesis and penile revascularization therapy.
Data collection
Demographic data such as age, ethnicity, body mass index (BMI) and smoking and alcohol consumption status were collected. Clinical information such as the year of ED diagnosis, chronic comorbidities and concurrent medications, severity of ED, presence and type of hypogonadism and causes of DRPs was also collected. defines terms used in this study.
Table 1 Definition of terms
Classification and assessment of DRPs
We used the Pharmaceutical Care Network Europe (PCNE) Classification for Drug Related Problems Version 5.01 (2006) as a tool to identify the types and causes of DRPs. There are six primary types of problems with 21 subtypes and six primary types of causes with 33 subtypes. The DRPs and their possible causes were identified from the patients’ medical records, with reference to the standard guidelines from established literature.Citation19–Citation23 The references were used to assess the appropriateness of drug indications, appropriateness of drug and dosage, possible drug interactions and adverse drug reactions and contraindications. The authors who are pharmacists were involved in the identification and classification of DRPs.
Statistical techniques
Statistical Package for Social Science version 21 (SPSS) (SPSS Inc., Chicago, IL, USA) was used to analyze all the collected and extracted data. Normality test (Shapiro–Wilk’s test) and visual inspection of the histogram, normal Q–Q plot and box plot were done to test the normality of continuous variables. The results were presented for skewness, kurtosis and standard error (SE). Normally distributed data were expressed as mean ± standard deviation. Nominal and ordinal categorical data were expressed as frequency or percentage (%). Binary logistic regression was used to determine the associations between categorical variables, and results were presented as odds ratio, 95% confidence interval level and P-value, where <0.05 indicated significance.
Results
A total of 499 cases and 200 male patients were included in this study. As shown in , the ethnicity of the majority was Chinese, followed by Malay and Indian. More than half of the patients were aged between 41 and 64 years and ranged from 31 to 91 years with a mean of 61.93±10.41 years. A Shapiro–Wilk’s test (P>0.05) and a visual inspection of the histogram, normal Q–Q plot and box plot showed approximately normally distributed population ages among the Chinese (skewness of −0.264 with SE =0.247, and kurtosis of −0.176 with SE =0.490), Malay (skewness of −0.146 with SE =0.287, and kurtosis of 0.283 with SE =0.566) and Indian (skewness of −0.719 with SE =0.398, and kurtosis of 0.503 with SE =0.778). For BMI, only 63.5% of the data were retrievable, which showed that most of these patients were pre-obese followed by obese.
Table 2 Demographic characteristics of study population (N=200)
Clinical characteristics
The retrievable data showed that most of the patients had ED problem for 5–10 years. The mean of the ED onset age was 54 years with the earliest onset at 25 years and the latest at 76 years. Of 110 patients with an available record, 80% had ED onset between the ages of 40 and 64 years. On average, each patient had 3.5±1.5 comorbidities with a range between 1 and 8. Seventy-six percent of patients had three or more comorbidities. Hypertension, hyperlipidemia and type 2 diabetes mellitus (T2DM) were the top three leading comorbidities, and the other comorbidities were found in only 5.0% of patients or fewer. These included gout, nephropathy, glaucoma, atrial fibrillation, chronic kidney disease, fatty liver disease, depression, stroke, hypothyroidism, congestive heart failure, spinal cord injury, tuberculosis, ankylosing spondylitis, chronic pulmonary disease, thyrotoxicosis, end-stage renal failure and prostate cancer. In addition, other comorbidities only occurred in one patient. The number of medications taken ranged from 2 to 14 with an average of 5.9±2.5 per patient. Polypharmacy was reported in 67.5% of the 200 participants and in 70.7% of the 82 elderly. describes the clinical characteristics of the study population.
Table 3 Clinical characteristics of study population (N=200)
Medications used in study population
ED medications
Sildenafil was the most common ED medication used, followed by vardenafil and tadalafil, both of which had a similar percentage of usage (). Sildenafil 50 mg, vardenafil 20 mg and tadalafil 20 mg were among the most commonly prescribed dosages compared to other dosing. The results also showed that alprostadil (0.2%), testosterone undecanoate (2.2%) and enanthate (1.8%) were less common. The records retrieved from 61% of the 200 patients showed that for most had “Stable medication and dose”, followed by “Change medication”, “Change medication dose” and “Change medication and dose” (). Seventy-five percent of 56 patients with stable medication and dosage were sildenafil users. Changing medication from sildenafil to tadalafil and vice versa had similar frequency (six out of 34 patients), and these changes occurred the most compared with the others.
Figure 2 Potential interactions (N=132).
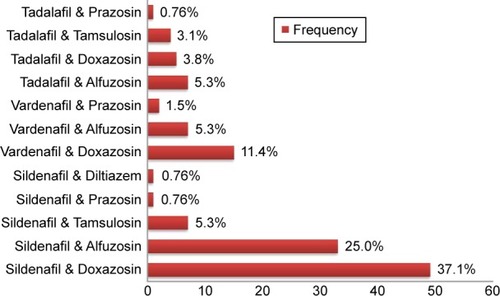
Table 4 Erectile dysfunction medications (N=499)
Concurrent medications
Lipid-lowering agents, hypoglycemic agents, antiplatelet medications, antihypertensive agents and benign prostatic hyperplasia (BPH) medications were the concurrent medications highly utilized by ED patients. Some took one or more concurrent medications due to multiple comorbidities.
Statins as lipid-lowering agents were the most frequently prescribed concurrent medication in nearly three-quarters of the 499 cases. Simvastatin 20 mg was the most commonly used statin in approximately 48% of 363 cases taking statins. Among hypoglycemic agents, biguanides were the most commonly used followed by sulfonylureas. Metformin 1,700/850 mg and gliclazide 120 mg M/R were the highly utilized hypoglycemic agents representing biguanide and sulfonylurea, respectively.
Monotherapy aspirin 100 mg was the most commonly used antiplatelet agent, which was prescribed in more than three-quarters of the 204 cases who took antiplatelets. Among antihypertensive agents, calcium channel blockers (CCBs) were most commonly used followed by angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs) and thiazide diuretics. Amlodipine, perindopril, losartan and hydrochlorothiazide were the most widely used agents representing each class, respectively. Approximately 41% of 191 cases prescribed with CCBs used amlodipine 10 mg, 33% of 164 cases prescribed with ACE inhibitors used perindopril 4 mg, 31% of 143 cases prescribed with ARBs used losartan 100 mg and more than half of 94 cases prescribed with thiazides used hydrochlorothiazide 25 mg.
Of the alpha-blockers, doxazosin 4 mg was the most widely used in approximately half of the 147 cases who took alpha-blockers. This was followed by alfuzosin 10 mg M/R (37.4%) and tamsulosin 400 μg (5.4%).
Drug-related problems
A total number of 244 DRPs were identified in 200 patients. On average, each patient had 1.2±2.1 DRPs with 1.2±2.1 causes for the problems. The number of DRPs in each patient ranged from 0 to 11, and 46.5% of the patients had at least one DRP. Under the six main types of problems, “Interactions” had the highest incidence followed by “Others”, “Drug choice problems”, “Adverse reactions”, “Drug use problems” and “Dosing problems”.
Adverse reactions
Ten cases of adverse reactions were identified and were mainly classified under the subtype “Side effect suffered (nonallergic)” (). All the nonallergic side effects reported were related to the use of PDE-5 inhibitors. Among the 320 sildenafil prescriptions, three cases (two cases of 100 mg and one case of 50 mg) had reported side effects such as palpitation, flushing over face, blocked nose and headache. Of the 93 vardenafil prescriptions, side effects were reported in six cases (four cases of 20 mg, one case of 10 mg and one with unknown dosage), which included occasional and minimal flushing of face, headache, gastritis, weakness, palpitation, nausea and giddiness. One case of urine incontinence had been reported with the use of tadalafil 10 mg from 80 prescriptions.
Table 5 Adverse reactions (N=244)
Drug choice problems
“Contraindication for drug” and “Inappropriate duplication of therapeutic group or active ingredient” were the two main drug choice problems (). The 20 cases identified as “Contraindication for drug” involved the concurrent use of PDE-5 inhibitors with isosorbide dinitrate (60%) and glyceryl trinitrate (15%), and the use of PDE-5 inhibitors in the presence of uncontrolled hypertension (20%) and recent stroke (5%). The percentage of cases in which nitrates were co-prescribed with sildenafil, vardenafil and tadalafil was 4.1% (n=320), 1.07% (n=93) and 1.25% (n=80), respectively. The single case of inappropriate duplication of therapeutic group involved the combined use of sildenafil 50 mg and tadalafil 20 mg.
Table 6 Drug choice problems (N=244)
Dosing problems
Four dosing problems under the subtype “Drug dose too high or dosage regime too frequent” were identified (). Two of the four cases involved the use of a high initial dose of PDE-5 inhibitors. In one, sildenafil 50 mg was used instead of 25 mg as the initial dose for the patient on stable alpha-blocker, and the other had used sildenafil 100 mg as the starting dose. In the other two cases, sildenafil 200 mg and vardenafil 40 mg exceeded the maximum daily dose that had been used.
Table 7 Dosing problems (N=244)
Drug use problems
Of 244 cases, only 2.9% had been detected as drug use problems. All the identified cases were under the subtype “Drug not taken/administered at all”. Among the seven cases identified, six involved sildenafil, and one involved tadalafil ().
Table 8 Drug use problems (N=244)
Interactions
“Interactions” was the most common DRP. The subtype “Potential interaction” comprised nearly 99% of the cases with only one case of “Manifested interaction” (). Potential interactions were detected between PDE-5 inhibitors with alpha-blockers (doxazosin, alfuzosin, tamsulosin, prazocin) and a CCB (diltiazem). As shown in , the highest frequency of potential interaction was found between sildenafil and doxazosin (36.6%). In addition, the “Manifested interaction” occurred between sildenafil and doxazosin.
Table 9 Drug interactions (N=244)
Others
Approximately one-quarter (28.3%) of cases were classified under “Others” with the main problem as “Dissatisfaction with therapy despite taking drug(s) correctly” (). Among the 69 cases, 33.4% were identified as dissatisfaction with sildenafil 50 mg, 23.3% with tadalafil 20 mg, 21.7% with sildenafil 100 mg and 8.7% with vardenafil 20 mg. Other minor complaints included therapy dissatisfaction towards testosterone enanthate, alprostadil, sildenafil 25 mg, tadalafil 5 mg, tadalafil 10 mg and vardenafil 10 mg.
Table 10 Other problems (N=244)
Causes of DRPs
We identified 244 causes of DRPs. “Drug use process” was the most common cause, which comprised more than half of all causes. This was followed by “Others” (29.5%), “Drug/dose selection” (13.5%) and “Patient/psychological” (1.6%). The three most common subtypes of the causes included “Inappropriate timing of administration and/or dosing interval” of the type “Drug use process”, “No obvious cause” of the type “Others” and “Inappropriate drug selection” of the type “Drug/dose selection” ().
Table 11 Causes of drug-related problems (N=244)
Factors associated with DRPs
Patients with BPH, lower urinary tract symptoms (LUTS) and end-stage renal disease (ESRD) or elderly were significantly at higher risk of acquired DRPs () and drug interactions (). In addition, LUTS, ESRD and elderly were also significantly associated with higher incidence of “Other” problems (). “Drug choice problems” was significantly more likely to occur in patients with ischemic heart disease (). However, T2DM patients were at lower risk of having DRPs (P=0.011) and drug interactions (P=0.024) compared with those without T2DM. Patients with hypertension were significantly at lower risk of having “Drug use problems” () and “Other” problems (). Polypharmacy was another factor significantly associated with lower risk of “Other” problems. For adverse reactions () and dosing problems (), we found no significantly associated factor.
Table 12 Factors associated with the occurrence of drug-related problems
Table 13 Factors associated with the occurrence of drug use problems
Table 14 Factors associated with the occurrence of drug interactions
Table 15 Factors associated with the occurrence of drug choice problems
Table 16 Factors associated with the occurrence of dosing problems
Table 17 Factors associated with the occurrence of other problems
Table 18 Factors associated with the occurrence of adverse reactions
Discussion
Of the 110 patients with available records, the majority had onset of ED within the age range of 40–64 years. Although other studies have reported that ED affects nearly half of men aged over 40, its actual onset time is unknown.Citation24 Therefore, we suggest future studies exploring both the timing of ED onset and whether it precedes or follows the associated comorbidities and the relationships between different comorbidities and ED onset must be conducted.
Hypertension, hyperlipidemia and T2DM were the three prevalent comorbidities found in the study population. Vascular abnormality is a common risk factor shared between these three comorbidities and ED.Citation25 The strong association between ED and hypertension, hyperlipidemia and diabetes found in other studies also supports this result.Citation26–Citation28 However, the prevalence rates of these three comorbidities were found to be higher than the study performed by Seftel et al on a large ED population (272,325 patients) in which hypertension was seen in 41.6%, hyperlipidemia in 42.2% and diabetes mellitus in 20.2%.Citation29 The small sample size used in our study is the most reasonable explanation for the higher percentage of disease occurrences.
We found that 16.5% of 200 ED patients had LUTS, which is similar to the finding of a recent study by Zaman Huri et al that showed 11% of 219 ED patients had LUTS.Citation30 Other studies have found that LUTS is an independent risk factor for ED regardless of age and comorbidities.Citation31
We observed polypharmacy in 67.5% of 200 patients, and 70.7% of the 82 elderly had polypharmacy. The presence of multiple diseases inevitably leads to the occurrence of polypharmacy, which is commonly observed in the elderly.Citation32 A retrospective cohort study conducted in Italy, which defined polypharmacy as five or more medications, found a prevalence of 39.4% polypharmacy among 887,165 elderly in outpatient settings.Citation33 However, in our study, the prevalence of polypharmacy in elderly was misleadingly higher due to the small number of elderly.
Drug-related problems
This is the first study to investigate DRPs in ED patients with multiple comorbidities. We found that almost half of the patients had at least one DRP with “Interactions” and “Others” being the most commonly identified. A study of DRPs in T2DM patients with hypertension found 90.5% of 200 patients had at least one DRP with an average of 1.9±1.2 problems per patient.Citation34 Another study investigated DRPs in T2DM patients with hyperlipidemia and found 91.8% of 208 patients had at least one DRP with an average of 1.94±1.10 problems per patient.Citation35 Since DRPs in our study were only identified from the perspective of ED, higher incidences of DRPs are expected when DRP detection involves a wider perspective of different comorbidities. We suggest future studies are needed to detect DRPs from all the different disease perspectives to provide an overview of DRPs.
Adverse reactions
The incidence of adverse reactions in our study only contributed to a small percentage of DRPs. All the cases of adverse reactions classified as subtype “Side effect suffered (nonallergic)” were related to the use of PDE-5 inhibitors. Despite the possibility of underreported adverse reactions in patients who were able to tolerate the side effects, this result indicated that only a minority of patients were not able to tolerate the side effects of PDE-5 inhibitors. However, a recent study found that the most common reason given by 70–79-year-old patients who discontinued the use of PDE-5 inhibitors was “Concern about the side effect of medications” because of their poor health condition and other comorbidities.Citation36 Therefore, adverse reactions are still a major concern in elderly ED patients taking PDE-5 inhibitors.
Drug choice problems
We identified 20 (8.2%) contraindications and one (0.4%) case of inappropriate duplication of medication that were identified as drug choice problems. The percentage of nitrates co-prescribed with sildenafil, vardenafil and tadalafil was 4.1% (n=320), 1.07% (n=93) and 1.25% (n =80), respectively. This result was similar to the finding of Chang et al study that showed the co-prescribed percentages of 1.07%, 0.83% and 1.07% for sildenafil, vardenafil and tadalafil, respectively.Citation37 Despite the overall result showing low incidence of contraindication, the need to double-check the intake of concomitant drugs is crucial for preventing severe hypotension.Citation38
There were four cases of concomitant use of PDE-5 inhibitors in patients with uncontrolled hypertension (>170/110). Although low incidences were detected, caution still needs to be taken because the safety of PDE-5 inhibitors has not yet been established.Citation39–Citation41 Despite a recent study that explored the use of sildenafil in stroke recovery, the concomitant use of PDE-5 inhibitors in recent stroke is still not encouraged within 6 months following an acute stroke due to the lack of clinical data.Citation42
In our study, an inappropriate duplication of medications involved a single case of co-prescribed sildenafil 50 mg and tadalafil 20 mg. However, no study has been done on the safety and efficacy of this combination, though recently a study of the use of long-term tadalafil 5 mg daily with sildenafil 50 mg added for the first few weeks showed better ED improvement without any increased adverse events than using only tadalafil.Citation43 However, further studies are required to provide more evidence-based data.
Dosing problems
We detected two cases of inappropriate initial dose of sildenafil. One case involved the use of sildenafil 50 mg as the initial dose for a patient on stable alpha-blocker, and the other involved sildenafil 100 mg as the starting dose for a patient with naive treatment. A low initial dose of PDE-5 inhibitors has been suggested for patients on stable alpha-blockers to minimize the risk of orthostatic hypotension.Citation38,Citation44 Despite recent studies that suggest the use of 100 mg sildenafil as a starting dose due to several advantages such as reducing the need for titration and preventing discouragement and treatment abandonment, this starting dose in patients with naive treatment was still considered as a high initial dose in our study because of the recommended dose in the product insert.Citation39,Citation45,Citation46 Although the result showed low incidence of inappropriate initial dosing, there might have been underestimation of incidence since not all cases were observed from the beginning.
In addition, the use of 200 mg sildenafil and 40 mg vardenafil that exceeded the maximum daily dose was identified. For sildenafil, a study by McMahon showed that 24.1% of patients who did not respond previously to a maximum dose of 100 mg responded to a higher dose of 150 mg and 200 mg; however, the usage was limited due to the high occurrence of side effects and a high rate of discontinuation.Citation47 For vardenafil, studies have found no significant difference between the efficacies of 20 mg and 40 mg, but there were slightly more side effects observed in those who took vardenafil 40 mg compared with the placebo.Citation48,Citation49 Therefore, patients with a poor response were not encouraged to exceed the maximum dose, although they were currently using a maximum dose. Instead, other strategies such as patient education, improvement of comorbidities, normalization of testosterone level, switching PDE-5 inhibitors, daily or continuous use of PDE-5 inhibitors and psychosexual counseling could be tried for patients who are not keen on other ED treatments.Citation50
Drug use problems
A minority of cases were identified as drug use problems when patients did not take the ED medications prescribed by the physician. Despite ED not being a life-threatening condition, studies have found that it can be a contributor to nonadherence to other long-term treatment for concurrent comorbidities if left untreated.Citation51 Psychological problems related to self-confidence, emotional states and the fear of medication adverse events were found to be the most common factor affecting the use of PDE-5 inhibitors.Citation52 Other affecting factors included medication-related factors (cost, drug efficacy and side effects), relational factors (relationship with partner) and circumstance factors (nonscheduled medication intake and trying natural products).Citation52 Therefore, the reason why a drug is not taken should be taken into consideration before further action.
Interactions
Potential interactions between PDE-5 inhibitors and alpha-blockers, primarily doxazosin, alfuzosin, tamsulosin and prazocin, were the most common DRPs in our study. One such interaction was between sildenafil and doxazosin, which could be explained by the significant association between BPH/LUTS and ED.Citation30 Despite coadministration of alpha-blockers and PDE-5 inhibitors that possess the risk of hypotension, a recent systematic review had found that a combination of both agents in treating BPH/LUTS and ED was beneficial.Citation53 Nevertheless, PDE-5 inhibitors still need to be used with caution in combination with alpha-blockers. Apart from that, potential interactions between diltiazem and sildenafil had also been detected. Caution needs to be taken when diltiazem, sildenafil and nitrate are used concomitantly as a study has reported that diltiazem-mediated inhibition of sildenafil metabolism may promote nitrate-induced hypotension.Citation54
Others
The second most common DRP in our study was “Others” with all the cases identified under the subtype “Dissatisfaction with therapy despite taking drug(s) correctly”. The most common complaint from patients was dissatisfaction with the use of sildenafil 50 mg, followed by tadalafil 20 mg, sildenafil 100 mg and vardenafil 20 mg. The main reasons for the dissatisfaction were ineffectiveness of the medications. A recent study that assessed patients’ satisfaction using a questionnaire had showed a high satisfaction rate (95.5%) in users of PDE-5 inhibitors.Citation55 In our study, the percentage of dissatisfaction might have been overestimated as therapeutic dissatisfaction of patients was judged on patients’ feedback that was recorded on the medical notes without any rating. In addition, we had assumed that patients took the medication correctly.
Causes of DRPs
Among a total of 244 causes, “Drug use process” was the most common cause of DRPs followed by “Others”, “Drug/dose selection” and “Patient/psychological”. Of the subtype “Drug use process”, inappropriate timing of administration was the cause assigned for the potential interaction between PDE-5 inhibitors and alpha-blockers. Despite different doses, different timing and different types of combination with possible different degrees of interaction, the timing of administration between the PDE-5 inhibitors and alpha-blockers remained a concern.Citation56 However, this result might be overestimated since patients might be warned of an appropriate timing of medication, which was not recorded in the medical note.
“No obvious cause” had been used to explain most of the cases of therapeutic dissatisfaction with unknown causes. This was necessary because of the limitation in obtaining the real causes of dissatisfaction, which was not recorded. “Other cause” explained other reasons for DRPs; for instance, spinal cord injury (SCI) might be the cause of therapeutic dissatisfaction. Patients with a low level of SCI lesion might have a poor response to PDE-5 inhibitors due to poor or impaired penile innervation.Citation57 There were also some causes that were beyond the control of health care professionals. For instance, one patient with stroke within 6 months insisted on taking a PDE-5 inhibitor at his own risk, and another patient refused to take the prescribed ED drug to work on his confidence first.
For “Drug/dose selection”, this involved inappropriate drug selection where PDE-5 inhibitors should not be given to patients who concurrently were prescribed another form of nitrate. A well-established screening process can minimize this problem. Apart from that, although “Patient/psychological” only comprised minor causes, proper counseling can be given for patients who are concerned about the drugs or the side effects, whereas a financial problem might need to be personally solved by the patient.
Factors associated with DRPs
Benign prostatic hyperplasia/lower urinary tract symptoms
We found that BPH and LUTS have a significant positive association with the occurrence of DRPs. This might be due to the relationship between ED, BPH and LUTS. ED and BPH are apparently linked together with a similar age and gender distribution, whereas BPH is the primary cause of LUTS.Citation58,Citation59 A recent study also proposed the co-diagnosis of LUTS and ED following preclinical evidence that had found several common pathophysiological mechanisms in them.Citation30
Incidences of drug interactions were also significantly higher in patients with BPH and LUTS. The concurrent use of PDE-5 inhibitors for ED and alpha-blockers for BPH/LUTS had contributed to this. Despite recent studies and clinical trials that had found the efficacy of the combined use of alpha-blockers and PDE-5 inhibitors for both ED and BPH/LUTS, the potential interaction between them should also be considered.Citation53,Citation60 LUTS alone were also significantly associated with higher incidence of “Other” problems, which represent patients’ dissatisfaction with therapy. The negative effect on quality of sexual life by LUTS might explain their contribution towards therapeutic dissatisfaction.Citation31
Elderly
Elderly was significantly associated with higher occurrence of DRPs, drug interactions and “Others” problems. The presence of multiple comorbidities in ED patients might explain this association.Citation11 Elderly patients were more susceptible and vulnerable to drug interaction and therapeutic dissatisfaction which might be due to age-related changes, for instance, changes in physiological, biological, physical and social functions.Citation61
End-stage renal disease
We also found that ESRD was significantly associated with higher occurrence of DRPs. The complexity of medication management in ESRD patients can cause the occurrence of DRPs in them.Citation62 In addition, the result of our study also showed that the occurrence of drug interaction was higher in ESRD patients compared with non-ESRD patients. Although the study by Rama et al had found a high occurrence of drug interaction in patients with ESRD, the interactions were not the result of ED medication.Citation63 Therefore, further studies are required to validate this relationship. Furthermore, “Other” problems that represent patients’ dissatisfaction with therapy were also significantly associated with ESRD. ESRD itself can cause ED because of the imbalance of hormone production through the hypothalamic–pituitary–gonadal axis and which accelerates the atherosclerosis process.Citation64 The dissatisfaction of therapy might be due to the ESRD. However, one study has shown that most of the ESRD patients improved in penile erection with the use of PDE-5 inhibitors.Citation65 Therefore, further studies are needed.
Type 2 diabetes mellitus
We found that T2DM has a negative association with DRPs and drug interactions. However, T2DM was commonly accompanied by other comorbidities that lead to management complexity.Citation66 A recent study showed that at least one DRP had occurred in 91.8% of T2DM patients with hyperlipi-demia, while another study found 90.5% of T2DM patients with hypertension had at least one DRP.Citation34,Citation35 The inconsistent result in our study might be due to DRPs being observed from different disease perspectives.
Ischemic heart disease
The contraindication of nitrate with PDE-5 inhibitors might be the link of significant association between ischemic heart disease and drug choice problems. Although PDE-5 inhibitors are contraindicated in patients who take any form of nitrates, for patients who develop ischemic heart disease after ED, nitrates are suggested not be taken within 24 hours of a sildenafil or vardenafil dose, and 48 hours of a tadalafil dose. In the case of emergency chest pain, non-nitrate-containing agents such as CCB or a beta blocker should substitute the use of nitrate.Citation39–Citation41,Citation67,Citation68
Hypertension
Patients with hypertension were significantly less likely to have therapeutic dissatisfaction. This indicates higher therapeutic satisfaction in hypertensive patients compared with patients without hypertension. Nonadherence and treatment discontinuation of antihypertensive agents were common DRPs found in hypertensive patients due to ED development after using certain antihypertensive medications (especially thiazide and beta-blockers). However, improvement in adherence to antihypertensive agents was observed when a PDE-5 inhibitor was given for ED.Citation51,Citation68,Citation69 This suggests that proper management of both hypertension and ED might produce a better response towards therapy.
Polypharmacy
Drug use problems as indicated by “Drug not taken/administered at all” were found to be significantly less likely to occur in patients with polypharmacy. Generally, polypharmacy was associated with higher risk of DRPs.Citation32 Increased prescribed medications will generally lead to medication nonadherence.Citation70 The only hypothesis that can be made from our study was that ED patients with polypharmacy might indicate the presence of multiple comorbidities. This might lead to more severe ED and the need to urge patients to adhere to ED medications. Further study is required to explore this relationship.
Conclusion
DRPs occurred in almost half of the total cases identified. “Drug interaction” and “Others” were the most common DRPs identified. Factors such as BPH, LUTS, ESRD and elderly were found to be significantly associated with the occurrence of DRPs. Therefore, early identification of the types and patterns of DRPs and the factors associated may enhance the prevention and management of DRPs in ED patients with multiple comorbidities.
Limitation of the study
The retrospective nature of the study can lead to risk of bias because it was highly dependent on patients’ clinical records as the only data source which is a limitation to the study.
Acknowledgments
The authors would like to thank the University of Malaya, Malaysia (RP024A-14HTM) and the University Malaya High Impact Research Grant (HIR/MOHE/MED/35 to AHAR) for financial and technical support.
Disclosure
The authors declare that they have no competing interests in this work.
References
- NIH Consensus Conference. Impotence. NIH Consensus Development Panel on ImpotenceJAMA1993270183908510302
- LewisRWFugl-MeyerKSCoronaGDefinitions/epidemiology/risk factors for sexual dysfunctionJ Sex Med201074 Pt 21598160720388160
- AytaIAMcKinlayJBKraneRJThe likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequencesBJU Int1999841505610444124
- RosenRCFisherWAEardleyINiederbergerCNadelASandMMen’s Attitudes to Life Events and Sexuality (MALES) StudyThe multinational Men’s Attitudes to Life Events and Sexuality (MALES) study: I. Prevalence of erectile dysfunction and related health concerns in the general populationCurr Med Res Opin200420560761715171225
- ChaoJKHwangTISContemporary management of erectile dysfunctionUrol Sci20132423540
- ChiurliaED’AmicoRRattiCGranataARRomagnoliRModenaMGSubclinical coronary artery atherosclerosis in patients with erectile dysfunctionJ Am Coll Cardiol20054681503150616226175
- WespesEErectile dysfunction: the medical treatmentEur Urol Suppl20131221317
- HatzimouratidisKAmarEEardleyIEuropean Association of UrologyGuidelines on male sexual dysfunction: erectile dysfunction and premature ejaculationEur Urol201057580481420189712
- WespesEEardleyIGiulianoFGuidelines on male sexual dysfunction: erectile dysfunction and premature ejaculationEuropean Association of Urology2014 Available from: https://uroweb.org/wp-content/uploads/14-Male-Sexual-Dysfunction_LR.pdfAccessed April 12, 2015
- Pharmaceutical Care Network Europe FoundationPCNE Classification for Drug Related Problems Version 5.012010
- GareriPCastagnaAFrancomanoDCerminaraGDe FazioPErectile dysfunction in the elderly: an old widespread issue with novel treatment perspectivesInt J Endocrinol20142014115
- WootenJGalavisJPolypharmacy. Keeping the elderly safeRN20056884450
- Ab RahmanAAAl-SadatNYun LowWPrevalence of erectile dysfunction in primary care setting, MalaysiaJ Mens Health20118Suppl 1S50S53
- ValderasJMStarfieldBSibbaldBSalisburyCRolandMDefining comorbidity: implications for understanding health and health servicesAnn Fam Med200974354363
- World Health Organization (WHO)Proposed working definition of an older person in Africa for the MDS Project2013 Available from: http://www.who.int/healthinfo/survey/ageingdefnolder/en/Accessed May 20, 2015
- ZainudinSDaudZMohamadMTong BoonATWan MohamedWMIA summary of the Malaysian clinical practice guidelines on management of obesityJ ASEAN Fed Endocr Soc2011262
- ViktilKKBlixHSMogerTAReikvamAPolypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problemsBr J Clin Pharmacol200763218719516939529
- VenesDTaber’s Cyclopedic Medical DictionaryPhiladelphia USAF.A. Davis Company2013
- LacyCFArmstrongLLGoldmanMPLanceLLDrug Information Handbook20th edHudson, OHLexi-Comp Inc.2011
- MIMS Malaysia128th edUBM Medica Pacific Ltd2012
- MedscapeAlprostadil intracavernous/urethral (Rx) Available from: http://reference.medscape.com/drug/caverject-edex-alprostadil-342846Accessed April 27, 2015
- KlonerRANew drugs and technologies: cardiovascular effects of the 3 phosphodiesterase-5 inhibitors approved for the treatment of erectile dysfunctionCirculation20041103149315515533876
- Straight HealthcareCytochrome 450 3A Available from: http://www.straighthealthcare.com/cytochrome-p450-3a4.html#howAccessed April 27, 2015
- NehraAKulaksizogluHGlobal perspectives and controversies in the epidemiology of male erectile dysfunctionCurr Opin Urol200212649349612409879
- GandagliaGBrigantiAJacksonGA systematic review of the association between erectile dysfunction and cardiovascular diseaseEur Urol201465596897824011423
- ViragRBouillyPFrydmanDIs impotence an arterial disorder? A study of arterial risk factors in 440 impotent menLancet1985184221811842857264
- JavaroniVNevesMFErectile dysfunction and hypertension: impact on cardiovascular risk and treatmentInt J Hypertens2012201262727822649713
- NunesKPLabaziHWebbRCNew insights into hypertension-associated erectile dysfunctionCurr Opin Nephrol Hypertens201221216317022240443
- SeftelADSunPSwindleRThe prevalence of hypertension, hyperlipidemia, diabetes mellitus and depression in men with erectile dysfunctionJ Urol20041716 Pt 12341234515126817
- Zaman HuriHLian ChooTSulaimanCZMarkRAbdul RazackAHOral drug treatments in patients with erectile dysfunction and multiple comorbidities: a retrospective observational studyBMJ Open201447e005381
- KirbyMCreangaDLStecherVJErectile function, erection hardness and tolerability in men treated with sildenafil 100 mg vs. 50 mg for erectile dysfunctionInt J Clin Pract201367101034103924073975
- NobiliAGarattiniSMannucciPMMultiple diseases and polyphar-macy in the elderly: challenges for the internist of the third millenniumJOC2011112844
- SlabaughSLMaioVTemplinMAbouzaidSPrevalence and risk of polypharmacy among the elderly in an outpatient setting: a retrospective cohort study in the Emilia-Romagna region, ItalyDrugs Aging201027121019102821087071
- Zaman HuriHFun WeeHDrug related problems in type 2 diabetes patients with hypertension: a cross-sectional retrospective studyBMC Endocr Disord201313223289895
- Zaman HuriHChai LingLDrug-related problems in type 2 diabetes mellitus patients with dyslipidemiaBMC Pub Health201313119224341672
- KimS-CLeeY-SSeoK-KJungG-WKimT-HReasons and predictive factors for discontinuation of PDE-5 inhibitors despite successful intercourse in erectile dysfunction patientsInt J Impot Res2014263879324305610
- ChangLLMaMAllmenHVHendersonSCHarperKHornbuckleKCo-possession of phosphodiesterase type-5 inhibitors (PDE5-I) with nitratesCurr Med Res Opin20102661451145920394470
- SchwartzBGKlonerRADrug interactions with phosphodiesterase-5 inhibitors used for the treatment of erectile dysfunction or pulmonary hypertensionCirculation20101221889520606131
- Viagra® (sildenafil) [prescribing information]Pfizer2010
- Levitra® (vardenafil) [prescribing information]Wayne, NJBayer Healthcare/GlaxoSmithKline2011
- Cialis® (tadalafil) [prescribing information]Indianapolis, INEli Lilly2011
- SandnerPHutterJTinelHZiegelbauerKBischoffEPDE5 inhibitors beyond erectile dysfunctionInt J Impot Res200719653354317625575
- CuiHLiuBSongZEfficacy and safety of long-term tadalafil 5 mg once daily combined with sildenafil 50 mg as needed at the early stage of treatment for patients with erectile dysfunctionAndrologia2015471202424387078
- KlonerRASadovskyRJohnsonEGMoDAhujaSEfficacy of tadalafil in the treatment of erectile dysfunction in hypertensive men on concomitant thiazide diuretic therapyInt J Impot Res200517545045416015377
- StröbergPKaminetskyJCParkNCGoldfischerERCreangaDLStecherVJHardness, function, emotional well-being, satisfaction and the overall sexual experience in men using 100-mg fixed-dose or flexible-dose sildenafil citrateInt J Impot Res201022428428920596083
- KirbyMChappleCJacksonGErectile dysfunction and lower urinary tract symptoms: a consensus on the importance of co-diagnosisInt J Clin Pract201367760661823617950
- McMahonCGHigh dose sildenafil citrate as a salvage therapy for severe erectile dysfunctionInt J Impot Res200214653353812494291
- StarkSSachseRLiedlTVardenafil increases penile rigidity and tumescence in men with erectile dysfunction after a single oral doseEur Urol2001402181188 discussion 181–19011528196
- CroweSMStreetmanDSVardenafil treatment for erectile dysfunctionAnn Pharmacother2004381778514742800
- ParkNCKimTNParkHJTreatment strategy for non-responders to PDE5 inhibitorsWorld J Mens Health2013311313523658863
- ScrantonREGoldsteinIStecherVJErectile dysfunction diagnosis and treatment as a means to improve medication adherence and optimize comorbidity managementJ Sex Med201310255156123153075
- CarvalheiraAForjazVPereiraNMAdherence to phosphodiesterase type 5 inhibitors in the treatment of erectile dysfunction in long-term users: how do men use the inhibitors?Sex Med2014229610225356304
- YanHZongHCuiYLiNZhangYThe efficacy of PDE5 inhibitors alone or in combination with alpha-blockers for the treatment of erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia: a systematic review and meta-analysisJ Sex Med20141161539154524621088
- HowesLDiltiazem-mediated inhibition of sildenafil metabolism may promote nitrate-induced hypotensionInt Med J2001316373 author reply 374–375
- HuangSTJiannBPAssessing satisfaction in men and their female partners after treatment with phosphodiesterase type 5 inhibitors for erectile dysfunctionInt J Impot Res201325517818223466660
- KlonerRErectile dysfunction and hypertensionInt J Impot Res200719329630217151696
- BrackettNLLynneCMIbrahimEOhlDASonksenJTreatment of infertility in men with spinal cord injuryNat Rev Urol20107316217220157304
- ValeJBenign prostatic hyperplasia and erectile dysfunction – is there a link?Curr Med Res Opin200016Suppl 1s63s6711329825
- RosenRCGiulianoFCarsonCCSexual dysfunction and lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH)Eur Urol200547682483715925080
- GovorovAKasyanGPriymakDPushkarDSorsaburuSTadalafil in the management of lower urinary tract symptoms: a review of the literature and current practices in RussiaCent Eur J Urol2014672167177
- StegemannSEckerFMaioMGeriatric drug therapy: neglecting the inevitable majorityAgeing Res Rev20109438439820478411
- StemerGLemmens-GruberRClinical pharmacy activities in chronic kidney disease and end-stage renal disease patients: a systematic literature reviewBMC Nephrol2011123521777480
- RamaMViswanathanGAcharyaLDAtturRPReddyPNRaghavanSVAssessment of drug-drug interactions among renal failure patients of nephrology ward in a south Indian tertiary care hospitalIndian J Pharm Sci2012741636823204624
- AyubWFletcherSEnd-stage renal disease and erectile dysfunction. Is there any hope?Nephrol Dial Transplant200015101525152811007818
- LasaponaraFSedighOPasqualeGPhosphodiesterase type 5 inhibitor treatment for erectile dysfunction in patients with end-stage renal disease receiving dialysis or after renal transplantationJ Sex Med201310112798281423346948
- PietteJDKerrEAThe impact of comorbid chronic conditions on diabetes careDiabetes Care200629372573116505540
- RosenRCJacksonGKostisJBErectile dysfunction and cardiac disease: recommendations of the Second Princeton ConferenceCurr Urol Rep20067649049617052447
- McLaughlinTHarnettJBurhaniSScottBEvaluation of erectile dysfunction therapy in patients previously nonadherent to long-term medications: a retrospective analysis of prescription claimsAm J Ther200512660561116280655
- ViigimaaMVlachopoulosCLazaridisADoumasMManagement of erectile dysfunction in hypertension: tips and tricksWorld J Cardiol20146990891525276292
- GolchinNFrankSHVinceAIshamLMeropolSBPolypharmacy in the elderlyJ Res Pharm Pract201542858825984546