
Abstract
Background
In total knee arthroplasty, it is better to use more than one reference point for correct alignment of the components. By measuring the distances of Achilles tendon (AT) and other conventional landmarks from the mechanical axis in magnetic resonance imaging (MRI) of the ankle, we aimed to demonstrate that, as a novel landmark which can help for correct alignment in the coronal plane, AT is a better option than other landmarks.
Materials and methods
This retrospective study was done on 53 ankle MRIs that met the criteria for inclusion to the study among 158 ankle MRIs. After identification of the mechanical axis, the distances of distal landmarks, which were extensor hallucis longus tendon (EHLT), tibialis anterior tendon (TAT), dorsalis pedis artery (DPA), AT, extensor digitorum longus tendon (EDLT), and malleoli, were measured from the mechanical axis and were statistically evaluated.
Results
In proximal measurements, the distances of the landmarks to the mechanical axis (on average) were AT, 2.64±1.62 mm lateral; EHLT, 3.89±2.45 mm medial; DPA, 4.69±2.39 mm medial; TAT, 8.24±3.60 mm medial; and EDLT, 14.2±4.14 mm lateral (P<0.001). In distal measurements, the distances of the landmarks to the mechanical axis (on average) were AT, 1.99±1.24 mm medial; EHLT, 4.27±2.49 mm medial; DPA, 4.79±2.10 mm medial; TAT, 12.9±4.07 mm medial; and EDLT, 12.18±4.17 mm lateral (P<0.001).
Conclusion
In this study, the mechanical axis line, which is the center of talus, passes through the AT. Our MRI investigations showed that the AT, EHLT, DPA, and malleolar center (3–5 mm medial) may help in correct alignment.
Introduction
The number of patients with severe osteoarthritis increases with aging. Therefore, the quality of life markedly is decreased. Total knee arthroplasty (TKA) is advised to be the best method for treating advanced osteoarthritis. TKA is thought to alleviate pain, restoration of joint function and betterment in quality of life, with 95% implant survivorship over 15 years.Citation1,Citation2 Plausibly, one of the most commonly used methods to assess coronal alignment is anteroposterior fluoroscopy in combination with an electrocautery cord. It is strung from the center of the femoral head to the center of the ankle joint. The fluoroscopy image of the knee will then demonstrate the mechanical axis (MA) of the lower limb.Citation3,Citation4
In TKA, and in all external reference systems used to ensure proper coronal alignment, the center of talus should be targeted. Previous studies have shown that, for the alignment to be considered as good, the axis deviation should be below 2 degrees.Citation5–Citation7 Numerous anatomical reference points that can help in proper alignment have been suggested. Second metatarsal bone,Citation8 extensor hallucis longus tendon (EHLT),Citation9 malleolar center,Citation10–Citation12 tibialis anterior tendon (TAT),Citation13 anterior tibial crest,Citation14,Citation15 and dorsalis pedis artery (DPA)Citation16 are some of these. The used landmarks have clinical advantages and disadvantages. Although tendons are palpable, they are affected by ankle movements.Citation9 DPA cannot be always palpated and may not be available during surgery due to the tourniquet application. Malleolar center, although palpable, is not exactly at the axis passing through the center of talus.Citation10–Citation12
We aimed to demonstrate that Achilles tendon (AT), as a novel landmark, is a better option that can help for correct alignment in the coronal plane when compared with other landmarks by measuring the distances of AT and other conventional landmarks from the MA in magnetic resonance imaging (MRI) of the ankle.
Materials and methods
This retrospective, observational MRI study was conducted on 53 ankle MRIs that met the criteria for inclusion to the study among 158 ankle MRIs. The MRIs were taken between years of 2013–2014 in Kırıkkale University Hospital. Approval of Kırıkkale University Ethics Committee was obtained (2015-28/01). Patients referred to the radiology department for an ankle MRI exam were considered eligible for inclusion in the present study. The inclusion criteria were as follows: subjects with no history of femoral and tibia fracture or surgery; age greater than or equal to 18 years; procurement of written informed consent to participate in the study. Subjects with ankle osteoarthritis, fracture sequela, tendon injuries, and tibial rotational deformities or those who had undergone surgery for fractures and similar causes were excluded (). The demographic data of patients who underwent measurements were recorded ().
Figure 1 Flow diagram of the exclusion criteria for this study.
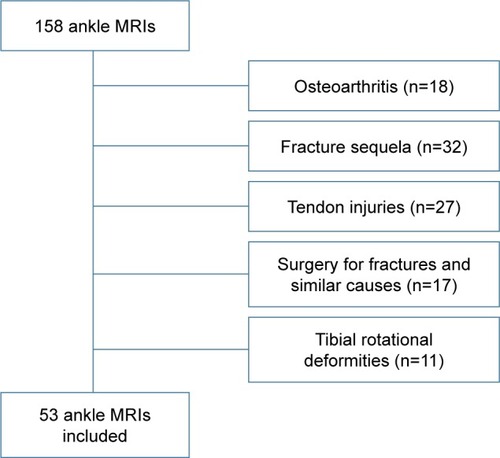
Table 1 Demographical characteristics of the patients
MR imaging technique
All MRIs were performed on an Achieva 1.5T MRI system (Philips Medical Systems, Best, the Netherlands) using ankle coil eight elements. The imaging protocol axial, sagittal, and coronal 3D T1-weighted TR (ms) 574, TE (ms) 20 TSE images (FOV, 170×121 mm and matrix, 344×195 mm) were obtained using a 2 mm slice thickness and 0.5 mm intersection gap; so 70 slices were obtained.
MRI measurements
In this study, the center of the talus and MA were determined in T1W axial, sagittal, and coronal images by 3D software. After identification of midpoints of each landmark (EHLT, DPA, TAT, AT, extensor digitorum longus tendon [EDLT]), their distances to the MA were measured from the point 2 mm proximal to the tibial distal articular surface and from the point 2 mm distal to the articular surface of talus (). In coronal T1W images, the distance from the most prominent regions of malleolar bone to the MA was measured as was skin thickness (). All measurements were made by a specialist in radiology.
Figure 2 Center of the talus and mechanical axis were determined in T1W axial, sagittal, and coronal images by 3D software.
Abbreviations: AT, Achilles tendon; DPA, dorsalis pedis artery; EDLT, extensor digitorum longus tendon; EHLT, extensor hallucis longus tendon; TAT, tibilais anterior tendon.
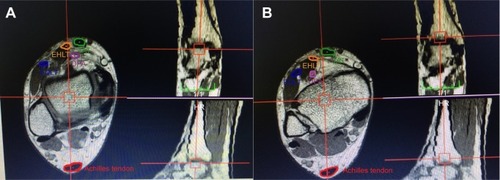
Figure 3 The distance from the most prominent regions of malleolar bone to the mechanical axis and also skin thickness were measured.

Statistical analysis
All statistical analyses were performed with Statistical Package for the Social Sciences (SPSS) version 16.0 (SPSS Inc., Chicago, IL, USA). A confidence interval of 95% and a two-tailed P<0.05 were determined to be statistically significant for all of the analyses. The distance between the center of the talus and each landmark was expressed as mean and standard deviation. One-way analysis of variance with Turkey–Kramer test was used for the comparison among landmarks. Student’s t-test was used to compare quantitative variables between distal and proximal measurements. Statistical significance was set at P<0.05.
Results
In this study, measurements were made on ankle MRIs of 53 patients. The study population consisted of 29 females and 24 males. The mean age of all patients was 44.8 years (range 21 to 65 years). Right ankle MRIs were taken in 27 patients and left ankle in 26 patients.
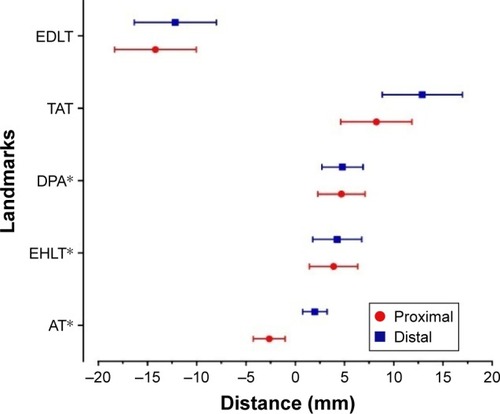
In proximal measurements, the distances of the landmarks to the MA (on average) were as follows: AT, 2.64±1.62 mm lateral; EHLT, 3.89±2.45 mm medial; DPA, 4.69±2.39 mm medial; TAT, 8.24±3.60 mm medial; and EDLT, 14.2±4.14 mm lateral. In distal measurements, the distances of the landmarks to the MA (on average) were as follows: AT, 1.99±1.24 mm medial; EHLT, 4.27±2.49 medial; DPA, 4.79±2.10 mm medial; TAT, 12.9±4.07 mm medial; and EDLT, 12.18±4.17 mm lateral. No statistically significant difference was found between proximal and distal measurements in terms of AT (P<0.099).
shows the distance between the ankle center and each landmark in 53 patients. There were no significant differences between proximal and distal measurement of each landmark. Among five anatomical landmarks, the AT was located anatomically closest to the ankle center in patients. Statistical analysis showed that the AT the DPA and the EHLT were located significantly closer to the ankle center when compared with the EDLT and the TAT in patients (P<0.001).
Figure 4 The distance between the ankle center and each landmark. TAT, EHLT, EDLT, DPA, and AT.
Abbreviations: AT, Achilles tendon; ANOVA, analysis of variance; DPA, dorsalis pedis artery; EDLT, extensor digitorum longus tendon; EHLT, extensor hallucis longus tendon; TAT, tibilais anterior tendon.
There were no difference in the distance of these landmarks between males and females and between left and right knees of males and females patients.
The distances of malleoli from the MA were as follows: for lateral malleolus (skin excluded) 26.14±2.99 mm on average and for medial malleolus (skin excluded) 22.57±2.13 mm on average. The average difference between malleoli was found to be 4.10±2.50 mm laterally. Average skin thicknesses were 3.67±2.11 laterally and 3.51±2.40 mm medially. The difference between lateral and medial skin thicknesses was 0.16±2.05 mm, being greater laterally.
In all measurements, AT was found to be passing through the MA. When proximal and distal measurements of AT were compared to the other landmarks, the distance of AT to the MA was found to be statistically better (P<0.001).
Discussion
Our MRI investigations showed that AT might be helpful for correct alignment in total knee replacement surgery. The landmarks used for coronal alignment during TKA have some advantages and disadvantages clinically. TAT is a palpable and easily detectable landmark. However, it is too medial to the center of the ankle. EHLT has been described as the best reference point. However, identification of this tendon during surgery is not as easy as TAT and it can be confused with EDLT. Additionally, the locations of these two tendons may vary with the position of the ankle and may mislead the surgeon.Citation9 The technique using the bi-malleolar center has been reported as another significant reference point. The point located 3–5 mm medial to the malleolar center has been suggested for use as the center of the ankle.Citation10,Citation12,Citation17–Citation19 Its disadvantage is difficulty in palpation, which sometimes occurs during surgery. Its advantage is that it is unaffected by ankle movements. Fukagawa et al,Citation14 in their study, suggested using the distal ¼ of tibial crest as the reference point. The disadvantage of this reference point is its inability to be used in overweight patients or patients who have tibial deformities or excess bowing.
In previously reported studies, EHLT, DPA, and malleolar center were shown to be located close to the center of the ankle in coronal plane.Citation9–Citation12 When tibial length is 353 mm, 6.2 mm deviation at the ankle center leads to 1 degree error in coronal plane.Citation20 In our study, AT, EHLT, DPA, and malleolar center were shown to help tibial alignment with an error of approximately less than 2 degrees.
Sugimura et al,Citation16 in their Doppler ultrasonography study on patients with valgus gonarthrosis determined that the average distances were as follows: DPA, 0.4±3.4 mm lateral; EHLT, 0.7±3.5 mm medial; malleolar center, 1.1±3.3 mm medial; EDLT, 5.7±3.1 mm lateral; and TAT, 12.0±3.3 mm medial. They suggested that DAP and EHLT might be used as external reference points for TKA and that TAT and EDLT should be avoided. The results of our investigation with ankle MRI were statistically similar to the study of Sugimura et al. In our study, the proximity order of landmarks to the MA was as follows: AT, EHLT, DAP, malleolar center, TAT, and EDLT. Sugimura et al had performed their measurements by ultrasonography, whereas ours were by MRI; we consider that our measurements were more effectively and objectively made.
Akagi et al,Citation10 in their study measuring the distance of malleolar center to the MA, found that it was 3.7±1.4 mm in coronal plane and 1.2±1.5 mm in axial plane. Thus, they showed that this difference had led to errors of 0.6±0.2 degrees in coronal plane and 0.2±0.3 degrees in the axial plane. They reported that malleolar center, although leading to minimal error laterally, might be suitable for use for tibial alignment. In our study, the distances of malleoli to the talus-centered MA were measured. On the basis of our results, we determined that malleoli may be suitable to be used for tibial alignment (P<0.001). The difference caused by soft tissues was found to be 0.16±2.05 mm, and this did not adversely affect the alignment. However, our suggestion is that the point 3–5 mm medial to the malleolar center is a more precise reference point, as advocated by many authors.Citation10,Citation12,Citation17–Citation19
The weaknesses of our study are as follows: this was a retrospective study and had all limitations of retrospective studies; gonarthrosis patients were not investigated; ethnic factors and anatomical variations might have affected our study results; and, finally, clinical applications were not studied.
Conclusion
In this study, it was shown that the MA line, which is the center of the talus, passes through AT. Our MRI investigations showed that AT, EHLT, DPA, and malleolar center (3–5 cm medial) might be helpful for correct alignment in total knee replacement surgery. EDTL and TAT, due to their distances, should not be preferred. The most significant advantage of AT, when compared to other reference points, is that it can be used both preoperatively and intra-operatively since it is palpable. Moreover, since there is no statistically significant difference between measurements made from points approximately 1 cm proximal and distal to the ankle joint, we consider that it can prevent the difficulties and errors that can occur in determination of the axis during surgery. Its disadvantage is not being suitable for present external reference devices, since it is located at the posterior side of the ankle. We suggest using AT in TKA as a tibial distal reference point for alignment in the coronal plane.
Ethics approval and consent to participate
This scientific research study was approved by the ethics committee of Kırıkkale University Ethics Committee (2015-28/01). Written informed consent was taken from all of the volunteers.
Disclosure
The authors report no conflicts of interest in this work.
References
- GandhiRDhotarHRazakFTsoPDaveyJRMahomedNNPredicting the longer term outcomes of total knee arthroplastyKnee2010171151819589683
- LachiewiczPFSoileauESFifteen year survival and osteolysis associated with a modular posterior stabilized knee replacement: a concise follow-up of a previous reportJ Bone Joint Surg Am20099161419142319487520
- PivecRIssaKKesterMHarwinSFMontMALong term outcomes of MUA for stiffness in primary TKAJ Knee Surg201326640541023512543
- SmithTOKingJJHingCBA meta-analysis of randomized controlled trials comparing the clinical and radiological outcomes following minimally invasive to conventional exposure for total knee arthroplastyKnee20121911721196121
- SikorskiJMComputer-assisted revision total knee replacementJ Bone Joint Surg Br20048651051415174544
- AgliettiPBuzziRPosteriorly stabilized total-condylar knee replacement. Three to eight years’ follow-up of 85 kneesJ Bone Joint Surg Br1988702112163346290
- ReedMRBlissWSherJLEmmersonKPJonesSMPartingtonPFExtramedullary or intramedullary tibial alignment guides: a randomized, prospective trial of radiological alignmentJ Bone Joint Surg Br20028485886012211678
- TewMWaughWTibiofemoral alignment and the results of knee replacementJ Bone Joint Surg Br1985675515564030849
- SchneiderMHeiselCAldingerPRBreuschSJUse of palpable tendons for extramedullary tibial alignment in total knee arthroplastyJ Arthroplasty20072221922617275637
- AkagiMAsadaSMoriSMatsushitaTHashimotoKHamanishiCEstimation of frontal alignment error of the extramedullary tibial guide on the bi-malleolar technique: a simulation study with magnetic resonance imagingKnee20121983684222507073
- DennisDAChannerMSusmanMHStringerEAIntramedullary versus extramedullary tibial alignment systems in total knee arthroplastyJ Arthroplasty1993843478436988
- SistonRADaubACGioriNJGoodmanSBDelpSLEvaluation of methods that locate the center of the ankle for computer-assisted total knee arthroplastyClin Orthop Relat Res200543912913516205151
- RajadhyakshaADMehtaHZelicofSBUse of tibialis anterior tendon as distal landmark for extramedullary tibial alignment in total knee arthroplasty: an anatomical studyAm J Orthop (Belle Mead NJ)2009383E68E7019377655
- FukagawaSMatsudaSMitsuyasuHAnterior border of the tibia as a landmark for extramedullary alignment guide in total knee arthroplasty for varus kneesJ Orthop Res20112991992421259337
- TsukeokaTLeeTHTsuneizumiYSuzukiMThe tibial crest as a practical useful landmark in total knee arthroplastyKnee201421128328923154034
- SugimuraNIkeuchiMIzumiMAsoKUshidaTTaniTThe dorsal pedis artery as a new distal landmark for extramedullary tibial alignment in total knee arthroplastyKnee Surg Sports Traumatol Arthrosc201422112618262223455389
- InsallJNEasleyMESurgical technique and instrumentation. Section X. Joint replacement and its alternativesInsallJNScottWNSurgery of the Knee3rd edPhiladelphia, PAChurchill Livingstone200115531620
- NofriniLSlomczykowskiMIaconoFMarcacciMEvaluation of accuracy in ankle center location for tibial mechanical axis identificationJ Invest Surg200417232914761825
- BekDEgeTYıldızCTunaySBaşbozkurtMThe accuracy of two different extra-medullary tibial cutting guides for posterior tibial slope in total knee arthroplastyEklem Hastalik Cerrahisi201425757925036392
- ParratteSPagnanoMWTrousdaleRTBerryDJEffect of postoperative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacementsJ Bone Joint Surg Am201092122143214920844155