
Abstract
Videolaryngoscopes improve the view of the entry to the larynx in morbidly obese patients. Super obesity is one of the risk factors for difficult mask ventilation as well as difficult intubation. Super obese patients should be intubated awake either with a fiber-optic scope or with a videolaryngoscope. The glottic view during video-intubation in super obese patients using different devices was compared. The McGrath MAC (MGM) was used in all patients and then compared to the King Vision (KV) in three patients, the APA videolaryngoscope in two patients and the Airtraq Avant with a video camera in four patients. The pictures were of the same patient for two used devices. All obtained images were analyzed using the Percentage of Glottic Opening (POGO) scale. The POGO score for the MGM was better than for the KV and the APA but comparable to the Airtraq device. The images were processed electronically, and the best view of the laryngeal inlet that was obtained by the evaluated devices in the same patient was superimposed onto the other one and then compared.
Introduction
Videolaryngoscopes improve the view of the entry to the larynx in morbidly obese patients.Citation1–Citation4 Moreover, videolaryngoscopes are described as devices that could help to reduce peri-intubation complications, eg, reducing the force required to visualize the glottis would reduce the number of intubation attempts.Citation5,Citation6 In the current literature, there are studies that compared videolaryngoscopes in the morbidly obese patients. These studies have shown differences in the Cormack–Lehane (C-L) laryngoscopic view and the user-friendliness between the devices in randomized groups of patients.Citation7 However, there are no studies available that compare videolaryngoscopes in the same patient. Videolaryngoscopes use modern video camera technology, which varies between different devices. This can result in a different image clarity and quality of the glottic view.Citation8 Despite continuous development of videolaryngoscopes, some important questions remain unanswered, eg, the limitations of these devices in specific circumstances and their comparative performance.Citation9
Super obesity is defined as body mass index (BMI) ≥50 kg·m−2.Citation10 It is one of the risk factors and predictors of both difficult mask ventilation and difficult intubation.Citation11 Super obese patients should be intubated awake either with a fiber-optic scope or with a videolaryngoscope.Citation12
The glottic view during video-intubation in super obese patients was compared.
Patients and methods
This study was approved by the ethics committee of the Medical University of Łódź (RNN/331/15/KE). Nine super obese patients were included into the study. Written informed consent was obtained from all patients before surgery. All participants provided written informed consent to publish this paper and accompanying images. Demographic data are presented in . The patients were scheduled for elective bariatric surgery in a teaching hospital. Anesthetic management was based on the guidelines of European Society for Perioperative Care of the Obese Patient (www.espcop.org). Following effective pre-oxygenation, general anesthesia was induced with intravenous propofol (dose adjusted for bispectral index monitoring [BIS 40-60]). After confirming that bag mask ventilation was possible, intravenous rocuronium was administrated at a dose of 1.2 mg·kg−1 of the ideal body weight. Once an adequate muscle paralysis was confirmed with train-of-four monitoring, the intubation attempts were commenced with the studied devices. All of the evaluated videolaryngoscopes were used in a random order. The McGrath MAC (MGM; Aircraft Medical, Edinburgh, United Kingdom) with blade size 3 was used in all studied cases. The King Vision (KV; Ambu, Ballerup, Denmark) with a non-channeled blade was used in three individuals (patient number 1, 2 and 3). The APA videolaryngoscope (Venner Medical, Singapore, Singapore) with an MAC blade size 3 was used in two cases (patient number 4 and 5) and the Airtraq Avant with a video camera (Prodol Meditec, Las Arena, Spain) was used in four patients, ie, patient number 6–9. The pictures were of the same patient for two used devices. A picture from the monitor display was taken when the best view of the glottis was achieved. This was always done with the same camera and the same investigator for both devices. An additional dose of propofol was administered during an intubation attempt with the second device in order to prevent accidental awareness. Bag mask ventilation was also performed to maintain oxygenation between intubation attempts. General anesthesia was continued once all relevant data were collected.
Table 1 Demographic data of the participants
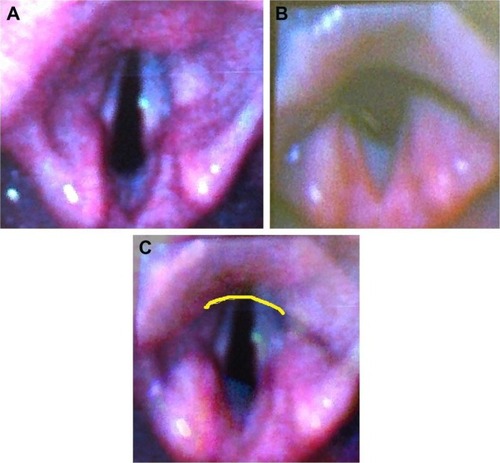
The images were processed electronically, and the best view of the laryngeal inlet that was obtained by the evaluated devices in the same patient was superimposed onto the other one and then compared (). All obtained images were analyzed using the Percentage of Glottic Opening (POGO) scale. The POGO score represents the percentage of the laryngeal inlet seen and can be defined as the line that spans from the anterior commissure to the interarytenoid notch.Citation13
Figure 1 Images electronically processed from patient number 3.
Abbreviations: MGM, McGrath MAC; KV, King Vision.
Results
The demographic data are presented in . The mean values were as follows: weight 146.33±19.87 kg, height 1.68±0.128 m, BMI 51.84±2.77 kg·m−2, age 41±12.13 years and neck circumference 47.66±3.9 cm. Five men and four women participated in the study. The results of the image evaluation are presented in . The examples of pictures taken during the study are shown in (comparison of the MGM and the KV), (comparison of the MGM and the APA) and (comparison of the MGM and the Airtraq). The POGO score for the MGM was better than for the KV and the APA but comparable to the Airtraq device. However, the C-L grade one view was achieved in all cases when the MGM was used. In one case during the use of the KV device, the C-L grade was 3, and there was grade 2 view (C-L) for the APA in one patient. For the Airtraq device, the C-L grade was 1 in all cases. Intubation was possible and uneventful during all attempts. There were no complications related to the glottic visualization.
Figure 2 Images obtained from the same patient with two devices.
Abbreviations: MGM, McGrath MAC; KV, King Vision.
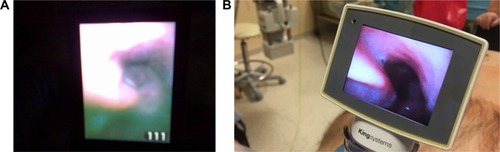
Figure 3 Images obtained from the same patient with two devices.
Abbreviation: MGM, McGrath MAC.
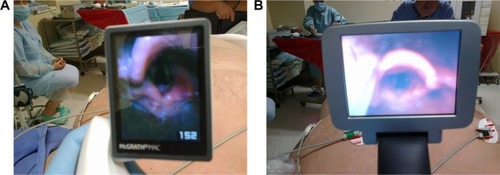
Figure 4 Images obtained from the same patient with two devices.
Abbreviation: MGM, McGrath MAC.
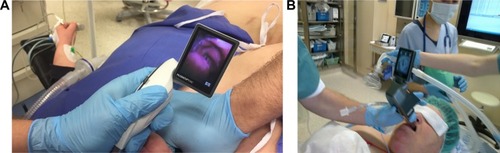
Table 2 Results of the image evaluation
Discussion
The probability of difficult intubation is increased with higher BMI values.Citation14 Neck circumference of >42 cm and BMI of >50 kg·m−2 (super obesity) are two independent predictors of difficult intubation.Citation15 Dixit et alCitation16 observed that 44.4% of super obese patients had C-L grade 3 and 4 views compared to 20.4% of the morbidly obese patients. These results confirm that it is necessary to be prepared for difficult intubation in super obese patients. Therefore, the use of videolaryngoscopes is justified in this group of patients.
In all the available articles, during video-intubation of morbidly obese patients, C-L grade 1 view was achieved in all patients.Citation1–Citation3 There is also a study available on the evaluation of the laryngeal inlet visualization in super obese patients using the TotalTrack Video Laryngeal Mask device. C-L grade 1 view was also achieved in that study.Citation17 There was no evaluation of more sensitive scale than the POGO.Citation13 The POGO score was chosen for this study instead of C-L classification because the former is more adequate. There are several problems regarding the C-L classification and grade 1 and 2 views in particular. The distinction between C-L grade 1 and 2 views is important because they were achieved in 99.7% of patients.Citation13 In addition to this, the variability within the grades is also significant. Benumof noted that the percentage of the vocal cords visible in grade 1 view could vary from 1 to 100%.Citation18 The POGO score appears to be more appropriate when videolaryngoscopes are used. In this study, only the performance of Airtraq Avant was similar to that of the MGM. It has already been described that the use of the Airtraq device provided very good conditions for intubation in the morbidly obese patients. However, no study has been performed in super obese patient population.Citation19–Citation21 Cierniak et al in their study assessed technical properties of video intubating devices, which showed that there could be significant differences between them regarding the clarity, focus and image quality.Citation8 As this was a manikin study, it is difficult to extrapolate the results of such studies into real patients. To the author’s knowledge, this is the first study to evaluate video intubating devices in patients with an increased risk of difficult intubation, ie, super obese patients. This study demonstrates that despite the use of videolaryngoscopes, the glottic visualization may not be perfect. Moreover, this study shows that videolaryngoscopes are good intubating devices in super obese patients. However, even in the same patient, the achieved glottic view may differ between devices.
The key points and findings are as follows:
Difficult intubation is very common in super obese patients.
Videolaryngoscopes may improve the view of the glottis in these patients.
Certain devices may be preferred over others in such a setting.
All anesthetists should know that adequate oxygenation is the cornerstone of rapid sequence induction and airway management.Citation22
Limitations
The weakness of the study is the small sample size. However, this work adds important information to the current literature on the new devices for intubation of super obese patients. The future work should focus on the evaluation of different video intubating devices. Such devices should be compared to one another and not to the classic Macintosh blade laryngoscope. The rationale for this is that video intubating devices always outperform the Macintosh blade laryngoscope in visualization of the glottis in patients known to be difficult to intubate. It is important to assess which video device offers both a better performance as well as increased safety.
Conclusion
The POGO score was better for the MGM than for the KV and the APA but comparable to the Airtraq device. All devices under study allowed safe and effective intubation in super obese patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- MarrelJBlancCFrascaroloPMagnussonLVideolaryngoscopy improves intubation condition in morbidly obese patientsEur J Anaesthesiol200724121045104917608975
- DhonneurGAbdiWNdokoSKVideo-assisted versus conventional tracheal intubation in morbidly obese patientsObes Surg20091981096110118836785
- YousefGTAbdalgalilDAIbrahimTHOrotracheal intubation of morbidly obese patients, comparison of GlideScope® video laryngoscope and the LMA CTrach™ with direct laryngoscopyAnesth Essays Res20126217417925885612
- GaszyńskiTClinical experience with the C-Mac videolaryngoscope in morbidly obese patientsAnaesthesiol Intensive Ther2014461141624643921
- MaassenRLeeRvan ZundertACooperRThe videolaryngoscope is less traumatic than the classic laryngoscope for a difficult airway in an obese patientJ Anesth200923344544819685133
- AndersenLHRovsingLOlsenKSGlideScope videolaryngoscope vs Macintosh direct laryngoscope for intubation of morbidly obese patients: a randomized trialActa Anaesthesiol Scand20115591090109722092206
- MaassenRLeeRHermansBMarcusMvan ZundertAA comparison of three videolaryngoscopes: the Macintosh laryngoscope blade reduces, but does not replace, routine stylet use for intubation in morbidly obese patientsAnesth Analg200910951560156519713258
- CierniakMTimlerDWieczorekASekalskiPBorkowskaNGaszyńskiTThe comparison of the technical parameters in endotracheal intubation devices: the Cmac, the Vividtrac, the McGrath Mac and the KingvisionJ Clin Monit Comput201630437938726120020
- NorrisAHeideggerTLimitations of videolaryngoscopyBr J Anaesth2016117214815027251753
- LeykinYPellisTDel MestroEMarzanoBFantiGBrodskyJBAnesthetic management of morbidly obese and super-morbidly obese patients undergoing bariatric operations: hospital course and outcomesObes Surg200616121563156917217630
- GaszyńskiTGaszyńskaESzewczykTDexmedetomidine for awake intubation and an opioid-free general anesthesia in a superobese patient with suspected difficult intubationDrug Des Devel Ther20148909912
- PelosiPGregorettiCPerioperative management of obese patientsBest Pract Res Clin Anaesthesiol201024221122520608558
- LevitanROchrochAKushSShoferFHollanderJAssessment of Airway Visualization: validation of the percentage of glottic opening (POGO) ScaleAcad Emerg Med1998599199239754506
- LundstrømLHMøllerAMRosenstockCAstrupGWetterslevJHigh body mass index is a weak predictor for difficult and failed tracheal intubation: a cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia DatabaseAnesthesiology2009110226627419194154
- RiadWVaezMNRaveendranRNeck circumference as a predictor of difficult intubation and difficult mask ventilation in morbidly obese patients: a prospective observational studyEur J Anaesthesiol201633424424926351829
- DixitAKulshresthaMMathewsJJBhandariMAre the obese difficult to intubate?Br J Anaesth2014112477077124645166
- GaszyńskiTTotalTrack video intubating laryngeal mask in super-obese patients – series of casusTher Clin Risk Manag20161233533827042078
- BenumofJLConventional orotracheal and nasotracheal intubationBenumofJLAirway Management: Principles and PracticeSt. LouisMosby-Year Book1996261276
- DhonneurGNdokoSAmathieuRHousseiniLEPonceletCTualLTracheal intubation using the Airtraq in morbid obese patients undergoing emergency cesarean deliveryAnesthesiology2007106362963017325521
- NdokoSKAmathieuRTualLTracheal intubation of morbidly obese patients: a randomized trial comparing performance of Macintosh and Airtraq laryngoscopesBr J Anaesth2008100226326818211999
- GaszyńskiTGaszyńskiWA comparison of AirTraq optical laryngoscope and classic Macintosh blade laryngoscope for endotracheal intubation in morbidly obese patients. [Porównanie zastosowania laryngoskopu optycznego AirTraq i laryngoskopu klasycznego z łopatką Macintosh do intubacji dotchawiczej u chorych z otyłością]Anaesthesiol Intensive Ther2009413145148
- BertranSChouillardEKassirRDifficult tracheal intubation in obese gastric bypass patientsObes Surg201626102490249127510589