Abstract
The relation of hemophilia A with thrombophilia V Leiden is extremely rare in the literature. Furthermore, hemophiliac patients have an increased risk of severe life-threatening hemorrhage, blood transfusions, and therefore hepatitis transmission, mainly hepatitis C (HCV).
Aims and methods
We present a 54-year-old male with a 5-year history of decompensated liver cirrhosis on the grounds of HCV hepatitis, hemophilia A, and thrombophilia V Leiden. He was admitted to our department because of severe abdominal distension, resembling ‘tense ascites’ despite the use of diuretics. Clinical examination showed shifting dullness and a protuberant abdomen, while hematological and blood chemistry results revealed thrombopenia (platelets: 77000/mL) and hypoalbuminemia. Repeated abdominal paracentesis (under factor VIII administration) failed to remove ascitic fluid, while abdominal echosonography and computed tomography revealed severe edema of mesenterium and intraabdominal viscus and the absence of free ascitic fluid, atrophic cirrhotic liver, and splenomegaly. Moreover, abdominal doppler echosonography revealed signs of portal hypertension, previous portal vein thrombosis, and revascularization of the portal vein. Gastroscopy showed esophageal varices grade II, without signs of bleeding. A-FP and all other laboratory examinations were normal.
Results
Our patient was intravenously treated with albumine and diuretics (furosemide) with mild improvement of his abdominal distension. During his hospitalization he presented an episode of spontaneous bacterial peritonitis and hepatic encephalopathy, which were successfully treated with lactulose clysmas and ciprofloxacine. He was discharged in a good general condition.
Conclusion
According to our case we consider the false clinical picture of ‘tense ascites’ of our patient as a rare clinical presentation of decompensated liver cirrhosis, with severe edema of mesenterium and viscus, on the grounds of preexisting portal vein thrombosis, in a patient with combined hemophilia A and thrombophilia V Leiden.
Introduction
The relation of hemophilia A with thrombophilia V Leiden is extremely rare in the literature.Citation1,Citation2 Furthermore, hemophiliac patients have an increased risk of severe life-threatening hemorrhage and blood transfusions, and consequently they are at increased risk of hepatitis transmission, mainly hepatitis C virus (HCV), which is a major health problem in this group of patients with hereditary hemorrhagic disorders, leading finally to cirrhosis.Citation3,Citation4 The problem becomes more complicated in the very rare case of cirrhoric patients with combined hereditary hemorrhagic and thrombophilic disorder. We report our experience from an interesting case of a patient with HCV liver cirrhosis and combined hemophilia A and thrombophilia V Leiden, who was admitted to our department with false clinical presentation of ‘tense ascites’.
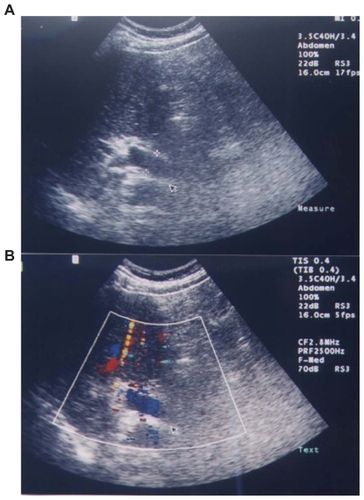
We present a 54-year-old male patient with a 5-year history of decompensated liver cirrhosis child C, on the grounds of HCV hepatitis, hemophilia A, and thrombophilia V Leiden. He was admitted to our department because of severe abdominal distension, resembling ‘tense ascites’ despite the use of diuretics. The patient had done all the pro-thrombotic workup including protein C, S, antithrombin, lupus anticoagulants, antiphospholipid antibodies, and cryoglobulins, which were normal. The levels of factor FVIII:C were 3.5%. Clinical examination showed shifting dullness and protuberant abdomen, while hematological and blood chemistry examination revealed thrombopenia (platelets: 77000/mL) and hypoalbuminemia. Repeated abdominal paracentesis (under factor VII administration) failed to remove ascitic fluid, while abdominal echosonography and computed tomography revealed severe edema of mesenterium and around the intraabdominal viscus and the absence of free ascitic fluid, atrophic cirrhotic liver, and splenomegaly (). Moreover, abdominal doppler echosonography revealed signs of portal hypertension, previous portal vein thrombosis, and revascularization of the portal vein (). Gastroscopy showed esophageal varices grade II, without signs of bleeding, while A-FP and all other laboratory examinations were normal.
Figure 1 Abdominal echosonography (A) and computed tomography (B) show severe edema of mesenterium and the absence of free ascitic fluid, atrophic cirrhotic liver, and splenomegaly.
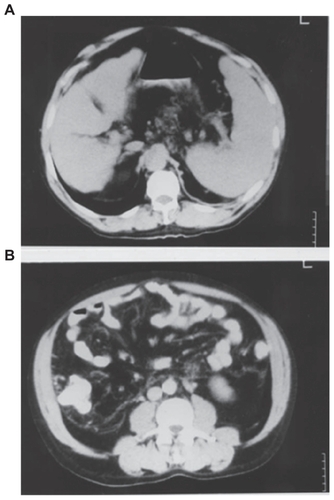
Figure 2 Abdominal doppler echosonography shows signs of portal hypertension, previous portal vein thrombosis, and revascularization of the portal vein.
Although inherited thrombophilic disorders (factor V Leiden [FVL], mutation G20210A of prothrombin [PTHR A(20210)], and mutation TT677 of methylenetetrahydrofolate reductase [MTHFR C677–>T]) have been identified and associated with increased risk of venous thrombosis, as well as in noncirrhotic portal thrombosis, while on the other hand, portal vein thrombosis has been reported in a few case reports in cirrhotic patients with hemophilia A, little is known about the therapy of choice in portal vein thrombosis in the extremely rare case of combined hereditary hemorrhagic and thrombophilic disorder as in our case.Citation4–Citation6
According to clinicolaboratory results of our patient, in combination with the absence of data regarding the definite therapy in similar cases, we decided to further treat the patient only with albumin and diuretics (furosemide) intravenously with mild improvement of his abdominal distension. Neither anticoagulant therapy nor antiplatelets were administered.
During his hospitalization he presented an episode of spontaneous bacterial peritonitis and hepatic encephalopathy, which were successfully treated with lactulose clysmas and ciprofloxacine intravenously. He was discharged in a good general condition. During the follow-up period one year after the diagnosis of portal vein thrombosis our patient is in a stable general condition under continuous diuretic therapy; however, the severe abdominal distension remained.
According to the present case we consider the false clinical picture of ‘tense ascites’ of our patient as a rare clinical presentation of decompensated liver cirrhosis, with severe edema of mesenterium and viscus, on the ground of preexisting portal vein thrombosis, in a patient with combined hemophilia A and thrombophilia V Leiden. However, further studies are necessary in order to determine the optional therapy in this rare but extremely life-threatening case.
Disclosure
No conflicts of interest were declared in relation to this paper.
References
- van ‘t VeerCGoldenNJKalafatisMAn in vitro analysis of the combination of hemophilia A and factor V (LEIDEN)Blood1997908306730729376587
- PettingshausenCESaguerIMKreuzWPortal vein thrombosis in a patient with severe haemophilia A and FV G1691A mutation during continuous infusion of F VIII after intramural jejunal bleeding–successful thrombolysis under heparin therapyEur J Pediatr1999158Suppl 3S18018210650865
- IguchiTUedaYAnalysis of HCV infection in patients with hemophiliaKansenshogaku Zasshi19967066136178741711
- SartoriMTMaresMGirolamiAPortal vein thrombosis in a patient with severe haemophilia A and post-hepatitis liver cirrhosisHaematologia (Budap)19912421171191667775
- AmitranoLBrancaccioVGuardascioneMAInherited coagulation disorders in cirrhotic patients with portal vein thrombosisHepatology200031234534810655256
- DenningerMHChaitYCasadevallNCause of portal or hepatic venous thrombosis in adults: the role of multiple concurrent factorsHepatology200031358759110706547